3.2. Consensus about the Core Elements of the Standardized Integrated Care Pathway PANOS
- 1.
Patient registration (REG)
In order to allow for a timely and equal access, easy-to understand, low-threshold clinical registration criteria were formulated under consideration of the international expert-based consensus processes for the definition of advanced PD [
18] (
Table 3;
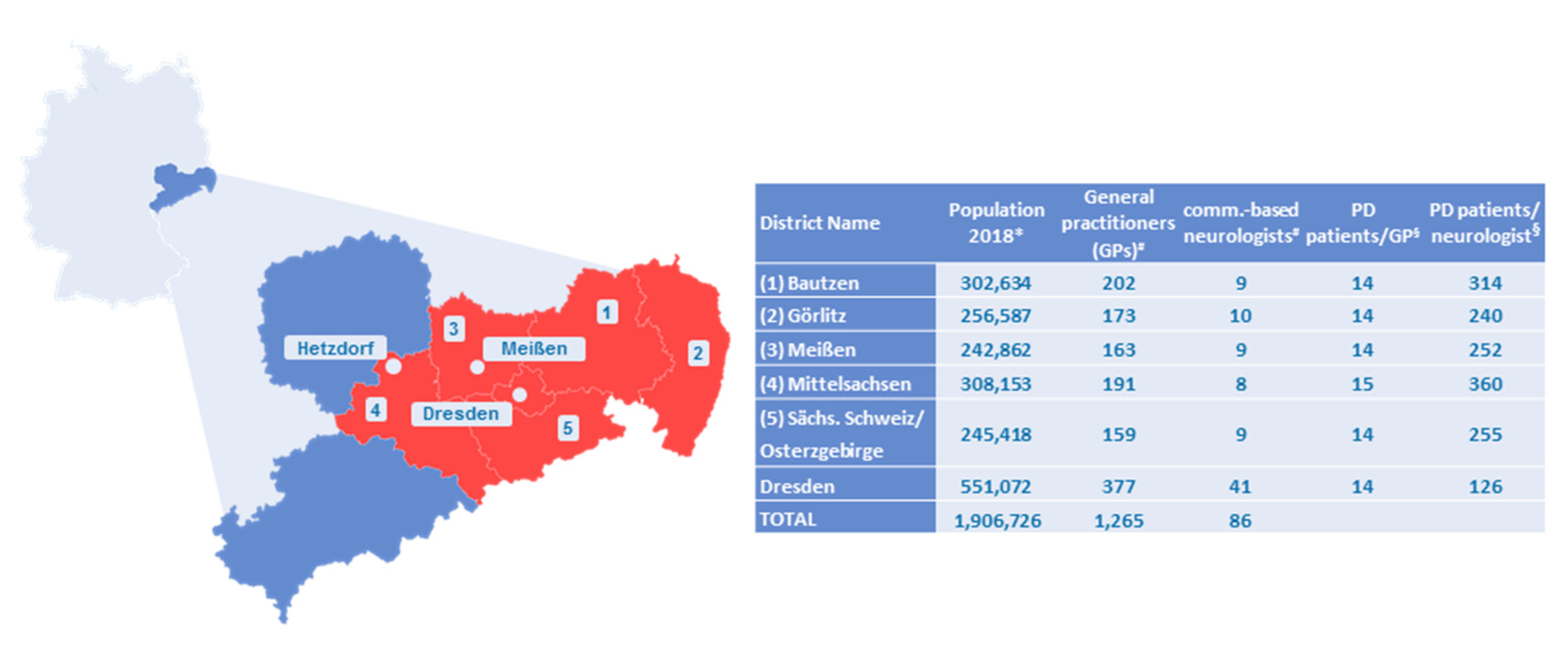
Table 4, REG2). However, these criteria were adopted to facilitate an easy understandability for both patients and GPs, and to be more sensitive to patients in the early transition phase from early to advanced PD. Since up to 40% of PD patients in the region of Eastern Saxony do not have access to a community-based neurologist, registration must also be possible for GPs (
Table 4, REG5). Inscribing physicians must provide information about urgency. A professional registration will be carried out via the web-based electronic health record (EHR) (
Table 4, REG1), but an additional paper-based registration and a patient self-assessment tool will be provided (
Table 4, REG3, 4). Since the varying motivation of >1.300 potentially registering physicians in Eastern Saxony could present a considerable bottle-neck, self-registration may exceptionally be undertaken by patients themselves (
Table 4, REG3, 4).
