Using Whole Breast Ultrasound Tomography to Improve Breast Cancer Risk Assessment: A Novel Risk Factor Based on the Quantitative Tissue Property of Sound Speed





Abstract
1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Identification and Selection of Cases
2.3. Identification and Selection of Controls
2.4. Breast Imaging
2.5. Breast Density Assessment
2.6. Mammography-Defined BD Measures
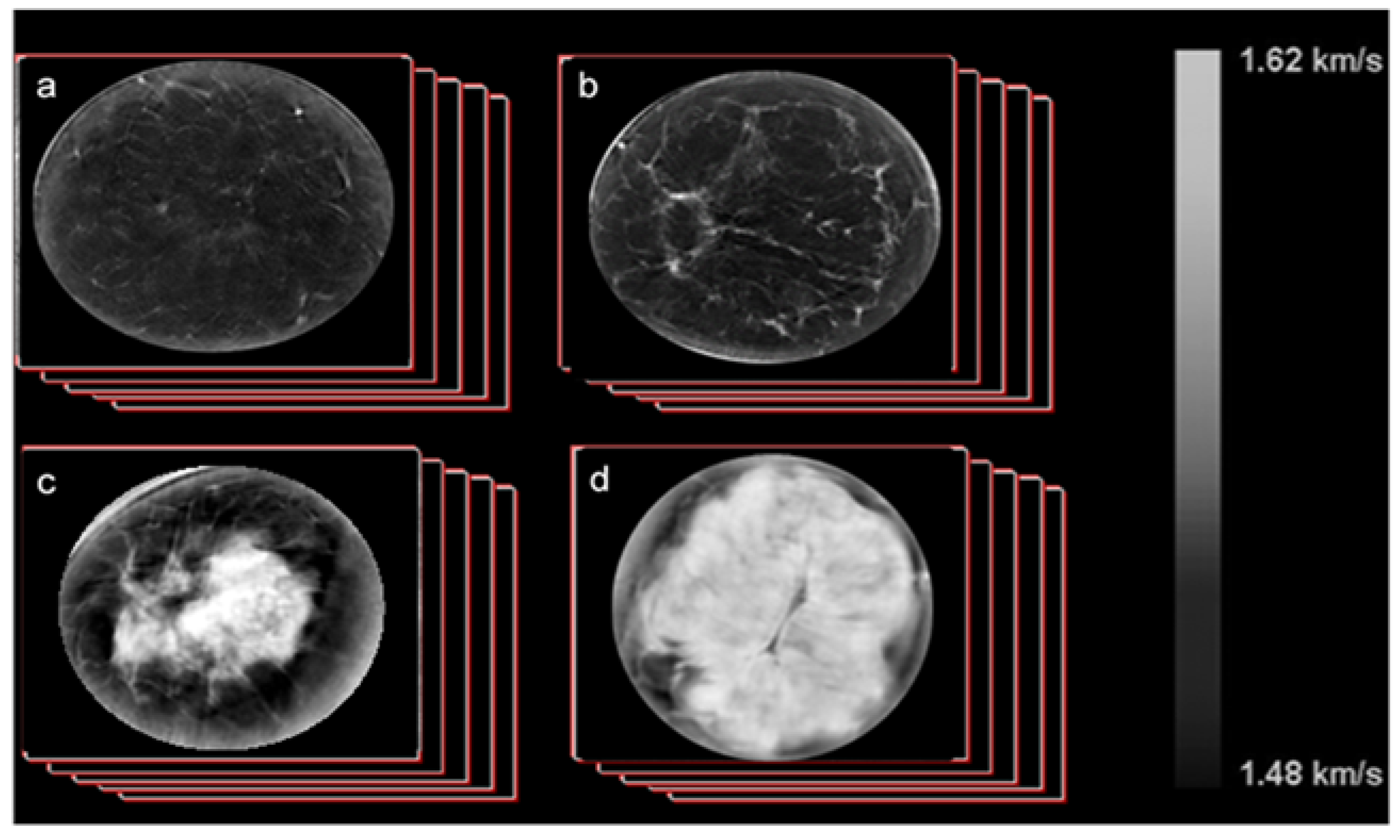
2.7. UST Imaging of Sound Speed
- Calculate the volume of the breast, V, through a direct pixel count using previously developed automated scripts.
