
Sex-Specific Differences in Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty

 , , , , ,
, , , , ,  , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Statistical Analysis
3. Results
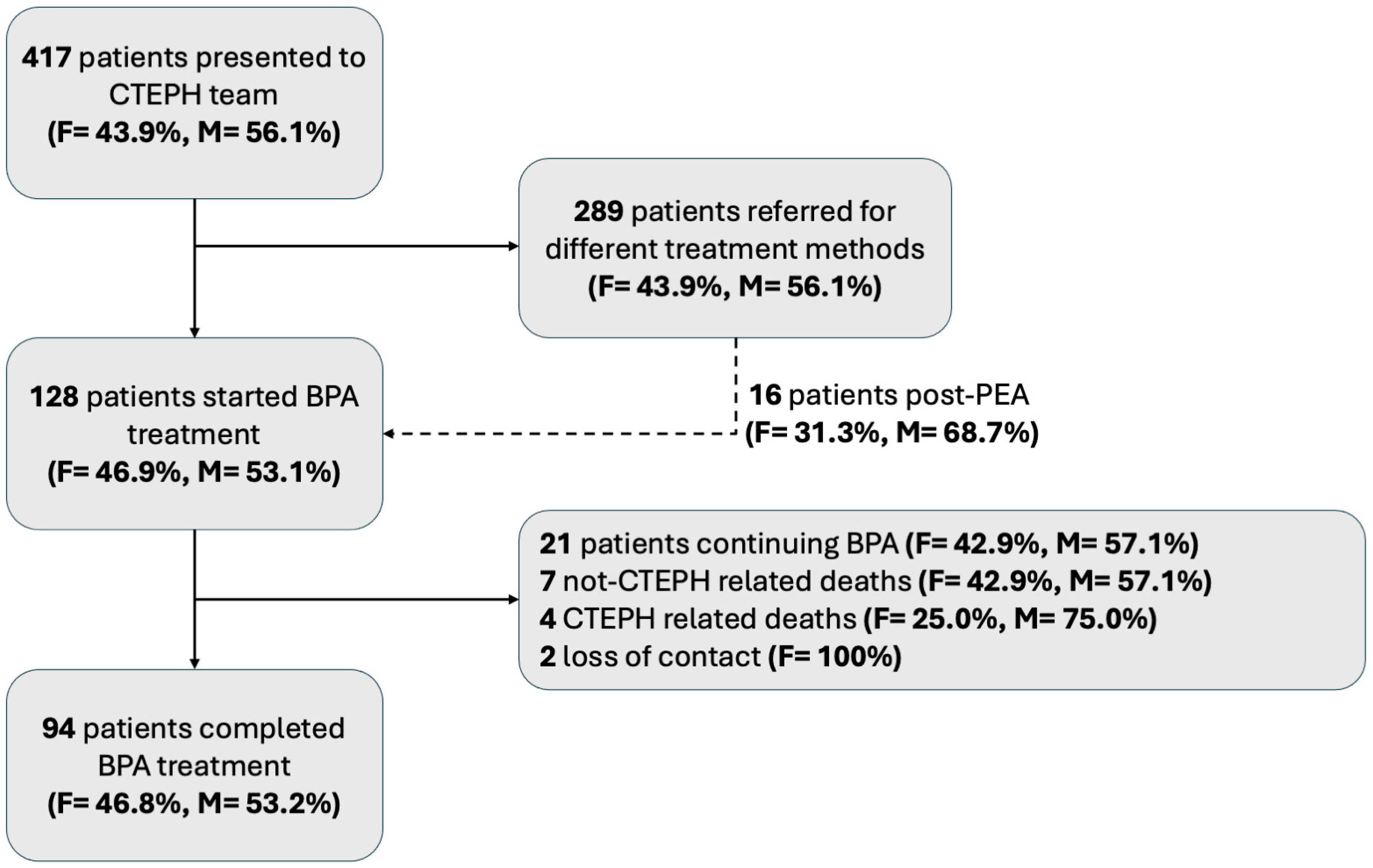
3.1. Patients
3.2. Evaluation at Baseline
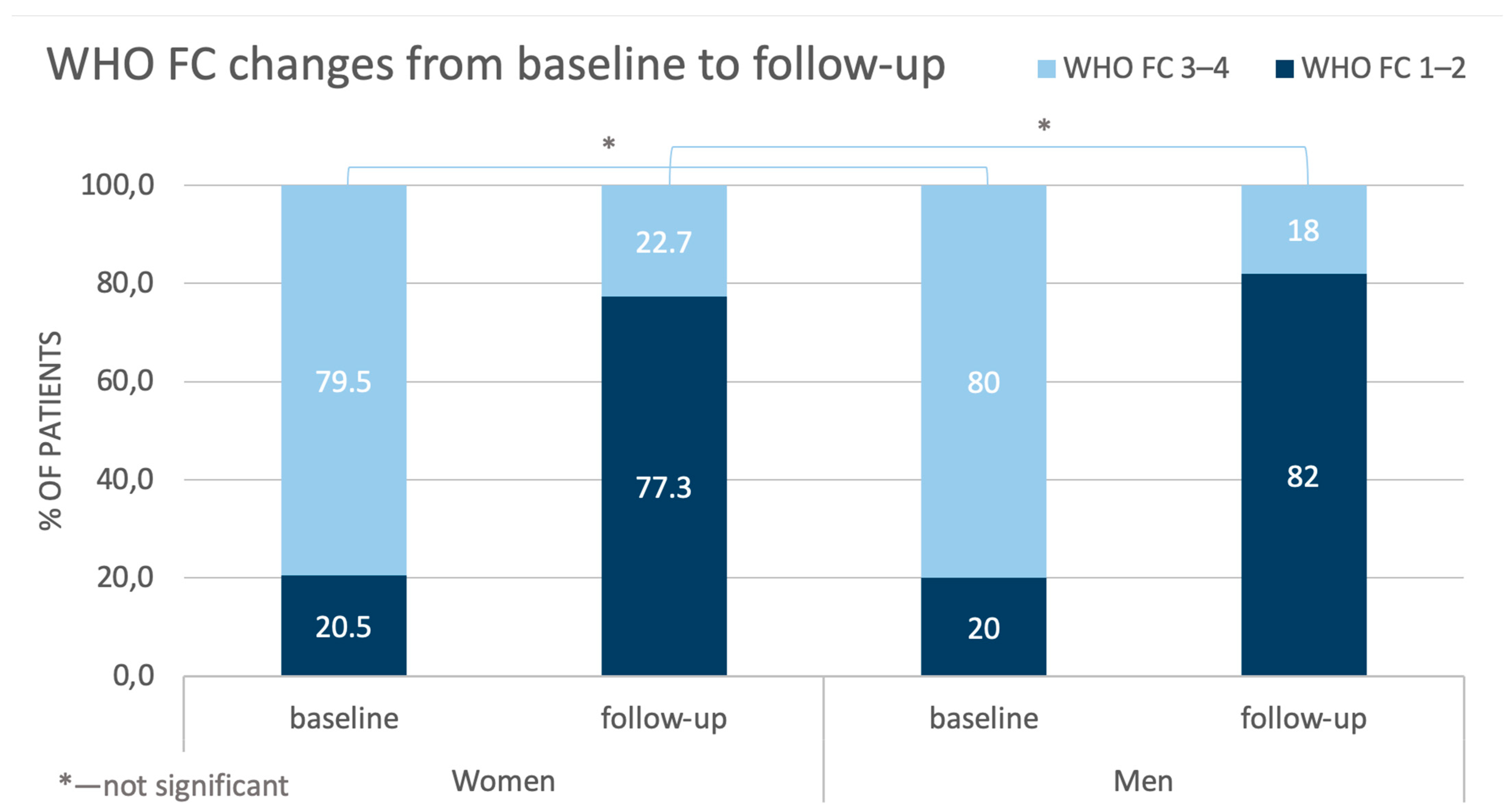
3.3. Evaluation at Follow-Up
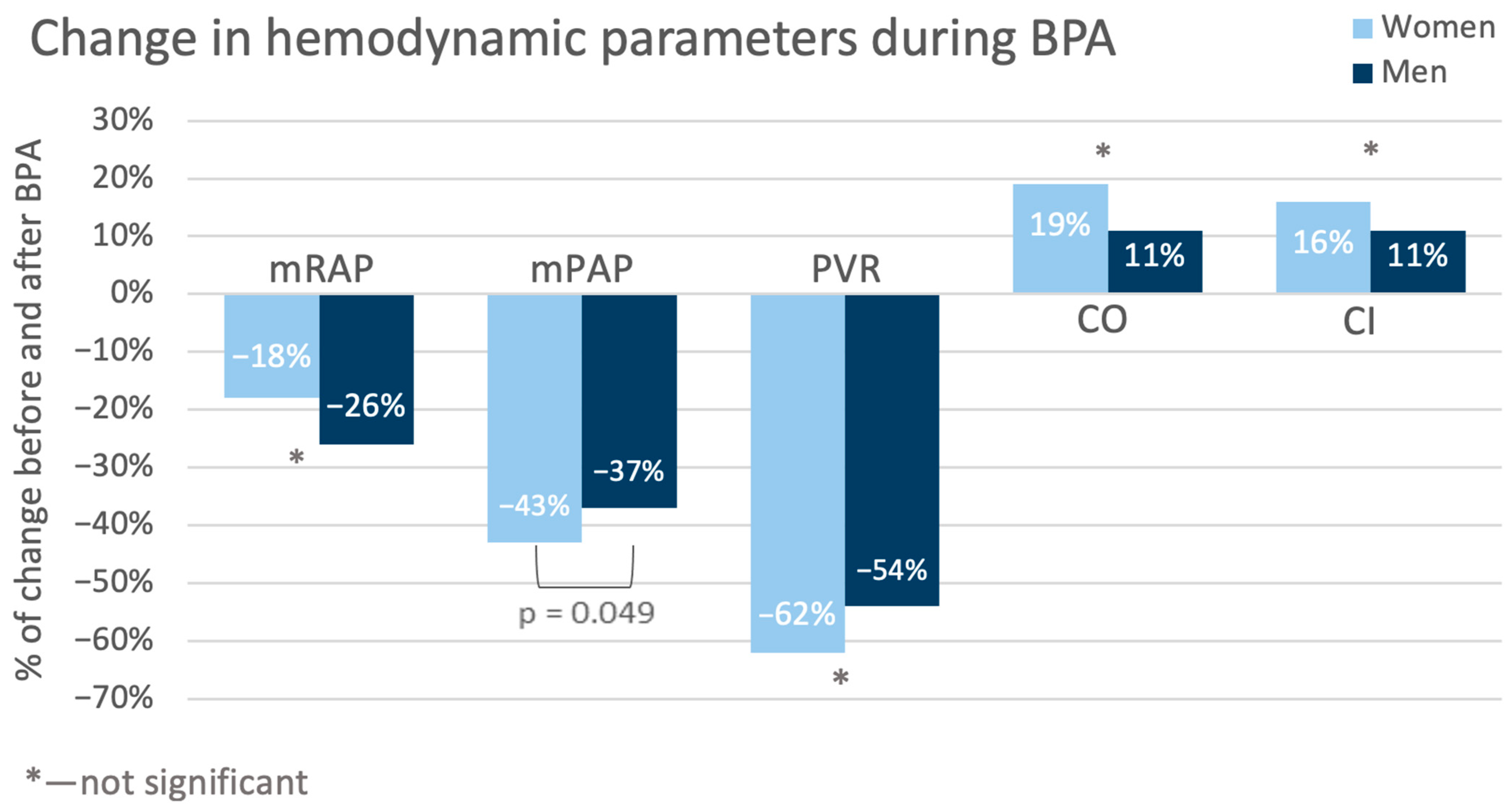
3.4. Treatment Outcomes
4. Discussion
Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BPA | balloon pulmonary angioplasty |
| CTEPH | chronic thrombo-embolic pulmonary hypertension |
| CVD | cardiovascular diseases |
| RHC | right heart catherization |
| PEA | pulmonary endarterectomy |
| 6-MWT | 6 min walking test |
| NT-proBNP | N-terminal pro-B-type natriuretic peptide |
| M | male |
| F | female |
| BMI | body mass index |
| DOAC | direct oral anticoagulants |
| PH | pulmonary hypertension |
| SD | standard deviation |
| VKA | vitamin K antagonists |
| LMWH | low-molecular-weight heparin |
| WHO FC | World Health Organization functional class |
| mRAP | mean right atrial pressure |
| sPAP | systolic pulmonary arterial pressure |
| dPAP | diastolic pulmonary arterial pressure |
| mPAP | mean pulmonary artery pressure |
| PCWP | pulmonary capillary wedge pressure |
| CI | cardiac index |
| SV | stroke volume |
| SVI | stroke volume index |
| PVR | pulmonary vascular resistance |
| IQR | interquartile range |
| COPD | chronic obstructive pulmonary disease |
References
- Mensah, G.A.; Fuster, V. Sex and Gender Differences in Cardiovascular Health. J. Am. Coll. Cardiol. 2022, 79, 1385–1387. [Google Scholar] [CrossRef] [PubMed]
- Ghofrani, H.-A.; Galiè, N.; Grimminger, F.; Grünig, E.; Humbert, M.; Jing, Z.-C.; Keogh, A.M.; Langleben, D.; Kilama, M.O.; Fritsch, A.; et al. Riociguat for the Treatment of Pulmonary Arterial Hypertension. N. Engl. J. Med. 2013, 369, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.S.; Blair, C.; Oudiz, R.J.; Dufton, C.; Olschewski, H.; Despain, D.; Gillies, H.; Kawut, S.M. Baseline and Follow-up 6-Min Walk Distance and Brain Natriuretic Peptide Predict 2-Year Mortality in Pulmonary Arterial Hypertension. Chest 2013, 143, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; D’Armini, A.M.; Grimminger, F.; Grünig, E.; Hoeper, M.M.; Jansa, P.; Mayer, E.; Neurohr, C.; Simonneau, G.; Torbicki, A.; et al. Haemodynamic Effects of Riociguat in Inoperable/Recurrent Chronic Thromboembolic Pulmonary Hypertension. Heart 2017, 103, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Nathan, S.D.; Behr, J.; Collard, H.R.; Cottin, V.; Hoeper, M.M.; Martinez, F.J.; Corte, T.J.; Keogh, A.M.; Leuchte, H.; Mogulkoc, N.; et al. Riociguat for Idiopathic Interstitial Pneumonia-Associated Pulmonary Hypertension (RISE-IIP): A Randomised, Placebo-Controlled Phase 2b Study. Lancet Respir. Med. 2019, 7, 780–790. [Google Scholar] [CrossRef]