However, patient self-registration raised concerns and was only consented after more detailed explanations were provided. The major concern was that it could present an uncontrollable bias to physician-based eligibility selection. The following procedural steps enabled the consensus: the case manager reviews all (self-) registrations and always informs the treating community-based physician in case one of his/her patients chooses self-registration. In case of dissent about eligibility, indicated urgency, or self-registration, the case manager will try to achieve an interprofessional consensus (collaborative consensus principle of PANOS) (
Table 4, REG6).
Registered patients are to be distributed between the three Parkinson centers according to their zip codes. Deviation from this principle might occur in case a strong imbalance in patient load develops between the three centers (
Table 4, REG6).
- 2.
Pre-consultation patient self-monitoring and baseline information collection (PCM)
Within PANOS, patients are to assume an active role in their own healthcare. In order to prepare patients for a more active role, a standardized patient education will be offered to promote self-management capacities (see below). One important self-management competence is self-monitoring [
19]. Before getting their first consultation in a Parkinson center, patients will be asked to fill in a standardized self-monitoring package at home, containing validated self-assessment tools for motor and non-motor symptoms and for psychosocial health domains (
Table 4, PCM1).
In addition, patients will be asked to contribute as much as possible to the gathering of their medical history as the baseline for the ongoing longitudinal care within PANOS. Patients will be supported by their individually assigned case manager and several iterations might take place, as long as the patient’s condition and the urgency as indicated by the inscribing physician permit this. The rational for this approach is to both involve the patient as an active partner and to allow for an efficient collection of standardized health-related information.
Self-monitoring packages will first be provided as machine-readable paper-based questionnaires in order to not exclude patients without sufficient digital competence. However, electronic patient self-monitoring (e.g., app-based), as well as sensor-based monitoring, are envisaged as the proximal expansion stages of PANOS. Returned information will be processed semiautomatically and integrated into the EHR.
- 3.
Triage (TRI)
Based on the comprehensive information gathered by the patient-based pre-consultation monitoring, all consultations will be organized based on a triage system with the criteria of urgency (emergency, urgent or regular) and expected complexity and associated time need (
Table 4, TRI1). Although a clear goal of PANOS is to promote outpatient care, inpatient hospital admissions can be initiated if required by the patient’s condition.
- 4.
Structured specialist consultation
Consultations with PD specialists in Parkinson centers will be based on a standardized process with clearly defined responsibilities among the center staff in order to ensure efficient workflows. The consultation duration and agenda are determined by the preceding triage process and the information available due to the pre-consultation patient self-monitoring.
Consultations will be divided into a non-medical visit with the case manager personally assigned to an individual patient and a subsequent medical consultation with the PD specialist. The case manager complements missing monitoring information together with the patient and performs additional professional tasks as assigned. The specialist can then base his/her consultation on this prior work contributed by the patient and his/her case manager. The entire workflow and all required documentations will be reflected by the EHR.
Work organization during structured consultations within the Parkinson centers, albeit discussed in the workshops, was not a subject matter of the structured consensus because of the deliberate focus on intersections relevant to intersectoral collaborative work organization.
- 5.
Individualized ongoing intersectoral care plan (ICP)
At the end of each center consultation, specialists are to suggest an individualized ongoing care plan for the following 12 months to all other involved healthcare providers and the patient (
Table 4, ICP1). As part of this care plan, the following aspects have to be determined:
- (a)
Frequency, time frames and relative professional contribution (community-based physician vs. specialist) to future scheduled outpatient consultations within PANOS. Depending on the individual patient’s condition, all distributions are possible, ranging from 100% care provision by community-based physicians (for patients still in the early transition phase) to a 100% care provision by Parkinson centers (for patients with complex therapeutic needs or important complications)
- (b)
Structured eligibility assessment for inpatient rehabilitation programs
- (c)
Recommendations for frequency and therapeutic objectives of active therapies (physiotherapy, occupational or speech therapy)
- (d)
Individualization of content or frequency of the predefined packages of the repetitive patient self-monitoring
This individualized ongoing care plan is understood to be an important instrument to allow for efficient resource allocation. The low-threshold clinical registration criteria imply that patients with important variations in therapeutic needs will be treated in PANOS. Without an element for individualized need-adjusted care intensity within the standards of the care pathway, an economic care delivery would be severely compromised.
