

Accuracy of Digital Impressions for Veneer Restorations: A Narrative Review and Case Illustration

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Review Search
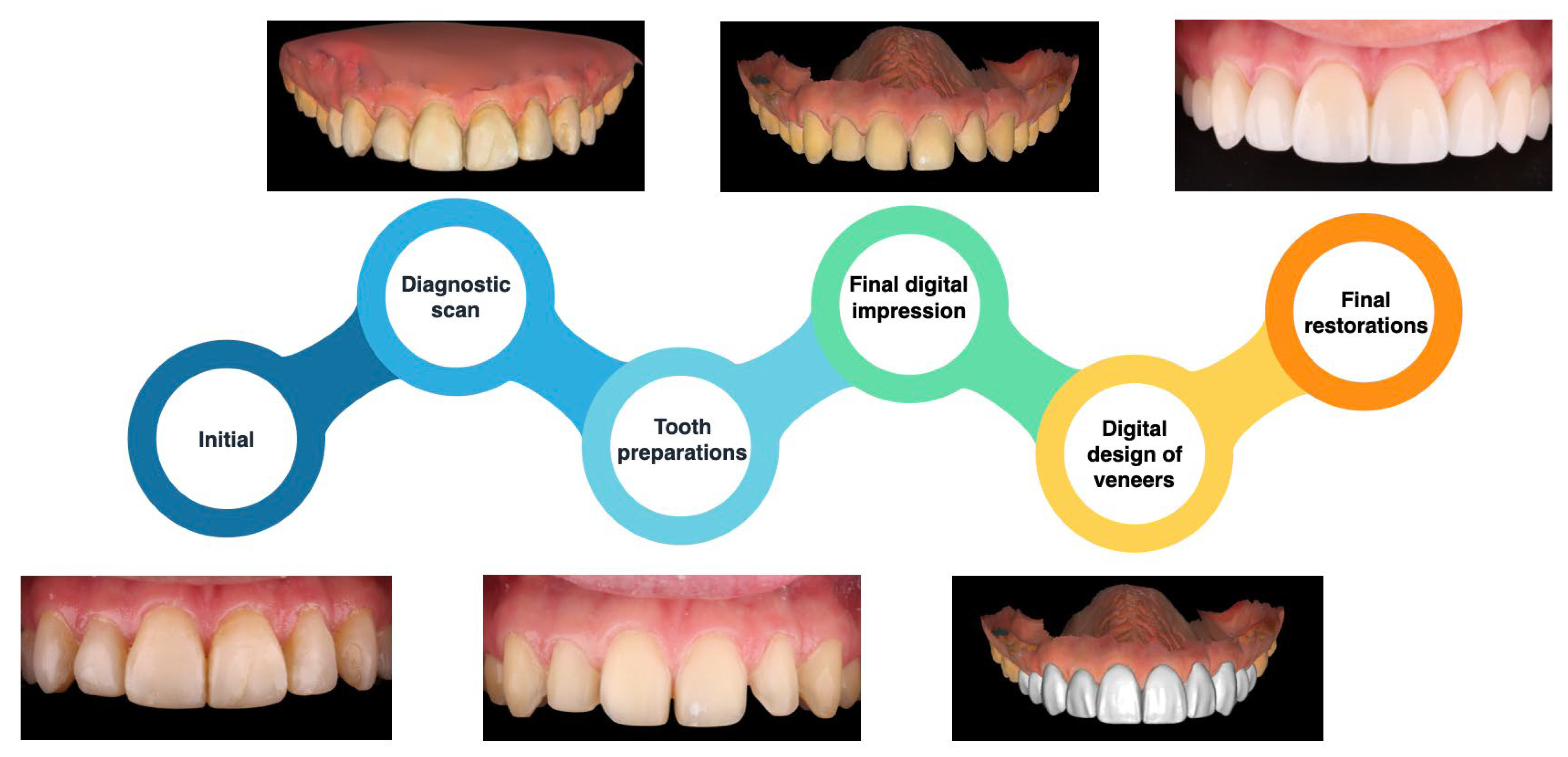
2.2. Case Study
- Stained and worn resin composite restorations spanning from the maxillary right first premolar to the left first premolar.
- Crack lines visible on the resin composite veneers of the maxillary left central incisor, left lateral incisor, and left canine.
