

Use of Prophylactic Methylxanthines to Prevent Extubation Failure in Preterm Neonates with a Birth Weight of 1250–2499 g: A Propensity Score-Matched Analysis

 ,
,  , , , ,
, , , ,
Abstract

1. Introduction
2. Methods
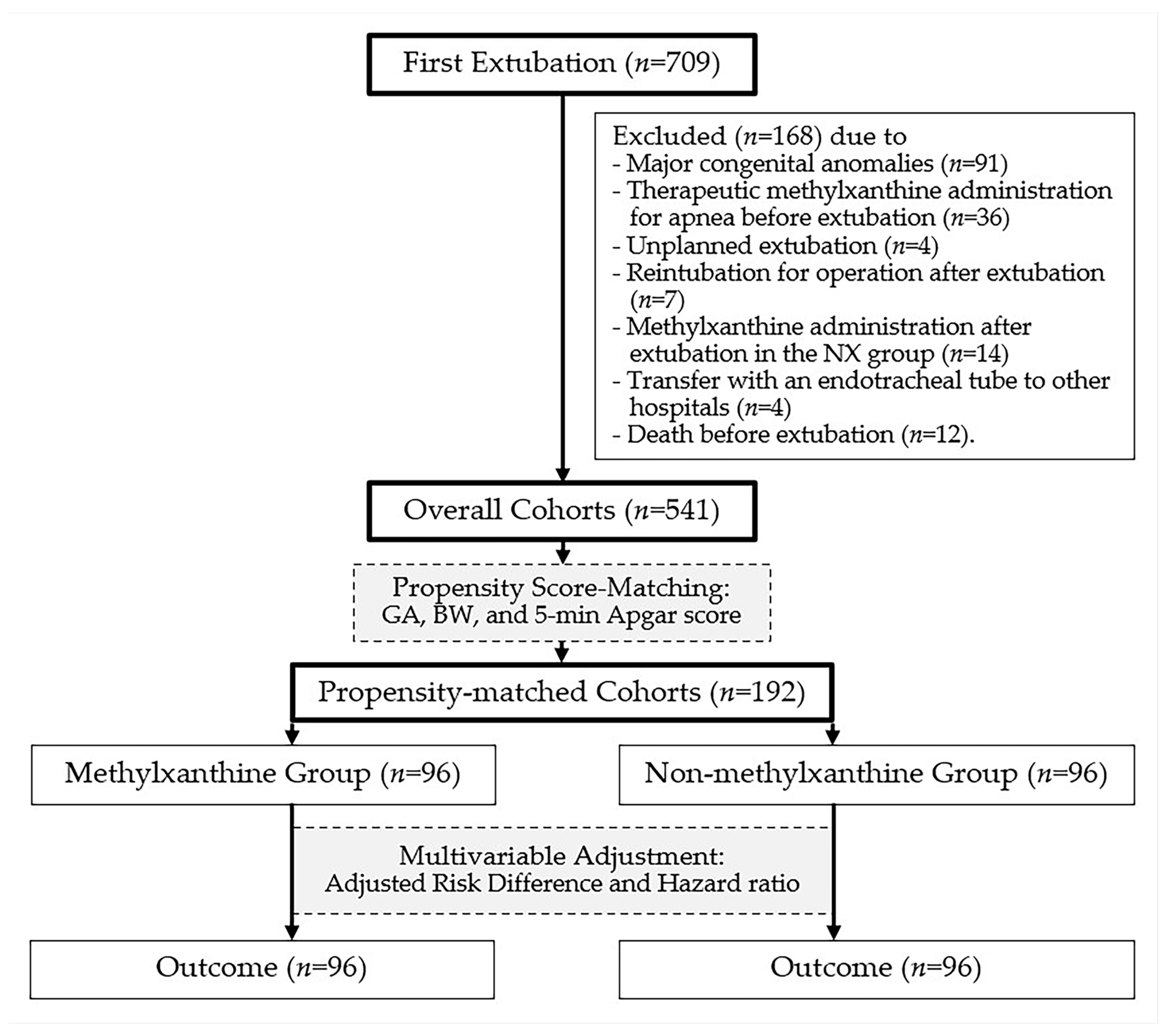
2.1. Study Design and Patient Domains
2.2. Ventilatory Care
2.3. Exposure, Comorbidities, and Outcomes
2.4. Sample Size Calculation
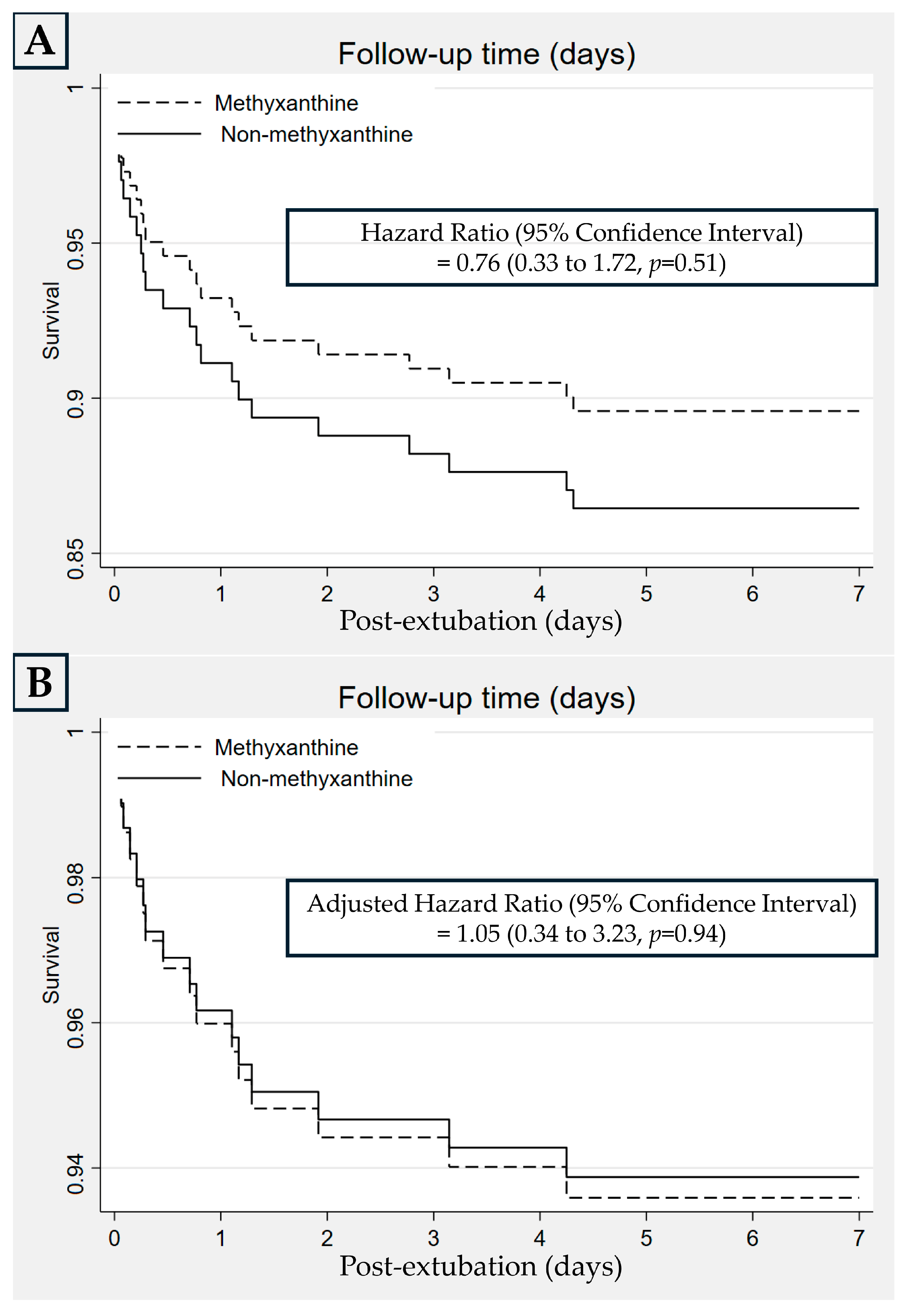
2.5. Statistical Analysis
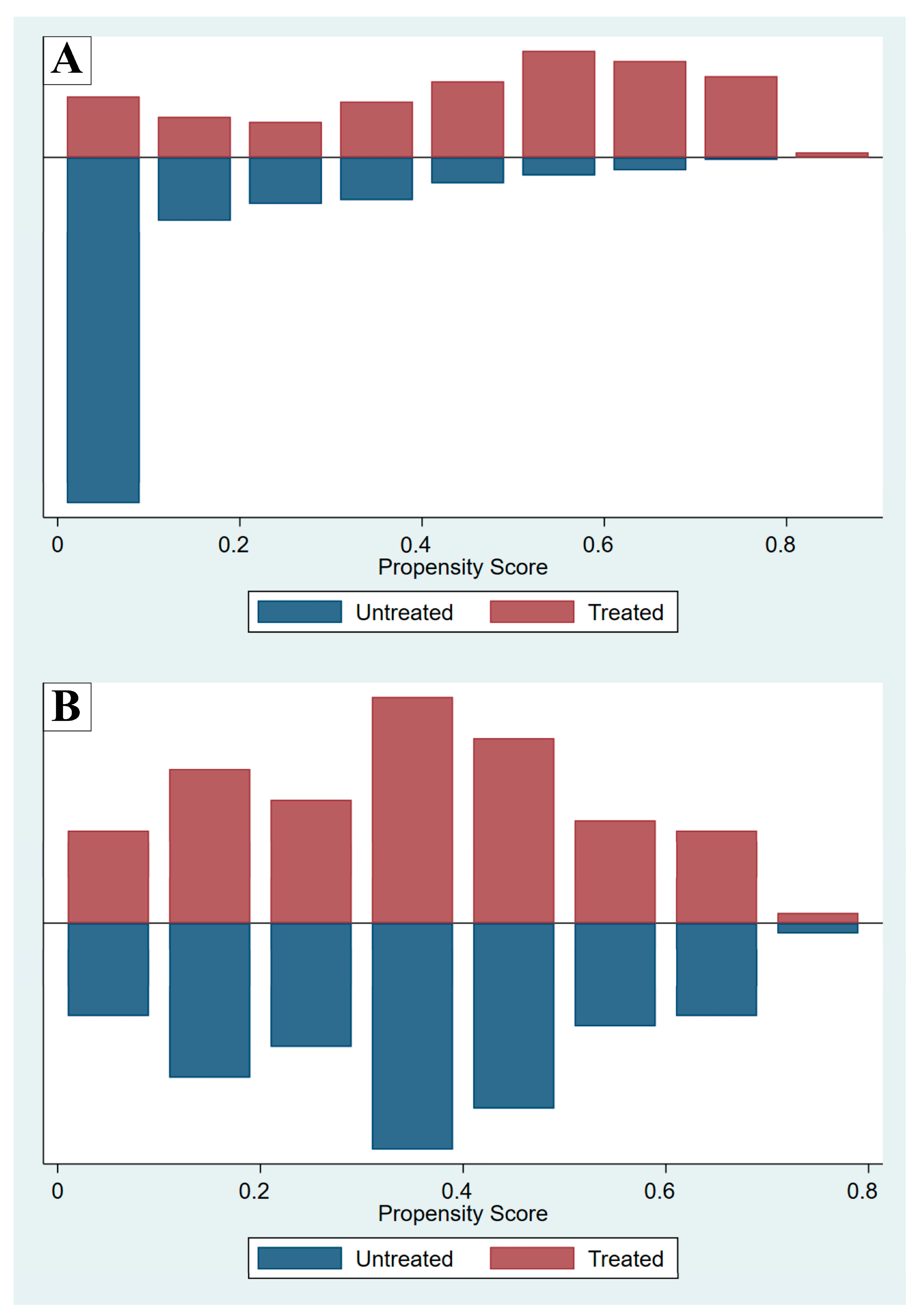
2.6. Propensity Score Matching
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AOP | apnea of prematurity |
| CAP | Caffeine for Apnea of Prematurity |
| BW | birth weight |
| BPD | bronchopulmonary dysplasia |
| LBW | low-birth weight |
| NIV | non-invasive ventilation |
| nCAP | nasal continuous positive airway pressure |
| GA | gestational age |
| HFOV | high-frequency oscillatory ventilation |
| nHFVO | nasal high-frequency oscillatory ventilation |
| n(S)IPPV | nasal (synchronized) intermittent positive pressure |
| IV | intravenous |
| MX group | methylxanthine group |
| NX group | non-methylxanthine group |
| PDA | patent ductus arteriosus |
| RD | risk difference |
| HR | hazard ratio |
| CI | confidence interval |
References
- Schmidt, B.; Roberts, R.S.; Davis, P.; Doyle, L.W.; Barrington, K.J.; Ohlsson, A.; Solimano, A.; Tin, W.; Caffeine for Apnea of Prematurity Trial Group. Caffeine therapy for apnea of prematurity. N. Engl. J. Med. 2006, 354, 2112–2121. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.; Roberts, R.S.; Davis, P.; Doyle, L.W.; Barrington, K.J.; Ohlsson, A.; Solimano, A.; Tin, W.; Caffeine for Apnea of Prematurity Trial Group. Long-term effects of caffeine therapy for apnea of prematurity. N. Engl. J. Med. 2007, 357, 1893–1902. [Google Scholar] [CrossRef] [PubMed]
