How Accurate Is Oral Implant Installation Using Surgical Guides Printed from a Degradable and Steam-Sterilized Biopolymer?

 ,
,  ,
,
Abstract
1. Introduction
2. Experimental Section
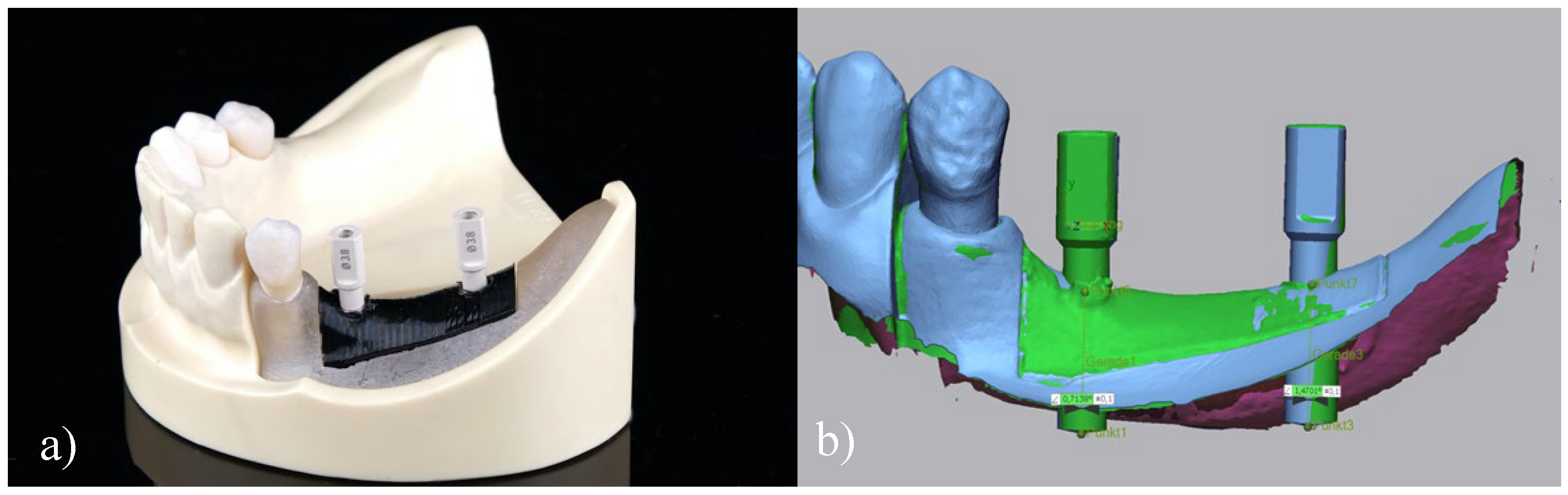
2.1. Reference Model
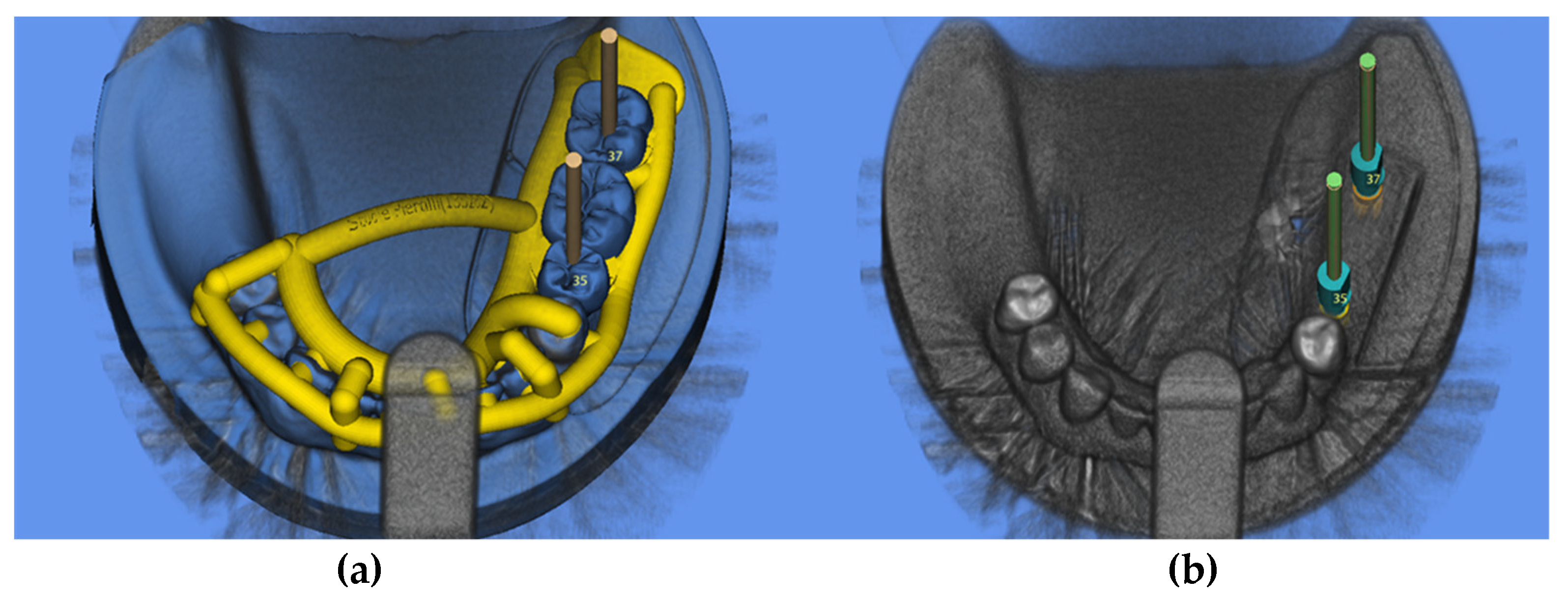
2.2. Digital Implant Planning
2.3. 3D Printing of Surgical Guides
2.4. Surgical Protocol
2.5. Data Acquisition
2.6. Statistical Analysis
3. Results
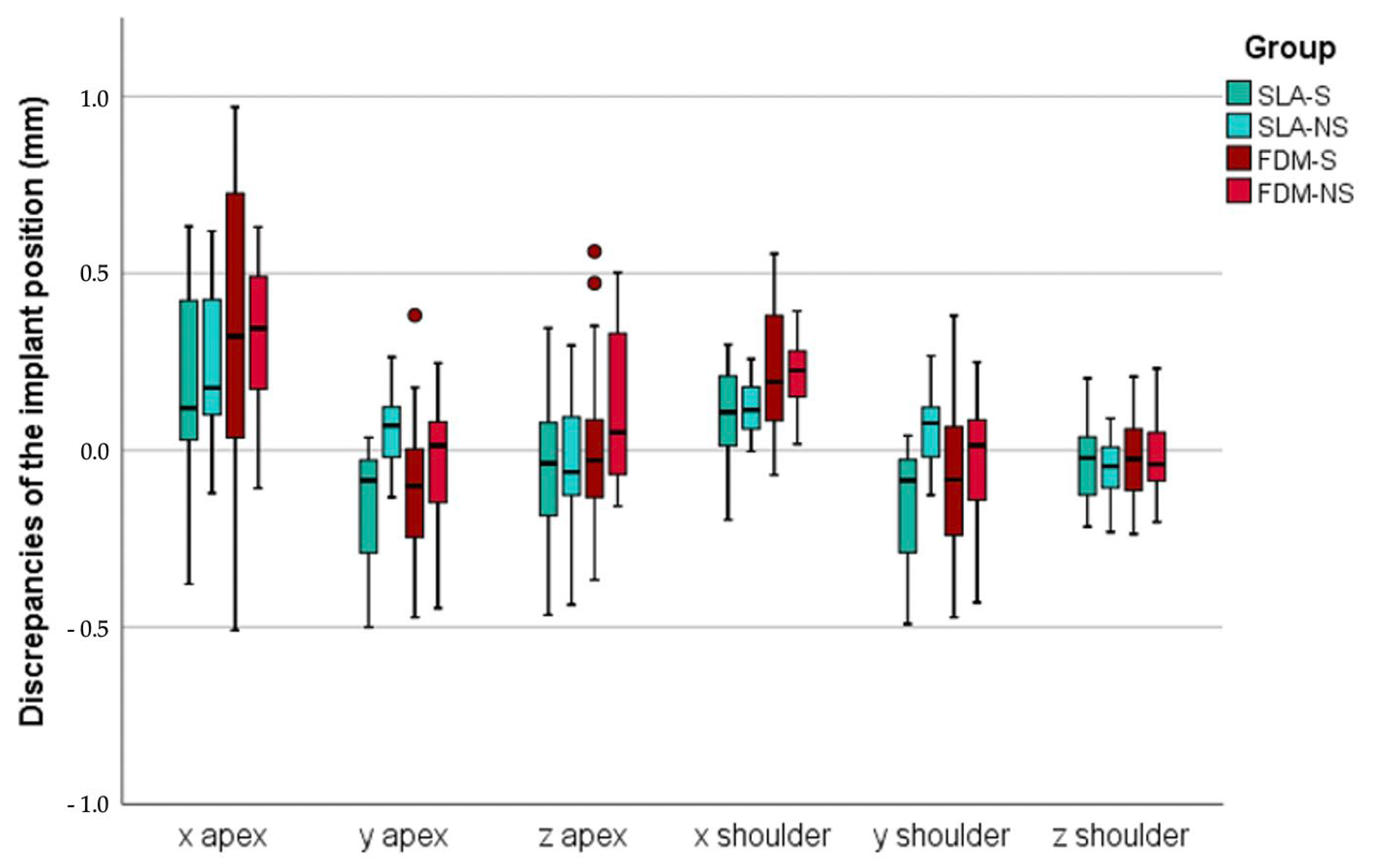
3.1. Sagittal Discrepancies (X)
3.2. Transversal Discrepancies (Y)
3.3. Vertical Deviations (z)
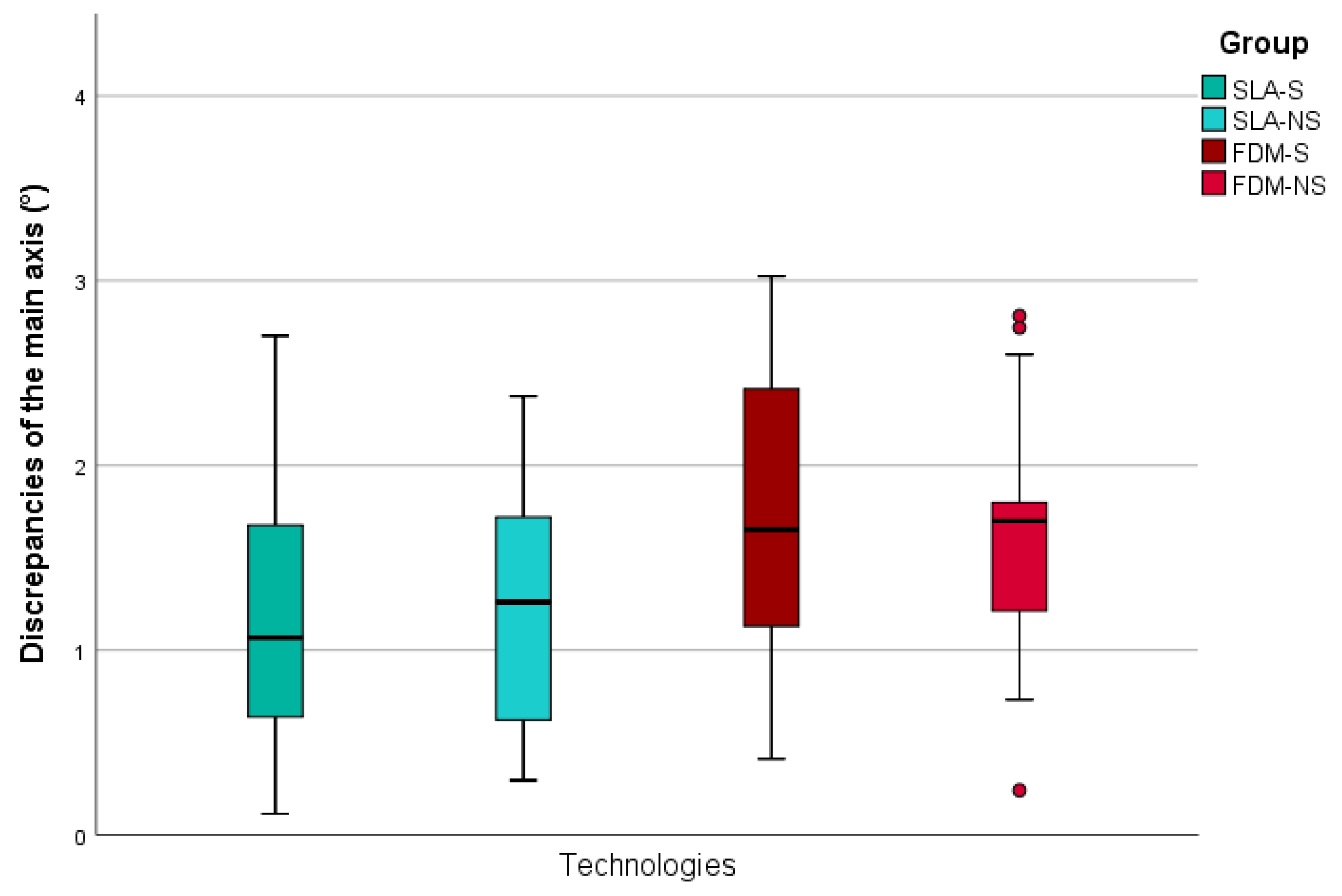
3.4. Main Axis Deviations
4. Discussion
5. Conclusions
- -
- Implant placement using FDM and SLA printed surgical guides resulted in comparable accuracy of implant position.
- -
- Both investigated implant positions (SP, SM) showed comparable deviations.
- -
- The use of metal sleeves for surgical guides did not improve the final accuracy of the implant position.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rabel, K.; Spies, B.C.; Pieralli, S.; Vach, K.; Kohal, R.J. The clinical performance of all-ceramic implant-supported single crowns: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29 (Suppl. 18), 196–223. [Google Scholar] [CrossRef] [PubMed]
- Pieralli, S.; Kohal, R.J.; Rabel, K.; von Stein-Lausnitz, M.; Vach, K.; Spies, B.C. Clinical outcomes of partial and full-arch all-ceramic implant-supported fixed dental prostheses. A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29 (Suppl. 18), 224–236. [Google Scholar] [CrossRef]
