Rate of Change in Bruch’s Membrane Opening-Minimum Rim Width and Peripapillary RNFL in Early Normal Tension Glaucoma


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Optical Coherence Tomography
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
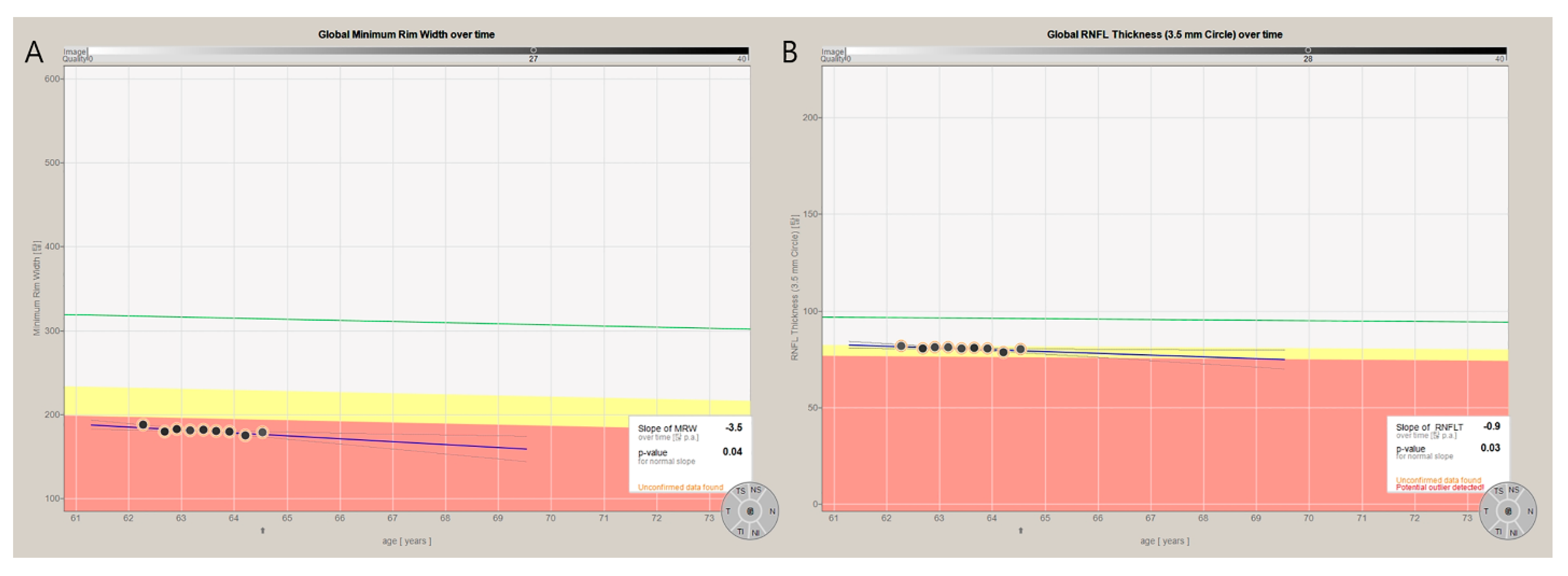
3.2. Baseline BMO-MRW and RNFL and the Rate of Change for Each Parameter
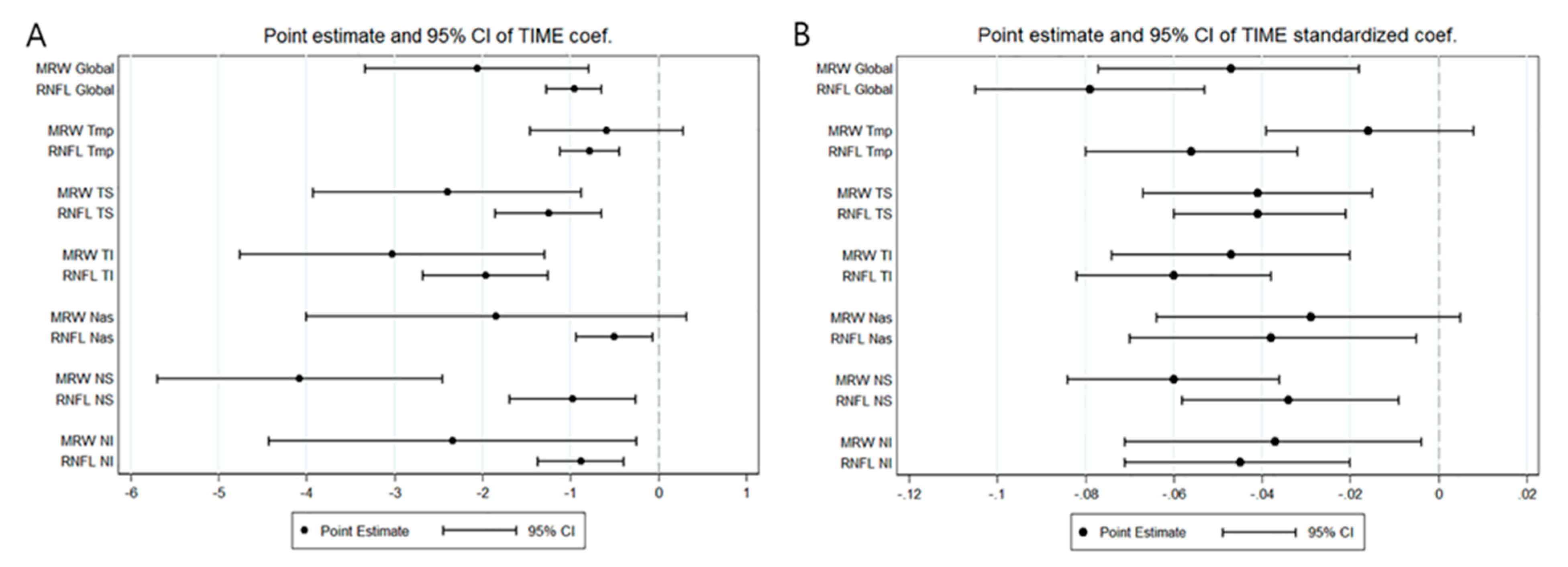
3.3. Comparison of the Rate of Change between BMO-MRW and RNFL
3.4. Comparison of the Rate of Change in Percent Reduction between BMO-MRW and RNFL
3.5. Comparison of Rate of Change in BMO-MRW and RNFL after Standardization
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Weinreb, R.N.; Khaw, P.T. Primary open-angle glaucoma. Lancet 2004, 363, 1711–1720. [Google Scholar] [CrossRef]
- Sommer, A.; Miller, N.R.; Pollack, I.; Maumenee, A.E.; George, T. The nerve fiber layer in the diagnosis of glaucoma. Arch. Ophthalmol. 1977, 95, 2149–2156. [Google Scholar] [CrossRef]
- Malik, R.; Swanson, W.H.; Garway-Heath, D.F. Structure-function relationship’ in glaucoma: Past thinking and current concepts. Clin. Exp. Ophthalmol. 2012, 40, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Keltner, J.L.; Johnson, C.A.; Anderson, D.R.; Levine, R.A.; Fan, J.; Cello, K.E.; Quigley, H.A.; Budenz, D.L.; Parrish, R.K.; Kass, M.A.; et al. The association between glaucomatous visual fields and optic nerve head features in the Ocular Hypertension Treatment Study. Ophthalmology 2006, 113, 1603–1612. [Google Scholar] [CrossRef] [PubMed]
- Hood, D.C.; Kardon, R.H. A framework for comparing structural and functional measures of glaucomatous damage. Prog. Retin. Eye Res. 2007, 26, 688–710. [Google Scholar] [CrossRef] [PubMed]
- Strouthidis, N.G.; Fortune, B.; Yang, H.; Sigal, I.A.; Burgoyne, C.F. Longitudinal change detected by spectral domain optical coherence tomography in the optic nerve head and peripapillary retina in experimental glaucoma. Invest. Ophthalmol. Vis. Sci. 2011, 52, 1206–1219. [Google Scholar] [CrossRef]
- Chauhan, B.C.; Danthurebandara, V.M.; Sharpe, G.P.; Demirel, S.; Girkin, C.A.; Mardin, C.Y.; Scheuerle, A.F.; Burgoyne, C.F. Bruch’s Membrane Opening Minimum Rim Width and Retinal Nerve Fiber Layer Thickness in a Normal White Population: A Multicenter Study. Ophthalmology 2015, 122, 1786–1794. [Google Scholar] [CrossRef]
