
Balancing Ethics and Innovation: Can Artificial Intelligence Safely Transform Emergency Surgery? A Narrative Perspective




Abstract
1. Introduction
2. Methods
3. Results
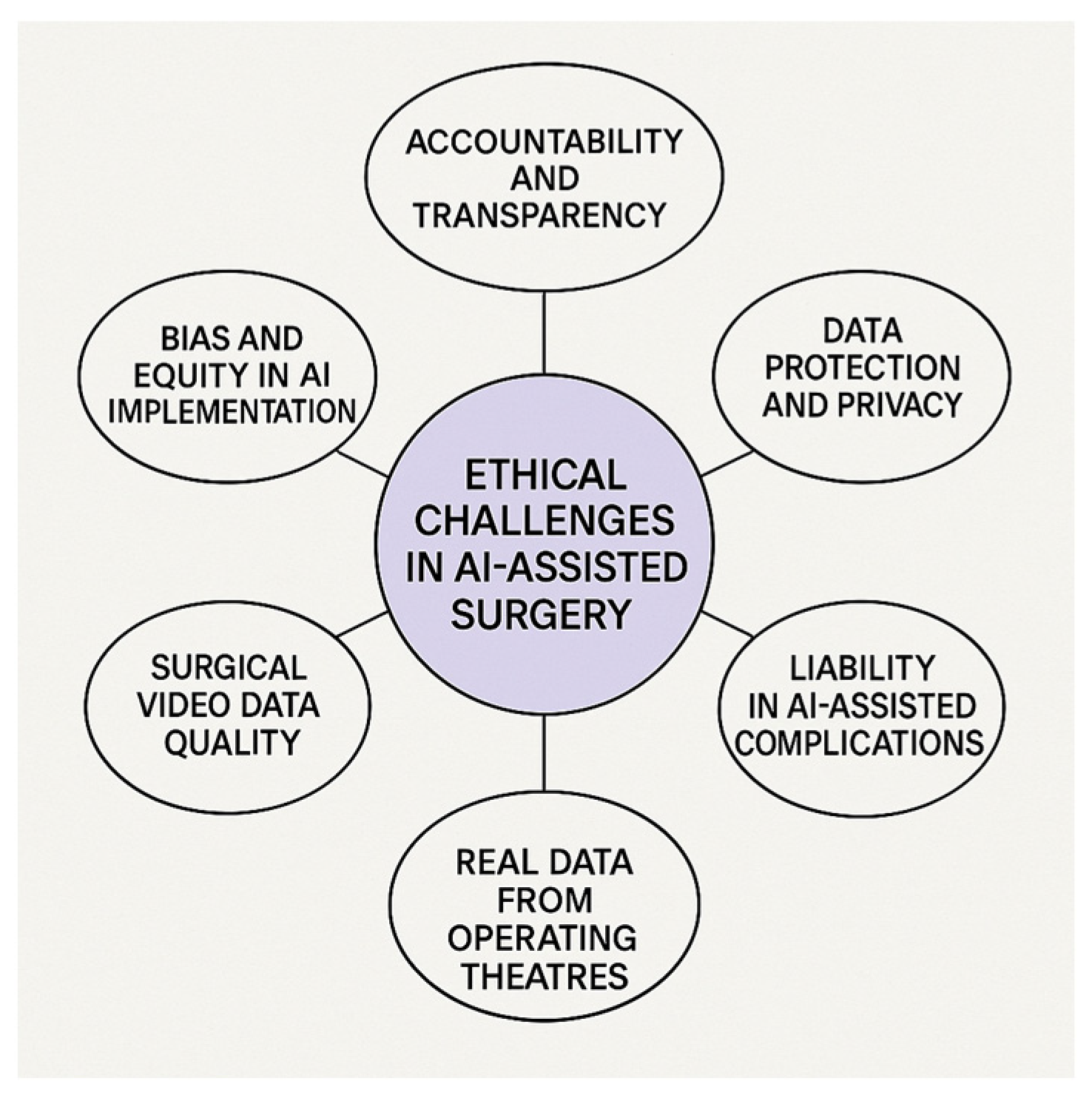
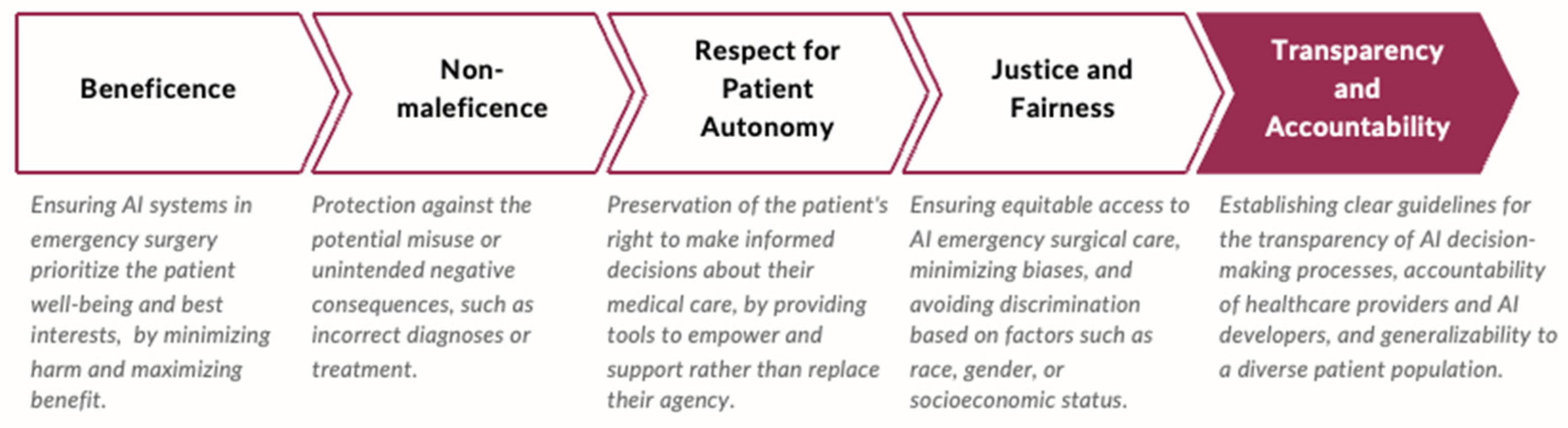
4. Ethical Considerations in AI-Assisted Emergency Surgery: Summary of Evidence and Discussion of Critical Issues for Implementation
4.1. Accountability and Transparency
4.2. Bias and Equity in AI Algorithms
4.3. Data Protection and Privacy
- Storage Capacity and Infrastructure:
- High Data Volume: Surgical procedures, especially those recorded in high-definition formats, generate substantial amounts of data. Continuous recording of all surgeries can quickly exceed existing storage capacities, necessitating significant investments in scalable storage solutions.
- Cost Implications: Maintaining and upgrading storage infrastructure to accommodate the growing volume of video data can be financially burdensome for healthcare institutions, particularly those with limited resources.
- Data Management and Accessibility:
- Efficient Retrieval: As the volume of stored video data increases, implementing effective data management systems becomes essential to ensure that relevant videos can be easily retrieved for analysis and review.
- Standardization Issues: Variations in video formats, annotations, and metadata can complicate data integration and analysis, underscoring the need for standardized protocols in video recording and storage.
- Legal and Ethical Considerations:
- Patient Privacy: Surgical videos often contain sensitive patient information. Ensuring compliance with data protection regulations, such as GDPR and HIPAA, is crucial to safeguard patient privacy and maintain trust.
- Consent and Data Ownership: Clarifying issues related to informed consent for recording and using surgical videos, as well as determining data ownership, is essential to address ethical and legal concerns.
4.4. Surgical Data Quality