- Calculate the volume averaged sound speed (VASS) for each stack by summing up all the pixel values and dividing by the volume determined above using our automated script.
- Apply this calculation to image stacks (approximately from 40 to 100 coronal slices per scan) from all cases and controls.
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics
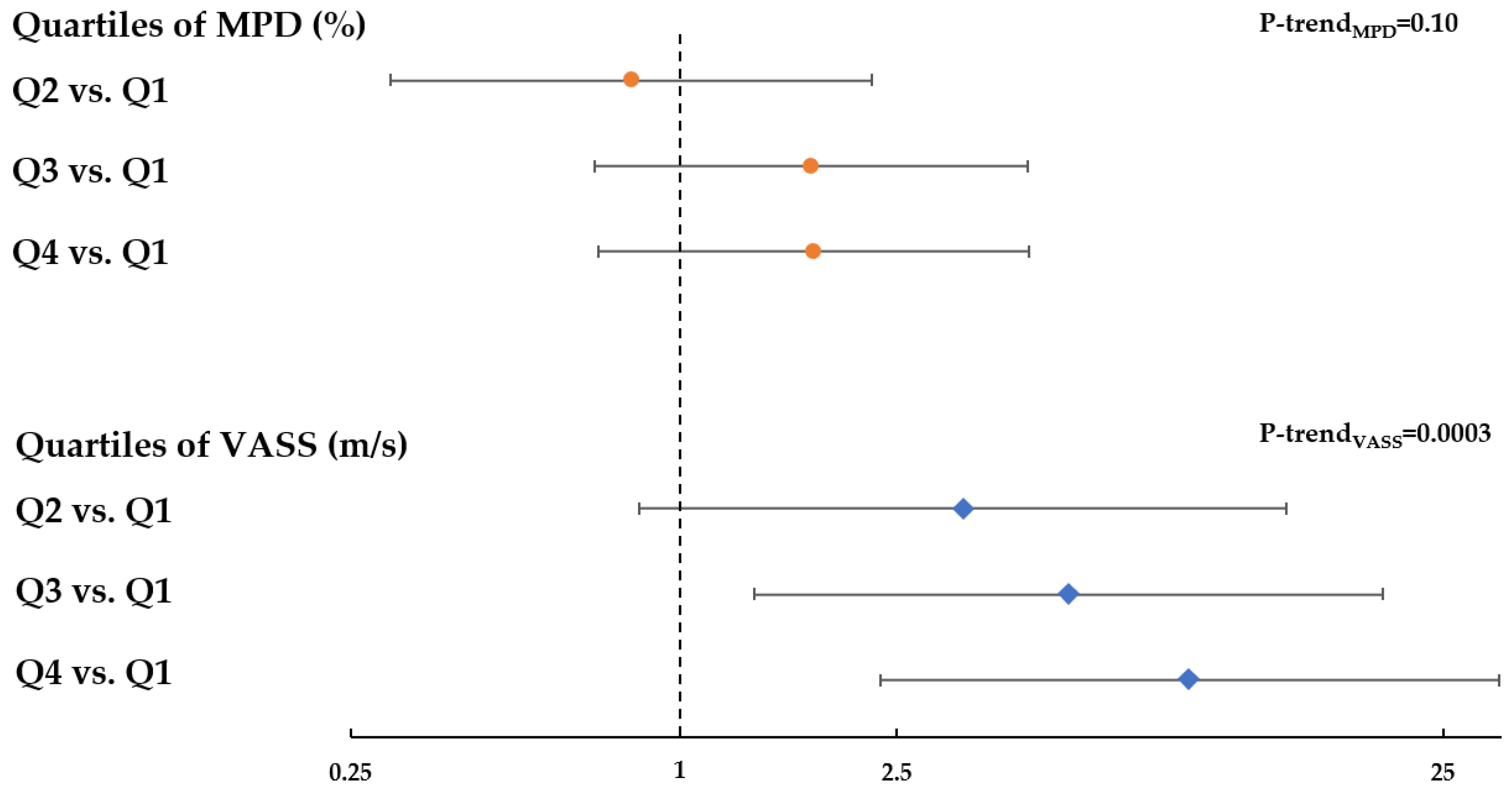
3.2. Relation between Breast Density and Breast Cancer Risk
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sak, M.A.; Littrup, P.J.; Duric, N.; Mullooly, M.; Sherman, M.E.; Gierach, G.L. Current and Future Methods for Measuring Breast Density: A Brief Comparative Review. Breast Cancer Manag. 2015, 4, 209–221. [Google Scholar] [CrossRef]
- Louro, J.; Posso, M.; Hilton Boon, M.; Roman, M.; Domingo, L.; Castells, X.; Sala, M. A systematic review and quality assessment of individualised breast cancer risk prediction models. Br. J. of Cancer 2019, 121, 76–85. [Google Scholar] [CrossRef]
- Kerlikowske, K.; Sprague, B.L.; Tosteson, A.N.A.; Wernli, K.J.; Rauscher, G.H.; Johnson, D.; Buist, D.S.M.; Onega, T.; Henderson, L.M.; O’Meara, E.S.; et al. Strategies to Identify Women at High Risk of Advanced Breast Cancer During Routine Screening for Discussion of Supplemental Imaging. JAMA Intern. Med. 2019, 179, 1230–1239. [Google Scholar] [CrossRef]
- Choudhury, P.P.; Wilcox, A.N.; Brook, M.N.; Zhang, Y.; Ahearn, T.; Orr, N.; Coulson, P.; Schoemaker, M.J.; Jones, M.E.; Gail, M.H.; et al. Comparative validation of breast cancer risk prediction models and projections for future risk stratification. J. Natl. Cancer Inst. 2019, djz113. [Google Scholar] [CrossRef]
- Boyd, N.; Martin, L.; Gunasekara, A.; Melnichouk, O.; Maudsley, G.; Peressotti, C.; Yaffe, M.; Minkin, S. Mammographic density and breast cancer risk: evaluation of a novel method of measuring breast tissue volumes. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1754–1762. [Google Scholar] [CrossRef]
- Yaffe, M.J.; Boone, J.M.; Packard, N.; Alonzo-Proulx, O.; Huang, S.Y.; Peressotti, C.L.; Al-Mayah, A.; Brock, K. The myth of the 50-50 breast. Med. Phys. 2009, 36, 5437–5443. [Google Scholar] [CrossRef]
- Boyd, N.; Martin, L.; Chavez, S.; Gunasekara, A.; Salleh, A.; Melnichouk, O.; Yaffe, M.; Friedenreich, C.; Minkin, S.; Bronskill, M. Breast-tissue composition and other risk factors for breast cancer in young women: a cross-sectional study. Lancet Oncol. 2009, 10, 569–580. [Google Scholar] [CrossRef]
- Yaffe, M.J.; Mainprize, J.G. Risk of radiation-induced breast cancer from mammographic screening. Radiology 2011, 258, 98–105. [Google Scholar] [CrossRef]