- Chauhan, B.C.; O’Leary, N.; AlMobarak, F.A.; Reis, A.S.C.; Yang, H.; Sharpe, G.P.; Hutchison, D.M.; Nicolela, M.T.; Burgoyne, C.F. Enhanced detection of open-angle glaucoma with an anatomically accurate optical coherence tomography-derived neuroretinal rim parameter. Ophthalmology 2013, 120, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, K.; Gosho, M.; Zako, M. Correlation between optic nerve head structural parameters and glaucomatous visual field indices. Clin. Ophthalmol. 2014, 8, 1203–1208. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pollet-Villard, F.; Chiquet, C.; Romanet, J.P.; Noel, C.; Aptel, F. Structure-function relationships with spectral-domain optical coherence tomography retinal nerve fiber layer and optic nerve head measurements. Invest. Ophthalmol. Vis. Sci. 2014, 55, 2953–2962. [Google Scholar] [CrossRef]
- Gardiner, S.K.; Ren, R.; Yang, H.; Fortune, B.; Burgoyne, C.F.; Demirel, S. A method to estimate the amount of neuroretinal rim tissue in glaucoma: Comparison with current methods for measuring rim area. Am. J. Ophthalmol. 2014, 157, 540–549.e1–2. [Google Scholar] [CrossRef] [PubMed]
- Enders, P.; Schaub, F.; Adler, W.; Hermann, M.M.; Dietlein, T.S.; Cursiefen, C.; Heindl, L.M.; Medscape. Bruch’s membrane opening-based optical coherence tomography of the optic nerve head: A useful diagnostic tool to detect glaucoma in macrodiscs. Eye 2018, 32, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Lopes, F.S.; Matsubara, I.; Almeida, I.; Dorairaj, S.K.; Vessani, R.M.; Paranhos, A., Jr.; Prata, T.S. Structure-function relationships in glaucoma using enhanced depth imaging optical coherence tomography-derived parameters: A cross-sectional observational study. BMC Ophthalmol. 2019, 19, 52. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.K.; Kee, C. Characteristics of Patients Showing Discrepancy Between Bruch’s Membrane Opening-Minimum Rim Width and Peripapillary Retinal Nerve Fiber Layer Thickness. J. Clin. Med. 2019, 8, 1362. [Google Scholar] [CrossRef]
- Cho, H.K.; Kee, C. Population-based glaucoma prevalence studies in Asians. Surv. Ophthalmol. 2014, 59, 434–447. [Google Scholar] [CrossRef]
- Kostanyan, T.; Sung, K.R.; Schuman, J.S.; Ling, Y.; Lucy, K.A.; Bilonick, R.A.; Ishikawa, H.; Kagemann, L.; Lee, J.Y.; Wollstein, G. Glaucoma Structural and Functional Progression in American and Korean Cohorts. Ophthalmology 2016, 123, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.Y.; Na, J.K.; Park, C.K. Detecting the progression of normal tension glaucoma: A comparison of perimetry, optic coherence tomography, and Heidelberg retinal tomography. Korean J. Ophthalmol. 2015, 29, 31–39. [Google Scholar] [CrossRef][Green Version]