Care plans as suggested by PD specialists will be shared via the EHR. In case of dissent, all involved healthcare providers can suggest changes until a mutual consensus is reached.
- 6.
Repetitive patient self-monitoring (MON)
All patients registered in PANOS will be asked to complete quarterly standardized self-monitoring packages.
In addition to the general arguments given above for self-monitoring, the quarterly repetitions are to function as a safeguard for the early detection of relevant changes in patient conditions, independent of the individualized ongoing care plans. Different content volumes will be defined for every 3, 6, and 12 months. Both frequency and volume can be individualized to exceed the predefined minimal monitoring standard if a patient’s specific situation warrants this. The monitoring results are recorded in the EHR and can be accessed by all relevant EHR-users.
Having repetitive detailed information about a patient’s condition means a gain in responsibility to take timely action. In order to assure this and not to overcharge community-based physicians, the main responsibility will be taken by the staff of the Parkinson centers (
Table 4, MON3).
Community-based physicians need explanations of the instruments and on the interpretation of results that will be displayed on the EHR (
Table 4, MON2). The option for community-based physicians to adjust the monitoring packages was not consented (
Table 4, MON1).
These results are in line with preceding split-group discussions. GPs especially expressed the concern of potentially being overcharged by more detailed insights into a patient’s condition as provided by the repetitive monitoring.
- 7.
Structured consultation with community-based physicians (CBP)
For all patients who do not require regular specialist consultations, the individualized ongoing care plan might envisage all or the majority of ongoing care to be provided by the collaborating community-based physician (e.g., patients in the late stages of their honeymoon phase, or early stages of transition phase). In order to enable collaborative work, all healthcare providers will have full access to the EHR, and their tasks will be defined by a structured workflow integrated into the EHR. Since both the extent of standardized responsibilities and the related design of data visualization will have an impact on the willingness to become an active contributor to PANOS, both aspects received substantial coverage. Even if registered in PANOS, not all patients will have access to community-based neurologists, and therefore some GPs will become active long-term contributors in collaboration with the Parkinson centers. It is therefore of high importance to understand and meet the needs of a diverse group of potential active contributors.
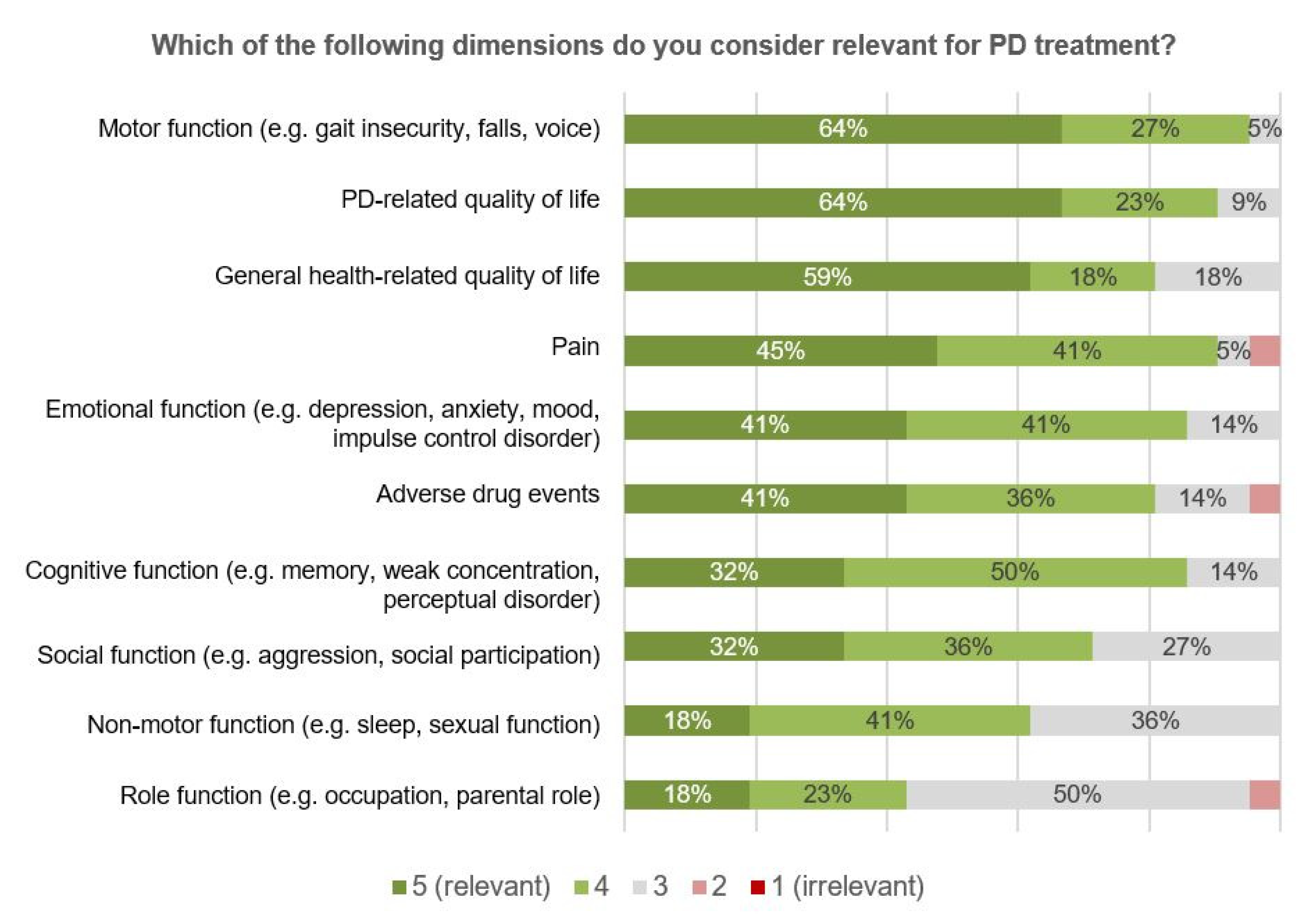
