

The Impact of Overtraining on Injury Rates in School-Age Athletes—A Scoping Review
 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
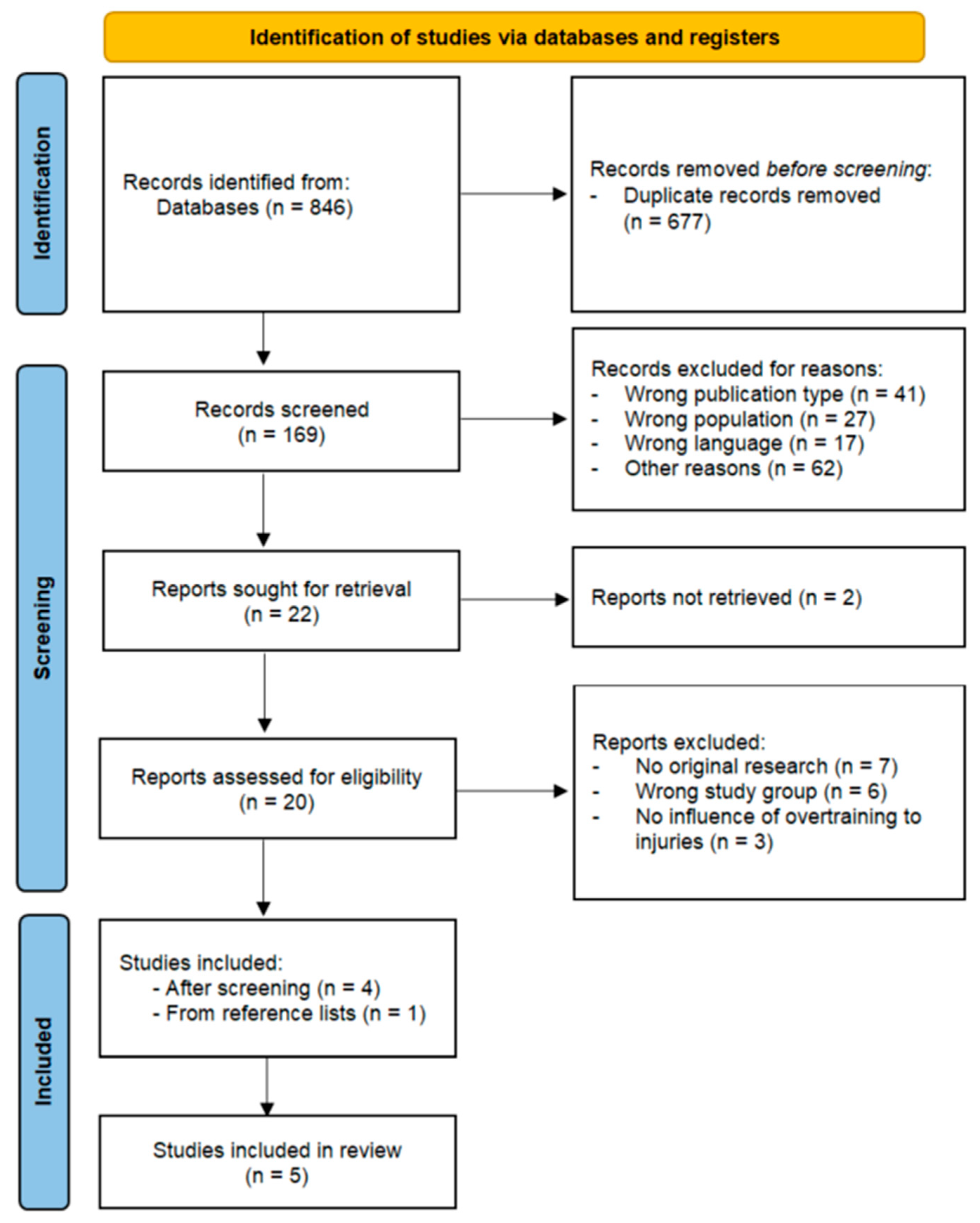
2.1. Search Strategy
2.2. Eligibility
2.3. Review Process
2.4. Data Extraction and Synthesis
3. Results

| Study | Study Design | Study Group: Age [years]; Body Mass [kg]; Body Height [cm] | Aim | Intervention | Affected Body Region | Results |
|---|---|---|---|---|---|---|
| Tak et al. [34] | Retrospective cross-sectional study | 63 footballers (63M); Age: 23.1 ± 4.2; Weight: 78.2 ± 7.9; Height: 182.3 ± 7.3. Age at start of football: 6.4 ± 2.4; Age of professional football start: 12.5 ± 2.9 | To investigate if there is a dose–response relationship between the frequency of playing football during skeletal growth and the presence of a cam deformity To investigate whether the age at which a player starts playing football is associated with the presence of a cam deformity in adulthood. | Cam deformity: Weight bearing in AP and frog-leg lateral radiographs. Measurement of the α angle in both hips. The threshold for cam deformity was set to α angle >60°. The threshold for pathological cam deformity was set to α angle >78°. Athletic activity: The age at which participants started playing football, the number of plays per week, and leg dominance were assessed by questionnaire. | Femoral neck | There was a higher prevalence of cam deformity in frog-leg lateral radiographs in players who started professional football training at a younger age. There was no difference in AP radiographs. |
| Matsuda et al. [35] | Case report | 1 footballer (M) Age: 11; Weight: 39; Height: 142 | To describe a bony bump on the femoral neck possibly induced by repetitive microtrauma, probably due to overtraining as a soccer goalkeeper. | X-ray, MRI, and CT were performed to find the cause of hip pain. Arthroscopy was performed to collect samples for histology and to perform resection of excessive tissue. | Femoral neck | The patient successfully returned to play within four months postoperatively, with no recurrence of symptoms observed during the one-year follow-up period. |
| McGowan et al. [36] | Cross-sectional study | 914 children (376M); Age: 12.6 ± 0.5; Weight: nd.; Height: nd. | To investigate whether early specialization and exceeding current recommendations regarding sport participation volume are associated with injury history in children. | Questionnaire assessment of specialization, participation volume, and occurrence of sports injuries in the last 12 months. | Lower limb (62%); Upper limb (26%); Head and torso (12%). | Neither early specialization in one sport nor exceeding currently recommended sport participation volumes increased the odds of reporting a history of injury. |