- De Kok, I.J.; Duqum, I.S.; Katz, L.H.; Cooper, L.F. Management of Implant/Prosthodontic Complications. Dent. Clin. North. Am. 2019, 63, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Buser, D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla—A systematic review. Int. J. Oral Maxillofac. Implants 2014, 29 (Suppl. g3.3), 186–215. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Tallarico, M.; Radovanovic, S.; Delibasic, B.; Covani, U.; Rakic, M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered peri-implantitis. Clin. Oral Implants Res. 2016, 27, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Burkhardt, F.; Strietzel, F.P.; Bitter, K.; Spies, B.C. Guided implant surgery for one-piece ceramic implants: A digital workflow. Int. J. Comput. Dent. 2020, 23, 73–82. [Google Scholar]
- Pozzi, A.; Polizzi, G.; Moy, P.K. Guided surgery with tooth-supported templates for single missing teeth: A critical review. Eur. J. Oral Implantol. 2016, 9 (Suppl. 1), S135–S153. [Google Scholar]
- Flugge, T.; Derksen, W.; Te Poel, J.; Hassan, B.; Nelson, K.; Wismeijer, D. Registration of cone beam computed tomography data and intraoral surface scans—A prerequisite for guided implant surgery with CAD/CAM drilling guides. Clin. Oral Implants Res. 2017, 28, 1113–1118. [Google Scholar] [CrossRef]
- Pieralli, S.; Gintaute, A.; Beuer, F.; Spies, B.C. Digital and Orthodontically Driven Implant Planning: A Multidisciplinary Case History Report. Int. J. Prosthodont 2019, 32, 214–216. [Google Scholar] [CrossRef]
- Bencharit, S.; Staffen, A.; Yeung, M.; Whitley, D., 3rd; Laskin, D.M.; Deeb, G.R. In Vivo Tooth-Supported Implant Surgical Guides Fabricated With Desktop Stereolithographic Printers: Fully Guided Surgery Is More Accurate Than Partially Guided Surgery. J. Oral Maxillofac. Surg. 2018, 76, 1431–1439. [Google Scholar] [CrossRef]
