Outcomes of Mechanical Circulatory Support for Giant Cell Myocarditis: A Systematic Review

 ,
,  ,
,
Abstract
1. Introduction
2. Experimental Section
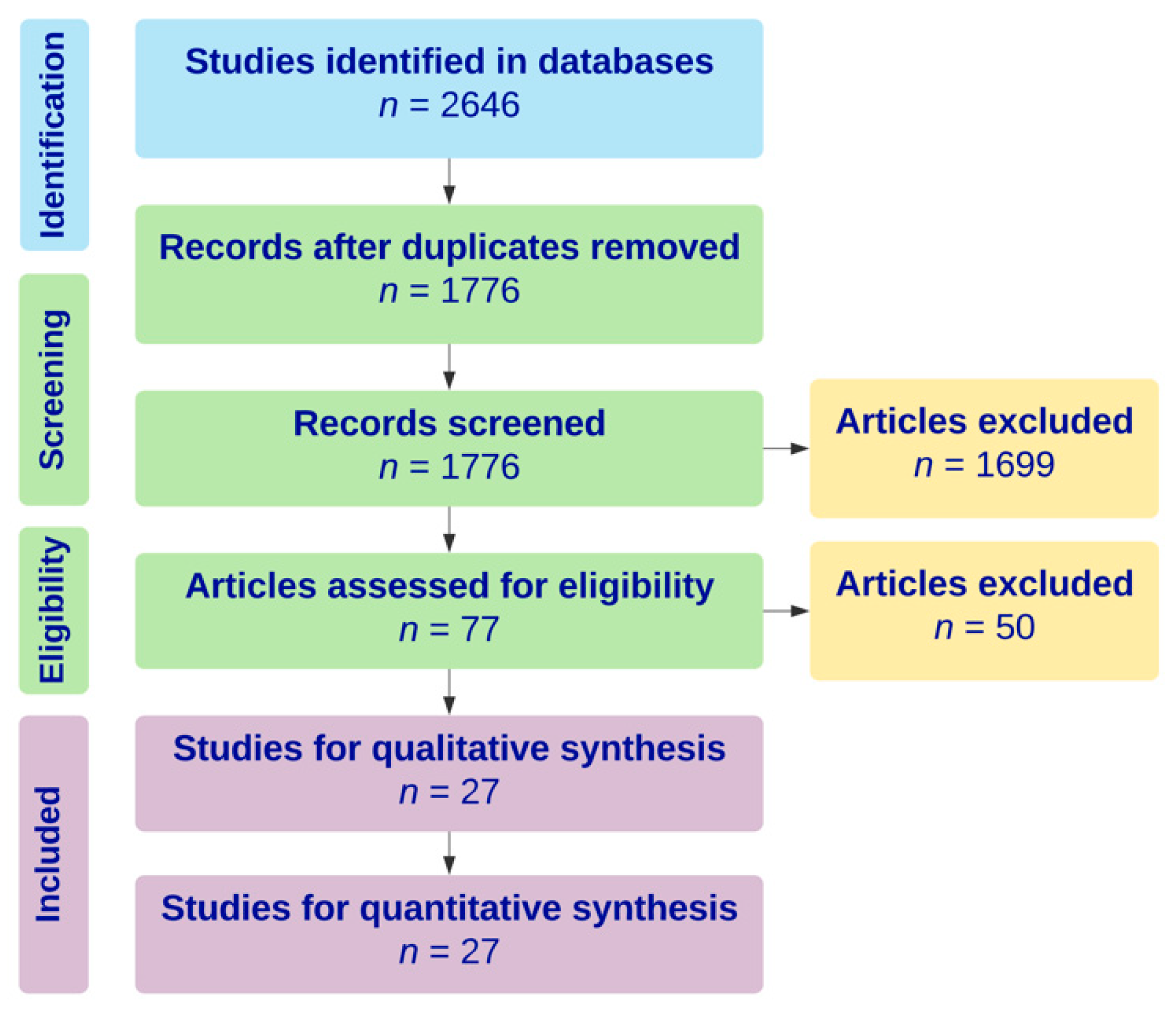
2.1. Literature Search
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
2.5. Evaluation of Missing Data
3. Results
3.1. Baseline Characteristics
3.2. Complications and Outcomes
4. Discussion
4.1. Discussion of Clinical Significance
4.2. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Davies, R.A.; Veinot, J.P.; Smith, S. Giant cell myocarditis: Clinical long-term outcome. J. Heart Lung Transpl. 2002, 21, 674–679. [Google Scholar] [CrossRef]
- Davidoff, R.; Palacios, I.; Southern, J.; Fallon, J.T.; Newell, J.; Dec, G.W. Giant cell versus lymphocytic myocarditis. A comparison of their clinical features and long-term outcomes. Circulation 1991, 83, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Bracamonte-Baran, W.; Čiháková, D. Cardiac autoimmunity: Myocarditis. Adv. Exp. Med. Biol. 2017, 1003, 187–221. [Google Scholar] [PubMed]
- Blauwet, L.A.; Cooper, L.T. Myocarditis. Prog. Cardiovasc. Dis. 2010, 52, 274–288. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T.; Shabetai, R. Announcement of multicenter giant-cell myocarditis study. Am. J. Cardiol. 1995, 76, 640. [Google Scholar] [CrossRef]
- Kandolin, R.; Lehtonen, J.; Salmenkivi, K.; Räisänen-Sokolowski, A.; Lommi, J.; Kupari, M. Diagnosis, treatment, and outcome of giant-cell myocarditis in the era of combined immunosuppression. Circ. Heart Fail. 2013, 6, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, M.N.; Køber, L.; Weeke, P.; Vasan, R.S.; Jeppesen, J.L.; Smith, J.G.; Gislason, G.H.; Torp-Pedersen, C.; Andersson, C. Age-specific trends in incidence, mortality, and comorbidities of heart failure in Denmark, 1995 to 2012. Circulation 2017, 135, 1214–1223. [Google Scholar] [CrossRef]