- Mürner-Lavanchy, I.M.; Doyle, L.W.; Schmidt, B.; Roberts, R.S.; Asztalos, E.V.; Costantini, L.; Davis, P.G.; Dewey, D.; D’Ilario, J.; Grunau, R.E.; et al. Caffeine for Apnea of Prematurity (CAP) Trial Group. Neurobehavioral outcomes 11 years after neonatal caffeine therapy for apnea of prematurity. Pediatrics 2018, 141, e20174047. [Google Scholar] [CrossRef]
- Henderson-Smart, D.J.; Davis, P.G. Prophylactic methylxanthines for endotracheal extubation in preterm infants. Cochrane Database Syst. Rev. 2010, 12, CD000139. [Google Scholar] [CrossRef]
- Durand, D.J.; Goodman, A.; Ray, P.; Ballard, R.A.; Clyman, R.I. Theophylline treatment in the extubation of infants weighing less than 1250 grams: A controlled trial. Pediatrics 1987, 80, 684–688. [Google Scholar] [CrossRef] [PubMed]
- Viscardi, R.M.; Faix, R.G.; Nicks, J.J.; Grasela, T.H. Efficacy of theophylline for prevention of post-extubation respiratory failure in very low birth weight infants. J. Pediatr. 1985, 107, 469–472. [Google Scholar] [CrossRef]
- Muro, M.; Perez-Rodriguez, J.; Garcia, M.; Arroyo, I.; Quero, J. Efficacy of caffeine for weaning premature infants from mechanical ventilation. Effects on pulmonary function. J. Perinat. Med. 1992, 20, 315. [Google Scholar]
- Pearlman, S.; Stefano, J. Caffeine(C.). vs theophylline (T) to facilitate extubation in preterm infants with RDS. In Pediatric Research; Williams & Wilkins: Baltimore, MD, USA, 1991; p. 362. [Google Scholar]
- Barrington, K.J.; Finer, N.N. A randomized, controlled trial of aminophylline in ventilatory weaning of premature infants. Crit. Care Med. 1993, 21, 846–850. [Google Scholar] [CrossRef]
- Greenough, A.; Elias-Jones, A.; Pool, J.; Morley, C.J.; Davis, J.A. The therapeutic actions of theophylline in preterm ventilated infants. Early Hum. Dev. 1985, 12, 15–22. [Google Scholar] [CrossRef]