- Cho, H.K.; Lee, J.; Lee, M.; Kee, C. Initial central scotomas vs peripheral scotomas in normal-tension glaucoma: Clinical characteristics and progression rates. Eye 2014, 28, 303–311. [Google Scholar] [CrossRef]
- Chauhan, B.C.; Burgoyne, C.F. From clinical examination of the optic disc to clinical assessment of the optic nerve head: A paradigm change. Am. J. Ophthalmol. 2013, 156, 218–227. [Google Scholar] [CrossRef]
- Kim, C.S.; Seong, G.J.; Lee, N.H.; Song, K.C.; Namil Study Group, K.G.S. Prevalence of primary open-angle glaucoma in central South Korea the Namil study. Ophthalmology 2011, 118, 1024–1030. [Google Scholar] [CrossRef]
- Kim, E.W.; Park, H.S.; Choi, W.; Lee, K.; Lee, S.Y.; Seong, G.J.; Kim, C.Y.; Bae, H.W. Progression patterns of normal-tension glaucoma groups classified by hierarchical cluster analysis. Eye 2020. [Google Scholar] [CrossRef] [PubMed]
- Vianna, J.R.; Danthurebandara, V.M.; Sharpe, G.P.; Hutchison, D.M.; Belliveau, A.C.; Shuba, L.M.; Nicolela, M.T.; Chauhan, B.C. Importance of Normal Aging in Estimating the Rate of Glaucomatous Neuroretinal Rim and Retinal Nerve Fiber Layer Loss. Ophthalmology 2015, 122, 2392–2398. [Google Scholar] [CrossRef] [PubMed]
- Bowd, C.; Zangwill, L.M.; Weinreb, R.N.; Girkin, C.A.; Fazio, M.A.; Liebmann, J.M.; Belghith, A. Racial Differences in Rate of Change of Spectral-Domain Optical Coherence Tomography-Measured Minimum Rim Width and Retinal Nerve Fiber Layer Thickness. Am. J. Ophthalmol. 2018, 196, 154–164. [Google Scholar] [CrossRef]
- Cho, H.K.; Kee, C. Comparison of Rate of change between Bruch’s Membrane Opening-Minimum Rim Width and RNFL in Eyes showing Optic Disc Hemorrhage. Am. J. Ophthalmol. 2020, 217, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Akagi, T.; Zangwill, L.M.; Saunders, L.J.; Yarmohammadi, A.; Manalastas, P.I.C.; Suh, M.H.; Girkin, C.A.; Liebmann, J.M.; Weinreb, R.N. Rates of Local Retinal Nerve Fiber Layer Thinning before and after Disc Hemorrhage in Glaucoma. Ophthalmology 2017, 124, 1403–1411. [Google Scholar] [CrossRef] [PubMed]
- Kotowski, J.; Wollstein, G.; Ishikawa, H.; Schuman, J.S. Imaging of the optic nerve and retinal nerve fiber layer: An essential part of glaucoma diagnosis and monitoring. Surv. Ophthalmol. 2014, 59, 458–467. [Google Scholar] [CrossRef][Green Version]
