
The Rise and Refinement of Breast Thread Lifting: A Contemporary Review

 , , , and
, , , and
Abstract
1. Introduction
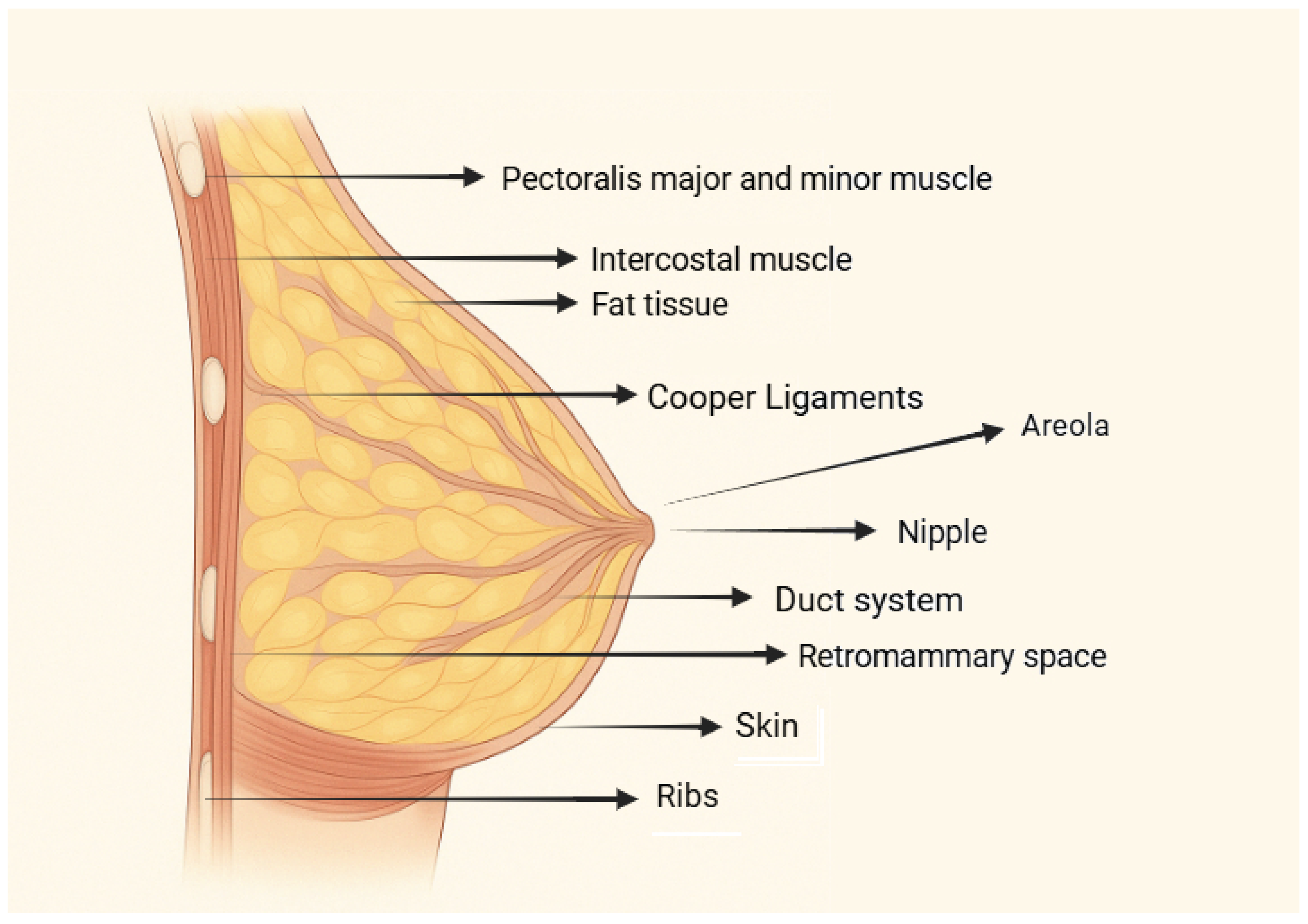
2. Anatomical Breast Structure
3. Scientific Classification of Breast Ptosis
4. Challenges in Surgical Techniques
5. Indications for Surgical Procedures
6. Ultrasonography Evaluation
7. Thread Lifting Technique
7.1. Preoperative Assessment