- Pugh, M.E.; Hemnes, A.R. Pulmonary Hypertension in Women. Expert. Rev. Cardiovasc. Ther. 2010, 8, 1549–1558. [Google Scholar] [CrossRef]
- Mair, K.M.; Johansen, A.K.Z.; Wright, A.F.; Wallace, E.; Maclean, M.R. Pulmonary Arterial Hypertension: Basis of Sex Differences in Incidence and Treatment Response. Br. J. Pharmacol. 2014, 171, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Leber, L.; Beaudet, A.; Muller, A. Epidemiology of Pulmonary Arterial Hypertension and Chronic Thromboembolic Pulmonary Hypertension: Identification of the Most Accurate Estimates from a Systematic Literature Review. Pulm. Circ. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Delcroix, M.; Torbicki, A.; Gopalan, D.; Sitbon, O.; Klok, F.A.; Lang, I.; Jenkins, D.; Kim, N.H.; Humbert, M.; Jais, X.; et al. ERS Statement on Chronic Thromboembolic Pulmonary Hypertension. Eur. Respir. J. 2021, 57, 2002828. [Google Scholar] [CrossRef] [PubMed]
- Kramm, T.; Wilkens, H.; Fuge, J.; Schäfers, H.J.; Guth, S.; Wiedenroth, C.B.; Weingard, B.; Huscher, D.; Pittrow, D.; Cebotari, S.; et al. Incidence and Characteristics of Chronic Thromboembolic Pulmonary Hypertension in Germany. Clin. Res. Cardiol. 2018, 107, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.M.; Andreassen, A.K.; Andersen, A.; Bouvaist, H.; Coghlan, G.; Escribano-Subias, P.; Jansa, P.; Kopec, G.; Kurzyna, M.; Matsubara, H.; et al. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: A Clinical Consensus Statement of the ESC Working Group on Pulmonary Circulation and Right Ventricular Function. Eur. Heart J. 2023, 44, 2659–2671. [Google Scholar] [CrossRef] [PubMed]
- Araszkiewicz, A.; Darocha, S.; Pietrasik, A.; Pietura, R.; Jankiewicz, S.; Banaszkiewicz, M.; Sławek-Szmyt, S.; Biederman, A.; Mularek-Kubzdela, T.; Lesiak, M.; et al. Balloon Pulmonary Angioplasty for the Treatment of Residual or Recurrent Pulmonary Hypertension after Pulmonary Endarterectomy. Int. J. Cardiol. 2019, 278, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Darocha, S.; Pietura, R.; Pietrasik, A.; Norwa, J.; Dobosiewicz, A.; Piłka, M.; Florczyk, M.; Biederman, A.; Torbicki, A.; Kurzyna, M. Improvement in Quality of Life and Hemodynamics in Chronic Thromboembolic Pulmonary Hypertension Treated With Balloon Pulmonary Angioplasty. Circ. J. 2017, 81, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Martinez, C.; Wallenhorst, C.; Teal, S.; Cohen, A.T.; Peacock, A.J. Incidence and Risk Factors of Chronic Thromboembolic Pulmonary Hypertension Following Venous Thromboembolism, a Population-Based Cohort Study in England. Pulm. Circ. 2018, 8, 2045894018791358. [Google Scholar] [CrossRef]