- Chen, T.C. Spectral domain optical coherence tomography in glaucoma: Qualitative and quantitative analysis of the optic nerve head and retinal nerve fiber layer (an AOS thesis). Trans. Am. Ophthalmol. Soc. 2009, 107, 254–281. [Google Scholar] [PubMed]
- Povazay, B.; Hofer, B.; Hermann, B.; Unterhuber, A.; Morgan, J.E.; Glittenberg, C.; Binder, S.; Drexler, W. Minimum distance mapping using three-dimensional optical coherence tomography for glaucoma diagnosis. J. Biomed. Opt. 2007, 12, 041204. [Google Scholar] [CrossRef]
- Toshev, A.P.; Lamparter, J.; Pfeiffer, N.; Hoffmann, E.M. Bruch’s Membrane Opening-Minimum Rim Width Assessment with Spectral-Domain Optical Coherence Tomography Performs Better Than Confocal Scanning Laser Ophthalmoscopy in Discriminating Early Glaucoma Patients from Control Subjects. J. Glaucoma 2017, 26, 27–33. [Google Scholar] [CrossRef]
- Reis, A.S.C.; Zangalli, C.E.S.; Abe, R.Y.; Silva, A.L.; Vianna, J.R.; Vasconcellos, J.P.C.; Costa, V.P. Intra- and interobserver reproducibility of Bruch’s membrane opening minimum rim width measurements with spectral domain optical coherence tomography. Acta Ophthalmol. 2017, 95, e548–e555. [Google Scholar] [CrossRef]
- Enders, P.; Bremen, A.; Schaub, F.; Hermann, M.M.; Diestelhorst, M.; Dietlein, T.; Cursiefen, C.; Heindl, L.M. Intraday Repeatability of Bruch’s Membrane Opening-Based Neuroretinal Rim Measurements. Invest. Ophthalmol. Vis. Sci. 2017, 58, 5195–5200. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Kim, J.; Lee, J. Reproducibility of Bruch Membrane Opening-Minimum Rim Width Measurements with Spectral Domain Optical Coherence Tomography. J. Glaucoma 2017, 26, 1041–1050. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Values |
|---|---|
| Number of subjects | 115 eyes (115 subjects) |
| Mean Age (year) | 56.08 ± 10.94 |
| Female gender (%) | 53/115 (46.09%) |
| Family history of glaucoma (%) | 11/115 (9.57%) |
| Disc hemorrhage (%) | 35/115 (30.43%) |
| Mean follow-up period (months) | 20.99 ± 6.99 |
| Mean number of OCT tests | 7.54 ± 2.12 |
| Quality score of RNFL | 29.44 ± 3.53 |
| Quality score of BMO-MRW | 32.38 ± 3.13 |
| FoBMO angle (°) | −6.16 ± 3.17 |
| NTG | 115/115 (100%) |
| Spherical equivalent (D) | −1.69 ± 2.81 |
| CCT (µm) | 540.13 ± 36.76 |
| Baseline IOP (mmHg) | 14.72 ± 2.70 |