| O’Keeffe et al. [37] | Prospective cohort study | 97 Gaelic footballers (97M); Age: 13.4 ± 1.1; Weight: 59.3 ± 12.5; Height: 160 ± 10. | Impact of internal load on injury incidence in male adolescent Gaelic footballers. | A self-recall diary was utilized to record sports and recreational activities. Injuries were monitored for 15.2 ± 8.9 weeks. Injury onset, occurrence, location, nature, mechanism, and severity (days missed from participation) were recorded. | Lower limb (68%); Upper limb (23%); Trunk (9%). | Higher than average values of weekly load, monotony, and absolute load change were significant injury factors. |
| Hildebrandt et al. [38] | Prospective cohort study | 91 elite ski racers; M: 52; Age: 12.1 ± 1.3; Weight: 42.7 ± 8.8; Height: 152.6 ± 9.8. F: 39 Age: 12.0 ± 1.3; Weight: 43.5 ± 9.7; Height: 152.4 ± 10.0. | To prospectively examine training load as it relates to the occurrence, severity, and burden of injuries and illness in youth alpine ski racers. | Prospective analysis of the training load characteristics, traumatic injuries, overuse injuries, and illness throughout 1 season. | Knee (39%); Lower leg (18%); Ankle (12%); Spine/back (10%); Upper leg (7%); Hip (5%); Foot (5%); Head (2%); Shoulder (2%). | A higher intensity and volume of the training were associated with increased illness, but not a higher risk of injury. |
3.1. Characteristics of Participants
3.2. Summary of Study Aims
3.3. Summary of Study Methods and Outcome Measures
3.4. Summary of Injury Sites
3.5. Summary of the Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schembri, R.; Quinto, A.M.V.; Aiello, F.; Sgrò, F. The relationship between the practice of physical activity and sport and the level of motor competence in primary school children. J. Phys. Educ. Sport 2019, 10, 1954–1959. [Google Scholar] [CrossRef]
- Alves, J.G.B.; Alves, G.V. Effects of physical activity on children’s growth. J. Pediatr. 2019, 95 (Suppl. 1), 72–78. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children: A Systematic Review. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef]
- Eime, R.; Charity, M.; Owen, K. The changing nature of how and where Australians play sport. BMC Public Health 2024, 24, 3165. [Google Scholar] [CrossRef] [PubMed]
- Black, L.I.; Terlizzi, E.P.; Vahratian, A. Organized Sports Participation Among Children Aged 6–17 Years: United States, 2020; National Center for Health Statistics: Hyattsville, MD, USA, 2022; pp. 1–8. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global Trends in Insufficient Physical Activity among Adolescents: A Pooled Analysis of 298 Population-Based Surveys with 1·6 Million Participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Ting, J.L.C.; Mukherjee, S.; Hwa, M.C.Y. Physical Activity and Sedentary Behavior Patterns of Singaporean Adolescents. J. Phys. Act. Health 2015, 12, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Jayanthi, N.; Pinkham, C.; Dugas, L.; Patrick, B.; Labella, C. Sports specialization in young athletes: Evidence-based recommendations. Sports Health 2013, 5, 251–257. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Myer, G.D. Resistance training among young athletes: Safety, efficacy and injury prevention effects. Br. J. Sports Med. 2010, 44, 56–63. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Oliver, J.L.; Faigenbaum, A.D.; Howard, R.; De Ste Croix, M.B.; Williams, C.A.; Best, T.M.; Alvar, B.A.; Micheli, L.J.; Thomas, D.P.; et al. Long-term athletic development, part 2: Barriers to success and potential solutions. J. Strength Cond. Res. 2015, 29, 1451–1464. [Google Scholar] [CrossRef]