- Henprasert, P.; Dawson, D.V.; El-Kerdani, T.; Song, X.; Couso-Queiruga, E.; Holloway, J.A. Comparison of the Accuracy of Implant Position Using Surgical Guides Fabricated by Additive and Subtractive Techniques. J. Prosthodont. 2020. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Altieri, F.; Giansanti, M.; Bellardini, M.; Brandetti, G.; Piccoli, L. Is there a learning curve in static computer-assisted implant surgery? A prospective clinical study. Int. J. Oral Maxillofac. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Aimar, A.; Palermo, A.; Innocenti, B. The Role of 3D Printing in Medical Applications: A State of the Art. J. Healthc. Eng. 2019, 2019, 5340616. [Google Scholar] [CrossRef] [PubMed]
- Revilla-Leon, M.; Sadeghpour, M.; Ozcan, M. An update on applications of 3D printing technologies used for processing polymers used in implant dentistry. Odontology 2019. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Altieri, F.; Di Giorgio, R.; Barbato, E. Palatal orthodontic miniscrew insertion using a CAD-CAM surgical guide: Description of a technique. Int. J. Oral Maxillofac. Surg. 2018, 47, 1195–1198. [Google Scholar] [CrossRef]
- Patzelt, S.B.; Bishti, S.; Stampf, S.; Att, W. Accuracy of computer-aided design/computer-aided manufacturing-generated dental casts based on intraoral scanner data. J. Am. Dent. Assoc. 2014, 145, 1133–1140. [Google Scholar] [CrossRef]
- Quan, H.; Zhang, T.; Xu, H.; Luo, S.; Nie, J.; Zhu, X. Photo-curing 3D printing technique and its challenges. Bioact. Mater. 2020, 5, 110–115. [Google Scholar] [CrossRef]
- Tallarico, M.; Kim, Y.J.; Cocchi, F.; Martinolli, M.; Meloni, S.M. Accuracy of newly developed sleeve-designed templates for insertion of dental implants: A prospective multicenters clinical trial. Clin. Implant. Dent. Relat Res. 2019, 21, 108–113. [Google Scholar] [CrossRef]
- Rungrojwittayakul, O.; Kan, J.Y.; Shiozaki, K.; Swamidass, R.S.; Goodacre, B.J.; Goodacre, C.J.; Lozada, J.L. Accuracy of 3D Printed Models Created by Two Technologies of Printers with Different Designs of Model Base. J. Prosthodont. 2020, 29, 124–128. [Google Scholar] [CrossRef]