As part of the online surveys, participants were asked to prioritize the monitoring of different PD-related symptoms, and of functional and psychosocial health-related domains (
Figure 4). By rating motor symptoms as the most, and PD-related quality of life (QoL) as the second most, important aspect, participants recognized the importance of monitoring different levels of health in PD, ranging from symptoms, over functions to the overall impact on the patient’s QoL [
20]. In general, a lower relevance was attributed to psychosocial health-related domains such as role or emotional functioning.
Regarding the work distribution between Parkinson centers and community-based physicians, the maintenance of the medication plan was consented to be a responsibility of community-based physicians (
Table 4, CBP1), but not the conduction of standardized clinical tests, such as the MoCA (
Table 4, CBP2). This was rather agreed to be a responsibility of the center-affiliated case managers (see below at intersectoral specialized case management).
- 8.
Additional time requirements of community-based physicians
Additional time requirements for community-based physicians are to be expected due to participation in PANOS. In order to account for this, there will be a supplementary payment of EUR 25–35. Acceptable additional time requirements were discussed in the split-group discussion rounds, and averaged acceptable durations from the split-group discussions were included in subsequent TED votings. As it already became evident in the discussion rounds, there was a huge variability in the time spent on an individual PD patient’s community-based care, accompanied by a large variation in the acceptable additional time requirements. Therefore, no overall consensus could be achieved (
Table 4, ATR1–7). However, under consideration of the supplementary payment, it was consented that each neurologist consultation could be extended by an additional 15 min (
Table 4, ATR6), and that there could be up to one additional quarterly consultation (
Table 4, ATR7).
3.3. Supportive Personal, Technical and Communicative Measurements
- 1.
Electronic health record (EHR)
An EHR tailored to the specific use case of the PANOS is regarded as a crucial basis for efficient and truly collaborative structured intersectoral care. The EHR will be a web-based application that visualizes not only all relevant clinical information (e.g., medical reports, diagnostic test results, results of the repetitive patient self-monitoring), but will also define workflows and associated tasks as part of the standardized care pathway. Where relevant and feasible, the interoperability to other EHRs is planned (e.g., the online communication and billing system by the German Association of SHI physicians KV-SafeNet). Both the definition of acceptable work packages and a high-quality user interface (UI) will have an important impact on efficiency, quality of care and on the professional motivation to become a reliable contributor.