- Franklin, C.C.; Weiss, J.M. Stopping sports injuries in kids: An overview of the last year in publications. Curr. Opin. Pediatr. 2012, 24, 64–67. [Google Scholar] [CrossRef]
- Meeusen, R.; Duclos, M.; Foster, C.; Fry, A.; Gleeson, M.; Nieman, D.; Raglin, J.; Rietjens, G.; Steinacker, J.; Urhausen, A. Prevention, diagnosis, and treatment of the overtraining syndrome: Joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med. Sci. Sports Exerc. 2013, 45, 186–205. [Google Scholar] [CrossRef] [PubMed]
- Jelínek, M.; Květon, P.; Burešová, I. Subjective Indicators of Overtraining and Their Relationship to Sport Fitness: A 1-year Observation of Elite Athletes. SAGE Open 2024, 14, 21582440241252001. [Google Scholar] [CrossRef]
- Carrard, J.; Rigort, A.C.; Appenzeller-Herzog, C.; Colledge, F.; Königstein, K.; Hinrichs, T.; Schmidt-Trucksäss, A. Diagnosing Overtraining Syndrome: A Scoping Review. Sports Health 2022, 14, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.W.; Micheli, L.J. Training the child athlete for prevention, health promotion, and performance: How much is enough, how much is too much? Clin. Sports Med. 2011, 30, 679–690. [Google Scholar] [CrossRef]
- Myer, G.D.; Jayanthi, N.; DiFiori, J.P.; Faigenbaum, A.D.; Kiefer, A.W.; Logerstedt, D.; Micheli, L.J. Sports Specialization, Part II: Alternative Solutions to Early Sport Specialization in Youth Athletes. Sports Health 2016, 8, 65–73. [Google Scholar] [CrossRef]
- Iona, T.; Raimo, S.; Coco, D.; Tortella, P.; Masala, D.; Ammendolia, A.; Mannocci, A.; La Torre, G. Specialization and Injury Risk in Different Youth Sports: A Bio-Emotional Social Approach. Front. Psychol. 2022, 13, 818739. [Google Scholar] [CrossRef] [PubMed]
- Güllich, A.; Barth, M. Effects of Early Talent Promotion on Junior and Senior Performance: A Systematic Review and Meta-Analysis. Sports Med. 2024, 54, 697–710. [Google Scholar] [CrossRef]
- Daley, M.M.; Reardon, C.L. Mental Health in the Youth Athlete. Clin. Sports Med. 2024, 43, 107–126. [Google Scholar] [CrossRef]
- Xanthopoulos, M.S.; Benton, T.; Lewis, J.; Case, J.A.; Master, C.L. Mental Health in the Young Athlete. Curr. Psychiatry Rep. 2020, 22, 63. [Google Scholar] [CrossRef]
- Veliz, P.; Mutumba, M. Assessing the Role of Sports Participation on Depression, Suicide Ideation, and Suicide Behaviors Among Adolescents Before and During COVID-19. J. Phys. Act. Health 2024, 21, 197–208. [Google Scholar] [CrossRef]
- Lee, O.; Park, S.; Kim, Y.; So, W.Y. Participation in Sports Activities before and after the Outbreak of COVID-19: Analysis of Data from the 2020 Korea National Sports Participation Survey. Healthcare 2022, 10, 122. [Google Scholar] [CrossRef] [PubMed]