- Berrington de Gonzalez, A.; Berg, C.D.; Visvanathan, K.; Robson, M. Estimated risk of radiation-induced breast cancer from mammographic screening for young BRCA mutation carriers. J. Natl. Cancer Inst. 2009, 101, 205–209. [Google Scholar] [CrossRef]
- Wang, J.; Azziz, A.; Fan, B.; Malkov, S.; Klifa, C.; Newitt, D.; Yitta, S.; Hylton, N.; Kerlikowske, K.; Shepherd, J.A. Agreement of mammographic measures of volumetric breast density to MRI. PLoS ONE 2013, 8, e81653. [Google Scholar] [CrossRef]
- Tagliafico, A.; Tagliafico, G.; Astengo, D.; Airaldi, S.; Calabrese, M.; Houssami, N. Comparative estimation of percentage breast tissue density for digital mammography, digital breast tomosynthesis, and magnetic resonance imaging. Breast Cancer Res. Treat. 2013, 138, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Tagliafico, A.; Bignotti, B.; Tagliafico, G.; Astengo, D.; Martino, L.; Airaldi, S.; Signori, A.; Sormani, M.P.; Houssami, N.; Calabrese, M. Breast density assessment using a 3T MRI system: comparison among different sequences. PLoS ONE 2014, 9, e99027. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Weiss, W.A.; Medved, M.; Abe, H.; Newstead, G.M.; Karczmar, G.S.; Giger, M.L. Breast density estimation from high spectral and spatial resolution MRI. J. Med. Imaging (Bellingham, Wash.) 2016, 3, 044507. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Stopeck, A.T.; Gao, Y.; Marron, M.T.; Wertheim, B.C.; Altbach, M.I.; Galons, J.P.; Roe, D.J.; Wang, F.; Maskarinec, G.; et al. Reproducible automated breast density measure with no ionizing radiation using fat-water decomposition MRI. J. Magn. Reson. Imaging JMRI 2018, 48, 971–981. [Google Scholar] [CrossRef]
- Bakker, M.F.; de Lange, S.V.; Pijnappel, R.M.; Mann, R.M.; Peeters, P.H.M.; Monninkhof, E.M.; Emaus, M.J.; Loo, C.E.; Bisschops, R.H.C.; Lobbes, M.B.I.; et al. Supplemental MRI Screening for Women with Extremely Dense Breast Tissue. N. Engl. J. Med. 2019, 381, 2091–2102. [Google Scholar] [CrossRef]
- Nayeem, F.; Ju, H.; Brunder, D.G.; Nagamani, M.; Anderson, K.E.; Khamapirad, T.; Lu, L.J. Similarity of fibroglandular breast tissue content measured from magnetic resonance and mammographic images and by a mathematical algorithm. Int. J. Breast Cancer 2014, 2014, 961679. [Google Scholar] [CrossRef]
- Chang, D.H.; Chen, J.H.; Lin, M.; Bahri, S.; Yu, H.J.; Mehta, R.S.; Nie, K.; Hsiang, D.J.; Nalcioglu, O.; Su, M.Y. Comparison of breast density measured on MR images acquired using fat-suppressed versus nonfat-suppressed sequences. Med. Phys. 2011, 38, 5961–5968. [Google Scholar] [CrossRef]
