Body-Mass-Index Associated Differences in Ortho- and Retronasal Olfactory Function and the Individual Significance of Olfaction in Health and Disease

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Pilot Study and Data Collection
2.2. Olfactory Tests
2.3. Individual Significance of Olfaction
2.4. Statistical Analysis
3. Results
3.1. Pilot Study
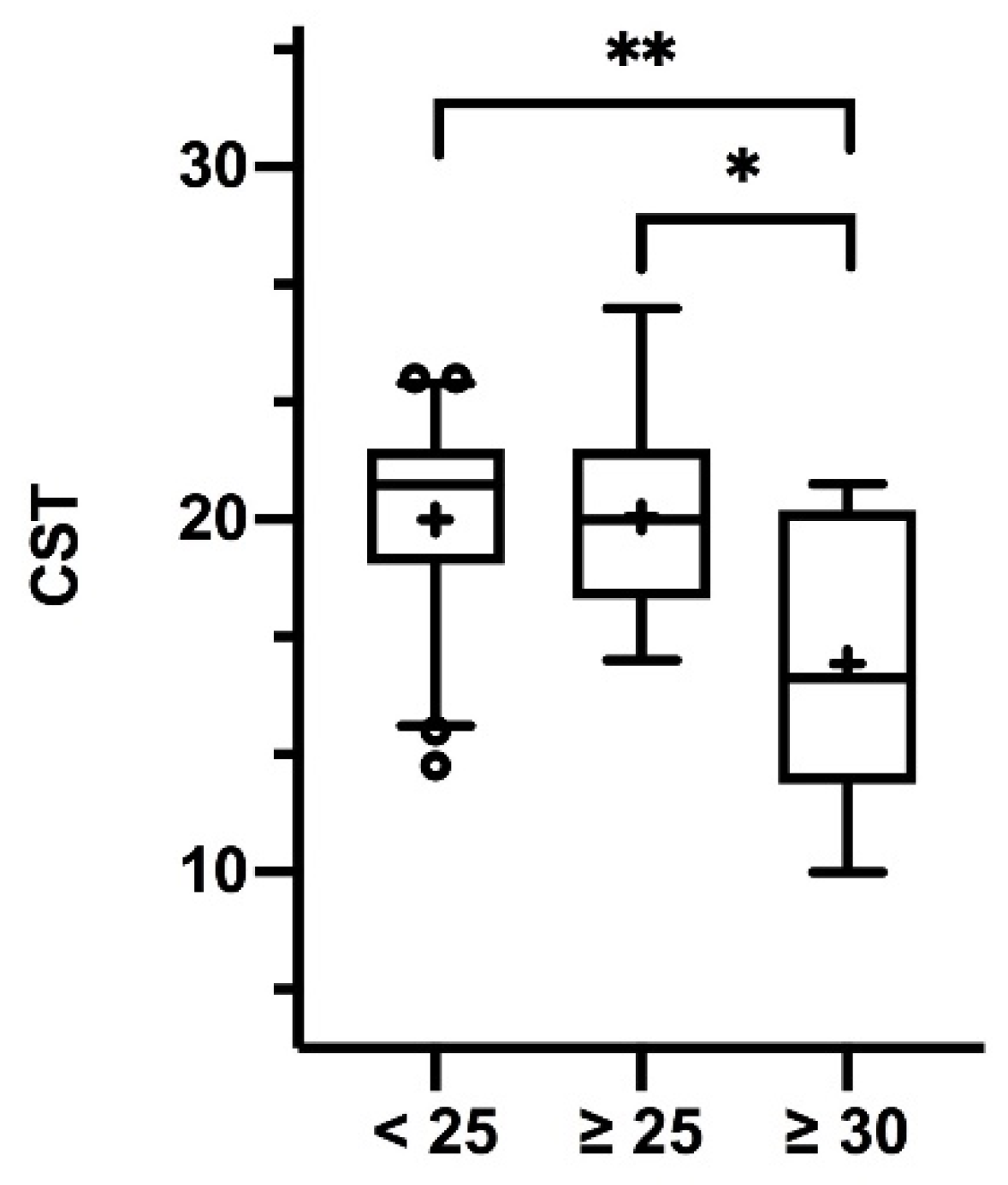
3.2. BMI and Olfaction
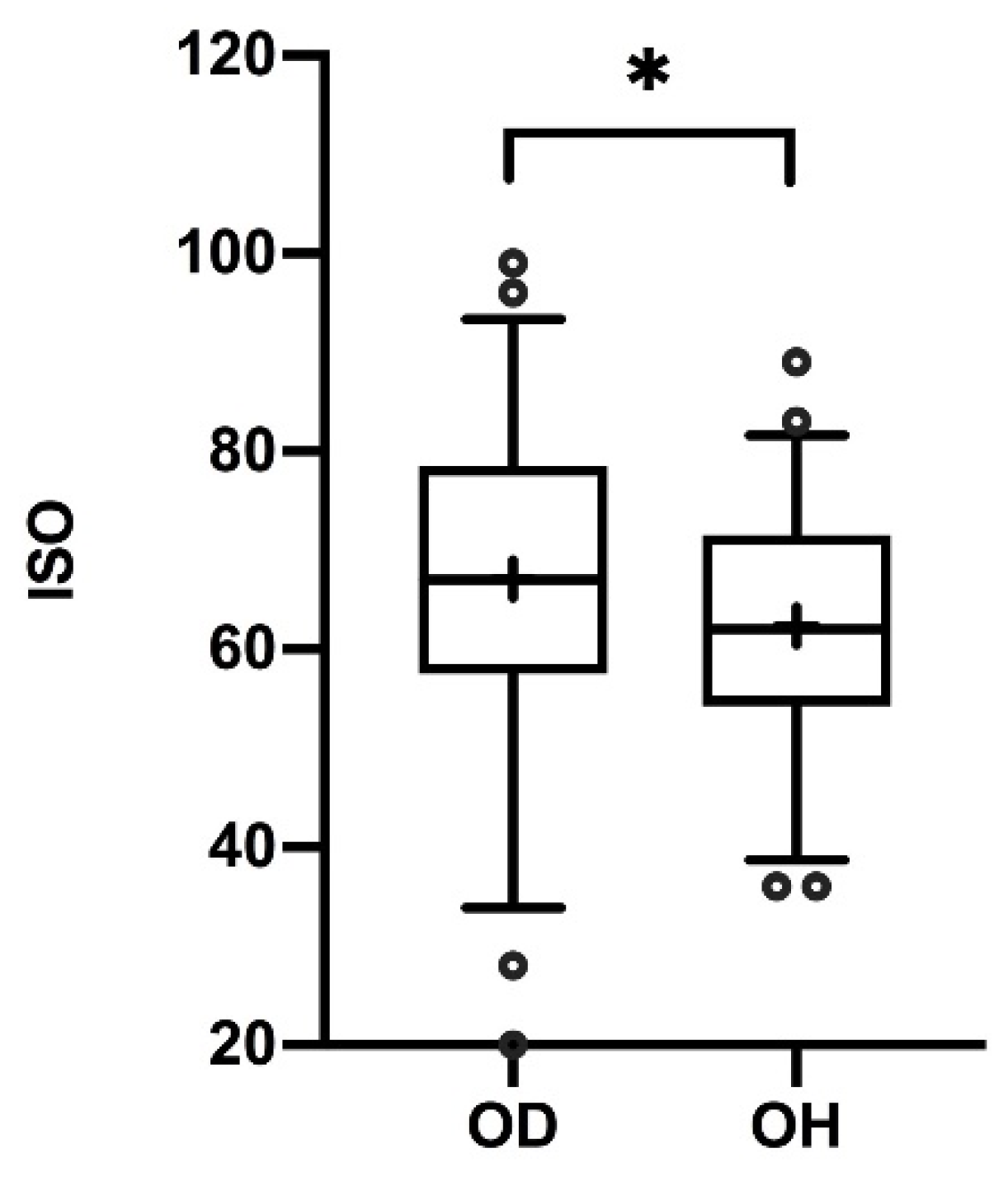
3.3. Individual Significance of Olfaction
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Wang, G.J.; Tomasi, D.; Baler, R.D. Obesity and addiction: Neurobiological overlaps. Obes. Rev. 2013, 14, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Pandit, R.; Mercer, J.G.; Overduin, J.; la Fleur, S.E.; Adan, R.A.H. Dietary factors affect food reward and motivation to eat. Obes. Facts. 2012, 5, 221–242. [Google Scholar] [CrossRef] [PubMed]
- Uygun, B.; Kiyici, S.; Özmen, S.; Gul, Z.; Sigirli, D.; Cavun, S. The Association Between Olfaction and Taste Functions with Serum Ghrelin and Leptin Levels in Obese Women. Metab. Syndr. Relat. Disord. 2019, 17, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Tang, K.; Wu, J.; Xu, H.; Zhang, W.; Cao, T.; Zhou, Y.; Yu, T.; Li, A. Leptin modulates olfactory discrimination and neural activity in the olfactory bulb. Acta. Physiol. (Oxf). 2019, 227, e13319. [Google Scholar] [CrossRef]
- Boesveldt, S.; de Graaf, K. The differential role of smell and taste for eating behavior. Perception 2017, 46, 307–319. [Google Scholar] [CrossRef]
- Riera, C.E.; Tsaousidou, E.; Halloran, J.; Follett, P.; Hahn, O.; Pereira, M.M.A.; Ruud, L.E.; Alber, J.; Tharp, K.; Anderson, C.M.; et al. The sense of smell impacts metabolic health and obesity. Cell Metab. 2017, 26, 198–211. [Google Scholar] [CrossRef]
- Aschenbrenner, K.; Hummel, C.; Teszmer, K.; Krone, F.; Ishimaru, T.; Seo, H.-S.; Hummel, T. The influence of olfactory loss on dietary behaviors. Laryngoscope 2008, 118, 135–144. [Google Scholar] [CrossRef]
- Peng, M.; Coutts, D.; Wang, T.; Cakmak, Y.O. Systematic review of olfactory shifts related to obesity. Obes. Rev. 2019, 20, 325–338. [Google Scholar] [CrossRef]
- Thiebaud, N.; Johnson, M.C.; Butler, J.L.; Bell, G.A.; Ferguson, K.L.; Fadool, A.R.; Fadool, J.C.; Gale, A.M.; Gale, D.S.; Fadool, D.A. Hyperlipidemic diet causes loss of olfactory sensory neurons, reduces olfactory discrimination, and disrupts odor-reversal learning. J. Neurosci. 2014, 34, 6970–6984. [Google Scholar] [CrossRef]
