Conversion to Everolimus was Beneficial and Safe for Fast and Slow Tacrolimus Metabolizers after Renal Transplantation

 ,
,
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Statistical Analyses
3. Results
3.1. Descriptive Statistics
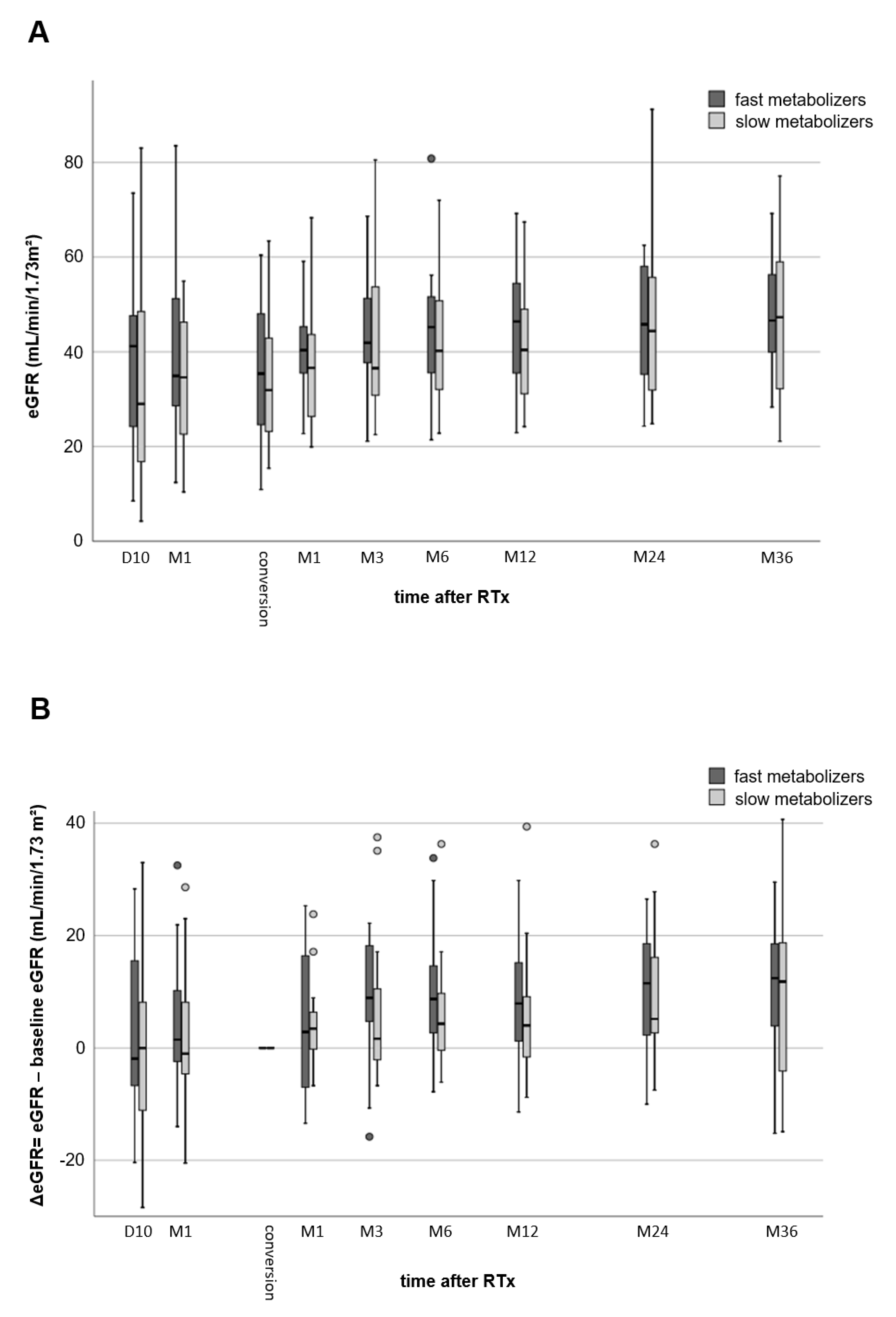
3.2. Renal Function
3.3. Adverse Events
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Kidney Disease: Improving Global Outcomes Transplant Work, G. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. 2009, 9 (Suppl. S3), S1–S155.