- Ledger, A.E.; Scurr, E.D.; Hughes, J.; Macdonald, A.; Wallace, T.; Thomas, K.; Wilson, R.; Leach, M.O.; Schmidt, M.A. Comparison of Dixon Sequences for Estimation of Percent Breast Fibroglandular Tissue. PLoS ONE 2016, 11, e0152152. [Google Scholar] [CrossRef]
- Gierach, G.L.; Choudhury, P.P.; Garcia-Closas, M. Toward Risk-Stratified Breast Cancer Screening: Considerations for Changes in Screening Guidelines. JAMA Oncol. 2019. [Google Scholar] [CrossRef]
- Glide, C.; Duric, N.; Littrup, P. Novel approach to evaluating breast density utilizing ultrasound tomography. Med. Phys. 2007, 34, 744–753. [Google Scholar] [CrossRef]
- Glide-Hurst, C.K.; Duric, N.; Littrup, P. Volumetric breast density evaluation from ultrasound tomography images. Med. Phys. 2008, 35, 3988–3997. [Google Scholar] [CrossRef] [PubMed]
- Duric, N.; Littrup, P.; Poulo, L.; Babkin, A.; Pevzner, R.; Holsapple, E.; Rama, O.; Glide, C. Detection of breast cancer with ultrasound tomography: first results with the Computed Ultrasound Risk Evaluation (CURE) prototype. Med. Phys. 2007, 34, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Manning, M.A.; Duric, N.; Littrup, P.; Bey-Knight, L.; Penner, L.; Albrecht, T.L. Knowledge of breast density and awareness of related breast cancer risk. J. Cancer Educ. 2013, 28, 270–274. [Google Scholar] [CrossRef]
- Sak, M.; Duric, N.; Littrup, P.; Bey-Knight, L.; Ali, H.; Vallieres, P.; Sherman, M.E.; Gierach, G.L. Using Speed of Sound Imaging to Characterize Breast Density. Ultrasound Med. Biol. 2017, 43, 91–103. [Google Scholar]
- O’Flynn, E.A.M.; Fromageau, J.; Ledger, A.E.; Messa, A.; D’Aquino, A.; Schoemaker, M.J.; Schmidt, M.; Duric, N.; Swerdlow, A.J.; Bamber, J.C. Ultrasound Tomography Evaluation of Breast Density: A Comparison With Noncontrast Magnetic Resonance Imaging. Investig. Radiol. 2017, 52, 343–348. [Google Scholar] [CrossRef]
- Duric, N.; Boyd, N.; Littrup, P.; Sak, M.; Myc, L.; Li, C.; West, E.; Minkin, S.; Martin, L.; Yaffe, M.; et al. Breast density measurements with ultrasound tomography: a comparison with film and digital mammography. Med. Phys. 2013, 40, 013501. [Google Scholar] [CrossRef]
- Boyd, N.F.; Martin, L.J.; Bronskill, M.; Yaffe, M.J.; Duric, N.; Minkin, S. Breast tissue composition and susceptibility to breast cancer. J. Natl. Cancer Inst. 2010, 102, 1224–1237. [Google Scholar] [CrossRef]
- Sak, M.; Duric, N.; Littrup, P. Volumetric Breast Density Comparisons between Waveform UST Sound Speed Imaging and Mammography (Conference Presentation); SPIE: Houston, TX, USA, 2018; Volume 10580. [Google Scholar]