- Royet, J.-P.; Plailly, J.; Saive, A.-L.; Veyrac, A.; Delon-Martin, C. The impact of expertise in olfaction. Front. Psychol. 2013, 4, 928. [Google Scholar] [CrossRef] [PubMed]
- Croy, I.; Buschhüter, D.; Seo, H.-S.; Negoias, S.; Hummel, T. Individual significance of olfaction: Development of a questionnaire. Eur. Arch. Oto-Rino-L. 2009, 267, 67. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.-S.; Guarneros, M.; Hudson, R.; Distel, H.; Min, B.-C.; Kang, J.-K.; Croy, I.; Vodicka, J.; Hummel, T. Attitudes toward olfaction: A cross-regional study. Chem. Senses. 2011, 36, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Hancı, D.; Altun, H.; Altun, H.; Batman, B.; Karip, A.B.; Serin, K.R. Laparoscopic sleeve gastrectomy improves olfaction sensitivity in morbidly obese patients. Obes. Surg. 2016, 26, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Besser, G.; Liu, D.T.; Prem, B.; Iabloncsik, D.; Pablik, E.; Mueller, C.A.; Renner, B. Retronasal olfactory testing using candies sent by post and for screening purposes: A feasibility study. Rhinology 2020. accepted. [Google Scholar]
- Müller, M.J.; Braun, W.; Enderle, J.; Bosy-Westphal, A. Beyond BMI: Conceptual Issues Related to Overweight and Obese Patients. Obes. Facts. 2016, 9, 193–205. [Google Scholar] [CrossRef]
- Oleszkiewicz, A.; Schriever, V.A.; Croy, I.; Hähner, A.; Hummel, T. Updated Sniffin’ Sticks normative data based on an extended sample of 9139 subjects. Eur. Arch. Oto-Rhino-L. 2019, 276, 719–728. [Google Scholar] [CrossRef]
- Kobal, G.; Hummel, T.; Sekinger, B.; Barz, S.; Roscher, S.; Wolf, S. ″Sniffin’ sticks″: screening of olfactory performance. Rhinology 1996, 34, 222–226. [Google Scholar]
- Kobal, G.; Klimek, L.; Wolfensberger, M.; Gudziol, H.; Temmel, A.; Owen, C.M.; Seeber, H.; Pauli, E.; Hummel, T. Multicenter investigation of 1036 subjects using a standardized method for the assessment of olfactory function combining tests of odor identification, odor discrimination, and olfactory thresholds. Eur. Arch. Oto-Rhino-L. 2000, 257, 205–211. [Google Scholar] [CrossRef]
- Hummel, T.; Kobal, G.; Gudziol, H.; Mackay-Sim, A. Normative data for the “Sniffin’ Sticks” including tests of odor identification, odor discrimination, and olfactory thresholds: an upgrade based on a group of more than 3000 subjects. Eur. Arch. Oto-Rrhino-L. 2007, 264, 237–243. [Google Scholar] [CrossRef]