3. Results
3.1. Literature Review Outcomes
3.2. Case Illustration Outcome
4. Discussion
4.1. Accuracy of Digital Impressions
4.2. Streamlined File Sharing
4.3. Expedited Process
4.4. Patient Comfort
4.5. Challenges Related to Cost
4.6. Technology Learning Curve
4.7. Limitations of the Review
4.8. Case Illustration
4.9. Take-Home Message
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rekow, E.D. CAD/CAM in dentistry: A historical perspective and view of the future. J. Can. Dent. Assoc. 1992, 58, 283, 287–288. [Google Scholar] [PubMed]
- Sannino, G.; Germano, F.; Arcuri, L.; Bigelli, E.; Arcuri, C.; Barlattani, A. CEREC CAD/CAM Chairside System. Oral Implantol. 2015, 7, 57–70. [Google Scholar] [PubMed] [PubMed Central]
- Mörmann, W.H. The evolution of the CEREC system. J. Am. Dent. Assoc. 2006, 137, 7S–13S. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A review of dental CAD/CAM: Current status and future perspectives from 20 years of experience. Dent. Mater. J. 2009, 28, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Maiti, N.; Mahapatra, N.; Patel, D.; Chanchad, J.; Saurabhbhai Shah, A.; Mahboob Rahaman, S.K.; Surana, P. Application of CAD-CAM in Dentistry. Bioinformation 2024, 20, 547–550. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Davidowitz, G.; Kotick, P.G. The use of CAD/CAM in dentistry. Dent. Clin. N. Am. 2011, 55, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Janeva, N.M.; Kovacevska, G.; Elencevski, S.; Panchevska, S.; Mijoska, A.; Lazarevska, B. Advantages of CAD/CAM versus Conventional Complete Dentures—A Review. Open Access Maced. J. Med. Sci. 2018, 6, 1498–1502. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Suganna, M.; Kausher, H.; Tarek Ahmed, S.; Sultan Alharbi, H.; Faraj Alsubaie, B.; Ds, A.; Haleem, S.; Meer Rownaq Ali, A.B. Contemporary Evidence of CAD-CAM in Dentistry: A Systematic Review. Cureus 2022, 14, e31687. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sonkesriya, S.; Kulkarni, R.; Satapathy, S.K.; Fathima, S.; Thomas, V.; Gangadharappa, P. Evaluation of the Impact of Digital Dentistry on the Precision of Implant Placement and Prosthesis Fabrication: An In-Vitro Study. Cureus 2024, 16, e60389. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nejatidanesh, F.; Amjadi, M.; Akouchekian, M.; Savabi, O. Clinical performance of CEREC AC Bluecam conservative ceramic restorations after five years--A retrospective study. J. Dent. 2015, 43, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Abdulkarim, L.I.; Alharamlah, F.S.S.; Abubshait, R.M.; Alotaibi, D.A.; Abouonq, A.O. Impact of Digital Workflow Integration on Fixed Prosthodontics: A Review of Advances and Clinical Outcomes. Cureus 2024, 16, e72286. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mahato, M.; Hota, S.; Jain, A.; Dutta, D.; Bhushan, P.; Raut, A. Comparison of Conventional and Digital Workflows in the Fabrication of Fixed Prostheses: A Systematic Review. Cureus 2024, 16, e61764. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zarbakhsh, A.; Jalalian, E.; Samiei, N.; Mahgoli, M.H.; Kaseb Ghane, H. Accuracy of Digital Impression Taking Using Intraoral Scanner versus the Conventional Technique. Front. Dent. 2021, 18, 6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Accuracy of crowns based on digital intraoral scanning compared to conventional impression-a split-mouth randomised clinical study. Clin. Oral Investig. 2019, 23, 4043–4050. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.Y.; Cao, Y.; Hu, Z.W.; Wang, Y.; Chen, H.; Sun, Y.C. Scanning Accuracy of 10 Intraoral Scanners for Single-crown and Three-unit Fixed Denture Preparations: An In Vitro Study. Chin. J. Dent. Res. 2022, 25, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Abduo, J.; Ho, G.; Centorame, A.; Chohan, S.; Park, C.; Abdouni, R.; Le, P.; Ngo, C. Marginal Accuracy of Monolithic and Veneered Zirconia Crowns Fabricated by Conventional and Digital Workflows. J. Prosthodont. 2023, 32, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Schubert, O.; Erdelt, K.J.; Tittenhofer, R.; Hajtó, J.; Bergmann, A.; Güth, J.F. Influence of intraoral scanning on the quality of preparations for all-ceramic single crowns. Clin. Oral Investig. 2020, 24, 4511–4518. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ahlholm, P.; Sipilä, K.; Vallittu, P.; Jakonen, M.; Kotiranta, U. Digital Versus Conventional Impressions in Fixed Prosthodontics: A Review. J. Prosthodont. 2018, 27, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Nathanson, D. Current developments in esthetic dentistry. Curr. Opin. Dent. 1991, 1, 206–211. [Google Scholar] [PubMed]
- Panayong, T.; Chengprapakorn, W.; Limpuangthip, N.; Serichetaphongse, P. Long-Term Outcomes of Ceramic Veneers Restorations: A Comprehensive Analysis of Clinical and Patient-Reported Metrics. J. Esthet. Restor. Dent. 2025, 37, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Mazzetti, T.; Collares, K.; Rodolfo, B.; da Rosa Rodolpho, P.A.; van de Sande, F.H.; Cenci, M.S. 10-year practice-based evaluation of ceramic and direct composite veneers. Dent. Mater. 2022, 38, 898–906. [Google Scholar] [CrossRef] [PubMed]
- AlJazairy, Y.H. Survival Rates for Porcelain Laminate Veneers: A Systematic Review. Eur. J. Dent. 2021, 15, 360–368. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ye, Z.; Jiang, J.; Yang, L.; Xu, T.; Lin, Y.; Luo, F. Research Progress and Clinical Application of All-Ceramic Micro-Veneer. Materials 2023, 16, 2957. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meijering, A.C.; Roeters, F.J.; Mulder, J.; Creugers, N.H. Patients’ satisfaction with different types of veneer restorations. J. Dent. 1997, 25, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, S.; Millar, B.J. The effect of veneers on cosmetic improvement. Br. Dent. J. 2009, 207, E3; discussion 72–73. [Google Scholar] [CrossRef] [PubMed]