- Khodr, Z.G.; Sak, M.A.; Pfeiffer, R.M.; Duric, N.; Littrup, P.; Bey-Knight, L.; Ali, H.; Vallieres, P.; Sherman, M.E.; Gierach, G.L. Determinants of the reliability of ultrasound tomography sound speed estimates as a surrogate for volumetric breast density. Med. Phys. 2015, 42, 5671–5678. [Google Scholar] [CrossRef]
- Vachon, C.M.; Brandt, K.R.; Ghosh, K.; Scott, C.G.; Maloney, S.D.; Carston, M.J.; Pankratz, V.S.; Sellers, T.A. Mammographic breast density as a general marker of breast cancer risk. Cancer Epidemiol. Biomark. Prev. 2007, 16, 43–49. [Google Scholar] [CrossRef][Green Version]
- Byng, J.W.; Boyd, N.F.; Fishell, E.; Jong, R.A.; Yaffe, M.J. The quantitative analysis of mammographic densities. Phys. Med. Biol. 1994, 39, 1629–1638. [Google Scholar] [CrossRef]
- McCormack, V.A.; dos Santos Silva, I. Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1159–1169. [Google Scholar] [CrossRef] [PubMed]
- Sprague, B.L.; Gangnon, R.E.; Burt, V.; Trentham-Dietz, A.; Hampton, J.M.; Wellman, R.D.; Kerlikowske, K.; Miglioretti, D.L. Prevalence of mammographically dense breasts in the United States. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed]
- Shawky, M.S.; Huo, C.W.; Henderson, M.A.; Redfern, A.; Britt, K.; Thompson, E.W. A review of the influence of mammographic density on breast cancer clinical and pathological phenotype. Breast Cancer Res. Treat. 2019, 177, 251–276. [Google Scholar] [CrossRef] [PubMed]
- Astley, S.M.; Harkness, E.F.; Sergeant, J.C.; Warwick, J.; Stavrinos, P.; Warren, R.; Wilson, M.; Beetles, U.; Gadde, S.; Lim, Y.; et al. A comparison of five methods of measuring mammographic density: a case-control study. Breast Cancer Res 2018, 20, 10. [Google Scholar] [CrossRef] [PubMed]
- Eng, A.; Gallant, Z.; Shepherd, J.; McCormack, V.; Li, J.; Dowsett, M.; Vinnicombe, S.; Allen, S.; dos-Santos-Silva, I. Digital mammographic density and breast cancer risk: a case-control study of six alternative density assessment methods. Breast Cancer Res. 2014, 16, 439. [Google Scholar] [CrossRef]
- Mullooly, M.; Gierach, G.L. The Potential for Mammographic Breast Density Change as a Biosensor of Adjuvant Tamoxifen Therapy Adherence and Response. JNCI Cancer Spectr. 2018, 2, pky072. [Google Scholar] [CrossRef]
- Turney, A. FDA In Brief: FDA advances new scientific framework to promote greater predictability, efficiency in oncology drug development. Available online: https://www.fda.gov/news-events/fda-brief/fda-brief-fda-advances-new-scientific-framework-promote-greater-predictability-efficiency-oncology (accessed on 20 December 2019).