7.2. Surgical Methods
7.3. Minimally Invasive Approach
8. Innovative Techniques
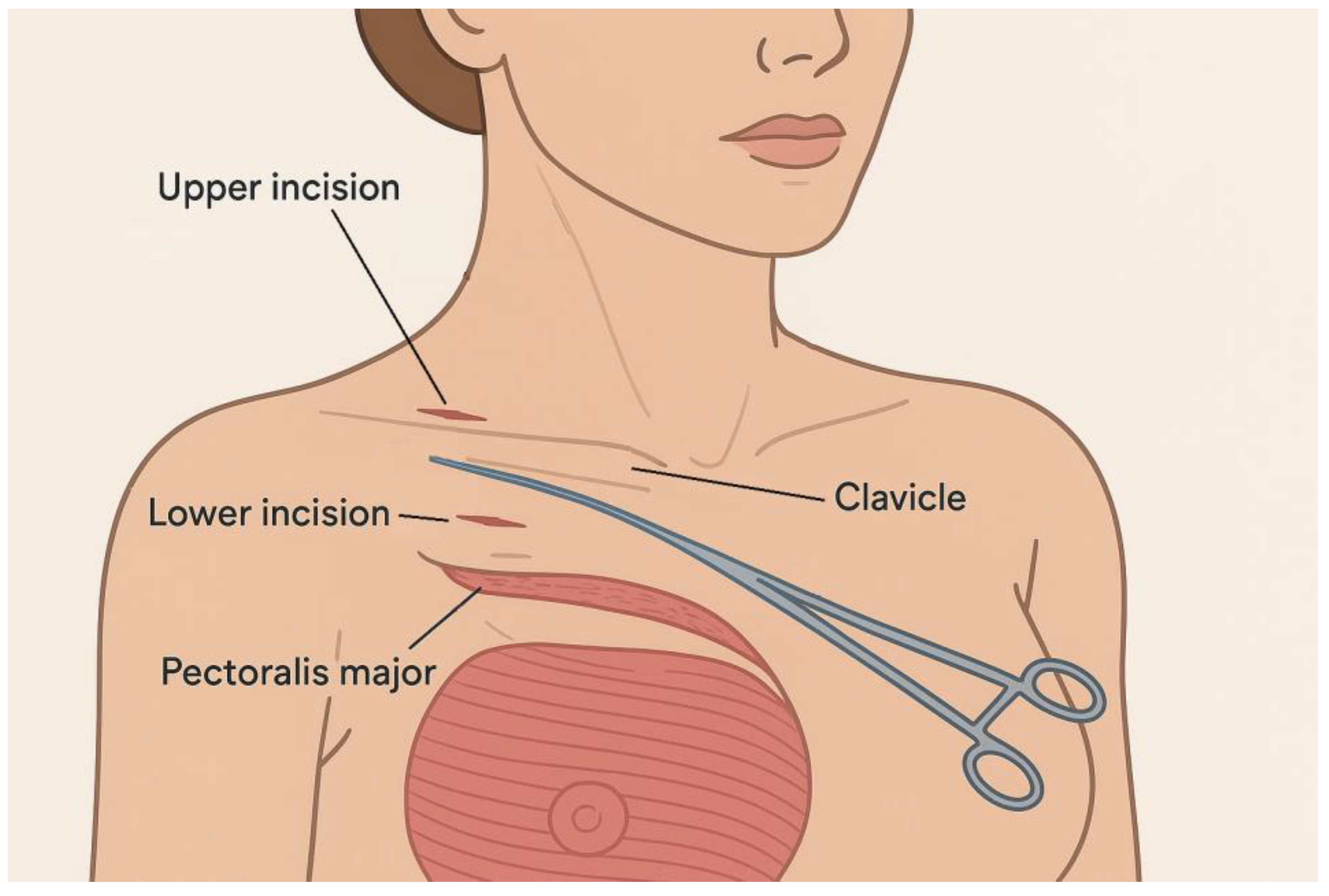
8.1. Thread Stabilization Technique
- -
- The inferior incision is situated at the level of the second intercostal space, adjacent to the fascia of the pectoralis major muscle.
- -
- The superior incision lies just above the clavicle, directly over the periosteal sheath.