| VFI (%) | 93.30 ± 6.40 |
| MD (dB) | −2.73 ± 2.26 |
| PSD (dB) | 4.75 ± 3.02 |
| Outcome | Baseline Value/ Progression Rate | Standard Error | 95% CI | p-Value | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| BMO Area | 2.29 * | 0.54 | |||
| 0.00462 † | 0.004336 | −0.00389 | 0.01313 | 0.287 | |
| BMO-MRW G | 202.12 * | 44.47 | |||
| −2.063 † | 0.649 | −3.338 | −0.788 | 0.0016 | |
| RNFL G | 79.29 * | 12.65 | |||
| −0.956 † | 0.160 | −1.270 | −0.643 | <0.0001 | |
| BMO-MRW T | 158.60 * | 38.28 | |||
| −0.586 † | 0.444 | −1.458 | 0.287 | 0.1878 | |
| RNFL T | 65.10 * | 13.84 | |||
| −0.785 † | 0.173 | −1.124 | −0.447 | <0.0001 | |
| BMO-MRW TS | 202.81 * | 59.34 | |||
| −2.401 † | 0.775 | −3.923 | −0.879 | 0.0020 | |
| RNFL TS | 108.24 * | 29.87 | |||
| −1.250 † | 0.309 | −1.857 | −0.644 | <0.0001 | |
| BMO-MRW TI | 180.54 * | 64.17 | |||
| −3.024 † | 0.882 | −4.756 | −1.292 | 0.0006 | |
| RNFL TI | 92.17 * | 32.91 | |||
| −1.964 † | 0.363 | −2.678 | −1.251 | <0.0001 | |
| BMO-MRW N | 224.29 * | 63.35 | |||
| −1.844 † | 1.100 | −4.004 | 0.317 | 0.0943 | |
| RNFL N | 65.37 * | 15.96 | |||
| −0.502 † | 0.222 | −0.937 | −0.067 | 0.0237 | |
| BMO-MRW NS | 231.50 * | 70.13 | |||
| −4.077 † | 0.826 | −5.699 | −2.455 | <0.0001 | |
| RNFL NS | 95.78 * | 30.30 | |||
| −0.974 † | 0.364 | −1.689 | −0.259 | 0.0076 | |
| BMO-MRW NI | 230.57 * | 59.59 | |||
| −2.340 † | 1.066 | −4.432 | −0.248 | 0.0284 | |
| RNFL NI | 89.54 * | 19.28 | |||
| −0.882 † | 0.251 | −1.375 | −0.390 | 0.0005 | |
| Compare Coefficients by Sector | ||
|---|---|---|
| Sector | Z-Score | p-Value |
| G | −1.6547 | 0.0980 |
| TMP | 0.4185 | 0.6756 |
| TS | −1.3788 | 0.1680 |
| TI | −1.1109 | 0.2666 |
| NAS | −1.1952 | 0.2320 |
| NS | −3.4375 | 0.0006 |
| NI | −1.3317 | 0.1830 |
| Compare Coefficients by Sector (Percent Reduction) | ||||
|---|---|---|---|---|
| Sector | Percent Coefficient, BMO-MRW | Percent Coefficient, RNFL | Z-Score | p-Value |
| G | −1.6394 ± 0.5161 | −1.2006 ± 0.2005 | −0.7926 | 0.4280 |
| T | −0.2576 ± 0.1954 | −1.0468 ± 0.2300 | 2.6150 | 0.0089 |
| TS | −1.7785 ± 0.5743 | −1.1964 ± 0.2954 | −0.9013 | 0.3674 |
| TI | −1.6193 ± 0.4724 | −2.6363 ± 0.4876 | 1.4979 | 0.1342 |
| N | −3.8762 ± 2.3132 | −0.7494 ± 0.3307 | −1.3381 | 0.1809 |
| NS | −2.3742 ± 0.4810 | −1.0316 ± 0.3856 | −2.1780 | 0.0294 |
| NI | −2.4171 ± 1.1006 | −0.9464 ± 0.2690 | −1.2980 | 0.1943 |
| Outcome | Standardized Coefficient | 95% CI | ||