{kind=link}
{kind=link}
{kind=link}
| Volume Averaged Sound Speed (VASS) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Quartile 1: <1440.63 | Quartile 2: 1440.63 to <1445.65 | Quartile 3: 1445.65 to <1452.81 | Quartile 4: ≥1452.81 | ||||||
| Participant Characteristics | N | % | N | % | N | % | N | % | p-Value * |
| Age: Median (range) | 54.2 | (32.7, 67) | 50.9 | (40.7, 67.7) | 49.6 | (35.4, 69.2) | 48.4 | (36.8, 64.8) | 0.03 ** |
| Race | |||||||||
| White | 12 | 30.0 | 11 | 25.6 | 12 | 29.3 | 16 | 39.0 | |
| Black | 27 | 67.5 | 30 | 69.8 | 28 | 68.3 | 24 | 58.5 | 0.91 † |
| Other | 1 | 2.5 | 2 | 4.7 | 1 | 2.4 | 1 | 2.4 | |
| BMI, kg/m2 | |||||||||
| <25 | 3 | 7.5 | 6 | 14.3 | 6 | 14.6 | 21 | 51.2 | <0.0001 |
| 25–30 | 10 | 25.0 | 12 | 28.6 | 12 | 29.3 | 12 | 29.3 | |
| 30+ | 27 | 67.5 | 24 | 57.1 | 23 | 56.1 | 8 | 19.5 | |
| Education | |||||||||
| At most, high school/GED | 14 | 35.0 | 14 | 32.6 | 7 | 17.1 | 11 | 26.8 | 0.54 |
| Some college/postsecondary courses | 11 | 27.5 | 16 | 37.2 | 18 | 43.9 | 14 | 34.2 | |
| College/graduate school | 15 | 37.5 | 13 | 30.2 | 16 | 39.0 | 16 | 39.0 | |
| Age at menarche | |||||||||
| ≤12 | 26 | 66.7 | 27 | 62.8 | 22 | 53.7 | 19 | 46.3 | 0.34 |
| 13 | 9 | 23.1 | 6 | 14.0 | 11 | 26.8 | 12 | 29.3 | |
| 14+ | 4 | 10.3 | 10 | 23.3 | 8 | 19.5 | 10 | 24.4 | |
| Age at first birth | |||||||||
| Nulliparous/≥30 | 13 | 32.5 | 14 | 32.6 | 12 | 29.3 | 15 | 36.5 | 0.92 |
| <30 | 27 | 67.5 | 29 | 67.4 | 29 | 70.7 | 26 | 63.4 | |
| Menopausal status | |||||||||
| Premenopausal | 14 | 35.0 | 22 | 51.2 | 26 | 63.4 | 31 | 75.6 | 0.0019 |
| Postmenopausal | 26 | 65.0 | 21 | 48.8 | 15 | 36.6 | 10 | 24.4 | |
| Any first degree relative with breast cancer | |||||||||
| No | 30 | 75.0 | 32 | 74.4 | 39 | 95.1 | 32 | 78.1 | 0.056 |
| Yes | 10 | 25.0 | 11 | 25.6 | 2 | 4.9 | 9 | 22.0 | |
| BI-RADS breast density | |||||||||
| a (entirely fat) | 20 | 50.0 | 14 | 32.6 | 6 | 14.6 | 1 | 2.4 | <0.0001 |
| b (scattered densities) | 19 | 47.5 | 27 | 62.8 | 26 | 63.4 | 7 | 17.1 | |
| c (heterogeneously dense) | 1 | 2.5 | 2 | 4.7 | 8 | 19.5 | 26 | 63.4 | |
| d (extremely dense) | 0 | 0.0 | 0 | 0.0 | 1 | 2.4 | 7 | 17.1 | |
| Mammographic percent density, quartiles | |||||||||
| <7.8% | 17 | 42.5 | 18 | 41.9 | 6 | 14.6 | 0 | 0.0 | <0.0001 |