- Renner, B.; Mueller, C.A.; Dreier, J.; Faulhaber, S.; Rascher, W.; Kobal, G. The candy smell test: a new test for retronasal olfactory performance. Laryngoscope 2009, 119, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Haxel, B.R.; Bertz-Duffy, S.; Faldum, A.; Trellakis, S.; Stein, B.; Renner, B.; Kobal, G.; Letzel, S.; Mann, W.J.; Muttray, A. The Candy Smell Test in clinical routine. Am. J. Rhinol. Allergy 2011, 25, 145–148. [Google Scholar] [CrossRef]
- Liu, D.T.; Besser, G.; Renner, B.; Seyferth, S.; Hummel, T.; Mueller, C.A. Retronasal olfactory function in patients with smell loss but subjectively normal flavor perception. Laryngoscope 2019. [Google Scholar] [CrossRef] [PubMed]
- Croy, I.; Angelo, S.D.; Olausson, H. Reduced pleasant touch appraisal in the presence of a disgusting odor. PLoS ONE 2014, 9, e92975. [Google Scholar] [CrossRef] [PubMed]
- Oleszkiewicz, A.; Walliczek-Dworschak, U.; Klötze, P.; Gerber, F.; Croy, I.; Hummel, T. Developmental changes in adolescents’ olfactory performance and significance of olfaction. PLoS ONE 2016, 11, 157560. [Google Scholar] [CrossRef] [PubMed]
- Besser, G.; Liu, D.T.; Renner, B.; Hummel, T.; Mueller, C.A. Olfactory implant: Demand for a future treatment option in patients with olfactory dysfunction. Laryngoscope 2019, 129, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Gudziol, V.; Lötsch, J.R.; Hähner, A.; Zahnert, T.; Hummel, T. Clinical significance of results from olfactory testing. Laryngoscope 2006, 116, 1858–1863. [Google Scholar] [CrossRef]
- Simchen, U.; Koebnick, C.; Hoyer, S.; Issanchou, S.; Zunft, H.-J.F. Odour and taste sensitivity is associated with body weight and extent of misreporting of body weight. Eur. J. Clin. Nutr. 2006, 60, 698–705. [Google Scholar] [CrossRef]
- Patel, Z.M.; DelGaudio, J.M.; Wise, S.K. Research Article Higher Body Mass Index Is Associated with Subjective Olfactory Dysfunction. Behav. Neurol. 2015, 2015, 675635. [Google Scholar] [CrossRef]
- Getchell, T.V.; Kwong, K.; Saunders, C.P.; Stromberg, A.J.; Getchell, M.L. Leptin regulates olfactory-mediated behavior in ob/ob mice. Physiol. Behav. 2006, 87, 848–856. [Google Scholar] [CrossRef]
- Croy, I.; Hoffmann, H.; Philpott, C.; Rombaux, P.; Welge-Luessen, A.; Vodicka, J.; Konstantinidis, I.; Morera, E.; Hummel, T. Retronasal testing of olfactory function: an investigation and comparison in seven countries. Eur. Arch. Oto-Rhino-L. 2014, 271, 1087–1095. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Garcia, J.C.; Alcaide, J.; Santiago-Fernandez, C.; Roca-Rodriguez, M.M.; Agüera, Z.; Baños, R.; Botella, C.; de la Torre, R.; Fernández-Real, J.M.; Frühbeck, G.; et al. An increase in visceral fat is associated with a decrease in the taste and olfactory capacity. PLoS ONE 2017, 12, e0171204. [Google Scholar]