- Jia, P.; Zhang, L.; Yu, W.; Yu, B.; Liu, M.; Zhang, D.; Yang, S. Correction: Impact of COVID-19 lockdown on activity patterns and weight status among youths in China: The COVID-19 Impact on Lifestyle Change Survey (COINLICS). Int. J. Obes. 2021, 45, 920. [Google Scholar] [CrossRef] [PubMed]
- Pajek, S.V. Impact of the COVID-19 Pandemic on the Motor Development of Schoolchildren in Rural and Urban Environments. BioMed. Res. Int. 2022, 2022, 8937693. [Google Scholar] [CrossRef]
- Lau, R.; Mukherjee, S. Development and validation of an overuse injury questionnaire for youth athletes: The Youth Overuse Injury Questionnaire. Phys. Ther. Sport 2024, 67, 47–53. [Google Scholar] [CrossRef]
- Lau, R.Y.; Mukherjee, S. Effectiveness of overuse injury prevention programs on upper extremity performance in overhead youth athletes: A systematic review. Sports Med. Health Sci. 2023, 5, 91–100. [Google Scholar] [CrossRef]
- Lau, R.; Mukherjee, S. The effects of an education and exercise-based injury prevention programme on knowledge, eccentric shoulder strength, shoulder range of motion, and thoracic range of motion among competitive youth volleyball athletes: A randomized controlled trial. Res. Sports Med. 2025, 33, 458–474. [Google Scholar] [CrossRef]
- Lau, R.; Mukherjee, S. Developing the Singapore youth shoulder overuse injury prevention program. Phys. Ther. Sport 2024, 65, 30–37. [Google Scholar] [CrossRef]
- Lau, R.; Mukherjee, S. Moving Beyond the Checklist—An Enhanced Approach to Context-Driven Overuse Injury Prevention in Overhead Youth Athletes. J. Clin. Med. 2025, 14, 971. [Google Scholar] [CrossRef]
- Aicale, R.; Tarantino, D.; Maffulli, N. Overuse injuries in sport: A comprehensive overview. J. Orthop. Surg. 2018, 13, 309. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Haddaway, N.R.; Page, M.J.; Pritchard, C.C.; McGuinness, L.A. PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Tak, I.; Weir, A.; Langhout, R.; Waarsing, J.H.; Stubbe, J.; Kerkhoffs, G.; Agricola, R. The relationship between the frequency of football practice during skeletal growth and the presence of a cam deformity in adult elite football players. Br. J. Sports Med. 2015, 49, 630–634. [Google Scholar] [CrossRef]
- Matsuda, Y.; Kobayashi, N.; Inaba, Y.; Kubota, S.; Yukizawa, Y.; Choe, H.; Kato, I.; Ohashi, K.; Saito, T. Reactive Osteochondromatous Lesion of the Femoral Neck in a Highly Active Preadolescent Patient: Is This the Pathogenesis of a Cam Deformity? Clin. J. Sport Med. 2018, 28, e95–e97. [Google Scholar] [CrossRef]
- McGowan, J.; Whatman, C.; Walters, S. The associations of early specialisation and sport volume with musculoskeletal injury in New Zealand children. J. Sci. Med. Sport 2020, 23, 139–144. [Google Scholar] [CrossRef]
- O’Keeffe, S.; O’Connor, S.; Ní Chéilleachair, N. Are internal load measures associated with injuries in male adolescent Gaelic football players? Eur. J. Sport Sci. 2020, 20, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, C.; Oberhoffer, R.; Raschner, C.; Müller, E.; Fink, C.; Steidl-Müller, L. Training load characteristics and injury and illness risk identification in elite youth ski racing: A prospective study. J. Sport Health Sci. 2021, 10, 230–236. [Google Scholar] [CrossRef]