4.5. Real-Time Data and Workflow in the Operating Room
4.6. Informed Consent in Emergency AI-Assisted Surgery
4.7. Regulatory and Legal Frameworks
- The issue of explainability is increasingly central to regulatory efforts. EU legislation, including the GDPR and amended Directive 2011/83 on Consumer Rights, outlines obligations for explainable AI in automated decision-making (e.g., GDPR Articles 13.2(f) and 14.2(g)) [55]. In practice, explainability entails providing clinicians with access to key information such as the following:
- The main features driving the model’s decision;
- All contributing data points;
- How features interact in the model’s logic;
- And, in some cases, the architecture of the model itself [58].
4.8. Liability in AI-Assisted Complications: Who Is Responsible?
- Supportive AI, aimed to support clinical decision-making;
- AI-assisted decision-making, which provides semi-autonomous guidance;
- Autonomous AI in predefined tasks, which automates specific surgical steps.
5. Call to Action and Clinical Recommendations for Ethical AI Implementation in Emergency Surgery
- Enhancing AI Transparency—Prioritizing the development of explainable AI (XAI) models to improve interpretability, ensuring that healthcare providers can critically assess and validate AI-generated recommendations.
- Developing Clear Communication Protocols—Standardizing the disclosure of AI involvement in patient care to maintain trust and uphold patient autonomy.
- Mitigating Bias in AI Training Data—Ensuring that AI training datasets are diverse and representative of all patient populations to prevent the exacerbation of health disparities.
- Aligning AI with Patient-Centered Care—Designing AI systems that integrate ethical considerations and patient values into their decision-making frameworks.
- Strengthening Regulatory Oversight—Establishing comprehensive legal frameworks to define AI accountability, enhance data protection, and uphold ethical standards in emergency surgical applications.