- Barco, S.; Klok, F.A.; Konstantinides, S.V.; Dartevelle, P.; Fadel, E.; Jenkins, D.; Kim, N.H.; Madani, M.; Matsubara, H.; Mayer, E.; et al. Sex-Specific Differences in Chronic Thromboembolic Pulmonary Hypertension. Results from the European CTEPH Registry. J. Thromb. Haemost. 2020, 18, 151–161. [Google Scholar] [CrossRef]
- Kurzyna, M.; Araszkiewicz, A.; Błaszczak, P.; Grabka, M.; Hawranek, M.; Kopec, G.; Mroczek, E.; Zembala, M.; Torbicki, A.; Ochała, A. Summary of Recommendations for the Haemodynamic and Angiographic Assessment of the Pulmonary Circulation. Joint Statement of the Polish Cardiac Society’s Working Group on Pulmonary Circulation and Association of Cardiovascular Interventions. Pol. Heart J. (Kardiol. Pol.) 2015, 73, 63–68. [Google Scholar] [CrossRef]
- Siennicka, A.; Darocha, S.; Banaszkiewicz, M.; Kędzierski, P.; Dobosiewicz, A.; Błaszczak, P.; Peregud-Pogorzelska, M.; Kasprzak, J.D.; Tomaszewski, M.; Mroczek, E.; et al. Treatment of Chronic Thromboembolic Pulmonary Hypertension in a Multidisciplinary Team. Ther. Adv. Respir. Dis. 2019, 13, 1753466619891529. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, A.; Satoh, T.; Fukuda, T.; Sugimura, K.; Fukumoto, Y.; Emoto, N.; Yamada, N.; Yao, A.; Ando, M.; Ogino, H.; et al. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: Results of a Multicenter Registry. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e004029. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef]
- Mizoguchi, H.; Ogawa, A.; Munemasa, M.; Mikouchi, H.; Ito, H.; Matsubara, H. Refined Balloon Pulmonary Angioplasty for Inoperable Patients with Chronic Thromboembolic Pulmonary Hypertension. Circ. Cardiovasc. Interv. 2012, 5, 748–755. [Google Scholar] [CrossRef]
- Medrek, S.; Safdar, Z. Epidemiology and Pathophysiology of Chronic Thromboembolic Pulmonary Hypertension: Risk Factors and Mechanisms. Methodist. Debakey Cardiovasc. J. 2016, 12, 195–198. [Google Scholar] [CrossRef]
- Guth, S.; D’armini, A.M.; Delcroix, M.; Nakayama, K.; Fadel, E.; Hoole, S.P.; Jenkins, D.P.; Kiely, D.G.; Kim, N.H.; Lang, I.M.; et al. Current Strategies for Managing Chronic Thromboembolic Pulmonary Hypertension: Results of the Worldwide Prospective CTEPH Registry. ERJ Open Res. 2021, 7, 00850-2020. [Google Scholar] [CrossRef] [PubMed]