- Hoff Calegari, L.; Goyal, M.; Dutta, S.; Mukerji, A. Predictors and outcomes of extubation failure in preterm neonates: A systematic review. Pediatrics 2025, 155, e2024068677. [Google Scholar] [CrossRef]
- Chen, F.; Chen, Y.; Wu, Y.; Zhu, X.; Shi, Y. A nomogram for predicting extubation failure in preterm infants with gestational age less than 29 weeks. Neonatology 2023, 120, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.; Hu, Z.; Yu, G.; Luo, Y.; Xiong, X.; Yang, Q.; Song, W.; Yu, Y.; Yang, T. Predictors of extubation failure in newborns: A systematic review and meta-analysis. Ital. J. Pediatr. 2023, 49, 133. [Google Scholar] [CrossRef]
- Natarajan, A.; Lam, G.; Liu, J.; Beam, A.L.; Beam, K.S.; Levin, J.C. Prediction of extubation failure among low birthweight neonates using machine learning. J. Perinatol. 2023, 43, 209–214. [Google Scholar] [CrossRef] [PubMed]
- CDC; NHSN. Pneumonia (Ventilator-Associated [VAP] and Non-Ventilator-Associated Pneumonia [PNEU]) Event. Available online: http://www.cdc.gov/nhsn/pdfs/pscmanual/6pscvapcurrent.pdf (accessed on 31 January 2024).
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Bell, M.J.; Ternberg, J.L.; Feigin, R.D.; Keating, J.P.; Marshall, R.; Barton, L.; Brotherton, T. Neonatal necrotizing enterocolitis: Therapeutic decisions based upon clinical staging. Ann. Surg. 1978, 187, 1–7. [Google Scholar] [CrossRef]
- Marques, K.A.; Bruschettini, M.; Roehr, C.C.; Davis, P.G.; Fiander, M.; Soll, R. Methylxanthine for the prevention and treatment of apnea in preterm infants. Cochrane Database Syst. Rev. 2023, 10, CD013830. [Google Scholar] [CrossRef]
- Prasad, R.; Saha, B.; Sk, M.H.; Sahoo, J.P.; Gupta, B.K.; Shaw, S.C. Noninvasive high-frequency oscillation ventilation as post-extubation respiratory support in neonates: Systematic review and meta-analysis. PLoS ONE 2024, 19, e0307903. [Google Scholar] [CrossRef]