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| ML | Machine Learning |
| DL | Deep Learning |
| CV | Computer Vision |
| CNNs | Convolutional Neural Networks |
| R-CNN | Region-based Convolutional Neural Network |
| FDA | U.S. Food and Drug Administration |
| GDPR | General Data Protection Regulation |
| EU | European Union |
| MHRA | Medicines and Healthcare products Regulatory Agency |
| NMPA | National Medical Products Administration |
References
- Panossian, V.S.; Argandykov, D.; Arnold, S.C.; Gebran, A.; Paranjape, C.N.; Hwabejire, J.O.; DeWane, M.P.; Velmahos, G.C.; Kaafarani, H.M.; POTTER Validation Group. Validation of Artificial Intelligence-Based POTTER Calculator in Emergency General Surgery Patients Undergoing Laparotomy: Prospective, Bi-Institutional Study. J. Am. Coll. Surg. 2025, 240, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Gebran, A.; Vapsi, A.; Maurer, L.R.; El Moheb, M.; Naar, L.; Thakur, S.S.; Sinyard, R.; Daye, D.; Velmahos, G.C.; Bertsimas, D.; et al. POTTER-ICU: An artificial intelligence smartphone-accessible tool to predict the need for intensive care after emergency surgery. Surgery 2022, 172, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Elhaddad, M.; Hamam, S. AI-Driven Clinical Decision Support Systems: An Ongoing Pursuit of Potential. Cureus 2024, 16, e57728. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Capelli, G.; Verdi, D.; Frigerio, I.; Rashidian, N.; Ficorilli, A.; Grasso, V.; Majidi, D.; Gumbs, A.A.; Spolverato, G.; Artificial Intelligence Surgery Editorial Board Study Group on Ethics. White paper: Ethics and trustworthiness of artificial intelligence in clinical surgery. Artif. Intell. Surg. 2023, 3, 111–122. [Google Scholar] [CrossRef]
- Cobianchi, L.; Verde, J.M.; Loftus, T.J.; Piccolo, D.; Dal Mas, F.; Mascagni, P.; Garcia Vazquez, A.; Ansaloni, L.; Marseglia, G.R.; Massaro, M.; et al. Artificial Intelligence and Surgery: Ethical Dilemmas and Open Issues. J. Am. Coll. Surg. 2022, 235, 268–275. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]
- Hashimoto, D.A.; Rosman, G.; Rus, D.; Meireles, O.R. Artificial Intelligence in Surgery: Promises and Perils. Ann. Surg. 2018, 268, 70–76. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mascagni, P.; Vardazaryan, A.; Alapatt, D.; Urade, T.; Emre, T.; Fiorillo, C.; Pessaux, P.; Mutter, D.; Marescaux, J.; Costamagna, G.; et al. Artificial Intelligence for Surgical Safety: Automatic Assessment of the Critical View of Safety in Laparoscopic Cholecystectomy Using Deep Learning. Ann. Surg. 2022, 275, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Mascagni, P.; Alapatt, D.; Urade, T.; Vardazaryan, A.; Mutter, D.; Marescaux, J.; Costamagna, G.; Dallemagne, B.; Padoy, N. A Computer Vision Platform to Automatically Locate Critical Events in Surgical Videos: Documenting Safety in Laparoscopic Cholecystectomy. Ann. Surg. 2021, 274, e93–e95. [Google Scholar] [CrossRef] [PubMed]
- Shinozuka, K.; Turuda, S.; Fujinaga, A.; Nakanuma, H.; Kawamura, M.; Matsunobu, Y.; Tanaka, Y.; Kamiyama, T.; Ebe, K.; Endo, Y.; et al. Artificial intelligence software available for medical devices: Surgical phase recognition in laparoscopic cholecystectomy. Surg. Endosc. 2022, 36, 7444–7452. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Madani, A.; Namazi, B.; Altieri, M.S.; Hashimoto, D.A.; Rivera, A.M.; Pucher, P.H.; Navarrete-Welton, A.; Sankaranarayanan, G.; Brunt, L.M.; Okrainec, A.; et al. Artificial Intelligence for Intraoperative Guidance: Using Semantic Segmentation to Identify Surgical Anatomy During Laparoscopic Cholecystectomy. Ann. Surg. 2022, 276, 363–369. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Simone, B.; Abu-Zidan, F.M.; Gumbs, A.A.; Chouillard, E.; Di Saverio, S.; Sartelli, M.; Coccolini, F.; Ansaloni, L.; Collins, T.; Kluger, Y.; et al. Knowledge, attitude, and practice of artificial intelligence in emergency and trauma surgery, the ARIES project: An international web-based survey. World J. Emerg. Surg. 2022, 17, 10. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rodgers, C.M.; Ellingson, S.R.; Chatterjee, P. Open Data and transparency in artificial intelligence and machine learning: A new era of research. F1000Research 2023, 12, 387. [Google Scholar] [CrossRef]