- Öngen, H.G.; Akdeniz, B.; Düzenli, M.A.; Chernyavsky, A.; Dabar, G.; Idrees, M.; Khludeeva, E.; Kültürsay, H.; Lukianchikova, V.; Martynyuk, T.; et al. Diagnosis and Treatment Patterns of Chronic Thromboembolic Pulmonary Hypertension in Russia, Kazakhstan, Turkey, Lebanon, and Saudi Arabia: A Registry Study. Drugs Real World Outcomes 2024, 11, 149–165. [Google Scholar] [CrossRef] [PubMed]
- Bambrick, M.; Grafham, G.; Lajkosz, K.; Donahoe, L.; de Perrot, M.; McInnis, M. Computed Tomography Identifies Sex-Specific Differences in Surgical Chronic Thromboembolic Pulmonary Hypertension. JHLT Open 2024, 6, 100130. [Google Scholar] [CrossRef]
- Chan, J.C.Y.; Man, H.S.J.; Asghar, U.M.; McRae, K.; Zhao, Y.; Donahoe, L.L.; Wu, L.; Granton, J.; de Perrot, M. Impact of Sex on Outcome after Pulmonary Endarterectomy for Chronic Thromboembolic Pulmonary Hypertension. J. Heart Lung Transplant. 2023, 42, 1578–1586. [Google Scholar] [CrossRef] [PubMed]
- Martin, Y.N.; Pabelick, C.M. Sex Differences in the Pulmonary Circulation: Implications for Pulmonary Hypertension. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H1253. [Google Scholar] [CrossRef] [PubMed]
- Bonderman, D.; Wilkens, H.; Wakounig, S.; Schäfers, H.J.; Jansa, P.; Lindner, J.; Simkova, I.; Martischnig, A.M.; Dudczak, J.; Sadushi, R.; et al. Risk Factors for Chronic Thromboembolic Pulmonary Hypertension. Eur. Respir. J. 2009, 33, 325–331. [Google Scholar] [CrossRef]
- Kerr, K.M.; Elliott, C.G.; Chin, K.; Benza, R.L.; Channick, R.N.; Davis, R.D.; He, F.; LaCroix, A.; Madani, M.M.; McLaughlin, V.V.; et al. Results From the United States Chronic Thromboembolic Pulmonary Hypertension Registry: Enrollment Characteristics and 1-Year Follow-Up. Chest 2021, 160, 1822–1831. [Google Scholar] [CrossRef] [PubMed]
- Souza, F.S.d.F.; Ferreira, M.G.; Melo, I.A.; de Sá, M.F.L.; Loureiro, C.M.C.; Abreu, R.; de Carvalho, P.H.A.; Viana, M.d.S.; Oliveira, V.; Ritt, L.E.F. Balloon Pulmonary Angioplasty in Patients with Chronic Thromboembolic Pulmonary Hypertension: Short- and Long-Term Results from a Cohort in Brazil. J. Bras. Pneumol. 2025, 50, e20240147. [Google Scholar] [CrossRef] [PubMed]
- Olsson, K.M.; Wiedenroth, C.B.; Kamp, J.C.; Breithecker, A.; Fuge, J.; Krombach, G.A.; Haas, M.; Hamm, C.; Kramm, T.; Guth, S.; et al. Balloon Pulmonary Angioplasty for Inoperable Patients with Chronic Thromboembolic Pulmonary Hypertension: The Initial German Experience. Eur. Respir. J. 2017, 49, 1602409. [Google Scholar] [CrossRef]