| 7.8 to <16.9% | 16 | 40.0 | 12 | 27.9 | 13 | 31.7 | 1 | 2.4 | |
| 16.9 to <30.8% | 7 | 17.5 | 8 | 18.6 | 15 | 36.6 | 10 | 24.4 | |
| ≥30.8% | 0 | 0.0 | 5 | 11.6 | 7 | 17.1 | 30 | 73.2 | |
| Quartile 1: <7.8% | Quartile 2: 7.8% to <16.9% | Quartile 3: 16.9% to <30.8% | Quartile 4: ≥30.8% | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Participant Characteristics | N | % | N | % | N | % | N | % | p-Value * |
| Age: Median (range) | 53.3 | (32.7, 68.5) | 53.6 | (35.4, 69.1) | 50.4 | (30.2,70.8) | 48.5 | (30.5, 64.8) | 0.018 ** |
| Race | |||||||||
| White | 11 | 26.8 | 11 | 26.2 | 14 | 35.0 | 15 | 35.7 | 0.93 † |
| Black | 28 | 68.3 | 30 | 71.4 | 25 | 62.5 | 26 | 61.9 | |
| Other | 2 | 4.9 | 1 | 2.4 | 1 | 2.5 | 1 | 2.4 | |
| BMI, kg/m2 | |||||||||
| <25 | 2 | 5.0 | 4 | 9.5 | 10 | 25.0 | 20 | 47.6 | <0.0001 |
| 25–30 | 9 | 22.5 | 11 | 26.2 | 15 | 37.5 | 11 | 26.2 | |
| 30+ | 29 | 72.5 | 27 | 64.3 | 15 | 37.5 | 11 | 26.2 | |
| Education | |||||||||
| At most, high school/GED | 12 | 29.3 | 15 | 35.7 | 10 | 25.0 | 9 | 21.4 | 0.86 |
| Some college/postsecondary courses | 15 | 36.6 | 13 | 31.0 | 14 | 35.0 | 17 | 40.5 | |
| College/graduate school | 14 | 34.2 | 14 | 33.3 | 16 | 40.0 | 16 | 38.1 | |
| Age at menarche | |||||||||
| ≤12 | 30 | 75.0 | 21 | 50.0 | 21 | 52.5 | 22 | 52.4 | 0.14 |
| 13 | 6 | 15.0 | 14 | 33.3 | 9 | 22.5 | 9 | 21.4 | |
| 14+ | 4 | 10.0 | 7 | 16.7 | 10 | 25.0 | 11 | 26.2 | |
| Age at first birth | |||||||||
| Nulliparous/≥30 | 14 | 34.2 | 15 | 35.7 | 11 | 27.5 | 14 | 33.3 | 0.87 |
| <30 | 27 | 65.9 | 27 | 64.3 | 29 | 72.5 | 28 | 66.7 | |
| Menopausal status | |||||||||
| Premenopausal | 17 | 41.5 | 21 | 50.0 | 26 | 65.0 | 29 | 69.1 | 0.039 |
| Postmenopausal | 24 | 58.5 | 21 | 50.0 | 14 | 35.0 | 13 | 31.0 | |
| Any first degree relative with breast cancer | |||||||||
| No | 32 | 78.1 | 35 | 83.3 | 35 | 87.5 | 31 | 73.8 | 0.42 |
| Yes | 9 | 22.0 | 7 | 16.7 | 5 | 12.5 | 11 | 26.2 | |
| BI-RADS breast density | |||||||||
| a (entirely fat) | 26 | 63.4 | 11 | 26.2 | 3 | 7.5 | 1 | 2.4 | <0.0001 |
| b (scattered densities) | 15 | 36.6 | 28 | 66.7 | 21 | 52.5 | 15 | 35.7 | |
| c (heterogeneously dense) | 0 | 0.0 | 2 | 4.8 | 15 | 37.5 | 20 | 47.6 | |
| d (extremely dense) | 0 | 0.0 | 1 | 2.4 | 1 | 2.5 | 6 | 14.3 | |
| Quartiles of baseline sound speed (m/s) | |||||||||