- Yin, M.Y.; Wever-Pinzon, O.; Mehra, M.R.; Selzman, C.H.; Toll, A.E.; Cherikh, W.S.; Nativi-Nicolau, J.; Fang, J.C.; Kfoury, A.G.; Gilbert, E.M.; et al. Post-transplant outcome in patients bridged to transplant with temporary mechanical circulatory support devices. J. Heart Lung Transpl. 2019, 38, 858–869. [Google Scholar] [CrossRef]
- Seeburger, J.; Doll, N.; Doll, S.; Borger, M.A.; Mohr, F.W. Mechanical assist and transplantation for treatment of giant cell myocarditis. Can. J. Cardiol. 2010, 26, 96. [Google Scholar] [CrossRef]
- ElAmm, C.A.; Al-Kindi, S.G.; Bianco, C.M.; Dhakal, B.P.; Oliveira, G.H. Heart transplantation in giant cell myocarditis: Analysis of the united network for organ sharing registry. J. Card. Fail. 2017, 23, 566–569. [Google Scholar] [CrossRef]
- Kong, G.; Madden, B.; Spyrou, N.; Pomerance, A.; Mitchell, A.; Yacoub, M. Response of recurrent giant cell myocarditis in a transplanted heart to intensive immunosuppression. Eur. Heart J. 1991, 12, 554–557. [Google Scholar] [CrossRef]
- Gries, W.; Farkas, D.; Winters, G.L.; Costanzo-Nordin, M.R. Giant cell myocarditis: First report of disease recurrence in the transplanted heart. J. Heart Lung Transplant. 1992, 11, 370–374. [Google Scholar]
- Cooper, L.T.; Berry, G.J.; Shabetai, R. Idiopathic giant-cell myocarditis - Natural history and treatment. N. Engl. J. Med. 1997, 336, 1860–1866. [Google Scholar] [CrossRef] [PubMed]
- Maleszewski, J.J.; Orellana, V.M.; Hodge, D.O.; Kuhl, U.; Schultheiss, H.-P.; Cooper, L.T. Long-term risk of recurrence, morbidity and mortality in giant cell myocarditis. Am. J. Cardiol. 2015, 115, 1733–1738. [Google Scholar] [CrossRef] [PubMed]
- Koul, D.; Kanwar, M.; Jefic, D.; Kolluru, A.; Singh, T.; Dhar, S.; Kumar, P.; Cohen, G. Fulminant giant cell myocarditis and cardiogenic shock: An unusual presentation of malignant thymoma. Cardiol. Res. Pract. 2010, 2010, 185896. [Google Scholar] [CrossRef]