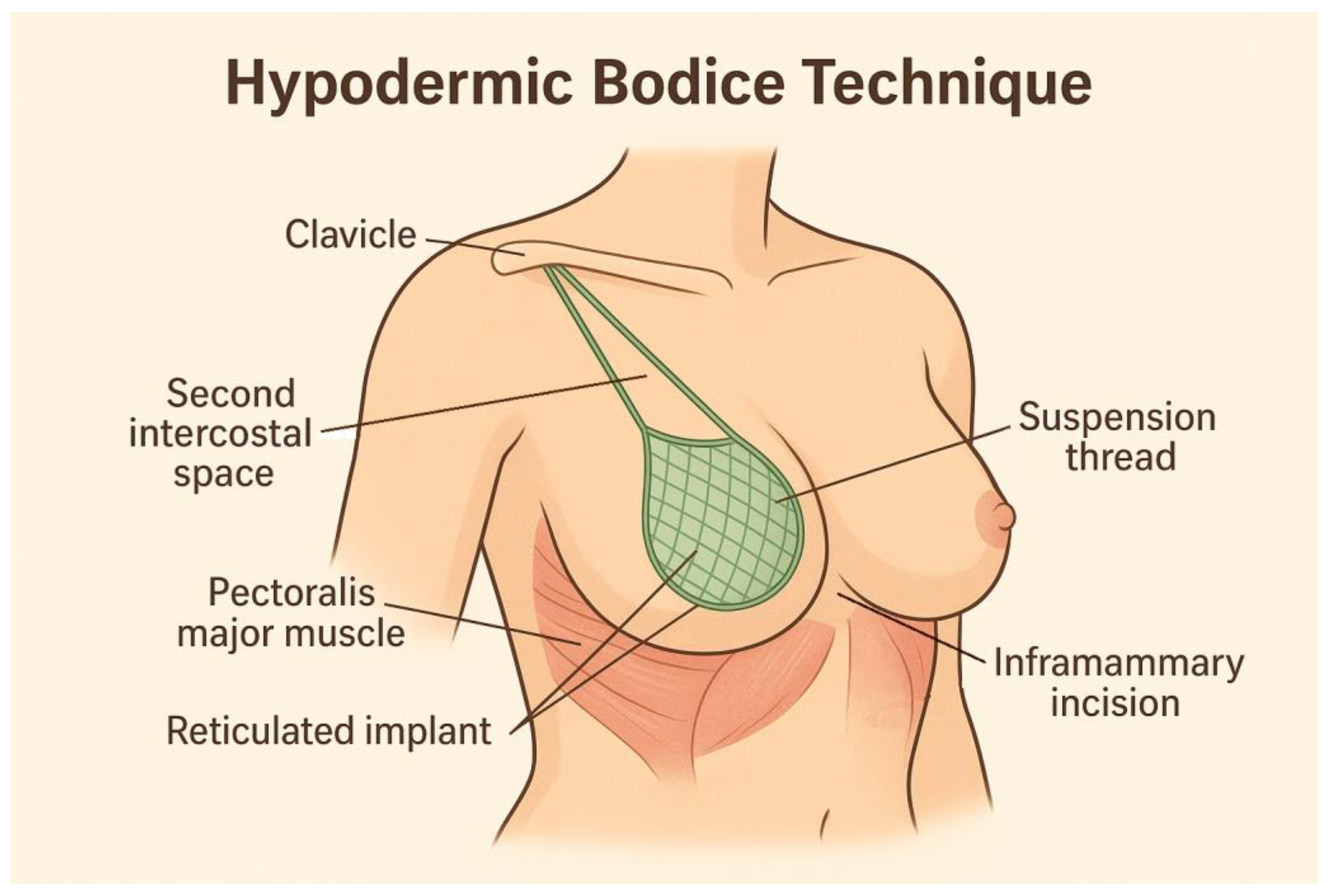
8.2. Hypodermic Bodice Technique
8.3. Multi-Level Subdermal Breast Elevation with Clavicular Thread Anchoring
9. Thread Materials
10. Limitations and Considerations
11. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rinker, B.; Veneracion, M.; Walsh, C.P. Breast Ptosis: Causes and Cure. Ann. Plast. Surg. 2010, 64, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Arora, G.; Arora, S. Thread Lift in Breast Ptosis. J. Cutan. Aesthet. Surg. 2017, 10, 228–230. [Google Scholar] [CrossRef] [PubMed]
- Collier, H. Thread lifting and medical aesthetics: Implantation methods and efficacy. J. Aesthetic Nurs. 2015, 4, 327–331. [Google Scholar] [CrossRef]
- Ali, Y.H. Two years’ outcome of thread lifting with absorbable barbed PDO threads: Innovative score for objective and subjective assessment. J. Cosmet. Laser Ther. 2018, 20, 41–49. [Google Scholar] [CrossRef]
- Khouri, R.K.; Eisenmann-Klein, M.; Cardoso, E.; Cooley, B.C.; Kacher, D.; Gombos, E.; Baker, T.J. Brava and Autologous Fat Transfer Is a Safe and Effective Breast Augmentation Alternative: Results of a 6-Year, 81-Patient, Prospective Multicenter Study. Plast. Reconstr. Surg. 2012, 129, 1173–1187. [Google Scholar] [CrossRef]
- Khouri, R.K.; Schlenz, I.; Murphy, B.J.; Baker, T.J. Nonsurgical Breast Enlargement Using an External Soft-Tissue Expansion System. Plast. Reconstr. Surg. 2000, 105, 2500–2512. [Google Scholar] [CrossRef]
- Mugea, T.T. New Breast Volume and Ptosis Classification System. In Aesthetic Surgery of the Breast; Mugea, T.T., Shiffman, M.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 605–633. [Google Scholar]
- Galbreath, S.; Goswami, T. Biomechanical Behavior of Female Breast—A Review. BioMed 2025, 5, 5. [Google Scholar] [CrossRef]
- Fede, C.; Clair, C.; Pirri, C.; Petrelli, L.; Zhao, X.; Sun, Y.; Macchi, V.; Stecco, C. The Human Superficial Fascia: A Narrative Review. Int. J. Mol. Sci. 2025, 26, 1289. [Google Scholar] [CrossRef]
- Graf, R.M.; Bernardes, A.; Auersvald, A.; Damasio, R.C.C. Subfascial Endoscopic Transaxillary Augmentation Mammaplasty. Aesthetic Plast. Surg. 2000, 24, 216–220. [Google Scholar] [CrossRef]
- Hur, J.H.; Wan, J.; Yoon, S.E.; Wong, S.; Yi, K.H. Anatomical Considerations for Hyaluronic Acid Filler Injection for Breast Augmentation in Young Female Patients. Life 2025, 15, 624. [Google Scholar] [CrossRef]
- Jinde, L.; Jianliang, S.; Xiaoping, C.; Xiaoyan, T.; Jiaqing, L.; Qun, M.; Bo, L. Anatomy and Clinical Significance of Pectoral Fascia. Plast. Reconstr. Surg. 2006, 118, 1557–1560. [Google Scholar] [CrossRef] [PubMed]