- Barry, L.; Lyons, M.; McCreesh, K.; Powell, C.; Comyns, T. The relationship between training load and pain, injury and illness in competitive swimming: A systematic review. Phys. Ther. Sport 2021, 48, 154–168. [Google Scholar] [CrossRef]
- Franco, M.F.; Madaleno, F.O.; de Paula, T.M.N.; Ferreira, T.V.; Pinto, R.Z.; Resende, R.A. Prevalence of overuse injuries in athletes from individual and team sports: A systematic review with meta-analysis and GRADE recommendations. Braz. J. Phys. Ther. 2021, 25, 500–513. [Google Scholar] [CrossRef]
- Chaudhry, H.; Ayeni, O.R. The etiology of femoroacetabular impingement: What we know and what we don’t. Sports Health 2014, 6, 157–161. [Google Scholar] [CrossRef]
- Fernquest, S.; Palmer, A.; Gimpel, M.; Birchall, R.; Broomfield, J.; Wedatilake, T.; Dijkstra, H.; Burchall, J.; Lloyd, T.; Pereira, C.; et al. A longitudinal cohort study of adolescent elite footballers and controls investigating the development of cam morphology. Sci. Rep. 2021, 11, 18567. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.; Barber Foss, K.; Hewett, T.E.; Myer, G.D. Sport specialization’s association with an increased risk of developing anterior knee pain in adolescent female athletes. J. Sport Rehabil. 2015, 24, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Young, B.W.; Starkes, J.L. Measuring Outcomes of Swimmers’ Non-Regulation during Practice: Relationships between Self-Report, Coaches’ Judgments, and Video-Observation. Int. J. Sports Sci. Coach. 2006, 1, 131–148. [Google Scholar] [CrossRef]
- Soler-López, A.; Gómez-Carmona, C.D.; Moreno-Villanueva, A.; Gutiérrez, A.M.; Pino-Ortega, J. Effects of Congested Matches and Training Schedules on Salivary Markers in Elite Futsal Players. Appl. Sci. 2024, 14, 4968. [Google Scholar] [CrossRef]
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borkowski, R.; Krzepota, J.; Wróbel, M.; Madej, D.; Błażkiewicz, M. The Impact of Overtraining on Injury Rates in School-Age Athletes—A Scoping Review. J. Clin. Med. 2025, 14, 4712. https://doi.org/10.3390/jcm14134712
Borkowski R, Krzepota J, Wróbel M, Madej D, Błażkiewicz M. The Impact of Overtraining on Injury Rates in School-Age Athletes—A Scoping Review. Journal of Clinical Medicine. 2025; 14(13):4712. https://doi.org/10.3390/jcm14134712
Chicago/Turabian StyleBorkowski, Rafał, Justyna Krzepota, Mikołaj Wróbel, Dominika Madej, and Michalina Błażkiewicz. 2025. "The Impact of Overtraining on Injury Rates in School-Age Athletes—A Scoping Review" Journal of Clinical Medicine 14, no. 13: 4712. https://doi.org/10.3390/jcm14134712
APA StyleBorkowski, R., Krzepota, J., Wróbel, M., Madej, D., & Błażkiewicz, M. (2025). The Impact of Overtraining on Injury Rates in School-Age Athletes—A Scoping Review. Journal of Clinical Medicine, 14(13), 4712. https://doi.org/10.3390/jcm14134712