- Kociol, R.D.; Cooper, L.T.; Fang, J.C.; Moslehi, J.J.; Pang, P.S.; Sabe, M.A.; Shah, R.V.; Sims, D.B.; Thiene, G.; Vardeny, O.; et al. Recognition and initial management of fulminant myocarditis. Circulation 2020, 141, 69–92. [Google Scholar] [CrossRef] [PubMed]
- Montero, S.; Aissaoui, N.; Tadié, J.-M.; Bizouarn, P.; Scherrer, V.; Persichini, R.; Delmas, C.; Rolle, F.; Besnier, E.; Le Guyader, A.; et al. Fulminant giant-cell myocarditis on mechanical circulatory support: Management and outcomes of a French multicentre cohort. Int. J. Cardiol. 2018, 253, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Tschöpe, C.; Van Linthout, S.; Klein, O.; Mairinger, T.; Krackhardt, F.; Potapov, E.V.; Schmidt, G.; Burkhoff, D.; Pieske, B.; Spillmann, F. Mechanical unloading by fulminant myocarditis: Lv-impella, ecmella, bi-pella, and propella concepts. J. Cardiovasc Transl. Res. 2019, 12, 116–123. [Google Scholar] [CrossRef]
- Suradi, H.; Breall, J.A. Successful use of the impella device in giant cell Myocarditis as a bridge to permanent left Ventricular mechanical support. Texas Heart Inst. J. 2011, 38, 437–440. [Google Scholar]
- Murray, L.K.; González-Costello, J.; Jonas, S.N.; Sims, D.B.; Morrison, K.A.; Colombo, P.C.; Mancini, D.M.; Restaino, S.W.; Joye, E.; Horn, E.; et al. Ventricular assist device support as a bridge to heart transplantation in patients with giant cell myocarditis. Eur. J. Heart Fail. 2012, 14, 312–318. [Google Scholar] [CrossRef]
- Gošev, I.; Kiernan, M.S.; Eckman, P.; Soleimani, B.; Kilic, A.; Uriel, N.; Rich, J.D.; Katz, J.N.; Cowger, J.; Lima, B.; et al. Long-term survival in patients receiving a continuous-flow left ventricular assist device. Ann. Thorac. Surg. 2018, 105, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Rose, E.A.; Gelijns, A.C.; Moskowitz, A.J.; Heitjan, D.F.; Stevenson, L.W.; Dembitsky, W.P.; Long, J.W.; Ascheim, D.D.; Tierney, A.R.; Levitan, R.G.; et al. Long-term use of a left ventricular assist device for end-stage heart failure. N. Engl. J. Med. 2001, 345, 1435–1443. [Google Scholar] [CrossRef] [PubMed]