- Katz, C.R.; de Andrade Mdo, R.; Lira, S.S.; Ramos Vieira, E.L.; Heimer, M.V. The concepts of minimally invasive dentistry and its impact on clinical practice: A survey with a group of Brazilian professionals. Int. Dent. J. 2013, 63, 85–90. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schmitter, M.; Seydler, B.B. Minimally invasive lithium disilicate ceramic veneers fabricated using chairside CAD/CAM: A clinical report. J. Prosthet. Dent. 2012, 107, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Al-Dwairi, Z.N.; Al-Sardi, M.; Goodacre, B.J.; Goodacre, C.J.; Al Hamad, K.Q.; Özcan, M.; Al-Haj Husain, N.; Baba, N.Z. Evaluation of Marginal and Internal Fit of Ceramic Laminate Veneers Fabricated with Five Intraoral Scanners and Indirect Digitization. Materials 2023, 16, 2181. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Imburgia, M.; Lerner, H.; Mangano, F. A Retrospective Clinical Study on 1075 Lithium Disilicate CAD/CAM Veneers with Feather-Edge Margins Cemented on 105 Patients. Eur. J. Prosthodont. Restor. Dent. 2021, 29, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Sen, N.; Olley, R.C. Retrospective Evaluation of Factors Affecting Long-Term Clinical Performance of CAD/CAM Laminate Veneers. Int. J. Prosthodont. 2024, 37, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Villalobos-Tinoco, J.; Floriani, F.; Rojas-Rueda, S.; Mekled, S.; Conner, C.; Colvert, S.; Jurado, C.A. Enhancing Smile Aesthetics and Function with Lithium Disilicate Veneers: A Brief Review and Case Study. Clin. Pract. 2025, 15, 66. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Badami, V.; Satya Priya, M.; Vijay, L.; Kethineni, H.; Akarapu, S.; Agarwal, S. Marginal Adaptation of Veneers: A Systematic Review. Cureus 2022, 14, e31885. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vafiadis, D.; Goldstein, G. Single visit fabrication of a porcelain laminate veneer with CAD/CAM technology: A clinical report. J. Prosthet. Dent. 2011, 106, 71–73. [Google Scholar] [CrossRef] [PubMed]
- Zandinejad, A.; Lin, W.S.; Atarodi, M.; Abdel-Azim, T.; Metz, M.J.; Morton, D. Digital workflow for virtually designing and milling ceramic lithium disilicate veneers: A clinical report. Oper Dent. 2015, 40, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.S.; Zandinejad, A.; Metz, M.J.; Harris, B.T.; Morton, D. Predictable Restorative Work Flow for Computer-Aided Design/Computer-Aided Manufacture-Fabricated Ceramic Veneers Utilizing a Virtual Smile Design Principle. Oper Dent. 2015, 40, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Stanley, M.; Paz, A.G.; Miguel, I.; Coachman, C. Fully digital workflow, integrating dental scan, smile design and CAD-CAM: Case report. BMC Oral Health 2018, 18, 134. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Revilla-León, M.; Besné-Torre, A.; Sánchez-Rubio, J.L.; Fábrega, J.J.; Özcan, M. Digital tools and 3D printing technologies integrated into the workflow of restorative treatment: A clinical report. J. Prosthet. Dent. 2019, 121, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Zhivago, P.; Yun, S.; Turkyilmaz, I. A comprehensive technique using digital workflow to improve an unpleasant smile: A clinical report. Prim. Dent. J. 2022, 11, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Rathee, M.; Divakar, S.; Jain, P.; Chahal, S.; Singh, S. Anterior esthetic rehabilitation with full and partial veneers using conventional and digital techniques: A case series. J. Conserv. Dent. Endod. 2023, 26, 601–607. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Figueira, J.; Guaqueta, N.; Ramirez, D.I.; Kois, J. Veneer tooth preparation utilizing a novel digital designed workflow: A case report. J. Esthet. Restor. Dent. 2023, 35, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Pandey, L.; Bhatt, A.; Samant, P.S.; Singh, J. Trios Lidisi Veneer, Transforming Smiles Using an Intraoral Scanner—A Case Report. Indian J. Dent. Res. 2023, 34, 461–463. [Google Scholar] [CrossRef] [PubMed]
- Santi, M.R.; Nastri, V.H.T.; Lins, R.B.E. Advanced digital planning approach using a 3D-printed mock-up. A case report. Int. J. Esthet. Dent. 2024, 19, 186–194. [Google Scholar] [PubMed]
- Sanchez, R.L.S.; Dos Santos, G.G.; Fukuoka, G.L.; Reis, I.N.R.D. Replacement of unsatisfactory ceramic veneers with the aid of a digital workflow. BMJ Case Rep. 2024, 17, e259491. [Google Scholar] [CrossRef] [PubMed]
- Osorio-Vélez, L.S.; Serna-Ceballos, J.D.; Latorre, F.; Ardila, C.M. A Conservative Approach to Ceramic Laminates in the Anterior Region: A Clinical Report. Cureus 2024, 16, e68137. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Al Hamad, K.Q.; Al Rashdan, B.A.; Al-Kaff, F.T. Virtual patient representation with silicone guide and a 3D scanner accessory for a user-friendly facial scanning workflow: A clinical report of smile design and ceramic veneers. J. Prosthet. Dent. 2025, 133, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.M.; Althagafi, R.A. Smile Makeover Utilizing Digital Esthetic Veneers Workflow: A Case Report. Int. J. Prosthodont. Restor. Dent. 2022, 12, 145–148. [Google Scholar] [CrossRef]
- do Vale Voigt, M.; Espíndola-Castro, L.F.; de Melo Monteiro, G.Q.; Ortigoza, L.S.; Dos Santos Torreão, A.; Georg, R. DSDapp use for multidisciplinary esthetic planning. J. Esthet. Restor. Dent. 2020, 32, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Boeddinghaus, M.; Breloer, E.S.; Rehmann, P.; Wöstmann, B. Accuracy of single-tooth restorations based on intraoral digital and conventional impressions in patients. Clin. Oral Investig. 2015, 19, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- Hategan, S.I.; Ionel, T.F.; Goguta, L.; Gavrilovici, A.; Negrutiu, M.L.; Jivanescu, A. Powder and Powder-Free Intra-Oral Scanners: Digital Impression Accuracy. Prim. Dent. J. 2018, 7, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Rotar, R.N.; Jivanescu, A.; Ille, C.; Podariu, A.C.; Jumanca, D.E.; Matichescu, A.M.; Balean, O.; Rusu, L.C. Trueness and Precision of Two Intraoral Scanners: A Comparative In Vitro Study. Scanning 2019, 2019, 1289570. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Diker, B.; Tak, Ö. Comparing the accuracy of six intraoral scanners on prepared teeth and effect of scanning sequence. J. Adv. Prosthodont. 2020, 12, 299–306. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chiu, A.; Chen, Y.W.; Hayashi, J.; Sadr, A. Accuracy of CAD/CAM Digital Impressions with Different Intraoral Scanner Parameters. Sensors 2020, 20, 1157. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Son, Y.T.; Son, K.; Lee, K.B. Trueness of intraoral scanners according to subgingival depth of abutment for fixed prosthesis. Sci Rep. 2022, 12, 20786. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Casucci, A.; Verniani, G.; Habib, R.; Ricci, N.M.; Carboncini, C.; Ferrari, M. Accuracy of Four Intra-Oral Scanners in Subgingival Vertical Preparation: An In Vitro 3-Dimensional Comparative Analysis. Materials 2023, 16, 6553. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Giuliodori, G.; Rappelli, G.; Aquilanti, L. Intraoral Scans of Full Dental Arches: An In Vitro Measurement Study of the Accuracy of Different Intraoral Scanners. Int. J. Environ. Res. Public Health 2023, 20, 4776. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, C.H.; Cheng, C.W.; Ye, S.Y.; Chien, C.H. A double blinded trial to compare the patient satisfaction and crown accuracy of two different intraoral scanners for the fabrication of monolithic lithium disilicate single crowns. J. Dent. Sci. 2023, 18, 1206–1211. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Park, Y.; Kim, J.H.; Park, J.K.; Son, S.A. Scanning accuracy of an intraoral scanner according to different inlay preparation designs. BMC Oral Health 2023, 23, 515. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, X.; Feng, K.; Dong, L.; Liu, L.; Ni, L.; Zheng, D. Accuracy and Efficiency of Digitally Fabricated All-Ceramic Crowns from Conventional Impressions and Intraoral Scans: A Single-Blind Clinical Randomized Controlled Trial. Int. J. Prosthodont. 2024, 37, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.; Kim, J.H.; Park, J.K.; Son, S.A. Evaluating the accuracy of CEREC intraoral scanners for inlay restorations: Impact of adjacent tooth materials. BMC Oral Health 2024, 24, 1033. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Revilla-León, M.; Alonso Pérez-Barquero, J.; Barmak, A.B.; Agustín-Panadero, R.; Fernández-Estevan, L.; Gómez-Polo, M. Accuracy of Intraoral Scanner Systems for Fabricating Inlay, Onlay, and Veneer Restorations: A Systematic Review and Meta-Analysis. J. Esthet. Restor. Dent. 2025, 37, 727–755. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.M.; Azhari, A.A.; Sedayo, L.; Alhaid, A.; Alhandar, R.; Almalki, A.; Jahlan, A.; Almutairi, A.; Kheder, W. Mapping the Landscape of the Digital Workflow of Esthetic Veneers from Design to Cementation: A Systematic Review. Dent. J. 2024, 12, 28. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pradies, G.; Gil, A.; Morón-Conejo, B.; Bonfanti-Gris, M.; Martínez-Rus, F.; Pérez-Barquero, J.A.; Barmak, A.B.; Agustín-Panadero, R.; Fernández-Estevan, L.; Gómez-Polo, M.; et al. Comparative Influence of Marginal Design and Digital Scanning Accuracy on the Clinical Longevity of Ceramic Restorations: An Evidence-Based Approach. Consensus Statement From SSRD, SEPES, and PROSEC Conference on Minimally Invasive Restorations. J. Esthet. Restor. Dent. 2025, 37, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Alghauli, M.A.; Alqutaibi, A.Y. 3D-printed intracoronal restorations, occlusal and laminate veneers: Clinical relevance, properties, and behavior compared to milled restorations; a systematic review and meta-analysis. J. Esthet Restor Dent. 2024, 36, 1153–1170. [Google Scholar] [CrossRef] [PubMed]
- Alkadi, L. A Comprehensive Review of Factors That Influence the Accuracy of Intraoral Scanners. Diagnostics 2023, 13, 3291. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Morsy, N.; El Kateb, M.; Azer, A.; Fathalla, S. Fit of zirconia fixed partial dentures fabricated from conventional impressions and digital scans: A systematic review and meta-analysis. J. Prosthet. Dent. 2023, 130, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Hawsah, A.; Rustom, R.; Alamri, A.; Althomairy, S.; Alenezi, M.; Shaker, S.; Alrawsaa, F.; Althumairy, A.; Alteraigi, A. Digital Impressions Versus Conventional Impressions in Prosthodontics: A Systematic Review. Cureus 2024, 16, e51537. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Malik, J.; Rodriguez, J.; Weisbloom, M.; Petridis, H. Comparison of Accuracy Between a Conventional and Two Digital Intraoral Impression Techniques. Int. J. Prosthodont. 2018, 31, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Güntekin, N.; Çiftçi, A.; Gözen, M.; İleri, S.A. The Effect of Image Count on Accuracy in Digital Measurements in Dentistry. Diagnostics 2024, 14, 2122. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abduo, J.; Elseyoufi, M. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Nagarkar, S.R.; Perdigão, J.; Seong, W.J.; Theis-Mahon, N. Digital versus conventional impressions for full-coverage restorations: A systematic review and meta-analysis. J. Am. Dent. Assoc. 2018, 149, 139–147.e1. [Google Scholar] [CrossRef] [PubMed]
- Eggmann, F.; Blatz, M.B. Recent Advances in Intraoral Scanners. J. Dent. Res. 2024, 103, 1349–1357. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Falih, M.Y.; Majeed, M.A. Trueness and Precision of Eight Intraoral Scanners with Different Finishing Line Designs: A Comparative In Vitro Study. Eur. J. Dent. 2023, 17, 1056–1064. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Turkyilmaz, I.; Wilkins, G.N.; Benli, M. Relationship between the data quality of digital scans from intraoral scanners and surface topography of prepared teeth. J. Dent. Sci. 2022, 17, 592–594. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jánosi, K.M.; Cerghizan, D.; Bai, E.E.; Mureșan, I.É.; Kovács, A.; Szász, A.; Hulpe, A.; Markovics, E.R.; Mártha, K.I.; Pop, S.I. An Evaluation of the Accuracy of Digital Models-An In Vitro Study. Dent. J. 2024, 12, 313. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yeslam, H.E.; Freifrau von Maltzahn, N.; Nassar, H.M. Revolutionizing CAD/CAM-based restorative dental processes and materials with artificial intelligence: A concise narrative review. PeerJ 2024, 12, e17793. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Afrashtehfar, K.I.; Alnakeb, N.A.; Assery, M.K.M. Accuracy of intraoral scanners versus traditional impressions: A rapid umbrella review. J. Evid. Based Dent. Pract. 2022, 22, 101719. [Google Scholar] [CrossRef] [PubMed]