- Schutte-Nutgen, K.; Tholking, G.; Suwelack, B.; Reuter, S. Tacrolimus—Pharmacokinetic Considerations for Clinicians. Curr. Drug Metab. 2018, 19, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Ji, E.; Choi, L.; Suh, K.S.; Cho, J.Y.; Han, N.; Oh, J.M. Combinational effect of intestinal and hepatic CYP3A5 genotypes on tacrolimus pharmacokinetics in recipients of living donor liver transplantation. Transplantation 2012, 94, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Tholking, G.; Fortmann, C.; Koch, R.; Gerth, H.U.; Pabst, D.; Pavenstadt, H.; Kabar, I.; Husing, A.; Wolters, H.; Reuter, S.; et al. The tacrolimus metabolism rate influences renal function after kidney transplantation. PLoS ONE 2014, 9, e111128. [Google Scholar] [CrossRef] [PubMed]
- Schutte-Nutgen, K.; Tholking, G.; Steinke, J.; Pavenstadt, H.; Schmidt, R.; Suwelack, B.; Reuter, S. Fast Tac Metabolizers at Risk (-) It is Time for a C/D Ratio Calculation. J. Clin. Med. 2019, 8, 587. [Google Scholar] [CrossRef] [PubMed]
- Tholking, G.; Siats, L.; Fortmann, C.; Koch, R.; Husing, A.; Cicinnati, V.R.; Gerth, H.U.; Wolters, H.H.; Anthoni, C.; Pavenstadt, H.; et al. Tacrolimus Concentration/Dose Ratio is Associated with Renal Function After Liver Transplantation. Ann. Transplant. 2016, 21, 167–179. [Google Scholar] [CrossRef]
- Jouve, T.; Fonrose, X.; Noble, J.; Janbon, B.; Fiard, G.; Malvezzi, P.; Stanke-Labesque, F.; Rostaing, L. The TOMATO study (TacrOlimus MetabolizAtion in kidney TransplantatiOn): Impact of the concentration-dose ratio on death-censored graft survival. Transplantation 2019. [Google Scholar] [CrossRef]
- Egeland, E.J.; Reisaeter, A.V.; Robertsen, I.; Midtvedt, K.; Strom, E.H.; Holdaas, H.; Hartmann, A.; Asberg, A. High tacrolimus clearance—A risk factor for development of interstitial fibrosis and tubular atrophy in the transplanted kidney: A retrospective single-center cohort study. Trans. Int. 2019, 32, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Egeland, E.J.; Robertsen, I.; Hermann, M.; Midtvedt, K.; Storset, E.; Gustavsen, M.T.; Reisaeter, A.V.; Klaasen, R.; Bergan, S.; Holdaas, H.; et al. High Tacrolimus Clearance Is a Risk Factor for Acute Rejection in the Early Phase After Renal Transplantation. Transplantation 2017, 101, e273–e279. [Google Scholar] [CrossRef] [PubMed]
- Tholking, G.; Schutte-Nutgen, K.; Schmitz, J.; Rovas, A.; Dahmen, M.; Bautz, J.; Jehn, U.; Pavenstadt, H.; Heitplatz, B.; Van Marck, V.; et al. A Low Tacrolimus Concentration/Dose Ratio Increases the Risk for the Development of Acute Calcineurin Inhibitor-Induced Nephrotoxicity. J. Clin. Med. 2019, 8, 1586. [Google Scholar] [CrossRef]
- Budde, K.; Lehner, F.; Sommerer, C.; Reinke, P.; Arns, W.; Eisenberger, U.; Wuthrich, R.P.; Muhlfeld, A.; Heller, K.; Porstner, M.; et al. Five-year outcomes in kidney transplant patients converted from cyclosporine to everolimus: The randomized ZEUS study. Am. J. Transplant. 2015, 15, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Budde, K.; Sommerer, C.; Rath, T.; Reinke, P.; Haller, H.; Witzke, O.; Suwelack, B.; Baeumer, D.; Sieder, C.; Porstner, M.; et al. Renal function to 5 years after late conversion of kidney transplant patients to everolimus: A randomized trial. J. Nephrol. 