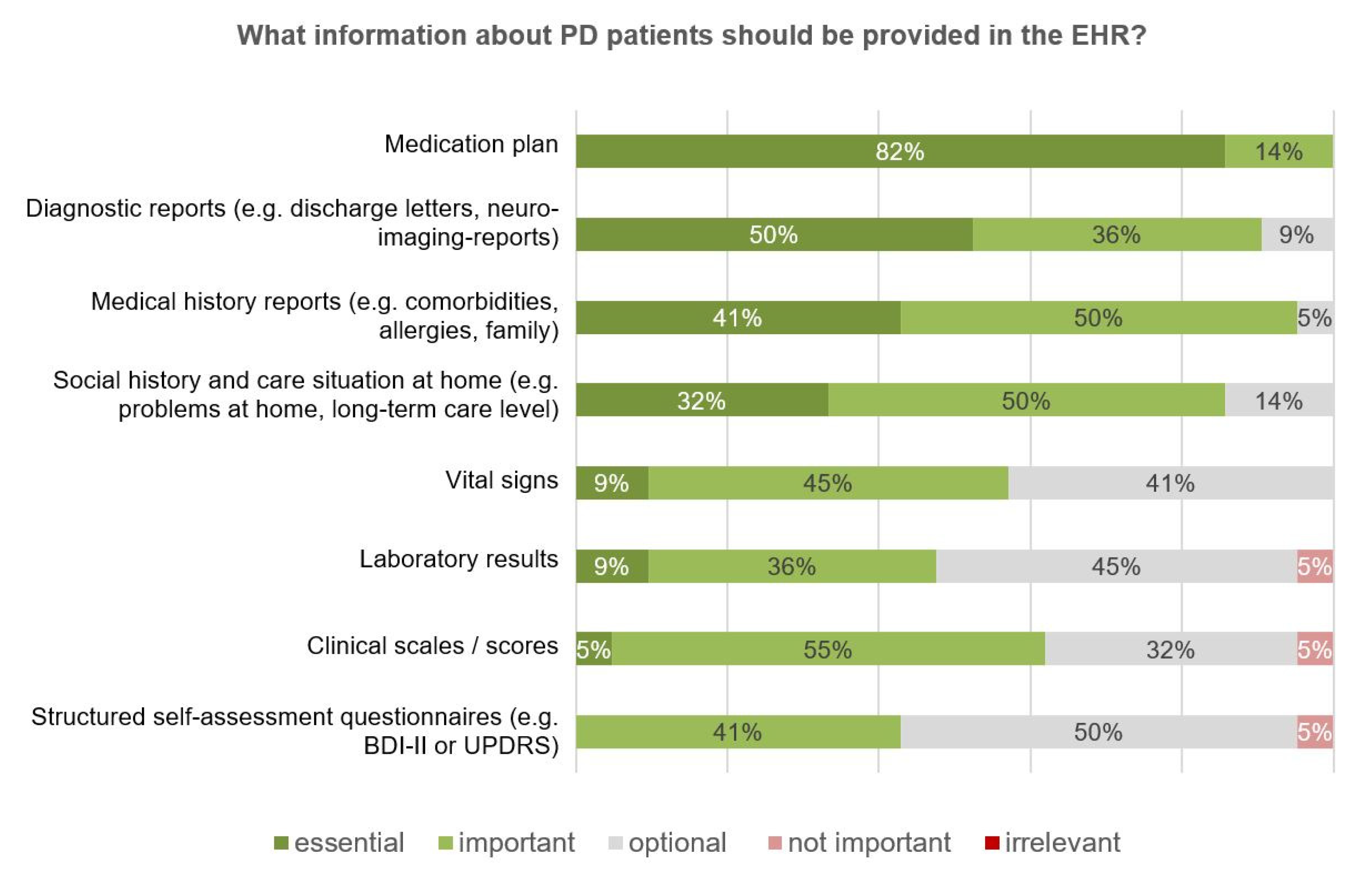
The relevance of different medical information to be provided in the EHR was assessed, with the medication plan ranking the highest (
Figure 5). Despite the overall acceptance of the concept of repetitive monitoring, the provision of the respective results had the lowest priority of all the medical information assessed.
All contributing community-based physicians will actively use the EHR as the basis for standardized care and documentation (
Table 5, EHR 1–4).