- Bernauer, S.A.; Zitzmann, N.U.; Joda, T. The Complete Digital Workflow in Fixed Prosthodontics Updated: A Systematic Review. Healthcare 2023, 11, 679. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sakornwimon, N.; Leevailoj, C. Clinical marginal fit of zirconia crowns and patients’ preferences for impression techniques using intraoral digital scanner versus polyvinyl siloxane material. J. Prosthet. Dent. 2017, 118, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Marti, A.M.; Harris, B.T.; Metz, M.J.; Morton, D.; Scarfe, W.C.; Metz, C.J.; Lin, W.S. Comparison of digital scanning and polyvinyl siloxane impression techniques by dental students: Instructional efficiency and attitudes towards technology. Eur. J. Dent. Educ. 2017, 21, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Sivaramakrishnan, G.; Alsobaiei, M.; Sridharan, K. Patient preference and operating time for digital versus conventional impressions: A network meta-analysis. Aust. Dent. J. 2020, 65, 58–69. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, N.R.C.; Pigozzo, M.N.; Sesma, N.; Laganá, D.C. Clinical efficiency and patient preference of digital and conventional workflow for single implant crowns using immediate and regular digital impression: A meta-analysis. Clin. Oral Implants Res. 2020, 31, 669–686. [Google Scholar] [CrossRef] [PubMed]
- Cicciù, M.; Fiorillo, L.; D’Amico, C.; Gambino, D.; Amantia, E.M.; Laino, L.; Crimi, S.; Campagna, P.; Bianchi, A.; Herford, A.S.; et al. 3D Digital Impression Systems Compared with Traditional Techniques in Dentistry: A Recent Data Systematic Review. Materials 2020, 13, 1982. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Saccomanno, S.; Saran, S.; Vanella, V.; Mastrapasqua, R.F.; Raffaelli, L.; Levrini, L. The Potential of Digital Impression in Orthodontics. Dent. J. 2022, 10, 147. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Resnick, C.M.; Doyle, M.; Calabrese, C.E.; Sanchez, K.; Padwa, B.L. Is It Cost Effective to Add an Intraoral Scanner to an Oral and Maxillofacial Surgery Practice? J. Oral Maxillofac. Surg. 2019, 77, 1687–1694. [Google Scholar] [CrossRef] [PubMed]
- Sampaio-Fernandes, M.A.; Pinto, R.J.; Almeida, P.R.; Sampaio-Fernandes, M.M.; Silva Marques, D.N.; Figueiral, M.H. Direct vs. Indirect Digital Implant Impressions: A Time and Cost Analysis. Dent. J. 2024, 12, 340. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Muçolli, G.; Nikç, F.; Muçolli, G. Intraoral scanners and conventional impressions: A literature review. Georgian Med. News 2024, 356, 94–99. Available online: https://pubmed.ncbi.nlm.nih.gov/39855170/ (accessed on 27 May 2025). [PubMed]
- Joda, T.; Gintaute, A.; Brägger, U.; Ferrari, M.; Weber, K.; Zitzmann, N.U. Time-efficiency and cost-analysis comparing three digital workflows for treatment with monolithic zirconia implant fixed dental prostheses: A double-blinded RCT. J. Dent. 2021, 113, 103779. [Google Scholar] [CrossRef] [PubMed]
- Ille, C.E.; Jivănescu, A.; Pop, D.; Stoica, E.T.; Flueras, R.; Talpoş-Niculescu, I.C.; Cosoroabă, R.M.; Popovici, R.A.; Olariu, I. Exploring the Properties and Indications of Chairside CAD/CAM Materials in Restorative Dentistry. J. Funct. Biomater. 2025, 16, 46. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Son, K.; Lee, W.S.; Lee, K.B. Prediction of the learning curves of 2 dental CAD software programs. J. Prosthet. Dent. 2019, 121, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Suganna, M.; Nayakar, R.P.; Alshaya, A.A.; Khalil, R.O.; Alkhunaizi, S.T.; Kayello, K.T.; Alnassar, L.A. The Digital Era Heralds a Paradigm Shift in Dentistry: A Cross-Sectional Study. Cureus 2024, 16, e53300. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lam, W.Y.; Mak, K.C.; Maghami, E.; Molinero-Mourelle, P. Dental students’ preference and perception on intraoral scanning and impression making. BMC Med. Educ. 2021, 21, 501. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criterion | Inclusion | Exclusion |
|---|---|---|
| Time period | Publications available between January 2010 and March 2025 | All publications published before January 2010 |
| Language | English | Non-English |
| Type of articles | All research types, including primary research (e.g., case studies, in vitro studies, and reviews); full text available | Letters, books, book chapters, case reports lacking details on the dental materials used and full text not available |
| Authors/Year | Title | Methods | Results |
|---|---|---|---|
| Zandinejad et al. (2015) [34] | Digital Workflow for Virtually Designing and Milling Ceramic Lithium Disilicate Veneers: A Clinical Report | A 43-year-old man with diastemas and esthetic concerns was treated with multiple lithium disilicate veneers. Digital impressions (Lava COS scanner) were taken after tooth preparation. A fully digital workflow was used for virtual design and remote milling of provisional and final restorations without physical casts. Final veneers were etched, silanated, and bonded with light-cure resin cement. | After one-year follow-up, all veneers exhibited excellent marginal fit, shape, contour, and esthetics. The digital workflow allowed high precision and predictable outcomes, although limitations in artistic detailing with the CAD software were noted. |
| Lin W.-S. et al. (2015) [35] | Predictable Restorative Workflow for CAD/CAM-Fabricated Ceramic Veneers Utilizing a Virtual Smile Design Principle | A 45-year-old woman received CAD/CAM lithium disilicate veneers on anterior teeth (canine to canine). Treatment included virtual smile design, intraoral scanning (iTero), and digital wax-up. | Intraoral scanning enabled precise digital planning and esthetic predictability. The workflow improved communication with the lab and achieved a successful esthetic result. |
| Stanley M et al. (2018) [36] | Fully digital workflow, integrating dental scan, smile design and CAD-CAM: case report | 47-year-old male; intraoral scanning using Carestream CS 3500 and CS 3600, digital smile design protocol, CAD/CAM fabrication of monolithic lithium disilicate veneers and crowns; minimal invasive preparation. | After treatment, the patient showed stable restorations with no fractures at 6-month follow-up, reported improved comfort and TMJ symptom relief, and adapted well to the increased vertical dimension. The digital workflow was efficient and accurate, but long-term studies are still needed. |