- Angelos, P. Complications, Errors, and Surgical Ethics. World J. Surg. 2009, 33, 609–611. [Google Scholar] [CrossRef] [PubMed]
- Fosch-Villaronga, E.; Khanna, P.; Drukarch, H.; Custers, B. The Role of Humans in Surgery Automation. Int. J. Soc. Robot. 2023, 15, 563–580. [Google Scholar] [CrossRef]
- Kim, Y.S.; Park, S.H.; Lee, I.Y.; Son, G.M.; Baek, K.R. AI-driven automatic compression system for colorectal anastomosis. J. Robot. Surg. 2024, 18, 290. [Google Scholar] [CrossRef] [PubMed]
- Habli, I.; Lawton, T.; Porter, Z. Artificial intelligence in health care: Accountability and safety. Bull. World Health Organ. 2020, 98, 251–256. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Adegbesan, A.; Akingbola, A.; Aremu, O.; Adewole, O.; Amamdikwa, J.C.; Shagaya, U. From Scalpels to Algorithms: The Risk of Dependence on Artificial Intelligence in Surgery. J. Med. Surg. Public Health 2024, 3, 100140. [Google Scholar] [CrossRef]
- Shahbazi, Z.; Byun, Y.C. Analysis of the Security and Reliability of Cryptocurrency Systems Using Knowledge Discovery and Machine Learning Methods. Sensors 2022, 22, 9083. [Google Scholar] [CrossRef]
- Brożek, B.; Furman, M.; Jakubiec, M.; Kucharzyk, B. The black box problem revisited. Real and imaginary challenges for automated legal decision making. Artif. Intell. Law 2023, 32, 427–440. [Google Scholar] [CrossRef]
- Iserson, K.; Baker, E.; Bissmeyer, P.; Derse, A. Artificial Intelligence in the ED: Ethical Issues. ACEP Now 2024, 43, 6. [Google Scholar]
- Hassija, V.; Chamola, V.; Mahapatra, A.; Singal, A.; Goel, D.; Huang, K.; Scardapane, S.; Spinelli, I.; Mahmud, M.; Hussain, A. Interpreting Black-Box Models: A Review on Explainable Artificial Intelligence. Cogn. Comput. 2024, 16, 45–74. [Google Scholar] [CrossRef]
- Agarwal, R.; Bjarnadottir, M.; Rhue, L.; Dugas, M.; Crowley, K.; Clark, J.; Gao, G. Addressing algorithmic bias and the perpetuation of health inequities: An AI bias aware framework. Health Policy Technol. 2023, 12, 100702. [Google Scholar] [CrossRef]
- Prien, C.; Lincango, E.P.; Holubar, S.D. Big Data in Surgery. Surg. Clin. N. Am. 2023, 103, 219–232. [Google Scholar] [CrossRef]
- Cross, J.L.; Choma, M.A.; Onofrey, J.A. Bias in medical AI: Implications for clinical decision-making. PLoS Digit. Health 2024, 3, e0000651. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ueda, D.; Kakinuma, T.; Fujita, S.; Kamagata, K.; Fushimi, Y.; Ito, R.; Matsui, Y.; Nozaki, T.; Nakaura, T.; Fujima, N.; et al. Fairness of artificial intelligence in healthcare: Review and recommendations. jpn J. Radiol. 2024, 42, 3–15. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- The Impact of the General Data Protection Regulation (GDPR) on Artificial Intelligence. Available online: https://www.europarl.europa.eu/RegData/etudes/STUD/2020/641530/EPRS_STU(2020)641530_EN.pdf (accessed on 20 March 2025).
- World Health Organization. WHO Calls for Safe and Ethical AI for Health. 2023. Available online: https://www.who.int/news/item/16-05-2023-who-calls-for-safe-and-ethical-ai-for-health (accessed on 20 March 2025).
- Wilkinson, M.D.; Dumontier, M.; Aalbersberg, I.J.; Appleton, G.; Axton, M.; Baak, A.; Blomberg, N.; Boiten, J.W.; da Silva Santos, L.B.; Bourne, P.E.; et al. The FAIR Guiding Principles for scientific data management and stewardship. Sci. Data 2016, 3, 160018, Erratum in Sci. Data 2019, 6, 6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- van Grinsven, M.J.J.P.; van Ginneken, B.; Hoyng, C.B.; Theelen, T.; Sanchez, C.I. Fast Convolutional Neural Network Training Using Selective Data Sampling: Application to Hemorrhage Detection in Color Fundus Images. IEEE Trans. Med. Imaging 2016, 35, 1273–1284. [Google Scholar] [CrossRef]