- Brenot, P.; Jaïs, X.; Taniguchi, Y.; Alonso, C.G.; Gerardin, B.; Mussot, S.; Mercier, O.; Fabre, D.; Parent, F.; Jevnikar, M.; et al. French Experience of Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension. Eur. Respir. J. 2019, 53, 1802095. [Google Scholar] [CrossRef]
- Lang, I.M.; Pesavento, R.; Bonderman, D.; Yuan, J.X.J. Risk Factors and Basic Mechanisms of Chronic Thromboembolic Pulmonary Hypertension: A Current Understanding. Eur. Respir. J. 2013, 41, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.; Boyer-Neumann, C.; Parent, F.; Eschwege, V.; Jaillet, H.; Meyer, D.; Simonneau, G. Thrombotic Risk Factors in Pulmonary Hypertension. Eur. Respir. J. 2000, 15, 395–399. [Google Scholar] [CrossRef]
- Bonderman, D.; Turecek, P.L.; Jakowitsch, J.; Weltermann, A.; Adlbrecht, C.; Schneider, B.; Kneussl, M.; Rubin, L.J.; Kyrle, P.A.; Klepetko, W.; et al. High Prevalence of Elevated Clotting Factor VIII in Chronic Thromboembolic Pulmonary Hypertension. Thromb. Haemost. 2003, 90, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Kain, K.; Carter, A.M.; Bamford, J.M.; Grant, P.J.; Catto, A.J. Gender Differences in Coagulation and Fibrinolysis in White Subjects with Acute Ischemic Stroke. J. Thromb. Haemost. 2003, 1, 390–392. [Google Scholar] [CrossRef] [PubMed]
- Pepke-Zaba, J.; Delcroix, M.; Lang, I.; Mayer, E.; Jansa, P.; Ambroz, D.; Treacy, C.; D’Armini, A.M.; Morsolini, M.; Snijder, R.; et al. Chronic Thromboembolic Pulmonary Hypertension (CTEPH): Results from an International Prospective Registry. Circulation 2011, 124, 1973–1981. [Google Scholar] [CrossRef]
- Cruz-Utrilla, A.; Cristo-Ropero, M.J.; Calderón-Flores, M.; Velázquez, M.; López-Gude, M.J.; Ostolaza, Y.R.; Vela, J.L.P.; de la Cruz-Bertolo, J.; Bueno, H.; Ynsaurriaga, F.A.; et al. Sex Differences in Chronic Thromboembolic Pulmonary Hypertension. Treatment Options over Time in a National Referral Center. J. Clin. Med. 2021, 10, 4251. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Hu, S.; Yan, X.X.; Peng, F.H.; Tan, J.S.; Guo, T.T.; Gao, X.; Hua, L. Chronic Thromboembolic Pulmonary Hypertension in Females: Clinical Features and Survival. J. Cardiovasc. Dev. Dis. 2022, 9, 308. [Google Scholar] [CrossRef] [PubMed]
- Lang, I.M. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: Clinical Outcomes. Eur. Cardiol. Rev. 2023, 18, e11. [Google Scholar] [CrossRef] [PubMed]
- Chausheva, S.; Naito, A.; Ogawa, A.; Seidl, V.; Winter, M.P.; Sharma, S.; Sadushi-Kolici, R.; Campean, I.A.; Taghavi, S.; Moser, B.; et al. Chronic Thromboembolic Pulmonary Hypertension in Austria and Japan. J. Thorac. Cardiovasc. Surg. 2019, 158, 604–614. [Google Scholar] [CrossRef] [PubMed]