2015, 28, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Tholking, G.; Schmidt, C.; Koch, R.; Schuette-Nuetgen, K.; Pabst, D.; Wolters, H.; Kabar, I.; Husing, A.; Pavenstadt, H.; Reuter, S.; et al. Influence of tacrolimus metabolism rate on BKV infection after kidney transplantation. Sci. Rep. 2016, 6, 32273. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am. J. Transplant. 2018, 18, 293–307. [Google Scholar] [CrossRef]
- Nowicka, M.; Gorska, M.; Nowicka, Z.; Edyko, K.; Edyko, P.; Wislicki, S.; Zawiasa-Bryszewska, A.; Strzelczyk, J.; Matych, J.; Kurnatowska, I. Tacrolimus: Influence of the Posttransplant Concentration/Dose Ratio on Kidney Graft Function in a Two-Year Follow-Up. Kidney Blood Press. Res. 2019, 44, 1075–1088. [Google Scholar] [CrossRef]
- Stegall, M.D.; Cornell, L.D.; Park, W.D.; Smith, B.H.; Cosio, F.G. Renal Allograft Histology at 10 Years After Transplantation in the Tacrolimus Era: Evidence of Pervasive Chronic Injury. Am. J. Transplant. 2018, 18, 180–188. [Google Scholar] [CrossRef]
- Einecke, G.; Reeve, J.; Halloran, P.F. Hyalinosis Lesions in Renal Transplant Biopsies: Time-Dependent Complexity of Interpretation. Am. J. Transplant. 2017, 17, 1346–1357. [Google Scholar] [CrossRef]
- Naesens, M.; Kuypers, D.R.; Sarwal, M. Calcineurin inhibitor nephrotoxicity. Clin. J. Am. Soc. Nephrol. 2009, 4, 481–508. [Google Scholar] [CrossRef]
- Nanmoku, K.; Shinzato, T.; Kubo, T.; Shimizu, T.; Yagisawa, T. Conversion to Everolimus in Kidney Transplant Recipients with Calcineurin Inhibitor-Induced Nephropathy: 3 Case Reports. Trans. Proc. 2019, 51, 1424–1427. [Google Scholar] [CrossRef]
- Morales, J.; Fierro, A.; Benavente, D.; Zehnder, C.; Ferrario, M.; Contreras, L.; Herzog, C.; Buckel, E. Conversion from a calcineurin inhibitor-based immunosuppressive regimen to everolimus in renal transplant recipients: Effect on renal function and proteinuria. Trans. Proc. 2007, 39, 591–593. [Google Scholar] [CrossRef]
- Hoskova, L.; Malek, I.; Kopkan, L.; Kautzner, J. Pathophysiological mechanisms of calcineurin inhibitor-induced nephrotoxicity and arterial hypertension. Physiol. Res. 2017, 66, 167–180. [Google Scholar] [CrossRef]
- Gardiner, S.M.; March, J.E.; Kemp, P.A.; Fallgren, B.; Bennett, T. Regional haemodynamic effects of cyclosporine A, tacrolimus and sirolimus in conscious rats. Br. J. Pharmacol. 2004, 141, 634–643. [Google Scholar] [CrossRef]
- Zaltzman, J.S. A comparison of short-term exposure of once-daily extended release tacrolimus and twice-daily cyclosporine on renal function in healthy volunteers. Transplantation 2010, 90, 1185–1191. [Google Scholar] [CrossRef]
- Alperovich, G.; Maldonado, R.; Moreso, F.; Fulladosa, X.; Grinyo, J.M.; Seron, D. Glomerular enlargement assessed by paired donor and early protocol renal allograft biopsies. Am. J. Transplant. 2004, 4, 650–654. [Google Scholar] [CrossRef]
- Ma, M.K.M.; Yung, S.; Chan, T.M. mTOR Inhibition and Kidney Diseases. Transplantation 2018, 102, S32–S40. [Google Scholar] [CrossRef]