- Eckhoff, J.A.; Rosman, G.; Altieri, M.S.; Speidel, S.; Stoyanov, D.; Anvari, M.; Meier-Hein, L.; März, K.; Jannin, P.; Pugh, C.; et al. SAGES consensus recommendations on surgical video data use, structure, and exploration (for research in artificial intelligence, clinical quality improvement, and surgical education). Surg. Endosc. 2023, 37, 8690–8707. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nyangoh Timoh, K.; Huaulme, A.; Cleary, K.; Zaheer, M.A.; Lavoué, V.; Donoho, D.; Jannin, P. A systematic review of annotation for surgical process model analysis in minimally invasive surgery based on video. Surg. Endosc. 2023, 37, 4298–4314. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meireles, O.R.; Rosman, G.; Altieri, M.S.; Carin, L.; Hager, G.; Madani, A.; Padoy, N.; Pugh, C.M.; Sylla, P.; Ward, T.M.; et al. SAGES consensus recommendations on an annotation framework for surgical video. Surg. Endosc. 2021, 35, 4918–4929. [Google Scholar] [CrossRef] [PubMed]
- Neugebauer, E.A.; Becker, M.; Buess, G.F.; Cuschieri, A.; Dauben, H.P.; Fingerhut, A.; Fuchs, K.H.; Habermalz, B.; Lantsberg, L.; Morino, M.; et al. EAES recommendations on methodology of innovation management in endoscopic surgery. Surg. Endosc. 2010, 24, 1594–1615. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Lee, J.; Park, B.; Alwusaibie, A.A.; Alfadhel, A.H.; Park, S.; Hyung, W.J.; Choi, M.-K. Rethinking Generalization Performance of Surgical Phase Recognition with Expert-Generated Annotations. arXiv 2021, arXiv:2110.11626. [Google Scholar]
- Goodman, E.D.; Patel, K.K.; Zhang, Y.; Locke, W.; Kennedy, C.J.; Mehrotra, R.; Ren, S.; Guan, M.; Zohar, O.; Downing, M.; et al. Analyzing Surgical Technique in Diverse Open Surgical Videos With Multitask Machine Learning. JAMA Surg. 2024, 159, 185–192. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, J.-D.; Chien, J.-C.; Hsu, Y.-T.; Wu, C.-T. Automatic Surgical Instrument Recognition—A Case of Comparison Study between the Faster R-CNN, Mask R-CNN, and Single-Shot Multi-Box Detectors. Appl. Sci. 2021, 11, 8097. [Google Scholar] [CrossRef]
- Jiang, K.; Pan, S.; Yang, L.; Yu, J.; Lin, Y.; Wang, H. Surgical Instrument Recognition Based on Improved YOLOv5. Appl. Sci. 2023, 13, 11709. [Google Scholar] [CrossRef]
- Sagheb, E.; Ramazanian, T.; Tafti, A.P.; Fu, S.; Kremers, W.K.; Berry, D.J.; Lewallen, D.G.; Sohn, S.; Maradit Kremers, H. Use of Natural Language Processing Algorithms to Identify Common Data Elements in Operative Notes for Knee Arthroplasty. J. Arthroplast. 2021, 36, 922–926. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Birkhoff, D.C.; van Dalen, A.S.H.M.; Schijven, M.P. A Review on the Current Applications of Artificial Intelligence in the Operating Room. Surg. Innov. 2021, 28, 611–619. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Simone, B.; Agnoletti, V.; Abu-Zidan, F.M.; Biffl, W.L.; Moore, E.E.; Chouillard, E.; Coccolini, F.; Sartelli, M.; Podda, M.; Di Saverio, S.; et al. The Operating Room management for emergency Surgical Activity (ORSA) study: A WSES international survey. Updates Surg. 2024, 76, 687–698. [Google Scholar] [CrossRef] [PubMed]
- De Simone, B.; Kluger, Y.; Moore, E.E.; Sartelli, M.; Abu-Zidan, F.M.; Coccolini, F.; Ansaloni, L.; Tebala, G.D.; Di Saverio, S.; Di Carlo, I.; et al. The new timing in acute care surgery (new TACS) classification: A WSES Delphi consensus study. World J. Emerg. Surg. 2023, 18, 32. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tony Peregrin. Black Box Technology Shines Light on Improving OR Safety, Efficiency. 2023. Available online: https://www.facs.org/for-medical-professionals/news-publications/news-and-articles/bulletin/2023/july-2023-volume-108-issue-7/black-box-technology-shines-light-on-improving-or-safety-efficiency/ (accessed on 20 March 2025).
- Mascagni, P.; Padoy, N. OR black box and surgical control tower: Recording and streaming data and analytics to improve surgical care. J. Visc. Surg. 2021, 158, S18–S25. [Google Scholar] [CrossRef] [PubMed]
- Bai, N. ‘Black Boxes’ in Stanford Hospital Operating Rooms aid Training and Safety. Stanford Medicine News Center, 28 September 2022. Available online: https://med.stanford.edu/news/all-news/2022/09/black-box-surgery.html (accessed on 24 May 2023).