| Revilla-León M et al. (2019) [37] | Digital tools and 3D printing technologies integrated into the workflow of restorative treatment: A clinical report | 58-year-old male; intraoral scanning performed with TRIOS 3 (3Shape). Full digital workflow used: intraoral scans, digital smile design, 3D printed mock-ups, CAD/CAM design of lithium disilicate veneers, milling and DLP additive manufacturing for definitive casts. | The fully digital workflow provided efficient treatment planning, precise esthetics, and predictable outcomes. Intraoral scanning and digital techniques allowed minimal intervention and high patient satisfaction with the final lithium disilicate veneer restorations. |
| Zhivago P et al. (2022) [38] | A comprehensive technique using digital workflow to improve an unpleasant smile: A clinical report | 42-year-old female; intraoral scanning performed using Medit i500 scanner. Smile design created with Smilecloud software, further sculpted with ZBrush software. Three-dimensionally printed mock-up fabricated with SprintRay Pro 55 printer. Lithium disilicate veneers (IPS e.max CAD) were fabricated and cemented. | The fully digital workflow allowed accurate visualization, planning, and realization of the esthetic rehabilitation. The integration of intraoral scanning, facial scans, digital smile design, and 3D-sculpting software provided efficient communication and predictable final esthetic results. |
| Rathee M et al. (2023) [39] | Anterior esthetic rehabilitation with full and partial veneers using conventional and digital techniques: A case series | Three cases: Conventional impressions were used for veneer cases. In Case 3, a digital workflow was incorporated with a desktop scanner (SMART Open Technologies FARO Europe) and Exocad software to create a virtual diagnostic wax-up and 3D-printed mock-up for zirconia restorations. | The digital workflow allowed accurate design and space evaluation for complex anterior rehabilitation. In all cases, patients were highly satisfied with esthetic results at 1-year follow-up. Digital techniques improved planning precision and restorative outcomes, particularly in cases with complex edentulous spaces. |
| Figueira J et al. (2023) [40] | Veneer tooth preparation utilizing a novel digital designed workflow: A case report | 42-year-old male; intraoral scanning performed to capture digital records for digital wax-up. Virtual guided tooth preparation designed using a BFEP (Bonded Functional Esthetic Prototype). 3D printed preparation guides were used to guide minimal and accurate enamel reduction. Final digital impressions taken after preparation. Veneers fabricated with CAD/CAM (Empress CAD Multi). | The fully digital workflow enabled precise and conservative preparation, preserving maximum enamel. Final restorations achieved excellent esthetics and patient satisfaction. The guided preparation protocol reduced operator error and improved predictability of the outcome. |
| Pandey et al. (2024) [41] | Trios Lidisi Veneer, Transforming Smiles Using an Intraoral Scanner—A Case Report | A 26-year-old female with anterior spacing was treated with lithium disilicate veneers. Intraoral scanning was performed using a Trios scanner after minimal tooth preparation. Digital models were created and 3D-printed, veneers were milled from lithium disilicate blocks, and restorations were adhesively cemented. | Six-month follow-up showed excellent esthetics, stable restorations, and full patient satisfaction with form, function, and appearance. The digital workflow improved precision, comfort, and efficiency compared to conventional impressions. |
| Santi M et al. (2024) [42] | Advanced digital planning approach using a 3D-printed mock-up. A case report | 45-year-old female; intraoral scanning with Trios 3 (3Shape) after clinical evaluation. Three-dimensional design using Exocad software, digital smile design applied, and a 0.6 mm thick mock-up 3D-printed from resin. Final plan based on the printed mock-up approved by patient. | The fully digital workflow, combining intraoral scanning and 3D printing, allowed an accurate and efficient preview of the esthetic outcome. The mock-up matched patient expectations and guided final restoration planning. The procedure was efficient, predictable, and cost-effective. |
| Sanchez RLS et al. (2024) [43] | Replacement of unsatisfactory ceramic veneers with the aid of a digital workflow | Case report of a woman in her 30s whose old veneers were replaced using a fully digital workflow. The process included intraoral scanning, digital wax-up, mock-up, tooth preparation, CAD design, and fabrication of leucite-reinforced ceramic veneers. | The digital workflow allowed improved communication, better control of marginal fit, reduced overcontouring, and enhanced esthetic and periodontal outcomes. At 1-year follow-up, the patient showed functional, esthetic restorations with no gingival inflammation. |
| Osorio-Vélez L.S. et al. (2024) [44] | A Conservative Approach to Ceramic Laminates in the Anterior Region: A Clinical Report | 40-year-old female; intraoral scan performed with TRIOS 3 (3Shape) for digital smile design, planning, and fabrication of minimal thickness (0.4 mm) lithium disilicate veneers. | The digital workflow, including intraoral scanning, enabled precise diagnosis, conservative tooth preparation, improved esthetics, and high patient satisfaction. |
| Al Hamad KQ et al. (2025) [45] | Virtual patient representation with silicone guide and a 3D scanner accessory for a user-friendly facial scanning workflow: A clinical report of smile design and ceramic veneers | 23-year-old female; intraoral scanning using Omnicam (Dentsply Sirona) and facial scanning with a Structure Sensor Pro (Occipital Inc) mounted on an iPad. Digital Smile Design (DSD) and 3D facial scans integrated with intraoral scans using a silicone guide for file alignment. Ceramic veneers fabricated using CAD/CAM workflow. | The use of intraoral and facial scans with a simple silicone guide provided an efficient and user friendly digital workflow. Veneers showed excellent fit, esthetics, and patient satisfaction. The protocol proved predictable and cost-effective for full 3D virtual patient generation and esthetic rehabilitation. |