- Husing, A.; Schmidt, M.; Beckebaum, S.; Cicinnati, V.R.; Koch, R.; Tholking, G.; Stella, J.; Heinzow, H.; Schmidt, H.H.; Kabar, I. Long-Term Renal Function in Liver Transplant Recipients After Conversion from Calcineurin Inhibitors to mTOR Inhibitors. Ann. Transplant. 2015, 20, 707–713. [Google Scholar] [CrossRef][Green Version]
- Lui, S.L.; Chan, K.W.; Tsang, R.; Yung, S.; Lai, K.N.; Chan, T.M. Effect of rapamycin on renal ischemia-reperfusion injury in mice. Trans. Int. 2006, 19, 834–839. [Google Scholar] [CrossRef]
- Smith, K.D.; Wrenshall, L.E.; Nicosia, R.F.; Pichler, R.; Marsh, C.L.; Alpers, C.E.; Polissar, N.; Davis, C.L. Delayed graft function and cast nephropathy associated with tacrolimus plus rapamycin use. J. Am. Soc. Nephrol. 2003, 14, 1037–1045. [Google Scholar] [CrossRef]
- Sanchez-Escuredo, A.; Diekmann, F.; Revuelta, I.; Esforzado, N.; Ricart, M.J.; Cofan, F.; Torregrosa, J.V.; Peri, L.; Ruiz, A.; Campistol, J.M.; et al. An mTOR-inhibitor-based protocol and calcineurin inhibitor (CNI)-free treatment in kidney transplant recipients from donors after cardiac death: Good renal function, but high incidence of conversion to CNI. Trans. Int. 2016, 29, 362–368. [Google Scholar] [CrossRef]
- Sommerer, C.; Suwelack, B.; Dragun, D.; Schenker, P.; Hauser, I.A.; Witzke, O.; Hugo, C.; Kamar, N.; Merville, P.; Junge, M.; et al. An open-label, randomized trial indicates that everolimus with tacrolimus or cyclosporine is comparable to standard immunosuppression in de novo kidney transplant patients. Kidney Int. 2019, 96, 231–244. [Google Scholar] [CrossRef]
- Tedesco-Silva, H.; Pascual, J.; Viklicky, O.; Basic-Jukic, N.; Cassuto, E.; Kim, D.Y.; Cruzado, J.M.; Sommerer, C.; Adel Bakr, M.; Garcia, V.D.; et al. Safety of Everolimus with Reduced Calcineurin Inhibitor Exposure in De Novo Kidney Transplants: An Analysis from the Randomized TRANSFORM Study. Transplantation 2019, 103, 1953–1963. [Google Scholar] [CrossRef]
- Manzia, T.M.; Carmellini, M.; Todeschini, P.; Secchi, A.; Sandrini, S.; Minetti, E.; Furian, L.; Spagnoletti, G.; Pisani, F.P.; Piredda, G.B.P.; et al. A 3-month, multicenter, randomized, open-label study to evaluate the impact on wound healing of the early [vs. delayed] introduction of everolimus in de novo kidney transplant recipients, with a follow-up evaluation at 12 month after transplant (NEVERWOUND study). Transplantation 2019. [Google Scholar] [CrossRef]
- Rivelli, R.F.; Goncalves, R.T.; Leite, M., Jr.; Santos, M.A.; Delgado, A.G.; Cardoso, L.R.; Takiya, C.M. Early withdrawal of calcineurin inhibitor from a sirolimus-based immunosuppression stabilizes fibrosis and the transforming growth factor-beta signalling pathway in kidney transplant. Nephrology 2015, 20, 168–176. [Google Scholar] [CrossRef] [PubMed]
- de Fijter, J.W.; Holdaas, H.; Oyen, O.; Sanders, J.S.; Sundar, S.; Bemelman, F.J.; Sommerer, C.; Pascual, J.; Avihingsanon, Y.; Pongskul, C.; et al. Early Conversion from Calcineurin Inhibitor—To Everolimus-Based Therapy Following Kidney Transplantation: Results of the Randomized ELEVATE Trial. Am. J. Transplant. 2017, 17, 1853–1867. [Google Scholar] [CrossRef]