- Esmaily, S.; Bobbio, E.; Bollano, E.; Dahlberg, P.; Bartfay, S.; Dellgren, G.; Karason, K. Inflammatory cardiomyopathy (ICM): Long-term survival after heart transplantation or implantation of mechanical circulatory support. J. Heart Lung Transpl. 2019, 38, 292–293. [Google Scholar] [CrossRef]
- Shields, R.C.; Tazelaar, H.D.; Berry, G.J.; Cooper, L.T. The role of right ventricular endomyocardial biopsy for idiopathic giant cell myocarditis. J. Card. Fail. 2002, 8, 74–78. [Google Scholar] [CrossRef]
- Raasch, H.; Simpson, R.J. Biventricular assist device terminates polymorphic ventricular tachycardia: In giant cell myocarditis. Texas Heart Inst. J. 2012, 39, 719–721. [Google Scholar]
- Baraldi-Junkins, C.; Levin, H.R.; Kasper, E.K.; Rayburn, B.K.; Herskowitz, A.; Baughman, K.L. Complications of endomyocardial biopsy in heart transplant patients. J. Heart Lung Transpl. 1993, 12, 63–67. [Google Scholar]
- Shehab, S.; Hayward, C.S. Choosing between left ventricular assist devices and biventricular assist devices. Card. Fail. Rev. 2019, 5, 19–23. [Google Scholar] [CrossRef]
- Cooper, L.T.; Hare, J.M.; Tazelaar, H.D.; Edwards, W.D.; Starling, R.C.; Deng, M.C.; Menon, S.; Mullen, G.M.; Jaski, B.; Bailey, K.R.; et al. Usefulness of immunosuppression for giant cell myocarditis. Am. J. Cardiol. 2008, 102, 1535–1539. [Google Scholar] [CrossRef]
- Lumish, H.; Clerkin, K.; Marboe, C.; Han, J.; Latif, F.; Restaino, S.; Farr, M.; Lin, E.; Takayama, H.; Takeda, K.; et al. Giant cell myocarditis patients undergoing heart transplantation have high rates of rejection, infection and cardiac allograft vasculopathy: Case series. J. Heart Lung Transpl. 2018, 37, 419. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics 1 | MCS Alone (n = 16) | MCS + IS (n = 27) | Total (n = 43) | p-Value |
|---|---|---|---|---|
| Female | 5/11 (45.5) | 11/27 (40.7) | 16/38 (42.1) | 1.00 |
| Age at diagnosis (years) | 41.0 (30.0, 55.0) | 49.0 (34.5, 58.5) | 44.5 (32.2, 56.5) | 0.25 |