- Kiendl, J.; Gao, C. Controlling toughness and strength of FDM 3D-printed PLA components through the raster layup. Compos. Part B Eng. 2019, 180. [Google Scholar] [CrossRef]
- Mazzanti, V.; Malagutti, L.; Mollica, F. FDM 3D Printing of Polymers Containing Natural Fillers: A Review of their Mechanical Properties. Polymers 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Ngo, T.; Kashani, A.; Imbalzano, G.; Nguyen, K.; Hui, D. Additive manufacturing (3D printing): A review of materials, methods, applications and challenges. Compos. Part B Eng. 2018, 143. [Google Scholar] [CrossRef]
- Li, H.; Wang, T.; Sun, J.; Yu, Z. The effect of process parameters in fused deposition modelling on bonding degree and mechanical properties. Rapid Prototyp. J. 2018, 24, 80–92. [Google Scholar] [CrossRef]
- Giammona, G.; Craparo, E.F. Biomedical Applications of Polylactide (PLA) and Its Copolymers. Molecules 2018, 23, 980. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Presta, R.; Lupi, S.M.; Giarratana, N.; Bloise, N.; Benedetti, L.; Cusella De Angelis, M.G.; Rodriguez, Y.B.R. Evaluation of Poly(Lactic-co-glycolic) Acid Alone or in Combination with Hydroxyapatite on Human-Periosteal Cells Bone Differentiation and in Sinus Lift Treatment. Molecules 2017, 22, 2109. [Google Scholar] [CrossRef]
- Oledzka, E.; Pachowska, D.; Orlowska, K.; Kolmas, J.; Drobniewska, A.; Figat, R.; Sobczak, M. Pamidronate-Conjugated Biodegradable Branched Copolyester Carriers: Synthesis and Characterization. Molecules 2017, 22, 1063. [Google Scholar] [CrossRef]
- Lekholm, U.; Zarb, G.A. Patient selection and preparation. In Tissue Integrated Prostheses: Osseointegration in Clinical Dentistry; Quintessence Publishing Co.: Chicago, IL, USA, 1985; pp. 199–209. [Google Scholar]