- Cataneo-Davila, A.; Zuniga-Varga, J.; Correa-Rotter, R.; Alberu, J. Renal function outcomes in kidney transplant recipients after conversion to everolimus-based immunosuppression regimen with CNI reduction or elimination. Trans. Proc. 2009, 41, 4138–4146. [Google Scholar] [CrossRef]
- Kamar, N.; Del Bello, A.; Congy-Jolivet, N.; Guilbeau-Frugier, C.; Cardeau-Desangles, I.; Fort, M.; Esposito, L.; Guitard, J.; Game, X.; Rostaing, L. Incidence of donor-specific antibodies in kidney transplant patients following conversion to an everolimus-based calcineurin inhibitor-free regimen. Clin. Transplant. 2013, 27, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Croze, L.E.; Tetaz, R.; Roustit, M.; Malvezzi, P.; Janbon, B.; Jouve, T.; Pinel, N.; Masson, D.; Quesada, J.L.; Bayle, F.; et al. Conversion to mammalian target of rapamycin inhibitors increases risk of de novo donor-specific antibodies. Trans. Int. 2014, 27, 775–783. [Google Scholar] [CrossRef]
- Fischer, L.; Klempnauer, J.; Beckebaum, S.; Metselaar, H.J.; Neuhaus, P.; Schemmer, P.; Settmacher, U.; Heyne, N.; Clavien, P.A.; Muehlbacher, F.; et al. A randomized, controlled study to assess the conversion from calcineurin-inhibitors to everolimus after liver transplantation--PROTECT. Am. J. Transplant. 2012, 12, 1855–1865. [Google Scholar] [CrossRef]
- Budde, K.; Lehner, F.; Sommerer, C.; Arns, W.; Reinke, P.; Eisenberger, U.; Wuthrich, R.P.; Scheidl, S.; May, C.; Paulus, E.M.; et al. Conversion from cyclosporine to everolimus at 4.5 months posttransplant: 3-year results from the randomized ZEUS study. Am. J. Transplant. 2012, 12, 1528–1540. [Google Scholar] [CrossRef]
- Diekmann, F.; Andres, A.; Oppenheimer, F. mTOR inhibitor-associated proteinuria in kidney transplant recipients. Transplant. Rev. 2012, 26, 27–29. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, A.C.; McCague, K.; Kim, Y.; Geissler, F.; Cooper, M. The effect of everolimus versus mycophenolate upon proteinuria following kidney transplant and relationship to graft outcomes. Am. J. Transplant. 2013, 13, 442–449. [Google Scholar] [CrossRef]
- Ponticelli, C.; Graziani, G. Proteinuria after kidney transplantation. Trans. Int. 2012, 25, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Giron, F.; Baez, Y.; Nino-Murcia, A.; Rodriguez, J.; Salcedo, S. Conversion therapy to everolimus in renal transplant recipients: Results after one year. Transplant. Proc. 2008, 40, 711–713. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fast Metabolizers (n = 17) | Slow Metabolizers (n = 17) | p-Values | |
|---|---|---|---|
| Recipient Characteristics | |||
| Sex (m/f) | 11 (65%)/6 (35%) | 10 (59%)/7 (41%) | 1 a |
| Age (year) | 48.0 ± 15.7 | 54.6 ± 12.8 | 0.187 b |
| Height (cm) | 175.0 ± 10.7 | 171.4 ± 10.2 | 0.317 b |
| Weight (kg) | 79.0 ± 20.6 | 69.0 ± 11.9 | 0.095 b |
| BMI (kg/m2) | 24.7 (18.7–35.8) | 22.3 (18.9–32.6) | 0.114 c |
| Transplant characteristics | |||
| Number of RTx | |||
| 1 | 15 (88%) | 13 (77%) | 0.511 a |
| 2 | 2 (12%) | 3 (18%) | |
| 3 | 0 | 1 (6%) | |
| Living donor transplantation | 6 (35%) | 7 (41%) | 1 a |
| ABOi | 0 | 2 (12%) | 0.485 a |
| ESP | 1 (6%) | 2 (12%) | 1 a |
| CIT (h) | 6.8 (1.6–17.4) | 5.5 (1.6–19.3) | 0.838 c |
| WIT (min) | 35 (20–45) | 30 (25–50) | 0.858 c |
| CMV risk | |||