Largely corresponding to those health-related dimensions where the availability of information was valued as the most meaningful (
Figure 4), community-based physicians were also expected to actively contribute to their collection (
Table 5, EHR 5–14). In line with this, a contribution of community-based physicians was consented in functional domains (
Table 5, EHR 5–9), in contrast to the contribution in psychosocial domains (
Table 5, EHR 11, 14). An exception was the information about QoL, valued as the second highest relevance (
Figure 4), but where a contribution to information collection by community-based physicians was not consented (
Table 5, EHR 12, 13). The assessment of QoL was rather regarded as a responsibility of case managers.
Repetitive quantitative data, e.g., scores from self-assessments tools, should be visualized as a color-coded heatmap (
Table 5, EHR 16) and should be customizable, e.g., by (de-) selecting scores (
Table 5, EHR 15).
There was a clear preference for closed selection fields over semi- or unstructured open text fields for documentation (
Table 5, EHR 21, 19, 20).
- 2.
Intersectoral specialized case management (ICM)
Case managers are pivotal for PANOS as they hold the major linkage between the outpatient sector and Parkinson centers. The team of case managers will represent the personal backbone of PANOS with an array of core responsibilities (
Table 6, ICM 1–7,
Table 4, MON 3):
To be the long-term one-spot contact person for individually assigned patients and for all of their healthcare providers;
To perform patient home consultations and home-based social assessments;
To assure the structured availability of required clinical information with a special focus on the repetitive patient self-monitoring;
To assure timely reactions of Parkinson centers in case of relevant changes in the monitoring results;
To plan and execute measurements for the active network management;
To execute the patient education program after adequate training (train-the-trainer principle);
To execute continuous quality control according to the quality management concept (see below).
Case managers will be prepared in a modular training program before taking up the above-mentioned diverse tasks. In order to support community-based physicians in their work in PANOS, services can be requested from case management (
Table 6, ICM 6).
- 3.
Active network management (ANM)
Mobilization and motivation of community-based physicians is not only an essential prerequisite to assure an equal and timely access of eligible patients, but also for the collaborative concept of an intersectoral care provision partnership.
This will be addressed by several strategies including: the structured acquisition of participants due to personal on-site consultations; releasing information updates about the network status; organization of educational symposiums; project discussion groups; topic-specific workgroups; stakeholder meetings and regional quality circles (
Table 7, ANM 1, 5, 6). No consensus could be achieved on an adequate frequency of plenary meetings.
- 4.
Structured patient education program according to self-management concept (EDU)
Structured patient education is deemed as an essential core measure within PANOS. It not only gives PD patients self-management education the highest priority when asked about expectations in the context of ICCs [
15,
17], but also deems expert panels self-management education measures as indispensable for healthcare delivery to chronic long-term conditions [
21].
This especially holds true for concepts such as PANOS, where patients are assigned an active role in their own care. The more empowered patients are to do this, the better the chance that they can become a meaningful active contributor to their own care [
22].
The self-management concept implies that PD-related knowledge is only one of several skills a patient has to master in order to induce and maintain health-promoting self-management behaviors. Developing beliefs regarding a sufficient self-efficacy as a core mediator for self-management behaviors, as well as additional skills such as action planning or adequate resource utilization, are indispensable for this [
23].
Generally, a multi-modular, small-group, in-class setting is used for implementation. Informal caregivers are mostly included, since most patients rely on them in order to perform self-management behaviors successfully [
24].
In Sweden, a sustainable nationwide implementation of a structured program for PD patients according to the self-management concept has been achieved in the recent years, including some evidence for its efficacy [
25,
26]. In order to allow for a timely implementation within PANOS, the concept of the Swedish National Parkinson School will be adopted together with the Swedish program initiators.