| History of autoimmune disease | 1/16 (6.2) | 7/24 (29.2) | 8/40 (20.0) | 0.17 |
| History of thymoma or other tumors | 0/16 (0.0) | 0/24 (0.0) | 0/40 (0.0) | 1.00 |
| Clinical presentation | ||||
| Acute heart failure | 5/16 (31.2) | 10/27 (37.0) | 15/43 (34.9) | 0.96 |
| Shortness of breath | 6/16 (37.5) | 4/27 (14.8) | 10/43 (23.3) | 0.18 |
| Cardiogenic shock | 3/16 (18.8) | 6/27 (22.2) | 9/43 (20.9) | 1.00 |
| Presyncope | 3/16 (18.8) | 3/27 (11.1) | 6/43 (14.0) | 0.81 |
| Chest pain | 2/16 (12.5) | 2/27 (7.4) | 4/43 (9.3) | 0.99 |
| Cardiac arrest requiring CPR | 0/16 (0.0) | 1/27 (3.7) | 1/43 (2.3) | 1.00 |
| ST segment elevation | 1/16 (6.2) | 4/27 (14.8) | 5/43 (11.6) | 0.72 |
| Arrhythmia | 11/15 (73.3) | 13/27 (48.1) | 24/42 (57.1) | 0.21 |
| Ventricular tachycardia | 5/15 (33.3) | 7/25 (28.0) | 12/40 (30.0) | 1.00 |
| Complete AV block | 3/15 (20.0) | 4/25 (16.0) | 7/40 (17.5) | 1.00 |
| Right bundle branch block | 2/15 (13.3) | 0/22 (0.0) | 2/37 (5.4) | 0.31 |
| Atrial fibrillation | 0/15 (0.0) | 1/25 (4.0) | 1/40 (2.5) | 1.00 |
| Time from symptoms to admission (days) | 7 (6, 7) | 8 (7, 11) | 7 (7, 10) | 0.20 |
| Elevated cardiac enzymes | 8/16 (50.0) | 3/27 (11.1) | 11/43 (25.6) | 0.13 |
| LVEF at presentation (%) | 17.0 (12.5, 20.0) | 28.0 (20.0, 30.0) | 20.0 (15.0, 28.2) | 0.03 |
| Biopsy proven | 16/16 (100.0) | 27/27 (100.0) | 43/43 (100.0) | 0.09 |
| Endomyocardial biopsy | 9/16 (56.2) | 22/27 (81.5) | 31/43 (72.1) | 0.15 |
| Apical sample during LVAD implantation | 6/16 (37.5) | 4/27 (14.8) | 10/43 (23.3) | 0.18 |
| Explanted heart | 1/43 (6.2) | 0/43 (0.0) | 1/43 (2.3) | 0.79 |
| Time from symptoms to diagnosis (days) | 16 (4,21) | 21 (9,54) | 18.5 (7,54) | 0.51 |
| Initial inotropic support | 11/14 (78.6) | 13/25 (52.0) | 24/39 (61.5) | 0.20 |
| MCS Characteristics 1 | MCS Only (n = 16) | MCS + IS (n = 27) | Total (n = 43) | p-Value |
|---|---|---|---|---|