- Keen, J.; Prisco, S.Z.; Prins, K.W. Sex Differences in Right Ventricular Dysfunction: Insights From the Bench to Bedside. Front. Physiol. 2021, 11, 623129. [Google Scholar] [CrossRef]
- Shigeta, A.; Tanabe, N.; Shimizu, H.; Hoshino, S.; Maruoka, M.; Sakao, S.; Tada, Y.; Kasahara, Y.; Takiguchi, Y.; Tatsumi, K.; et al. Gender Differences in Chronic Thromboembolic Pulmonary Hypertension in Japan. Circ. J. 2008, 72, 2069–2074. [Google Scholar] [CrossRef] [PubMed]
- Kaldararova, M.; Simkova, I.; Bohacekova, M.; Reptova, A.; Hlavata, T.; Pacak, J.; Lindner, J.; Jansa, P. Central versus Peripheral CTEPH-Clinical and Hemodynamic Specifications. Medicina 2022, 58, 1538. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.L.; Yu, Y.Z.; Yuan, P.; Gong, S.G.; Wang, C.Y.; Li, Y.; Zhao, Q.H.; Jiang, R.; Wu, W.H.; He, J.; et al. Sex Differences of Hemodynamics during Acute Vasoreactivity Testing to Predict the Outcomes of Chronic Thromboembolic Pulmonary Hypertension. Clin. Respir. J. 2020, 14, 611–621. [Google Scholar] [CrossRef]
- Zoppellaro, G.; Badawy, M.R.; Squizzato, A.; Denas, G.; Tarantini, G.; Pengo, V. Balloon Pulmonary Angioplasty in Patients With Chronic Thromboembolic Pulmonary Hypertension—A Systematic Review and Meta-Analysis. Circ. J. 2019, 83, 1660–1667. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, M.K.; Kennedy, S.A.; Tan, K.T.; de Perrot, M.; Bassett, P.; McInnis, M.C.; Thenganatt, J.; Donahoe, L.; Granton, J.; Mafeld, S. Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension: A Systematic Review and Meta-Analysis. Cardiovasc. Interv. Radiol. 2023, 46, 5–18. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Female (n = 44) | Male (n = 50) | p-Value | |
|---|---|---|---|---|
| Age, years | 54 (47–70) | 66 (54–73) | 0.07 | |
| Anthropometric measures | Weight, kg | 67 (61–74) | 81 (74–93) | <0.001 |
| Height, cm | 162 (7.8) | 175 (7.4) | <0.001 | |
| BSA, m2 | 1.73 (0.18) | 1.98 (0.17) | <0.001 | |
| BMI, kg/m2 | 25.6 (23.3–28.4) | 26.8 (24.5–29.9) | 0.19 | |
| Comorbidities | Previous venous thrombosis, % | 19 (43.2) | 26 (52.0) | 0.42 |
| Previous acute pulmonary embolism, % | 37 (84.1) | 36 (72.0) | 0.22 | |
| Hypertension, % | 19 (43.2) | 28 (56.0) | 0.30 | |
| Diabetes, % | 2 (4.6) | 7 (14.0) | 0.23 | |
| Coronary artery disease, % | 9 (20.5) | 14 (28.0) | 0.47 | |
| Hyperlipidemia, % | 13 (29.6) | 19 (38.0) | 0.51 | |
| Chronic obstructive pulmonary disease, % | 0 (0.0) | 13 (26.0) | <0.001 | |
| Chronic kidney disease, % | 8 (18.2) | 10 (20.0) | 1.00 | |