| Ahmed et al. (2022) [46] | Smile Makeover Utilizing Digital Esthetic Veneers Workflow: A Case Report | A 40-year-old patient seeking to have a new smile to enhance his stained and esthetically unproportional teeth. 3Shape intraoral scanner was used for the diagnosis and final digital impression to fabricate the final veneers from right second premolar to left second premolar. | The use of digital workflow in managing esthetic cases enhanced the treatment predictability and increased the survival and success of the restorations due to the conservation of tooth structure. |
| do Vale Voigt et al. (2020) [47] | DSDapp use for multidisciplinary esthetic planning | 3Shape intraoral scan was used to obtain initial and final impression. Exocad software was used to design the final lithium disilicate veneer restorations | The use of the DSDapp accelerated the initial planning steps and facilitated better communication with the patient and the multidisciplinary team. The use of this application allowed active participation of the patient during the planning process. Additionally, the digital workflow favored greater predictability of the results and achieved the results planned in the DSDapp. |
| Authors/Year | Title | Methods | Results |
|---|---|---|---|
| Boeddinghaus M. et al. (2015) [48] | Accuracy of Single-Tooth Restorations Based on Intraoral Digital and Conventional Impressions in Patients | Clinical study comparing the marginal fit of zirconia copings from three IOSs (3M True Definition, TRIOS, Omnicam) and a conventional impression scanned in lab (3Shape D700) in 49 teeth from 24 patients. | Intraoral scanners (especially 3M and TRIOS) achieved marginal gaps comparable or better than conventional impressions. The study concludes digital IOS can be a reliable alternative when the finish line is visible and dry. |
| Hategan S.I. et al. (2018) [49] | Powder and Powder-Free Intraoral Scanners: Digital Impression Accuracy | In vitro study comparing the accuracy of two IOSs (Apollo DI—powder and Omnicam—powder-free) used by students, residents, and specialists to scan crown preparations on a typodont. | Powder-free systems (Omnicam) showed higher precision and better marginal adaptation compared to powder systems. Operator experience significantly affected scan quality. Intraoral scanning, especially powder-free, was concluded to offer high clinical accuracy when properly used. |
| Rotar R.N. et al. (2019) [50] | Trueness and Precision of Two Intraoral Scanners: A Comparative In Vitro Study | In vitro study comparing trueness and precision of Planmeca PlanScan and CEREC Omnicam scanning a prepared molar for an onlay. STL files analyzed with metrology software (Geomagic Control X). | Both scanners showed good accuracy. PlanScan achieved slightly better trueness (48.6 µm) and precision (24.9 µm) than Omnicam (trueness 53 µm, precision 35.6 µm). No statistically significant differences. Intraoral scanning was reliable for onlay preparations. |
| Diker B., et al. (2020) [51] | Comparing the Accuracy of Six Intraoral Scanners on Prepared Teeth and Effect of Scanning Sequence | In vitro study comparing trueness and precision of six IOSs (Trios 3, iTero, Omnicam, Primescan, Emerald, Virtuo Vivo) for single-crown preparations on canines in a full-arch model. Ten scans per scanner. | Primescan showed highest trueness (25 µm) and precision (10 µm), followed by Trios and Omnicam. Emerald had the lowest accuracy. Scanning sequence significantly affected iTero accuracy. All results were within clinically acceptable range. |
| Chiu A. et al. (2020) [52] | Accuracy of CAD/CAM Digital Impressions with Different Intraoral Scanner Parameters | In vitro study comparing scan accuracy of 3Shape TRIOS 3 under three resolution settings (Standard, High, Combined) for crown prep finish line on typodont molar. Trueness assessed via Geomagic Control X. | All settings yielded high trueness (<34 µm). No significant difference in accuracy among resolution modes. Accuracy was clinically acceptable; scanner resolution had minimal impact on finish line accuracy. |
| Son Y.-T. et al. (2022) [53] | Trueness of Intraoral Scanners According to Subgingival Depth of Abutment for Fixed Prosthesis | In vitro study comparing the trueness of two IOSs (i500 and CS3600) at subgingival finish lines (0 mm, 0.25 mm, 0.5 mm, 0.75 mm, and 1 mm) with and without gingival retraction cords. | Without gingival retraction, trueness decreased as subgingival depth increased (>100 μm beyond 0.5 mm). With retraction cord, trueness remained <100 μm at all depths. Gingival retraction improved trueness by ~90%. |
| Casucci A. et al. (2023) [54] | Accuracy of Four Intraoral Scanners in Subgingival Vertical Preparation: An In Vitro 3D Comparative Analysis | In vitro study evaluating trueness and precision of Trios 3, Medit i700, Vivascan, and Experimental GC IOS in full crowns with subgingival margins (#16, #21). | All IOS showed clinically acceptable accuracy on full abutments (<100 µm RMS). Experimental GC IOS had best precision. Vivascan showed lower performance. Accuracy decreased at subgingival margins. |
| Giuliodori G. et al. (2023) [55] | Intraoral Scans of Full Dental Arches: An In Vitro Measurement Study of the Accuracy of Different Intraoral Scanners | In vitro study, using 6 IOSs (Medit i700, Primescan, Trios 4, iTero 5D, Omnicam, Dexis IS 3700), scanning an epoxy maxillary model with different strategies. Three hundred scans compared to industrial reference scanner. | Medit i700 and Primescan showed the best trueness and precision (<25 µm). Scanning strategy and operator experience influenced scan time but not clinically significant accuracy. All IOSs achieved acceptable accuracy. |
| Yang C.-H. et al. (2023) [56] | A Double-Blinded Trial to Compare the Patient Satisfaction and Crown Accuracy of Two Different Intraoral Scanners for the Fabrication of Monolithic Lithium Disilicate Single Crowns | Clinical study (double-blinded crossover trial) comparing Carestream CS3500 vs. MIRDC IOS for scanning posterior tooth-supported crowns in 15 patients (n = 40 crowns). Assessed patient satisfaction and crown accuracy (fit, proximal and occlusal contact, general satisfaction). | Both scanners provided high patient satisfaction. Carestream CS3500 showed significantly better accuracy in all crown quality metrics (mean accuracy score 13.3 vs. 6.1, p < 0.001). MIRDC IOS was less clinically acceptable. |