- Jung, J.J.; Jüni, P.; Lebovic, G.; Grantcharov, T. First-year Analysis of the Operating Room Black Box Study. Ann. Surg. 2020, 271, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.K.; Abreu, A.A.; Zeh, H.J.; Daniel, W.C.; Palter, V.N.; Bishop, S.J.; Sims, S.; Odeh, J.M.; Evans, K.; Dandekar, P.; et al. Using OR Black Box Technology to Determine Quality Improvement Outcomes for In-situ Timeout and Debrief Simulation. Ann. Surg. 2024. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Rai, A.; Beland, L.; Aro, T.; Jarrett, M.; Kavoussi, L. Patient Safety in the Operating Room During Urologic Surgery: The OR Black Box Experience. World J. Surg. 2021, 45, 3306–3312. [Google Scholar] [CrossRef] [PubMed]
- Golany, T.; Aides, A.; Freedman, D.; Rabani, N.; Liu, Y.; Rivlin, E.; Corrado, G.S.; Matias, Y.; Khoury, W.; Kashtan, H.; et al. Artificial intelligence for phase recognition in complex laparoscopic cholecystectomy. Surg. Endosc. 2022, 36, 9215–9223. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Deol, E.S.; Henning, G.; Basourakos, S.; Vasdev, R.M.S.; Sharma, V.; Kavoussi, N.L.; Karnes, R.J.; Leibovich, B.C.; Boorjian, S.A.; Khanna, A. Artificial intelligence model for automated surgical instrument detection and counting: An experimental proof-of-concept study. Patient Saf. Surg. 2024, 18, 24. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Park, H.J. Patient perspectives on informed consent for medical AI: A web-based experiment. Digit Health 2024, 10, 20552076241247938. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kituuka, O.; Munabi, I.G.; Mwaka, E.S.; Galukande, M.; Harris, M.; Sewankambo, N. Informed consent process for emergency surgery: A scoping review of stakeholders’ perspectives, challenges, ethical concepts, and policies. SAGE Open Med. 2023, 11, 20503121231176666. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Teasdale, A.; Mills, L.; Costello, R. Artificial Intelligence-Powered Surgical Consent: Patient Insights. Cureus 2024, 16, e68134. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Harishbhai Tilala, M.; Kumar Chenchala, P.; Choppadandi, A.; Kaur, J.; Naguri, S.; Saoji, R.; Devaguptapu, B. Ethical Considerations in the Use of Artificial Intelligence and Machine Learning in Health Care: A Comprehensive Review. Cureus 2024, 16, e62443. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Artificial Intelligence and Machine Learning (AI/ML)-Enabled Medical Devices. Available online: https://www.fda.gov/medical-devices/software-medical-device-samd/artificial-intelligence-and-machine-learning-aiml-enabled-medical-devices (accessed on 20 March 2025).
- World Health Organization. WHO Outlines Considerations for Regulation of Artificial Intelligence for Health. 2023. Available online: https://www.who.int/news/item/19-10-2023-who-outlines-considerations-for-regulation-of-artificial-intelligence-for-health (accessed on 20 March 2025).
- EU AI Act: First Regulation on Artificial Intelligence. Topics European Parliament. 2023. Available online: https://www.europarl.europa.eu/topics/en/article/20230601STO93804/eu-ai-act-first-regulation-on-artificial-intelligence (accessed on 20 March 2025).
- Directive 2011/83/EU of the European Parliament and of the Council of 25 October 2011 on Consumer Rights, Amending Council Directive 93/13/EEC and Directive 1999/44/EC of the European Parliament and of the Council and Repealing Council Directive 85/577/EEC and Directive 97/7/EC of the European Parliament and of the Council Text with EEA Relevance. Available online: https://eur-lex.europa.eu/eli/dir/2011/83/oj/eng (accessed on 20 March 2025).
- Bibal, A.; Lognoul, M.; De Streel, A.; Frénay, B. Legal requirements on explainability in machine learning. Artif. Intell. Law 2021, 29, 149–169. [Google Scholar] [CrossRef]
- Ahuja, A.S. The impact of artificial intelligence in medicine on the future role of the physician. PeerJ 2019, 7, e7702. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Maleki Varnosfaderani, S.; Forouzanfar, M. The Role of AI in Hospitals and Clinics: Transforming Healthcare in the 21st Century. Bioengineering 2024, 11, 337. [Google Scholar] [CrossRef]
- Cestonaro, C.; Delicati, A.; Marcante, B.; Caenazzo, L.; Tozzo, P. Defining medical liability when artificial intelligence is applied on diagnostic algorithms: A systematic review. Front. Med. 2023, 10, 1305756. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eldakak, A.; Alremeithi, A.; Dahiyat, E.; El-Gheriani, M.; Mohamed, H.; Abdulrahim Abdulla, M.I. Civil liability for the actions of autonomous AI in healthcare: An invitation to further contemplation. Humanit. Soc. Sci. Commun. 2024, 11, 305. [Google Scholar] [CrossRef]
- Brandenburg, J.M.; Müller-Stich, B.P.; Wagner, M.; van der Schaar, M. Can surgeons trust AI? Perspectives on machine learning in surgery and the importance of eXplainable Artificial Intelligence (XAI). Langenbeck’s Arch. Surg. 2025, 410, 53. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- OECD AI Principles Overview. Available online: https://oecd.ai/en/ai-principles (accessed on 20 March 2025).
- The GPAI Initiative and OECD Work on AI Have Joined Forces Under the GPAI Brand to Create an Integrated Partnership. GPAI Work Is Now Available on the OECD AI Policy Observatory. Available online: https://gpai.ai/ (accessed on 20 March 2025).