| <1440.63 | 17 | 41.5 | 16 | 38.1 | 7 | 17.5 | 0 | 0.0 | <0.0001 |
| 1440.63 to <1445.65 | 18 | 43.9 | 12 | 28.6 | 8 | 20.0 | 5 | 11.9 | |
| 1445.65 to <1452.81 | 6 | 14.6 | 13 | 30.9 | 15 | 37.5 | 7 | 16.7 | |
| ≥1452.81 | 0 | 0.0 | 1 | 2.4 | 10 | 25.0 | 30 | 71.4 | |
| Case | Control | |||
|---|---|---|---|---|
| (N = 61) | (N = 165) | |||
| N | % | N | % | |
| Quartiles * of MPD, % | ||||
| <7.8 | 10 | 16.4 | 41 | 24.9 |
| 7.8 to <16.9 | 9 | 14.8 | 42 | 25.5 |
| 16.9 to <30.8 | 20 | 32.8 | 40 | 24.2 |
| ≥30.8 | 22 | 36.1 | 42 | 25.5 |
| Quartiles * of VASS, m/s | ||||
| <1440.6 | 3 | 4.9 | 40 | 24.2 |
| 1440.6 to <1445.6 | 11 | 18 | 43 | 26.1 |
| 1445.6 to <1452.8 | 17 | 27.9 | 41 | 24.9 |
| ≥1452.8 | 30 | 49.2 | 41 | 24.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duric, N.; Sak, M.; Fan, S.; Pfeiffer, R.M.; Littrup, P.J.; Simon, M.S.; Gorski, D.H.; Ali, H.; Purrington, K.S.; Brem, R.F.; et al. Using Whole Breast Ultrasound Tomography to Improve Breast Cancer Risk Assessment: A Novel Risk Factor Based on the Quantitative Tissue Property of Sound Speed. J. Clin. Med. 2020, 9, 367. https://doi.org/10.3390/jcm9020367
Duric N, Sak M, Fan S, Pfeiffer RM, Littrup PJ, Simon MS, Gorski DH, Ali H, Purrington KS, Brem RF, et al. Using Whole Breast Ultrasound Tomography to Improve Breast Cancer Risk Assessment: A Novel Risk Factor Based on the Quantitative Tissue Property of Sound Speed. Journal of Clinical Medicine. 2020; 9(2):367. https://doi.org/10.3390/jcm9020367
Chicago/Turabian StyleDuric, Neb, Mark Sak, Shaoqi Fan, Ruth M. Pfeiffer, Peter J. Littrup, Michael S. Simon, David H. Gorski, Haythem Ali, Kristen S. Purrington, Rachel F. Brem, and et al. 2020. "Using Whole Breast Ultrasound Tomography to Improve Breast Cancer Risk Assessment: A Novel Risk Factor Based on the Quantitative Tissue Property of Sound Speed" Journal of Clinical Medicine 9, no. 2: 367. https://doi.org/10.3390/jcm9020367
APA StyleDuric, N., Sak, M., Fan, S., Pfeiffer, R. M., Littrup, P. J., Simon, M. S., Gorski, D. H., Ali, H., Purrington, K. S., Brem, R. F., Sherman, M. E., & Gierach, G. L. (2020). Using Whole Breast Ultrasound Tomography to Improve Breast Cancer Risk Assessment: A Novel Risk Factor Based on the Quantitative Tissue Property of Sound Speed. Journal of Clinical Medicine, 9(2), 367. https://doi.org/10.3390/jcm9020367