- Herschdorfer, L.; Negreiros, W.M.; Gallucci, G.O.; Hamilton, A. Comparison of the accuracy of implants placed with CAD-CAM surgical templates manufactured with various 3D printers: An in vitro study. J. Prosthet Dent. 2020. [Google Scholar] [CrossRef]
- Skjerven, H.; Riis, U.H.; Herlofsson, B.B.; Ellingsen, J.E. In Vivo Accuracy of Implant Placement Using a Full Digital Planning Modality and Stereolithographic Guides. Int. J. Oral Maxillofac. Implants 2019, 34, 124–132. [Google Scholar] [CrossRef]
- Derksen, W.; Wismeijer, D.; Flugge, T.; Hassan, B.; Tahmaseb, A. The accuracy of computer-guided implant surgery with tooth-supported, digitally designed drill guides based on CBCT and intraoral scanning. A prospective cohort study. Clin. Oral Implants Res. 2019, 30, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Younes, F.; Cosyn, J.; De Bruyckere, T.; Cleymaet, R.; Bouckaert, E.; Eghbali, A. A randomized controlled study on the accuracy of free-handed, pilot-drill guided and fully guided implant surgery in partially edentulous patients. J. Clin. Periodontol. 2018, 45, 721–732. [Google Scholar] [CrossRef]
- Skjerven, H.; Olsen-Bergem, H.; Ronold, H.J.; Riis, U.H.; Ellingsen, J.E. Comparison of postoperative intraoral scan versus cone beam computerised tomography to measure accuracy of guided implant placement-A prospective clinical study. Clin. Oral Implants Res. 2019, 30, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Kurt, B.R. Template guided surgery with the open-access software “smop”. Swiss Dent. J. 2014, 124, 305–323. [Google Scholar] [PubMed]