| MCS as initial treatment | 16/16 (100.0) | 16/19 (84.2) | 32/35 (91.4) | 0.73 |
| MCS after immunosuppression failed | 3/19 (15.8) | 3/35 (8.6) | ||
| Time from admission to MCS (days) | 14 (5, 39) | 8 (4, 17) | 9 (4, 22) | 0.38 |
| Intra-aortic balloon pump | 2/14 (14.3) | 4/22 (18.2) | 6/36 (16.7) | 1.00 |
| Impella | 0/16 (0.0) | 3/27 (11.1) | 3/43 (7.0) | 0.45 |
| VA ECMO | 2/13 (15.4) | 7/23 (30.4) | 9/36 (25.0) | 0.55 |
| Temporary LVAD prior to durable LVAD | 1/16 (6.2) | 1/27 (3.7) | 2/43 (4.7) | 1.00 |
| Temporary LVAD prior to durable BiVAD | 3/16 (18.8) | 2/27 (7.4) | 5/43 (11.6) | 0.53 |
| Any LVAD | 16/16 (100.0) | 27/27 (100.0) | 43/43 (100.0) | 0.09 |
| Bridge to transplant | 8/16 (50.0) | 18/27 (66.7) | 26/43 (60.5) | 0.45 |
| Bridge to recovery | 8/16 (50.0) | 9/27 (33.3) | 17/43 (39.5) | 0.45 |
| Time from admission to LVAD (days) | 14 (5, 39) | 8 (4, 17) | 9 (4, 22) | 0.38 |
| VAD support duration (days) | 20 (13, 98) | 48 (17, 137) | 39 (15, 137) | 0.54 |
| Durable LVAD | 4/16 (25.0) | 6/27 (22.2) | 10/43 (23.3) | 1.00 |
| HeartMate II LVAD | 3/16 (18.8) | 2/27 (7.4) | 5/43 (11.6) | 0.53 |
| Jarvik 2000 LVAD | 1/16 (6.2) | 1/27 (3.7) | 2/43 (4.7) | 1.00 |
| Unspecified durable LVAD | 0/16 (0.0) | 3/27 (11.1) | 3/43 (7.0) | 0.45 |
| Any biventricular support | 12/16 (75.0) | 21/27 (77.8) | 33/43 (76.7) | 1.00 |
| Durable BiVAD | 4/16 (25.0) | 7/27 (25.9) | 11/43 (25.5) | 0.95 |
| HeartWare BiVAD | 1/16 (6.2) | 3/27 (11.1) | 4/43 (9.3) | 1.00 |
| Total artificial heart | 0/16 (0.0) | 1/27 (3.7) | 1/43 (2.3) | 1.00 |
| Unspecified durable BiVAD | 3/16 (18.8) | 1/27 (3.7) | 4/43 (9.3) | 1.00 |
| Durable LVAD + Temporary RVAD | 1/16 (6.2) | 2/27 (7.4) | 3/43 (7.0) | 0.88 |
| HeartMate II LVAD + Centrimag RVAD | 1/16 (6.2) | 1/27 (3.7) | 2/43 (4.7) | 1.00 |
| HeartMate II LVAD + Abiomed RVAD | 0/16 (0.0) | 1/27 (3.7) | 1/43 (2.3) | 1.00 |
| Temporary Centrimag BiVAD | 4/16 (25.0) | 4/27 (14.8) | 8/43 (18.6) | 0.67 |