| Atrial fibrillation, % | 4 (9.1) | 12 (24.0) | 0.10 | |
| Inferior vena cava filter, % | 6 (13.6) | 5 (10.0) | 0.75 | |
| Anticoagulant treatment | VKA, % | 12 (27.3) | 14 (28.0) | 0.75 |
| LMWH, % | 7 (15.9) | 9 (18.0) | ||
| DOAC, % | 24 (54.6) | 27 (54.0) | ||
| PH specific therapy | Sildenafil or riociguat, % | 36 (81.8) | 39 (78.0) | 0.71 |
| Oxygen therapy, % | 8 (18.2) | 7 (14.0) | 0.58 | |
| Reasons for rejection from PEA | Distal pulmonary vascular obstruction, % | 28 (63.6) | 26 (52.0) | 0.33 |
| Comorbidities, % | 6 (13.6) | 10 (20.0) | ||
| Lack of patient consent, % | 5 (11.4) | 3 (6.0) | ||
| Post-PEA CTEPH, % | 5 (11.4) | 11 (22.0) | ||
| Variable | Female (n = 44) | Male (n = 50) | p-Value | |
|---|---|---|---|---|
| Heart rate, bpm | 77 (66–92) | 72 (65–78) | 0.09 | |
| WHO FC, n (%) | 1 | 0 | 0 | 0.69 |
| 2 | 9 (20.5) | 10 (20.0) | ||
| 3 | 32 (72.7) | 34 (68.0) | ||
| 4 | 3 (6.8) | 6 (12.0) | ||
| 6-MWT, m | 341 (135.8) | 366 (135.3) | 0.43 | |
| Borg Dyspnea Scale, points (%) | 0 | 17 (50.0) | 22 (62.9) | 0.89 |
| 1 | 0 | 0 | ||
| 2 | 4 (11.8) | 4 (11.4) | ||
| 3 | 5 (14.7) | 3 (8.6) | ||
| 4 | 2 (5.9) | 1 (2.9) | ||
| 5 | 3 (8.8) | 3 (8.6) | ||
| 6 | 0 | 0 | ||
| 7 | 0 | 0 | ||
| 8 | 3 (8.8) | 2 (5.7) | ||
| 9 | 0 | 0 | ||
| 10 | 0 | 0 | ||
| Laboratory tests | NT-proBNP, pg/mL | 1195 (412–1970) | 1367 (652–2533) | 0.71 |
| Troponin T, ng/mL | 0.011 (0.006–0.021) | 0.015 (0.009–0.026) | 0.07 | |
| Creatinine, mg/dL | 0.86 (0.80–0.98) | 1.13 (0.99–1.30) | <0.001 | |
| Variable | Female (n = 44) | Male (n = 50) | p-Value |
|---|---|---|---|
| mRAP, mmHg | 7 (5–10) | 9 (5–12) | 0.31 |
| sPAP, mmHg | 85 (17.6) | 76 (18.5) | 0.03 |
| dPAP, mmHg | 29 (7.9) | 28 (8.1) | 0.56 |
| mPAP, mmHg | 49 (10.7) | 45 (10.5) | 0.08 |
| PCWP, mmHg | 9 (6–12) | 10 (9–12) | 0.30 |
| CI, L/min/m2 | 2.24 (1.81–2.80) | 2.24 (1.92–2.50) | 0.70 |
| SV, mL/beat | 54 (17.2) | 64 (17.5) | 0.01 |
| SVI, mL/beat/m2 | 31.59 (9.9) | 31.91 (7.9) | 0.86 |
| PVR, Wood Units | 9.89 (6.31–14.06) | 8.21 (5.55–10.17) | 0.03 |
| Variable | Female (n = 44) | Male (n = 50) | p-Value | |
|---|---|---|---|---|
| Heart rate, bpm | 68 (61–78) | 67 (59–78) | 0.53 | |
| WHO FC, n (%) | 1 | 14 (31.8) | 13 (26.0) | 0.59 |
| 2 | 20 (45.5) | 28 (56.0) | ||
| 3 | 10 (22.7) | 9 (18.0) | ||
| 4 | 0 | 0 | ||
| 6-MWT, m | 428 (134) | 444 (134) | 0.57 | |
| 6-MWT, Δm | +93 (96.6) | +76 (108) | 0.47 | |
| Borg Dyspnea Scale, points (%) | 0 | 34 (87.2) | 35 (79.6) | 0.03 |
| 1 | 0 | 0 | ||
| 2 | 3 (7.7) | 0 | ||
| 3 | 0 | 2 (4.5) | ||
| 4 | 0 | 1 (2.6) | ||