- Rehnke, R.D. Clinical Implications of the Fascial System: A Commentary on One Surgeon’s Journey. Life 2024, 14, 89. [Google Scholar] [CrossRef] [PubMed]
- Allen, G.; Nahabedian, M.; Maxwell, P.; Storm, T. Spear’s Surgery of the Breast Principles and Art; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2020; 1850p. [Google Scholar]
- Nahai, F.; Behr, S. The Art of Aesthetic Surgery: Principles and Techniques; Quality Medical Publishing, Inc.: St. Louis, Mo, USA, 2005; 2500p. [Google Scholar]
- Regnault, P. Breast Ptosis. Clin. Plast. Surg. 1976, 3, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Yoshimatsu, H.; Miyashita, H.; Karakawa, R.; Fuse, Y.; Yano, T. Filling the Upper Pole with the Pectoralis Major Muscle Flap in Profunda Femoris Artery Perforator Flap Breast Reconstruction. Medicina 2022, 58, 458. [Google Scholar] [CrossRef] [PubMed]
- Abbed, T.; Chen, C.; Kortesis, B.; Hunstad, J.P.; Bharti, G. Labiaplasty: Current Trends of ASAPS Members. Aesthetic Surg. J. 2018, 38, NP114–NP117. [Google Scholar] [CrossRef]
- Wu, W. Barbed sutures in facial rejuvenation. Aesthetic Surg. J. 2004, 24, 582–587. [Google Scholar] [CrossRef]
- Hong, G.W.; Wan, J.; Yoon, S.E.; Wong, S.; Yi, K.H. Pre- and Post-Procedural Considerations and Thread Types for Thread Lifting. Life 2025, 15, 85. [Google Scholar] [CrossRef]
- Park, S.Y.; Kim, S.; Wan, J.; Samin, K.A.; Lee, K.W.A.; Chan, L.K.W.; Suwanchinda, A.; Yi, K. Reverse and antegrade vector thread lifting techniques: Correcting nasolabial and marionette lines. J. Cosmet. Dermatol. 2024, 23, 4153–4160. [Google Scholar] [CrossRef]
- Salas-López, A.; Morgado-Águila, C.; López-de-Celis, C.; Rodríguez-Sanz, J.; Ortiz-Miguel, S.; Pérez-Bellmunt, A. Breast Vascularization and Its Implication in Breast Reduction and Mastopexy Surgery: Anatomical Study. J. Pers. Med. 2024, 14, 536. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.W.; Hu, H.; Park, S.Y.; Wan, J.; Yi, K.H. What Are the Factors That Enable Thread Lifting to Last Longer? Cosmetics 2024, 11, 42. [Google Scholar] [CrossRef]
- Rinker, B.; Veneracion, M.; Walsh, C. The Effect of Breastfeeding on Breast Aesthetics. Aesthetic Surg. J. 2008, 28, 534–537. [Google Scholar] [CrossRef]
- Coleman-Belin, J.C.; Barnett, J.; Khavanin, N.; Nelson, J.A.; Stern, C.S.; Allen, R.J. Imaging in Autologous Breast Reconstruction. Cancers 2024, 16, 2851. [Google Scholar] [CrossRef] [PubMed]
- Barkat, L.; Freiman, M.; Azhari, H. Image Translation of Breast Ultrasound to Pseudo Anatomical Display by CycleGAN. Bioengineering 2023, 10, 388. [Google Scholar] [CrossRef]