| Unspecified BiVAD | 3/16 (18.8) | 8/27 (29.6) | 11/43 (25.5) | 0.43 |
| Characteristics of Immunotherapy 1 | MCS + IS (n = 27) |
|---|---|
| Initial (short-term) immunosuppression | |
| Immunosuppressants per regimen | 2.0 (2.0, 2.0) |
| Immunosuppression as first-line treatment | 16/24 (66.7) |
| Immunosuppression started after VAD | 8/24 (33.3) |
| Steroid-free regimen | 1/27 (3.7) |
| Steroids alone | 4/27 (14.8) |
| Combined steroids + other immunosuppressant 2 | 22/27 (81.5) |
| Cyclosporine | 11/27 (40.7) |
| Cyclophosphamide | 5/27 (18.5) |
| IV immunoglobulin | 4/27 (14.8) |
| Antithymocyte globulin | 2/27 (7.7) |
| Mycophenolate mofetil | 2/27 (7.4) |
| Azathioprine | 1/27 (3.7) |
| Tacrolimus | 1/27 (3.7) |
| Rituximab | 1/27 (3.8) |
| Muromonab | 1/27 (3.7) |
| Maintenance (long-term) immunosuppression | |
| Maintenance immunosuppression 2 | 11/27 (40.7) |
| Steroids | 11/26 (42.3) |
| Cyclosporine | 2/26 (7.4) |
| Mycophenolate mofetil | 6/26 (23.1) |
| Tacrolimus | 5/26 (19.2) |
| Rituximab | 1/26 (3.8) |
| Complications and Outcomes 1 | MCS alone (n = 16) | MCS + IS (n = 27) | Total (n = 43) | p-Value |
|---|---|---|---|---|
| Complications | ||||
| At least one infectious adverse event | 1/2 (50.0) | 5/10 (50.0) | 6/12 (50.0) | 1.00 |
| Recurrent GCM | 2/16 (12.5) | 3/27 (11.1) | 5/43(11.6) | 1.00 |
| Recurrent GCM after OHT | 0/16 (0.0) | 2/27 (7.4) | 2/43 (4.7) | 0.71 |
| New dual-chamber pacemaker placed | 1/16 (6.3) | 3/27 (1.1) | 4/43 (9.3) | 0.34 |
| Renal failure | 1/16 (6.3) | 1/19 (5.3) | 2/35 (5.7) | 0.90 |
| Severe hemorrhage | 1/1 (100.0) | 1/3 (33.3) | 2/4 (50.0) | 1.00 |
| Outcomes | ||||
| Transplant | 7/15 (46.7) | 17/26 (65.38) | 24/41 (58.5) | 0.24 |
| Time from diagnosis to transplant (days) | 175 (123, 270) | 70 (48, 247) | 104 (58, 255) | 0.35 |
| Overall mortality at the end of follow-up | 11/16 (68.8) | 11/27 (40.7) | 22/43 (51.2) | 0.14 |
| 30-day mortality | 8/16 (50.0) | 5/27 (18.5) | 13/43 (30.2) | 0.07 |