- Phatigomet, M.; Thatrimontrichai, A.; Maneenil, G.; Dissaneevate, S.; Janjindamai, W. Reintubation rate between nasal high-frequency oscillatory ventilation versus synchronized nasal intermittent positive pressure ventilation in neonates: A parallel randomized controlled trial. Am. J. Perinatol. 2024, 41, 1504–1511. [Google Scholar] [CrossRef] [PubMed]
- Lemyre, B.; Deguise, M.O.; Benson, P.; Kirpalani, H.; De Paoli, A.G.; Davis, P.G. Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation. Cochrane Database Syst. Rev. 2023, 7, CD003212. [Google Scholar] [CrossRef]
- Wang, K.; Yue, G.; Gao, S.; Li, F.; Ju, R. Non-invasive high-frequency oscillatory ventilation (NHFOV) versus nasal continuous positive airway pressure (NCPAP) for preterm infants: A systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2024, 109, 397–404. [Google Scholar] [CrossRef]
- Thatrimontrichai, A.; Sirianansopa, K.; Janjindamai, W.; Dissaneevate, S.; Maneenil, G. Comparison of endotracheal reintubation between nasal high-frequency oscillation and continuous positive airway pressure in neonates. Am. J. Perinatol. 2020, 37, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Baingam, K.; Phatigomet, M.; Thatrimontrichai, A.; Maneenil, G.; Dissaneevate, S.; Janjindamai, W. Carbon dioxide level between nasal high-frequency oscillatory ventilation and synchronized nasal intermittent positive pressure ventilation after extubation in neonates: A cross-over randomized controlled trial. Am. J. Perinatol. 2024, 41, 1495–1503. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristic | Overall Cohort (n = 541) | Propensity Score-Matched Cohort (n = 192) | ||||||
|---|---|---|---|---|---|---|---|---|