- Schnutenhaus, S.; Groller, S.; Luthardt, R.G.; Rudolph, H. Accuracy of the match between cone beam computed tomography and model scan data in template-guided implant planning: A prospective controlled clinical study. Clin. Implant. Dent. Relat Res. 2018, 20, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Kernen, F.; Benic, G.I.; Payer, M.; Schar, A.; Muller-Gerbl, M.; Filippi, A.; Kuhl, S. Accuracy of Three-Dimensional Printed Templates for Guided Implant Placement Based on Matching a Surface Scan with CBCT. Clin. Implant. Dent. Relat Res. 2016, 18, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Behneke, A.; Burwinkel, M.; Behneke, N. Factors influencing transfer accuracy of cone beam CT-derived template-based implant placement. Clin. Oral Implants Res. 2012, 23, 416–423. [Google Scholar] [CrossRef]
- Schnutenhaus, S.; Edelmann, C.; Rudolph, H.; Dreyhaupt, J.; Luthardt, R.G. 3D accuracy of implant positions in template-guided implant placement as a function of the remaining teeth and the surgical procedure: A retrospective study. Clin. Oral Investig. 2018, 22, 2363–2372. [Google Scholar] [CrossRef]
- Cassetta, M.; Di Mambro, A.; Giansanti, M.; Stefanelli, L.V.; Cavallini, C. The intrinsic error of a stereolithographic surgical template in implant guided surgery. Int. J. Oral Maxillofac. Surg. 2013, 42, 264–275. [Google Scholar] [CrossRef]
- Laederach, V.; Mukaddam, K.; Payer, M.; Filippi, A.; Kuhl, S. Deviations of different systems for guided implant surgery. Clin. Oral Implants Res. 2017, 28, 1147–1151. [Google Scholar] [CrossRef]
- Kim, Y.; Ju, S.; Kim, M.; Park, M.; Jun, S.; Ahn, J. Direct Measurement of Heat Produced during Drilling for Implant Site Preparation. Appl. Sci. 2019, 9, 1898. [Google Scholar] [CrossRef]
- Van der Cruyssen, F.; Vasconcelos, K.; Verhelst, P.-J.; Shujaat, S.; Delsupehe, A.-M.; Hauben, E.; Orhan, K.; Politis, C.; Jacobs, R. Metal debris after dental implant placement: A proof-of-concept study in fresh frozen cadavers using MRI and histological analysis. Int. J. Oral Implantol. 2019, 12, 349–356. [Google Scholar]