| Low | 6 (35%) | 2 (12%) | 0.139 a |
| Intermediate | 7 (41%) | 13 (77%) | |
| High | 4 (24%) | 2 (12%) | |
| Donor characteristics | |||
| Donor sex (m/f) | 10 (59%)/7 (41%) | 6 (35%)/11 (66%) | 0.303 a |
| Donor age (year) | 56.8 ± 8.8 | 57.4 ± 10.9 | 0.877 b |
| Immunosuppression at M1 | |||
| TAC dose (mg) | 12 (7–23) | 7 (4–12) | <0.001 c |
| TAC trough level (ng/mL) | 8.5 (4.6–17.6) | 10.0 (5.6–14.1) | 0.208 c |
| TAC C/D ratio (ng/mL*1/mg) | 0.77 (0.40–1.00) | 1.35 (1.05–2.56) | <0.001 b |
| Prednisolone dose (mg) | 20 (15–40) | 20 (15–50) | 0.422 c |
| Mycophenolate mofetil dose (mg) | 1000 (750–2000) | 1000 (1000–2000) | 0.501 c |
| Fast Metabolizers (n = 17) | Slow Metabolizers (n = 17) | p-Value | |
|---|---|---|---|
| CNI-nephrotoxicity | 13 (77%) | 10 (59%) | 0.277 |
| chronic rejection | 0 | 2 (12%) | |
| DGF | 1 (6%) | 2 (12%) | |
| NODAT | 2 (12%) | 0 | |
| BKV-infection | 0 | 1 (6%) | |
| neutropenia | 0 | 1 (6%) | |
| neurotoxicity | 0 | 1 (6%) | |
| study | 1 (6%) | 0 |
| Fast Metabolizers (n = 17) | Slow Metabolizers (n = 17) | p-Value | |
|---|---|---|---|
| DGF | 4 (24%) | 5 (29%) | 1 a |
| Antibodies and rejection | |||
| Preformed Class II DSA | 1 (6%) | 1 (6%) | 1 a |
| Class II DSA before conversion | 1 (6%) | 1 (6%) | 1 a |
| Class I DSA after conversion | 1 (6%) | 0 | 1 a |
| BPAR before conversion to EVR | |||
| AMR | 1 (6%) | 1 (6%) | 0.490 b |
| TCMR | 1 (6%) | 2 (12%) | |
| Combined AMR + TCMR | 7 (41%) | 3 (18%) | |
| BPAR after conversion to EVR | |||
| AMR | 0 | 0 | 0.485 a |
| TCMR | 2 (12%) | 0 | |
| Combined AMR + TCMR | 0 | 1 (6%) | |
| Infections | |||
| CMV infection before conversion | 2 (12%) | 4 (24%) | 0.656 a |
| CMV infection after conversion | 1 (6%) | 0 | 1 a |
| BKV infection before conversion | 2 (12%) | 1 (6%) | 1 a |
| BKV infection after conversion | 0 | 0 | - |
| Death | 0 | 1 (6%) | 1 a |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thölking, G.; Gillhaus, N.H.; Schütte-Nütgen, K.; Pavenstädt, H.; Koch, R.; Suwelack, B.; Reuter, S. Conversion to Everolimus was Beneficial and Safe for Fast and Slow Tacrolimus Metabolizers after Renal Transplantation. J. Clin. Med. 2020, 9, 328. https://doi.org/10.3390/jcm9020328
Thölking G, Gillhaus NH, Schütte-Nütgen K, Pavenstädt H, Koch R, Suwelack B, Reuter S. Conversion to Everolimus was Beneficial and Safe for Fast and Slow Tacrolimus Metabolizers after Renal Transplantation. Journal of Clinical Medicine. 2020; 9(2):328. https://doi.org/10.3390/jcm9020328
Chicago/Turabian StyleThölking, Gerold, Nils Hendrik Gillhaus, Katharina Schütte-Nütgen, Hermann Pavenstädt, Raphael Koch, Barbara Suwelack, and Stefan Reuter. 2020. "Conversion to Everolimus was Beneficial and Safe for Fast and Slow Tacrolimus Metabolizers after Renal Transplantation" Journal of Clinical Medicine 9, no. 2: 328. https://doi.org/10.3390/jcm9020328
APA StyleThölking, G., Gillhaus, N. H., Schütte-Nütgen, K., Pavenstädt, H., Koch, R., Suwelack, B., & Reuter, S. (2020). Conversion to Everolimus was Beneficial and Safe for Fast and Slow Tacrolimus Metabolizers after Renal Transplantation. Journal of Clinical Medicine, 9(2), 328. https://doi.org/10.3390/jcm9020328