| MX (n = 110) | NX (n = 431) | Standardized Difference | p-Value | MX (n = 96) | NX (n = 96) | Standardized Difference | p-Value | |
| Gestational age, weeks | 30.7 ± 1.8 | 32.9 ± 2.1 | 1.16 | <0.01 | 30.9 ± 1.9 | 31.0 ± 2.0 | 0.02 | 0.88 |
| Birth weight, g | 1551 ± 280 | 1916 ± 346 | 1.16 | <0.01 | 1583 ± 285 | 1586 ± 263 | 0.01 | 0.95 |
| 5-min Apgar score | 9 (7–9) | 9 (8–9) | 0.15 | 0.16 | 9 (7–9) | 9 (7–9) | 0.004 | 0.94 |
| Baseline Characteristic | MX (n = 96) | NX (n = 96) | p-Value |
|---|---|---|---|
| Inborn neonate, n (%) | 95 (99.0) | 72 (75.0) | <0.01 |
| Multifetal gestation, n (%) | 28 (29.2) | 16 (16.7) | 0.04 |
| Cesarean section, n (%) | 79 (82.3) | 65 (67.7) | 0.02 |
| Male sex, n (%) | 56 (58.3) | 51 (53.1) | 0.47 |
| Respiratory distress syndrome, n (%) | 88 (91.7) | 56 (58.3) | <0.01 |
| Surfactant administration, n (%) | 50 (52.1) | 31 (32.3) | 0.01 |
| Ventilator-associated pneumonia, n (%) | 2 (2.1) | 3 (3.1) | 0.65 |
| Patent ductus arteriosus, n (%) | 43 (44.8) | 24 (25.0) | <0.01 |
| Persistent pulmonary hypertension, n (%) | 1 (1.0) | 5 (5.2) | 0.10 |
| Risk Factors on Date of Extubation | MX (n = 96) | NX (n = 96) | p-Value |
| Body weight, g a | 1559 ± 296 | 1722 ± 378 | <0.01 |
| Postnatal age, days b | 2 (1–5) | 3 (1–15) | 0.02 |
| Mean airway pressure, cmH2O a | 7.5 ± 1.2 | 7.1 ± 1.4 | 0.08 |
| Fraction of inspired oxygen a | 0.27 ± 0.06 | 0.29 ± 0.07 | 0.16 |
| Arterial pH a | 7.36 ± 0.07 | 7.35 ± 0.06 | 0.26 |
| Arterial pCO2, mmHg b | 38.5 (32.8–44.0) | 39.8 (34.9–45.5) | 0.22 |
| Sedative drug use, n (%) | 5 (5.2) | 2 (2.1) | 0.25 |
| New modes of non-invasive ventilation, n (%) | 60 (62.5) | 33 (34.4) | <0.01 |
| Outcome | MX (n = 96), n (%) | NX (n = 96), n (%) | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|---|---|