|---|---|---|---|---|
| Lower | Upper | |||
| BMO-MRW G | Intercept (µm) | 0.922 | −0.400 | 2.242 |
| Time (µm/yr) | −0.047 | −0.077 | −0.018 | |
| RNFL G | Intercept (µm) | 0.050 | −1.029 | 1.130 |
| Time (µm/yr) | −0.079 | −0.105 | −0.053 | |
| BMO-MRW T | Intercept (µm) | 2.137 | 1.228 | 3.046 |
| Time (µm/yr) | −0.016 | −0.039 | 0.008 | |
| RNFL T | Intercept (µm) | 0.782 | −0.244 | 1.809 |
| Time (µm/yr) | −0.056 | −0.080 | −0.032 | |
| BMO-MRW TS | Intercept (µm) | 0.605 | −0.560 | 1.769 |
| Time (µm/yr) | −0.041 | −0.067 | −0.015 | |
| RNFL TS | Intercept (µm) | −0.101 | −1.089 | 0.886 |
| Time (µm/yr) | −0.041 | −0.060 | −0.021 | |
| BMO-MRW TI | Intercept (µm) | 1.011 | −0.008 | 2.029 |
| Time (µm/yr) | −0.047 | −0.074 | −0.020 | |
| RNFL TI | Intercept (µm) | −0.442 | −1.459 | 0.576 |
| Time (µm/yr) | −0.060 | −0.082 | −0.038 | |
| BMO-MRW N | Intercept (µm) | 0.484 | −0.959 | 1.927 |
| Time (µm/yr) | −0.029 | −0.064 | 0.005 | |
| RNFL N | Intercept (µm) | 0.046 | −1.077 | 1.168 |
| Time (µm/yr) | −0.038 | −0.070 | −0.005 | |
| BMO-MRW NS | Intercept (µm) | 0.137 | −0.950 | 1.223 |
| Time (µm/yr) | −0.060 | −0.084 | −0.036 | |
| RNFL NS | Intercept (µm) | −0.159 | −1.207 | 0.890 |
| Time (µm/yr) | −0.034 | −0.058 | −0.009 | |
| BMO-MRW NI | Intercept (µm) | −0.034 | −1.245 | 1.177 |
| Time (µm/yr) | −0.037 | −0.071 | −0.004 | |
| RNFL NI | Intercept (µm) | 0.197 | −0.850 | 1.244 |
| Time (µm/yr) | −0.045 | −0.071 | −0.020 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, H.-k.; Kee, C. Rate of Change in Bruch’s Membrane Opening-Minimum Rim Width and Peripapillary RNFL in Early Normal Tension Glaucoma. J. Clin. Med. 2020, 9, 2321. https://doi.org/10.3390/jcm9082321
Cho H-k, Kee C. Rate of Change in Bruch’s Membrane Opening-Minimum Rim Width and Peripapillary RNFL in Early Normal Tension Glaucoma. Journal of Clinical Medicine. 2020; 9(8):2321. https://doi.org/10.3390/jcm9082321
Chicago/Turabian StyleCho, Hyun-kyung, and Changwon Kee. 2020. "Rate of Change in Bruch’s Membrane Opening-Minimum Rim Width and Peripapillary RNFL in Early Normal Tension Glaucoma" Journal of Clinical Medicine 9, no. 8: 2321. https://doi.org/10.3390/jcm9082321
APA StyleCho, H.-k., & Kee, C. (2020). Rate of Change in Bruch’s Membrane Opening-Minimum Rim Width and Peripapillary RNFL in Early Normal Tension Glaucoma. Journal of Clinical Medicine, 9(8), 2321. https://doi.org/10.3390/jcm9082321