| 5 | 0 | 4 (10.5) | ||
| 6 | 0 | 1 (2.6) | ||
| 7 | 2 (5.1) | 0 | ||
| 8 | 0 | 0 | ||
| 9 | 0 | 0 | ||
| 10 | 0 | 0 | ||
| Laboratory tests | NT-proBNP, pg/mL | 152 (87–376) | 223 (73–743) | 0.60 |
| Troponin T, ng/L | 0.007 (0.004–0.012) | 0.014 (0.009–0.022) | <0.001 | |
| Creatinine, mg/dL | 0.79 (0.72–0.90) | 1.05 (0.96–1.20) | <0.001 | |
| Variable | Female (n = 44) | Male (n = 50) | p-Value | |
|---|---|---|---|---|
| mRAP, mmHg | 5 (4–7) | 6 (3–7) | 0.77 | |
| sPAP, mmHg | 43 (37–49) | 49 (41–54) | 0.04 | |
| dPAP, mmHg | 15 (12–18) | 17 (13–22) | 0.05 | |
| mPAP, mmHg | 26 (22–30) | 29 (23–33) | 0.11 | |
| Δnominal | −20.9 (±12.2) | −15.8 (±10.8) | 0.04 | |
| Δ% | −43% (−57–25) | −37% (−47–−18) | 0.049 | |
| PCWP, mmHg | 9 (8–11) | 10 (9–14) | 0.03 | |
| CI, L/min/m2 | 2.82 (0.50) | 2.57 (0.53) | 0.03 | |
| Δnominal | +0.40 (±0.77) | +0.30 (±0.50) | 0.42 | |
| Δ% | +16% (−1–51) | +11% (−5–32) | 0.34 | |
| SV, mL/beat | 70.87 (14.37) | 76.62 (20.02) | 0.12 | |
| SVI, mL/beat/m2 | 40.77 (7.61) | 38.33 (9.21) | 0.17 | |
| PVR, Wood Units | 3.34 (2.63–3.87) | 3.08 (2.58–4.49) | 0.65 | |
| Δnominal | −6.64 (−10.28–−2.85) | −3.85 (−6.48–−1.77) | 0.048 | |
| Δ% | −62% (−79–−42) | −54% (−69–−36) | 0.12 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurzyna, P.; Witowicz, A.; Kędzierski, P.; Florczyk, M.; Banaszkiewicz, M.; Szwed, P.; Piłka, M.; Gąsecka, A.; Pietrasik, A.; Torbicki, A.; et al. Sex-Specific Differences in Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty. J. Clin. Med. 2025, 14, 899. https://doi.org/10.3390/jcm14030899
Kurzyna P, Witowicz A, Kędzierski P, Florczyk M, Banaszkiewicz M, Szwed P, Piłka M, Gąsecka A, Pietrasik A, Torbicki A, et al. Sex-Specific Differences in Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty. Journal of Clinical Medicine. 2025; 14(3):899. https://doi.org/10.3390/jcm14030899
Chicago/Turabian StyleKurzyna, Paweł, Anna Witowicz, Piotr Kędzierski, Michał Florczyk, Marta Banaszkiewicz, Piotr Szwed, Michał Piłka, Aleksandra Gąsecka, Arkadiusz Pietrasik, Adam Torbicki, and et al. 2025. "Sex-Specific Differences in Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty" Journal of Clinical Medicine 14, no. 3: 899. https://doi.org/10.3390/jcm14030899
APA StyleKurzyna, P., Witowicz, A., Kędzierski, P., Florczyk, M., Banaszkiewicz, M., Szwed, P., Piłka, M., Gąsecka, A., Pietrasik, A., Torbicki, A., Kurzyna, M., & Darocha, S. (2025). Sex-Specific Differences in Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty. Journal of Clinical Medicine, 14(3), 899. https://doi.org/10.3390/jcm14030899