| RD (95% CI) | p-Value | Adjusted RD (95% CI) a | p-Value | |||
| Extubation failure within 7 days | ||||||
| Birth weight 1250–2499 g | 10/96 (10.4) | 13/96 (13.5) | −0.03 (−0.12, 0.06) | 0.50 | 0.01 (−0.10, 0.13) | 0.83 |
| Birth weight 1250–1999 g | 10/88 (11.4) | 12/88 (13.6) | −0.02 (−0.12, 0.08) | 0.65 | 0.04 (−0.08, 0.16) | 0.50 |
| Birth weight 1250–1499 g | 6/48 (12.5) | 6/48 (12.5) | 0 (−0.13, 0.13) | 1.00 | 0.04 (−0.16, 0.23) | 0.71 |
| Moderate or severe bronchopulmonary dysplasia | 7 (7.3) | 8 (8.3) | −0.01 (−0.09, 0.07) | 0.79 | −0.04 (−0.14, 0.06) | 0.40 |
| Severe neurological injury b | 7/73 (9.6) | 6/57 (10.5) | −0.01 (−0.11, 0.10) | 0.86 | 0.05 (−0.08, 0.17) | 0.44 |
| Feeding intolerance | 17 (17.7) | 5 (5.2) | 0.13 (0.04, 0.21) | 0.01 | 0.10 (−0.03, 0.22) | 0.12 |
| Necrotizing enterocolitis | 6 (6.3) | 6 (6.3) | 0 (−0.07, 0.07) | 1.00 | 0.02 (−0.07, 0.11) | 0.66 |
| Spontaneous intestinal perforation c | 0 (0) | 2 (2.1) | – | – | ||
| Tachycardia c | 1 (1.0) | 3 (3.1) | – | – | ||
| Study Year | Country | Population | Methylxanthine | Extubation Failure (Intervention vs. Control) | Note |
|---|---|---|---|---|---|
| 1985 [10] | UK | <34 weeks | Theophylline | 2/18 vs. 8/20 | BW 1448 g in intervention |
| 1985 [6] | US | <1250 g | Theophylline | 5/14 vs. 10/11 | CPAP after extubation |
| 1987 [5] | US | <1250 g | Aminophylline | 5/23 vs. 15/28 | No CPAP after extubation |
| 1991 [8] | - | <2000 g | Caffeine or Theophylline | 8/31 vs. 4/14 | Proceeding |
| 1992 [7] | Spain | <1750 g | Caffeine | 4/12 vs. 6/6 | BW 1389 g in intervention; some CPAP after extubation |
| 1993 [9] | Canada | <2500 g | Aminophylline | 3/10 vs. 2/10 | BW 1415 g in intervention |
| Meta-analyses of all trials [5,6,7,8,9,10] | 27/108 vs. 45/89 | 25.0% vs. 50.6% | |||