- Fretwurst, T.; Nelson, K.; Tarnow, D.P.; Wang, H.-L.; Giannobile, W.V. Is Metal Particle Release Associated with Peri-implant Bone Destruction? An Emerging Concept. J. Dental Res. 2018, 97, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Schnutenhaus, S.; von Koenigsmarck, V.; Blender, S.; Ambrosius, L.; Luthardt, R.G.; Rudolph, H. Precision of sleeveless 3D drill guides for insertion of one-piece ceramic implants: A prospective clinical trial. Int. J. Comput. Dent. 2018, 21, 97–105. [Google Scholar] [PubMed]
- Martone, P.T.; Estevez, J.M.; Lu, F.; Ruel, K.; Denny, M.W.; Somerville, C.; Ralph, J. Discovery of Lignin in Seaweed Reveals Convergent Evolution of Cell-Wall Architecture. Curr. Biol. 2009, 19, 169–175. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Position | Technology | Guidance | Apex (mm) | Shoulder (mm) | Axis (°) | ||||
|---|---|---|---|---|---|---|---|---|---|
| x | y | z | x | y | z | ||||
| 35 | SLA | S | 0.3 ± 0.2 | −0.2 ± 0.2 | −0.1 ± 0.2 | 0.1 ± 0.1 | −0.2 ± 0.2 | −0.1 ± 0.1 | 1.3 ± 0.9 |
| NS | 0.3 ± 0.2 | 0.1 ± 0.1 | −0.1 ± 0.2 | 0.1 ± 0.1 | 0.1 ± 0.1 | −0.1 ± 0.1 | 1.6 ± 0.5 | ||
| FDM | S | 0.2 ± 0.4 | −0.3 ± 0.1 | 0.1 ± 0.3 | 0.1 ± 0.2 | −0.3 ± 0.1 | 0 ± 0.1 | 1.9 ± 0.8 | |
| NS | 0.3 ± 0.2 | −0.1 ± 0.2 | 0.2 ± 0.3 | 0.2 ± 0.1 | −0.1 ± 0.2 | 0 ± 0,1 | 1.9 ± 0.8 | ||
| 37 | SLA | S | 0.1 ± 0.3 | −0.1 ± 0.1 | 0.0 ± 0.2 | 0.1 ± 0.1 | −0.1 ± 0.1 | 0.0 ± 0,1 | 1.2 ± 0.6 |
| NS | 0.1 ± 0.2 | 0.0 ± 0.1 | 0.0 ± 0.2 | 0.1± 0.1 | −0.1 ± 0.1 | 0.0 ± 0,1 | 0.8 ± 0.5 | ||
| FDM | S | 0.4 ± 0.4 | 0.0 ± 0.2 | −0.1 ± 0.1 | 0.3 ± 0.1 | 0.1 ± 0.2 | 0.0 ± 0.1 | 1.7 ± 0.9 | |
| NS | 0.3 ± 0.2 | 0.1 ± 0.1 | 0.1 ± 0.2 | 0.2 ± 0.1 | 0.1 ± 0.1 | 0.0 ± 0,1 | 1.3 ± 0.4 | ||