- De Simone, B.; Chouillard, E.; Gumbs, A.A.; Loftus, T.J.; Kaafarani, H.; Catena, F. Artificial intelligence in surgery: The emergency surgeon’s perspective (the ARIES project). Discov. Health Syst. 2022, 1, 9. [Google Scholar] [CrossRef]
- De Simone, B.; Di Saverio, S. Invited Commentary: Artificial Intelligence in Surgical Care: We Must Overcome Ethical Boundaries. J. Am. Coll. Surg. 2022, 235, 275–277. [Google Scholar] [CrossRef]
- De Simone, B.; Kluger, Y.; Moore, E.E.; Di Saverio, S.; Sartelli, M.; Ansaloni, L.; Coccolini, F.; Biffl, W.L.; Catena, F. The WSES: What do we see in the future? World J. Emerg. Surg. 2021, 16, 13. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Simone, B.; Abu-Zidan, F.M.; Saeidi, S.; Deeken, G.; Biffl, W.L.; Moore, E.E.; Sartelli, M.; Coccolini, F.; Ansaloni, L.; Di Saverio, S.; et al. Knowledge, attitudes and practices of using Indocyanine Green (ICG) fluorescence in emergency surgery: An international web-based survey in the ARtificial Intelligence in Emergency and trauma Surgery (ARIES)-WSES project. Updates Surg. 2024, 76, 1969–1981. [Google Scholar] [CrossRef] [PubMed]
- De Simone, B.; Abu-Zidan, F.M.; Boni, L.; Castillo, A.M.G.; Cassinotti, E.; Corradi, F.; Di Maggio, F.; Ashraf, H.; Baiocchi, G.L.; Tarasconi, A.; et al. Indocyanine green fluorescence-guided surgery in the emergency setting: The WSES international consensus position paper. World J. Emerg. Surg. 2025, 20, 13. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Saeidi, H.; Opfermann, J.D.; Kam, M.; Wei, S.; Léonard, S.; Hsieh, M.H. Autonomous robotic laparoscopic surgery for intestinal anastomosis. Sci. Robot. 2022, 7, eabj2908. [Google Scholar] [PubMed]
- Shademan, A.; Decker, R.S.; Opfermann, J.D.; Leonard, S.; Krieger, A.; Kim, P.C. Supervised autonomous robotic soft tissue surgery. Sci. Transl. Med. 2016, 8, 337ra64. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Study Focus | Setting | Key Ethical or Clinical Implications |
|---|---|---|---|
| Panossian et al. (2025) [1] | Validation of AI-based risk calculator in emergency laparotomy | Emergency Surgery | Accountability, clinical reliability |
| Gebran et al. (2022) [2] | AI tool to predict ICU need after emergency surgery | Emergency Surgery | Predictive validity, clinical utility |
| Elhaddad and Hamam (2024) [3] | Review on AI-driven clinical decision-support systems | General Healthcare | Potential vs. limitations of AI in decision-making |
| Capelli et al. (2023) [4] | White paper on ethics and trust in AI-assisted surgery | Clinical Surgery | Trustworthiness, transparency |
| Cobianchi et al. (2022) [5] | Ethical dilemmas of AI in surgery | General Surgery | Bias, autonomy, data governance |
| Hashimoto et al. (2018) [7] | Promises and perils of AI in surgery | General Surgery | Technological optimism, black box concerns |
| Mascagni et al. (2022) [8] | AI for surgical safety: critical view assessment | Laparoscopic Surgery | AI-driven safety enhancement |
| Mascagni et al. (2021) [9] | Computer vision for detecting surgical events | Laparoscopic Surgery | Video annotation and decision support |
| Shinozuka et al. (2022) [10] | AI for surgical phase recognition | Laparoscopic Surgery | Workflow optimization, data use |
| Madani et al. (2022) [11] | Semantic segmentation for intraoperative guidance | Laparoscopic Surgery | Surgical anatomy identification |
| De Simone et al. (2022) [12] | Global survey about AI-assisted implementation in emergency surgical practices | Emergency Surgery | Knowledge, attitudes, perspectives, and barriers perceived by emergency surgeons to AI-driven tool implementation in the emergency setting |
| Regulatory Body | Region | Key AI Guidelines | Major Challenges |
|---|---|---|---|
| FDA (U.S.) | United States | AI/ML-based surgical tools must undergo premarket approval (PMA) or 510(k) clearance. | Lack of standardized AI-specific rules; most AI tools classified as decision-support rather than autonomous systems. |
| GDPR (EU) | European Union | Focuses on data privacy, informed consent, and algorithmic transparency. | No clear AI-specific medical regulations; AI explainability requirements are still evolving. |
| EU AI Act | European Union | First global AI regulatory framework, categorizing AI applications based on risk levels (minimal, high, unacceptable). | Surgical AI could be classified as “high risk”, requiring stringent validation and real-time monitoring. |
| WHO AI Ethics Framework | Global | Calls for ethical AI integration with principles of trustworthiness, fairness, and transparency. | Non-binding recommendations; lacks enforcement mechanisms for individual countries. |
| MHRA (UK) | United Kingdom | Requires AI as a Medical Device (AIaMD) to meet CE marking for safety and performance. | Post-market AI monitoring is weak, making it difficult to detect AI-related adverse events in real time. |
| China NMPA AI Regulations | China | Encourages AI in healthcare but requires strict cybersecurity measures and data localization. | AI models must be trained on Chinese patient data, limiting generalizability across global populations. |
| AI Role | Description | Case Example in Emergency Surgery | Ethical and Practical Considerations |