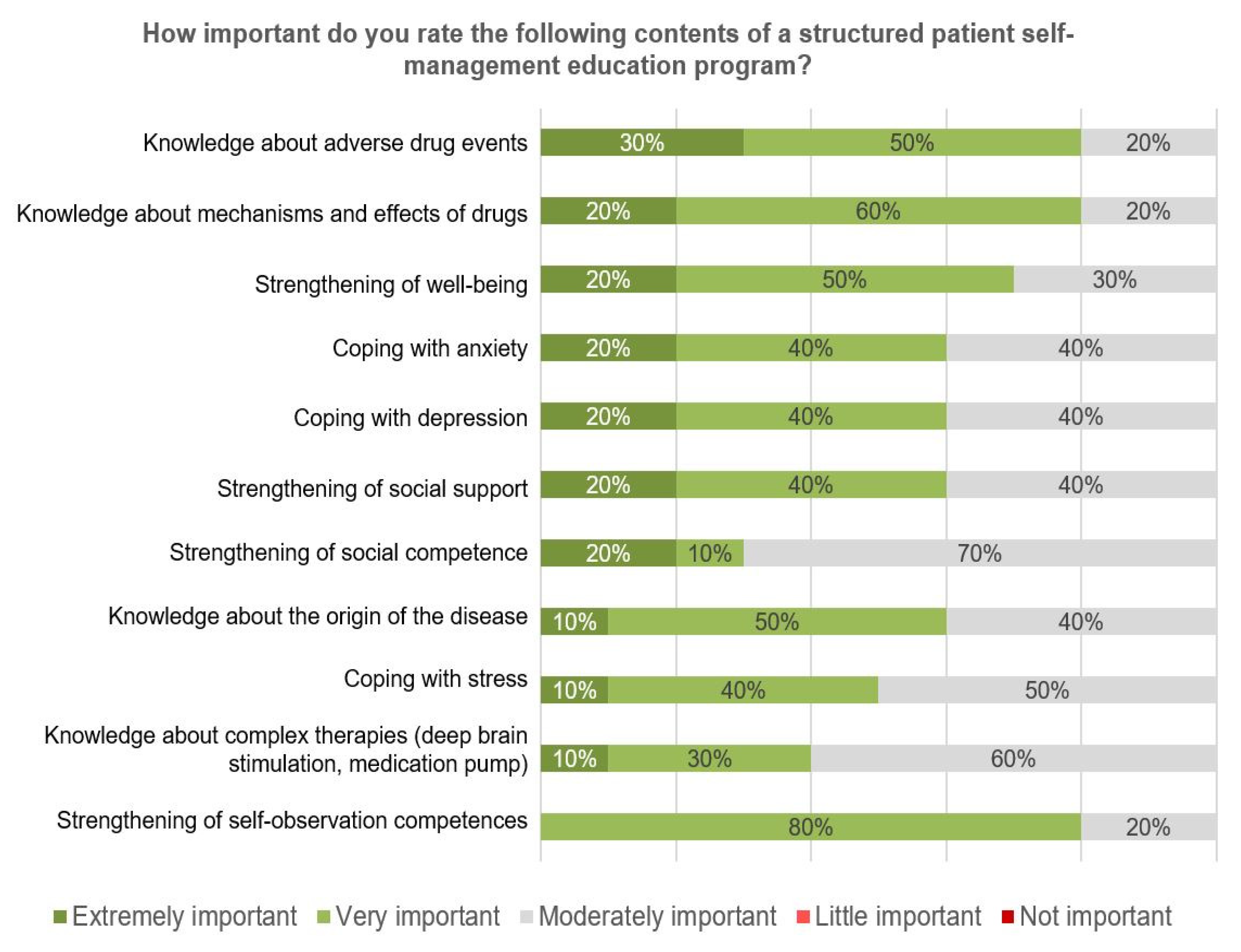
Participants were asked to rate the importance of potential curriculum topics. The highest relevance was given to a knowledge domain (adverse drug events), followed by self-management behaviors such as coping with emotional impact (
Figure 6).
Both the general concept of a structured program according to the self-management concept and several knowledge domains were consented (
Table 8, EDU 1–7).
Patients and caregivers will be provided with patient letters in lay language about clinical and treatment statuses and the care plan. Patient letters will be created automatically based on data recorded in the EHR using preset text modules, tested for patient-orientated comprehensibility.
- 5.
Structured professional education curriculum
Both community-based neurologists and GPs are an integral part of PANOS. To enable participating physicians to perform their tasks in patient selection and in participating in ongoing care, a structured education curriculum for all professional care providers will be established. The physician education curriculum is to focus on both the timely recognition of patients in the transition phase and in need of specialized care, as well as on the knowledge and skills needed to become a productive active long-term collaborator. Given the special importance of GPs in care provision to PD patients in Eastern Saxony, an education module is planned to specifically target the needs of GPs (“PD for GPs”).


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}