- Soter, A.; Kim, J.; Jackman, A.; Tourbier, I.; Kaul, A.; Doty, R.L. Accuracy of self-report in detecting taste dysfunction. Laryngoscope 2008, 118, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, L.F.; Bennett, L.; Baic, S.; Melichar, J.K. Taste and weight: is there a link? Am. J. Clin. Nutr. 2009, 90, 800S–803S. [Google Scholar] [CrossRef] [PubMed]
- Heilmann, S.; Strehle, G.; Rosenheim, K.; Damm, M.; Hummel, T. Clinical assessment of retronasal olfactory function. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, G.M. Smell images and the flavour system in the human brain. Nature 2006, 444, 316–321. [Google Scholar] [CrossRef]
- Breslin, P.A.S. An evolutionary perspective on food and human taste. Curr. Biol. 2013, 23, 409–418. [Google Scholar] [CrossRef]
- Stevenson, R.J.; Boakes, R.A.; Oaten, M.J.; Yeomans, M.R.; Mahmut, M.; Francis, H.M. Chemosensory abilities in consumers of a western-style diet. Chem. Senses. 2016, 41, 505–513. [Google Scholar] [CrossRef]
- Uerlich, M.F.; Yumuk, V.; Finer, N.; Basdevant, A.; Visscher, T.L.S. Obesity management in Europe: current status and objectives for the future. Obes. Facts. 2016, 9, 273–283. [Google Scholar] [CrossRef]
- Cho, Y.; Hong, N.; Kim, K.-W.; Cho, S.J.; Lee, M.; Lee, Y.-H.; Lee, Y.-H.; Kang, E.S.; Cha, B.-S.; Lee, B.-W. The effectiveness of Intermittent fasting to reduce body mass index and glucose metabolism: a systematic review and meta-analysis. J. Clin. Med. 2019, 8, 1645. [Google Scholar] [CrossRef]
- Ramaekers, M.G.; Boesveldt, S.; Lakemond, C.M.M.; van Boekel, M.A.J.S.; Luning, P.A. Odors: appetizing or satiating? Development of appetite during odor exposure over time. Int. J. Obes. (Lond) 2014, 38, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.J.; Hardman, C.A. Food reward. What it is and how to measure it. Appetite 2015, 90, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, A.; Green, E.; Haase, L.; Szajer, J.; Murphy, C. Differential Effects of BMI on Brain Response to Odor in Olfactory, Reward and Memory Regions: Evidence from fMRI. Nutrients 2019, 4, 926. [Google Scholar] [CrossRef] [PubMed]
- Proserpio, C.; Laureati, M.; Invitti, C.; Cattaneo, C.; Pagliarini, E. BMI and gender related differences in cross-modal interaction and liking of sensory stimuli. Food Qual. Prefer. 2017, 56, 49–54. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No. | Item 1 | Item 2 | Item 3 | Item 4 |