- Ciocan, R.A.; Graur, F.; Ciocan, A.; Cismaru, C.A.; Pintilie, S.R.; Berindan-Neagoe, I.; Hajjar, N.A.; Gherman, C.D. Robot-Guided Ultrasonography in Surgical Interventions. Diagnostics 2023, 13, 2456. [Google Scholar] [CrossRef]
- Akter, A.; Nahar, M.; Boby, N.; Islam, M.d.A.; Afroz, S.; Husna, A. Effectiveness of Ultrasonography Guided Pectoral Nerve Block for Post-Operative Analgesia in Modified Radical Mastectomy. Sch. J. Appl. Med. Sci. 2023, 11, 1538–1543. [Google Scholar] [CrossRef]
- Fukaya, M. Long-term effect of the insoluble thread-lifting technique. Clin. Cosmet. Investig. Dermatol. 2017, 10, 483–491. [Google Scholar] [CrossRef]
- Park, S.Y.; Kim, S.; Suwanchinda, A.; Yi, K. Non-surgical rhinoplasty through minimal invasive nose thread procedures: Adverse effects and prevention methods. Ski. Res. Technol. 2024, 30, e13590. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.H.; Lee, W.; Kim, S.H. Evaluation of a Novel Method for Temporary Eyebrow Lifting Using Polydioxanone Threads: Preliminary Findings. J. Clin. Med. 2025, 14, 490. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.; Oh, S. Lateral facial thread lifting procedure with temporal anchoring in deep temporal fascia: Anatomical perspectives of superficial temporal artery. Ski. Res. Technol. 2024, 30, e13587. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.W.; Kim, S.B.; Park, S.Y.; Wan, J.; Yi, K.H. Thread Lifting Materials: A Review of Its Difference in Terms of Technical and Mechanical Perspective. Clin. Cosmet. Investig. Dermatol. 2024, 17, 999–1006. [Google Scholar] [CrossRef]
- Zhang, M.; Chang, Z.; Wang, X.; Li, Q. Synthesis of Poly(l-lactide-co-ε-caprolactone) Copolymer: Structure, Toughness, and Elasticity. Polymers 2021, 13, 1270. [Google Scholar] [CrossRef] [PubMed]
- Hou, Z.; Kobayashi, H.; Tanaka, K.; Takarada, W.; Kikutani, T.; Takasaki, M. Laser-Assisted Melt Electrospinning of Poly(L-lactide-co-ε-caprolactone): Analyses on Processing Behavior and Characteristics of Prepared Fibers. Polymers 2022, 14, 2511. [Google Scholar] [CrossRef]
- Burko, P.; Sulamanidze, G.; Nikishin, D. Long-Term Efficacy of Poly(L-lactide-co-ε-caprolactone) Copolymer Lifting Threads with Encapsulated MICROscale Hyaluronic Acid Particles Using NAMICA Technology: Investigating Biorevitalizing Effects in Skin Remodeling (Part 1). Cosmetics 2025, 12, 20. [Google Scholar] [CrossRef]
- Wong, V. The Science of Absorbable Poly(L-Lactide-Co-ϵ-Caprolactone) Threads for Soft Tissue Repositioning of the Face: An Evidence-Based Evaluation of Their Physical Properties and Clinical Application. Clin. Cosmet. Investig. Dermatol. 2021, 14, 45–54. [Google Scholar] [CrossRef]