|---|---|---|---|
| AI as a Decision-Support Tool (Assistive AI) | Provides real-time data analysis, risk assessment, and decision-making support without making autonomous choices. | POTTER Calculator predicts postoperative mortality and complications in emergency general surgery, improving triage and resource allocation. | Surgeons retain full control; AI acts as an augmentation tool to reduce cognitive load. Trust and interpretability (XAI) are key. |
| AI-Assisted Decision-Making (Semi-Autonomous AI) | AI suggests interventions based on real-time surgical video, patient data, or intraoperative findings. The final decision remains with the surgeon. | Computer vision evaluates intestinal perfusion via ICG fluorescence imaging, aiding in anastomotic leak prevention. | AI requires explainability and surgeon oversight. If AI misinterprets perfusion, who is responsible? There is a lack of clear medico-legal guidelines. |
| AI-Enabled Automation (Task-Specific AI) | AI executes predefined actions autonomously within a controlled scope. | AI-powered automatic staplers (e.g., Medtronic Signia™) adjust stapling depth and compression based on tissue thickness sensors, reducing human error in colorectal anastomosis. | This event requires human intervention in case of AI failure. If a staple misfires, is it a surgeon’s or manufacturer’s responsibility? There are not clear regulations on it. |
| Fully Autonomous AI Surgery (Future Concept) | AI performs entire surgical procedures autonomously without direct human input. | STAR Robot (Smart Tissue Autonomous Robot) successfully performed soft-tissue anastomosis in a porcine model with greater precision than human surgeons. | Not yet ethically or legally acceptable in humans. Requires new regulatory frameworks to define accountability and patient consent. |
| Scenario | Example | Liability Considerations |
|---|---|---|
| AI as a Decision-Support Tool (Assistive AI) | POTTER calculator underestimates a patient’s risk, leading to an anastomosis that fails instead of a safer Hartmann’s procedure. | The surgeon retains final decision-making authority, so primary liability falls on the clinician. However, if AI models were trained on biased datasets, legal responsibility may extend to developers and institutions. |
| AI-Assisted Surgical Decision-Making | AI misinterprets ICG fluorescence imaging and fails to detect ischemia before an anastomosis, leading to a leak. | If the surgeon over-relied on AI despite conflicting clinical findings, they may share liability. However, if AI misdiagnosis results from algorithmic failure, the AI vendor could be held accountable under product liability laws. |
| AI-Enabled Automation (Task-Specific AI) | AI-powered stapler malfunctions and misfires, causing anastomotic dehiscence. | Product liability law applies—manufacturer is responsible for device failure unless the surgeon misused the device against recommendations. AI safety validation is crucial. |
| Ethical Issue | Clinical Recommendation |
|---|---|
| Informed Consent in Emergency Settings | Implement standardized protocols to inform patients or their proxies about AI involvement during emergency procedures. |
| Explainability and Transparency | Adopt explainable AI tools to ensure clinicians can interpret and validate system outputs in real time. |
| Bias and Equity in AI Models | Ensure diverse and representative datasets are used to train AI, reducing bias across populations. |
| Liability in AI-Assisted Complications | Develop shared responsibility models between surgeons, institutions, and AI developers for adverse outcomes. |
| Surgical Video Data Governance | Follow ethical and legal frameworks (e.g., GDPR, HIPAA) for storage, use, and consent of surgical video data. |
| Workflow Integration in Emergency Surgery | Use AI tools to support—rather than replace—surgeon decision-making; maintain human oversight during intraoperative use. |
| Data Quality and Annotation | Promote the prospective collection of high-quality clinical data and intraoperative images through standardized acquisition protocols, expert-validated annotation, and interoperability between centers. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Simone, B.; Deeken, G.; Catena, F. Balancing Ethics and Innovation: Can Artificial Intelligence Safely Transform Emergency Surgery? A Narrative Perspective. J. Clin. Med. 2025, 14, 3111. https://doi.org/10.3390/jcm14093111
De Simone B, Deeken G, Catena F. Balancing Ethics and Innovation: Can Artificial Intelligence Safely Transform Emergency Surgery? A Narrative Perspective. Journal of Clinical Medicine. 2025; 14(9):3111. https://doi.org/10.3390/jcm14093111
Chicago/Turabian StyleDe Simone, Belinda, Genevieve Deeken, and Fausto Catena. 2025. "Balancing Ethics and Innovation: Can Artificial Intelligence Safely Transform Emergency Surgery? A Narrative Perspective" Journal of Clinical Medicine 14, no. 9: 3111. https://doi.org/10.3390/jcm14093111
APA StyleDe Simone, B., Deeken, G., & Catena, F. (2025). Balancing Ethics and Innovation: Can Artificial Intelligence Safely Transform Emergency Surgery? A Narrative Perspective. Journal of Clinical Medicine, 14(9), 3111. https://doi.org/10.3390/jcm14093111