|---|---|---|---|---|
| 1 | lemon | apple | peppermint | gingerbread |
| 2 | chocolate | raspberry | coconut | cherry |
| 3 | walnut | tomato | coke | peach |
| 4 | cinnamon | pear | apple | woodruff |
| 5 | cucumber | chocolate | banana | orange |
| 6 | grapes | vanilla | hazelnut | orange |
| 7 | lemon | cube sugar | pineapple | nut nougat |
| 8 | honeydew | coffee | strawberry | mandarin |
| 9 | orange | coke | peach | chocolate |
| 10 | woodruff | chocolate | peanut | strawberry |
| 11 | cucumber | cinnamon | pear | licorice |
| 12 | banana | gingerbread | lemon | grapes |
| 13 | coconut | strawberry | walnut | blackcurrant |
| 14 | mandarin | peanut | anise | caramel |
| 15 | passion fruit | blackcurrant | hazelnut | pineapple |
| 16 | mandarin | nougat | kiwi | vanilla |
| 17 | apple | peanut | orange | coke |
| 18 | coke | vanilla | hazelnut | tomato |
| 19 | cucumber | coconut | cube sugar | cherry |
| 20 | coconut | orange | coke | apricot |
| 21 | coffee | rhubarb | walnut | lemon |
| 22 | vanilla | kiwi | coconut | orange |
| 23 | peppermint | chocolate | eisbonbon | tomato |
| 24 | plum | anise | gingerbread | licorice |
| 25 | condensed milk | mandarin | walnut | chocolate |
| 26 | raspberry | nut nougat | honeydew | vanilla |
| 27 | licorice | anise | peppermint | apple |
| No. | Statement | A | B | C | D |
|---|---|---|---|---|---|
| 1 | I pay attention to odors in my surroundings when leaving the house | ||||
| 2 | When eating an apple, I think of its smell | ||||
| 3 | When I see flowers, I consciously smell them | ||||
| 4 | On a market, I consciously notice the odors | ||||
| 5 | When cooking, I smell each ingredient to see if they match | ||||
| 6 | When a bedroom smells unpleasant, I let some air in | ||||
| 7 | Thinking of my partner, I think of his/her smell | ||||
| 8 | Smelling a glass of wine, I pay attention to different aromas | ||||
| 9 | I remember body odors of relatives/friends/familiar persons | ||||
| 10 | When buying flowers, I decide by the smell | ||||
| 11 | After a rainfall, I notice odors more intensely | ||||
| 12 | When cooking, I pay attention to the smell of each ingredient | ||||
| 13 | Often during the course of the day, I check if my hands, armpits, breath et cetera smell funny | ||||
| 14 | I notice seasonal (winter/summer) differences in surrounding odors | ||||
| 15 | For my occupation a good sense of smell is essential | ||||
| 16 | For my hobbies a good sense of smell is essential | ||||