| Park Y. et al. (2023) [57] | Scanning Accuracy of an Intraoral Scanner According to Different Inlay Preparation Designs | In vitro study comparing the accuracy (trueness and precision) of CEREC Primescan for 4 inlay designs on mandibular molars, varying occlusal cavity depth and gingival floor width. Ten scans per group; 3D analysis with GOM Inspect. | The Primescan achieved high accuracy (trueness ~18.5–20.8 μm). Wide and deep cavity designs yielded significantly better trueness. All results were within clinically acceptable range. The study confirms IOS can reliably capture inlay preparations if design allows proper access. |
| Liu X. et al. (2024) [58] | Accuracy and Efficiency of Digitally Fabricated All-Ceramic Crowns from Conventional Impressions and Intraoral Scans | Single-blind RCT comparing TRIOS intraoral scanning vs. PVS impressions (n = 70 crowns). Evaluated marginal/internal fit, adjustment time, occlusal contacts, and dentist satisfaction (VAS). | Intraoral scanning showed significantly better marginal fit (57.9 µm vs. 83 µm), shorter adjustment times, better internal fit, and higher dentist satisfaction (VAS = 8.95 vs. 7.95, p < 0.05). Authors concluded IOS was more accurate and efficient than conventional techniques. |
| Kwon et al. (2024) [59] | Evaluating the Accuracy of CEREC Intraoral Scanners for Inlay Restorations: Impact of Adjacent Tooth Materials | In vitro study evaluating the trueness and precision of Primescan, Omnicam, and Bluecam scanners for inlay restorations on tooth-supported models. | All scanners showed clinically acceptable accuracy. Bluecam achieved the highest trueness. Adjacent gold surfaces improved scanning accuracy compared to zirconia and resin. |
| Authors/Year | Title | Methods | Results |
|---|---|---|---|
| Revilla-Leon et al. (2025) [60] | Accuracy of Intraoral Scanner Systems for Fabricating Inlay, Onlay, and Veneer Restorations: A Systematic Review and Meta-Analysis | A literature search was conducted in PubMed, Scopus, Embase, Web of Science, and Cochrane. A total of 34 articles were included in the analysis, with 17 focusing on the accuracy of definitive virtual casts and 17 evaluating marginal and internal discrepancies. | Better trueness but worse precision was observed in the definitive virtual casts of inlay restorations compared to those of onlay restorations. The impression method used did not affect the marginal discrepancy of inlay and onlay restorations. Further studies are needed to evaluate the accuracy of definitive virtual casts for fabricating veneer restorations using intraoral scanners and to assess the fit of the fabricated veneer restorations. |
| Ahmed et al. (2024) [61] | Mapping the Landscape of the Digital Workflow of Esthetic Veneers from Design to Cementation: A Systematic Review | Twenty articles were chosen to evaluate the digital veneer workflow and the accuracy of digital preparations and cementation guidelines for laminate veneers. | Based on our findings, the digitally fabricated laminate-veneer workflow demonstrated superior predictability and accuracy compared to the conventional workflow. |
| Pradies et al. (2025) [62] | Comparative Influence of Marginal Design and Digital Scanning Accuracy on the Clinical Longevity of Ceramic Restorations: An Evidence-Based Approach. Consensus Statement From SSRD, SEPES, and PROSEC Conference on Minimally Invasive Restorations | Two systematic reviews with meta-analyses were conducted following PRISMA guidelines. The first review analyzed 15 studies comparing vertical and horizontal finishing lines. The second review included 33 studies on IOS accuracy for inlays, onlays, and veneers. | Vertical and horizontal finish lines demonstrated no significant differences in restoration survival, success rates (65–100%), or periodontal outcomes over 3–7 years. Intraoral scans reliably fabricated single-unit inlay and onlay restorations with high accuracy, but data on veneer restorations remained inconclusive due to limited studies. |
| Alghauli ET AL (2024) [63] | 3D-printed intracoronal restorations, occlusal and laminate veneers: Clinical relevance, properties, and behavior compared to milled restorations; a systematic review and meta-analysis | All studies that assessed 3D-printed partial coverage restorations, including inlays, onlays, laminate, and occlusal veneers, were retrieved. Seventeen records were included in the final review. | Three-dimensionally printed laminate veneers and intracoronal restorations exhibited superior trueness, as well as better marginal and internal fit compared to milled restorations. Some limitations still accompany the resin materials, but this could be overcome by further development of the materials and printing technology. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas-Rueda, S.; Robles, M.; Pagan-Banchs, M.; Garcia, P.; Algamaiah, H.; Jurado, C.A.; Alshabib, A. Accuracy of Digital Impressions for Veneer Restorations: A Narrative Review and Case Illustration. J. Clin. Med. 2025, 14, 3859. https://doi.org/10.3390/jcm14113859
Rojas-Rueda S, Robles M, Pagan-Banchs M, Garcia P, Algamaiah H, Jurado CA, Alshabib A. Accuracy of Digital Impressions for Veneer Restorations: A Narrative Review and Case Illustration. Journal of Clinical Medicine. 2025; 14(11):3859. https://doi.org/10.3390/jcm14113859
Chicago/Turabian StyleRojas-Rueda, Silvia, Manuel Robles, Margiezel Pagan-Banchs, Pablo Garcia, Hamad Algamaiah, Carlos A. Jurado, and Abdulrahman Alshabib. 2025. "Accuracy of Digital Impressions for Veneer Restorations: A Narrative Review and Case Illustration" Journal of Clinical Medicine 14, no. 11: 3859. https://doi.org/10.3390/jcm14113859
APA StyleRojas-Rueda, S., Robles, M., Pagan-Banchs, M., Garcia, P., Algamaiah, H., Jurado, C. A., & Alshabib, A. (2025). Accuracy of Digital Impressions for Veneer Restorations: A Narrative Review and Case Illustration. Journal of Clinical Medicine, 14(11), 3859. https://doi.org/10.3390/jcm14113859