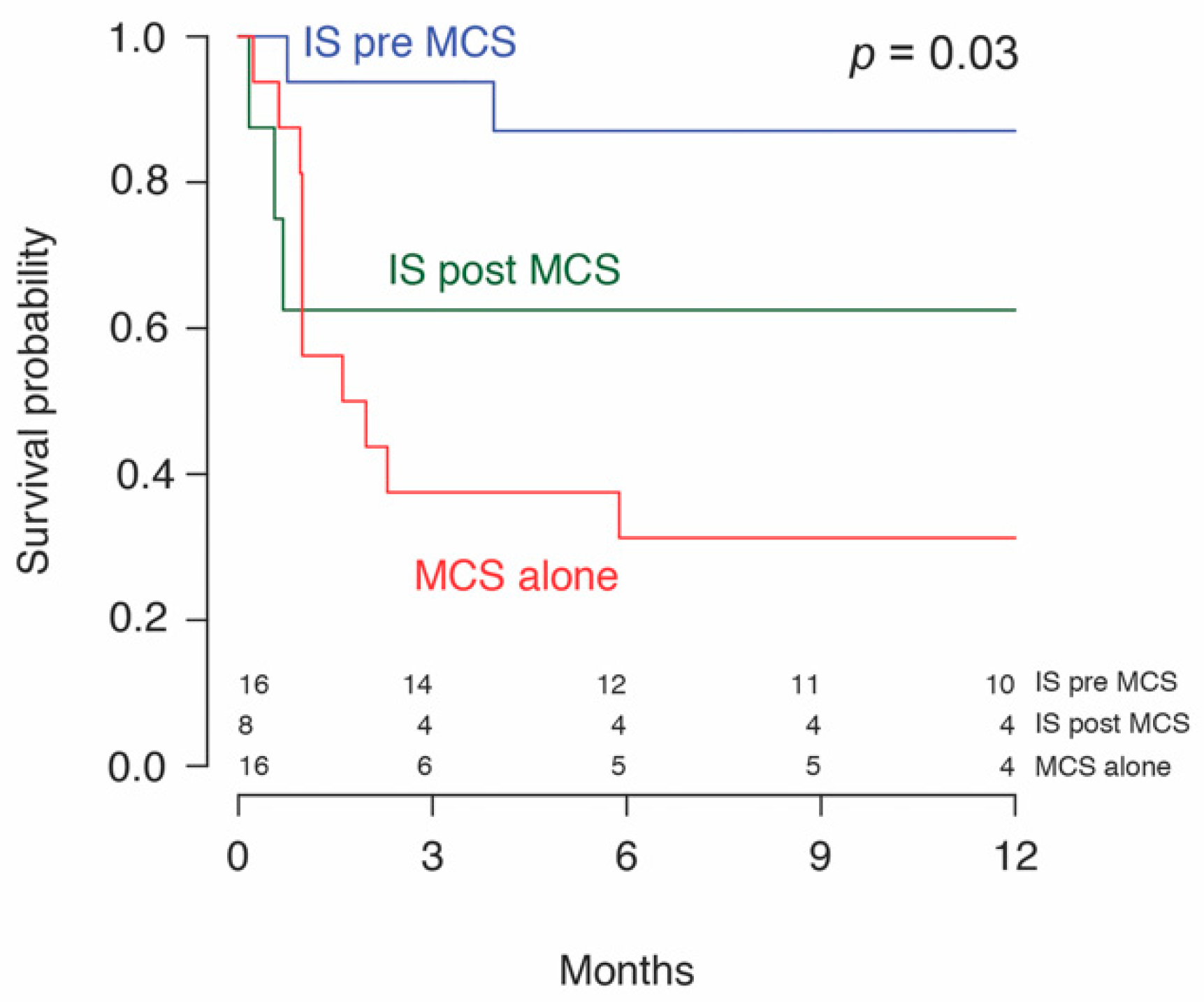
| One-year survival | 5/16 (31.2) | 16/22 (72.7) | 21/38 (55.3) | 0.03 |
| Duration of follow up (months) | 1.8 (1.0, 14.0) | 24.0 (3.5, 36.2) | 11.5 (1.0, 34.5) | 0.06 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p-Value | HR (95% CI) | p-Value |
| Immunosuppression used | 0.42 (0.18–0.99) | 0.049 | 0.45 (0.19–1.10) | 0.078 |
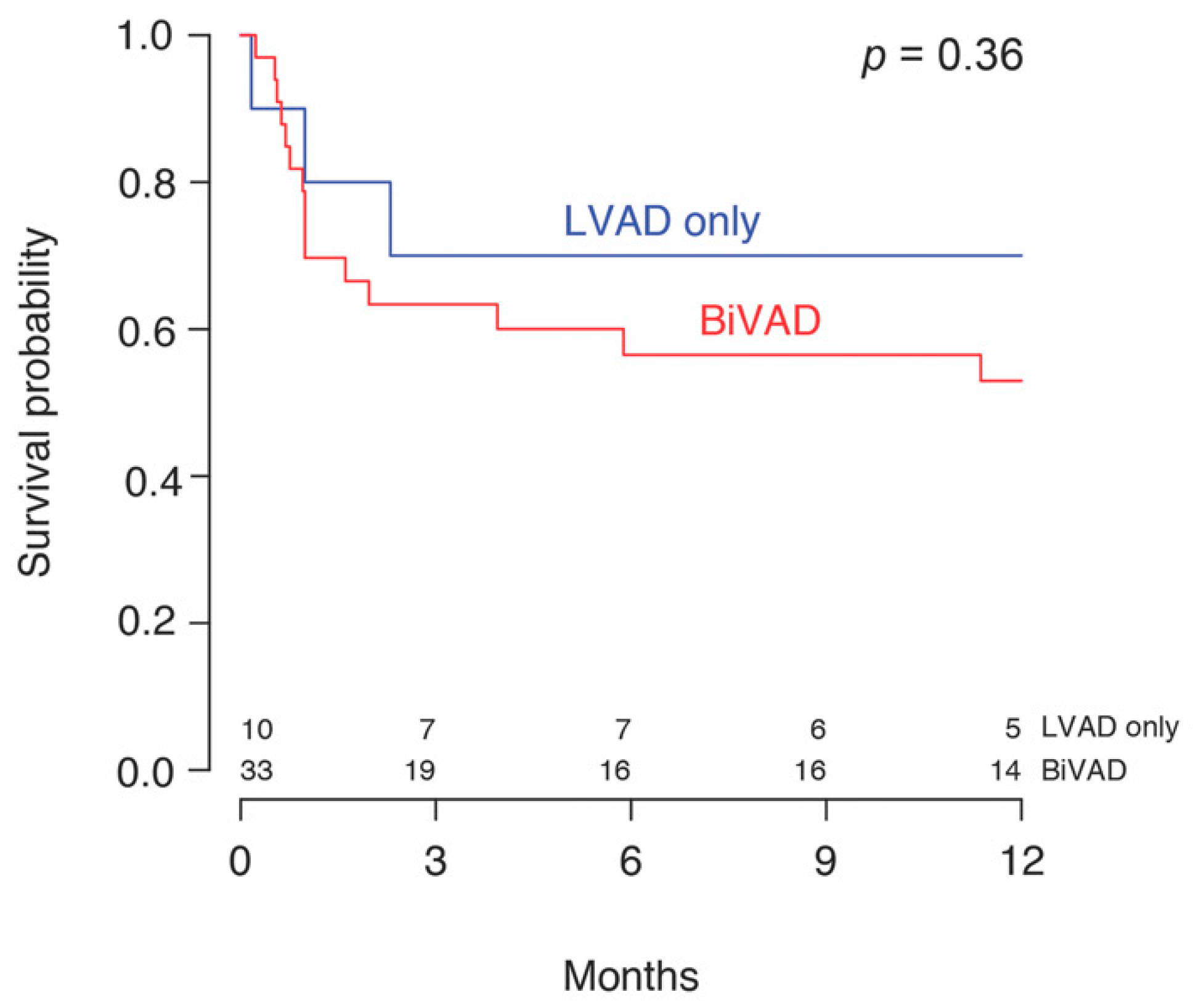
| tMCS * used before durable MCS | 0.58 (0.23–1.45) | 0.246 | 0.68 (0.27–1.75) | 0.429 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, P.M.; Saxena, A.; Wood, C.T.; O’Malley, T.J.; Maynes, E.J.; Entwistle, J.W.C.; Massey, H.T.; Pirlamarla, P.R.; Alvarez, R.J.; Cooper, L.T.; et al. Outcomes of Mechanical Circulatory Support for Giant Cell Myocarditis: A Systematic Review. J. Clin. Med. 2020, 9, 3905. https://doi.org/10.3390/jcm9123905
Patel PM, Saxena A, Wood CT, O’Malley TJ, Maynes EJ, Entwistle JWC, Massey HT, Pirlamarla PR, Alvarez RJ, Cooper LT, et al. Outcomes of Mechanical Circulatory Support for Giant Cell Myocarditis: A Systematic Review. Journal of Clinical Medicine. 2020; 9(12):3905. https://doi.org/10.3390/jcm9123905
Chicago/Turabian StylePatel, Preeyal M., Abhiraj Saxena, Chelsey T. Wood, Thomas J. O’Malley, Elizabeth J. Maynes, John W. C. Entwistle, H. Todd Massey, Preethi R. Pirlamarla, René J. Alvarez, Leslie T. Cooper, and et al. 2020. "Outcomes of Mechanical Circulatory Support for Giant Cell Myocarditis: A Systematic Review" Journal of Clinical Medicine 9, no. 12: 3905. https://doi.org/10.3390/jcm9123905
APA StylePatel, P. M., Saxena, A., Wood, C. T., O’Malley, T. J., Maynes, E. J., Entwistle, J. W. C., Massey, H. T., Pirlamarla, P. R., Alvarez, R. J., Cooper, L. T., Rame, J. E., & Tchantchaleishvili, V. (2020). Outcomes of Mechanical Circulatory Support for Giant Cell Myocarditis: A Systematic Review. Journal of Clinical Medicine, 9(12), 3905. https://doi.org/10.3390/jcm9123905