| 17 | Good food is my greatest passion | ||||
| 18 | Enjoying good wine makes me happy |
| n = 15 | ||
|---|---|---|
| Mean | SD | |
| Age | 43.7 | 11.2 |
| BMI | 44.3 | 6.2 |
| Odor threshold | 6.0 | 2.5 |
| Odor discrimination | 12.1 | 1.7 |
| Odor identification | 13.3 | 1.8 |
| TDI | 31.3 | 4.7 |
| ISO | 65.5 | 14.1 |
| n = 7 | ||
| Candy Smell Test | 15.3 | 4.6 |
| n = 185 (122 f, 63 m) | Mean | SD |
| Age | 31.1 | 12.4 |
| BMI | 24.9 | 7.0 |
| Odor identification | 13.8 | 1.3 |
| n = 74 (47 f, 27 m) | Mean | SD |
| Age | 32.8 | 11.9 |
| BMI | 27.3 | 9.5 |
| Odor threshold | 6.7 | 2.8 |
| Odor discrimination | 13.6 | 1.7 |
| Odor identification | 13.9 | 1.3 |
| TDI | 33.0 | 4.5 |
| n = 66 (42 f, 24 m) | Mean | SD |
| Age | 30.9 | 10.8 |
| BMI | 25.2 | 7.4 |
| Candy Smell Test | 19.4 | 3.3 |
| n = 48 (30 f, 18 m) OH | Mean | SD |
| Age | 33.3 | 12.4 |
| BMI | 29.8 | 10.8 |
| ISO | 62.3 | 12.0 |
| n = 52 (35 f, 17 m) OD | Mean | SD |
| Age | 55.9 | 17.7 |
| BMI | 25.7 | 4.5 |
| ISO | 68.4 | 15.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Besser, G.; Erlacher, B.; Aydinkoc-Tuzcu, K.; Liu, D.T.; Pablik, E.; Niebauer, V.; Koenighofer, M.; Renner, B.; Mueller, C.A. Body-Mass-Index Associated Differences in Ortho- and Retronasal Olfactory Function and the Individual Significance of Olfaction in Health and Disease. J. Clin. Med. 2020, 9, 366. https://doi.org/10.3390/jcm9020366
Besser G, Erlacher B, Aydinkoc-Tuzcu K, Liu DT, Pablik E, Niebauer V, Koenighofer M, Renner B, Mueller CA. Body-Mass-Index Associated Differences in Ortho- and Retronasal Olfactory Function and the Individual Significance of Olfaction in Health and Disease. Journal of Clinical Medicine. 2020; 9(2):366. https://doi.org/10.3390/jcm9020366
Chicago/Turabian StyleBesser, Gerold, Brigitte Erlacher, Kadriye Aydinkoc-Tuzcu, David T. Liu, Eleonore Pablik, Verena Niebauer, Martin Koenighofer, Bertold Renner, and Christian A. Mueller. 2020. "Body-Mass-Index Associated Differences in Ortho- and Retronasal Olfactory Function and the Individual Significance of Olfaction in Health and Disease" Journal of Clinical Medicine 9, no. 2: 366. https://doi.org/10.3390/jcm9020366
APA StyleBesser, G., Erlacher, B., Aydinkoc-Tuzcu, K., Liu, D. T., Pablik, E., Niebauer, V., Koenighofer, M., Renner, B., & Mueller, C. A. (2020). Body-Mass-Index Associated Differences in Ortho- and Retronasal Olfactory Function and the Individual Significance of Olfaction in Health and Disease. Journal of Clinical Medicine, 9(2), 366. https://doi.org/10.3390/jcm9020366