| MANOVA | Position | Multiple Comparisons | Tukey Test | |||
|---|---|---|---|---|---|---|
| Significance | Group (A) | Group (B) | Significance | |||
| Apex | x | 0.050 | ||||
| y | 0.001 | 35 | SLA-NS | SLA-S | 0.001 | |
| FDM-S | 0.001 | |||||
| FDM-NS | 0.045 | |||||
| z | 0.054 | |||||
| Shoulder | x | 0.001 | 37 | SLA-S | FDM-S | 0.001 |
| FDM-NS | 0.017 | |||||
| SLA-NS | FDM-S | 0.001 | ||||
| FDM-NS | 0.033 | |||||
| y | 0.001 | 35 | SLA-NS | SLA-S | 0.001 | |
| FDM-S | 0.001 | |||||
| 37 | SLA-S | FDM-NS | 0.035 | |||
| z | 0.352 | |||||
| Axis | 0.033 | 37 | SLA-NS | FDM-S | 0.020 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pieralli, S.; Spies, B.C.; Hromadnik, V.; Nicic, R.; Beuer, F.; Wesemann, C. How Accurate Is Oral Implant Installation Using Surgical Guides Printed from a Degradable and Steam-Sterilized Biopolymer? J. Clin. Med. 2020, 9, 2322. https://doi.org/10.3390/jcm9082322
Pieralli S, Spies BC, Hromadnik V, Nicic R, Beuer F, Wesemann C. How Accurate Is Oral Implant Installation Using Surgical Guides Printed from a Degradable and Steam-Sterilized Biopolymer? Journal of Clinical Medicine. 2020; 9(8):2322. https://doi.org/10.3390/jcm9082322
Chicago/Turabian StylePieralli, Stefano, Benedikt Christopher Spies, Valentin Hromadnik, Robert Nicic, Florian Beuer, and Christian Wesemann. 2020. "How Accurate Is Oral Implant Installation Using Surgical Guides Printed from a Degradable and Steam-Sterilized Biopolymer?" Journal of Clinical Medicine 9, no. 8: 2322. https://doi.org/10.3390/jcm9082322
APA StylePieralli, S., Spies, B. C., Hromadnik, V., Nicic, R., Beuer, F., & Wesemann, C. (2020). How Accurate Is Oral Implant Installation Using Surgical Guides Printed from a Degradable and Steam-Sterilized Biopolymer? Journal of Clinical Medicine, 9(8), 2322. https://doi.org/10.3390/jcm9082322