| Some trials [7,8,9,10] excluded infants with a BW < 1250 g [5,6] | 17/71 vs. 20/50 | 23.9% vs. 40.0% | |||
| Present study | 1250–2499 g | Aminophylline, Caffeine | 10/96 vs. 13/96 | Propensity score matching of 541 neonates | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suwankomonkul, P.; Thatrimontrichai, A.; Pakhathirathien, P.; Praditaukrit, M.; Maneenil, G.; Dissaneevate, S.; Trangkhanon, C.; Phon-in, N. Use of Prophylactic Methylxanthines to Prevent Extubation Failure in Preterm Neonates with a Birth Weight of 1250–2499 g: A Propensity Score-Matched Analysis. J. Clin. Med. 2025, 14, 3856. https://doi.org/10.3390/jcm14113856
Suwankomonkul P, Thatrimontrichai A, Pakhathirathien P, Praditaukrit M, Maneenil G, Dissaneevate S, Trangkhanon C, Phon-in N. Use of Prophylactic Methylxanthines to Prevent Extubation Failure in Preterm Neonates with a Birth Weight of 1250–2499 g: A Propensity Score-Matched Analysis. Journal of Clinical Medicine. 2025; 14(11):3856. https://doi.org/10.3390/jcm14113856
Chicago/Turabian StyleSuwankomonkul, Pachima, Anucha Thatrimontrichai, Pattima Pakhathirathien, Manapat Praditaukrit, Gunlawadee Maneenil, Supaporn Dissaneevate, Chamaiporn Trangkhanon, and Neeracha Phon-in. 2025. "Use of Prophylactic Methylxanthines to Prevent Extubation Failure in Preterm Neonates with a Birth Weight of 1250–2499 g: A Propensity Score-Matched Analysis" Journal of Clinical Medicine 14, no. 11: 3856. https://doi.org/10.3390/jcm14113856
APA StyleSuwankomonkul, P., Thatrimontrichai, A., Pakhathirathien, P., Praditaukrit, M., Maneenil, G., Dissaneevate, S., Trangkhanon, C., & Phon-in, N. (2025). Use of Prophylactic Methylxanthines to Prevent Extubation Failure in Preterm Neonates with a Birth Weight of 1250–2499 g: A Propensity Score-Matched Analysis. Journal of Clinical Medicine, 14(11), 3856. https://doi.org/10.3390/jcm14113856