- Varnava, C.; Bogusch, M.; Wellenbrock, S.; Hirsch, T.; Wiebringhaus, P.; Kueckelhaus, M. Mastopexy Strategies for Ptotic Breasts in Patients Choosing Autologous Reconstruction Following Prophylactic Mastectomy. J. Clin. Med. 2023, 12, 3082. [Google Scholar] [CrossRef]
- Fansa, H.; Linder, S. Autologous Breast Reconstruction with Free Nipple–Areola Graft after Circumareolar (Skin Reducing) Mastectomy. J. Pers. Med. 2022, 12, 1588. [Google Scholar] [CrossRef]
- Bertozzi, N.; Pesce, M.; Santi, P.L.; Raposio, E. Oncoplastic breast surgery: Comprehensive review. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2572–2585. [Google Scholar] [PubMed]
- Atzori, G.; Franchelli, S.; Gipponi, M.; Cornacchia, C.; Diaz, R.; Depaoli, F.; Murelli, F.; Sparavigna, M.; Fregatti, P.; Friedman, D. Inferior Pedicle Reduction Mammoplasty as Corrective Surgery after Breast Conserving Surgery and Radiation Therapy. J. Pers. Med. 2022, 12, 1569. [Google Scholar] [CrossRef] [PubMed]
- Dastagir, K.; Obed, D.; Bucher, F.; Hofmann, T.; Koyro, K.I.; Vogt, P.M. Non-Invasive and Surgical Modalities for Scar Management: A Clinical Algorithm. J. Pers. Med. 2021, 11, 1259. [Google Scholar] [CrossRef]
- Jiang, D.; Rinkevich, Y. Furnishing Wound Repair by the Subcutaneous Fascia. Int. J. Mol. Sci. 2021, 22, 9006. [Google Scholar] [CrossRef]
- Guo, Y.; Song, Y.; Xiong, S.; Wang, T.; Liu, W.; Yu, Z.; Ma, X. Mechanical Stretch Induced Skin Regeneration: Molecular and Cellular Mechanism in Skin Soft Tissue Expansion. Int. J. Mol. Sci. 2022, 23, 9622. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Zhang, J.; Beeraka, N.M.; Sinelnikov, M.Y.; Zhang, X.; Cao, Y.; Lu, P. Robot-Assisted Minimally Invasive Breast Surgery: Recent Evidence with Comparative Clinical Outcomes. J. Clin. Med. 2022, 11, 1827. [Google Scholar] [CrossRef] [PubMed]
- Amro, C.; Sorenson, T.J.; Boyd, C.J.; Hemal, K.; Vernice, N.A.; Park, J.J.; Cohen, O.D.; Choi, M.; Karp, N.S. The Evolution of Implant-Based Breast Reconstruction: Innovations, Trends, and Future Directions. J. Clin. Med. 2024, 13, 7407. [Google Scholar] [CrossRef] [PubMed]
- Dai, H.; Cao, X.; Wu, H.; Liang, F.; Xie, Y.; Chung, K.; Zhang, Q.; Li, T.; Qiu, M.; Yang, H.; et al. Reverse-sequence endoscopic nipple-sparing mastectomy with direct-to-implant breast reconstruction and air inflation adjustment technique in breast cancer patients with large or severe ptotic breast: A single-center prospective cohort study. Lancet Reg. Health West. Pac. 2025, 55, 101432. [Google Scholar] [CrossRef]
- Xie, Y.; Hu, X.; Du, Z.; Liang, F.; Lv, Q.; Li, B. Minimally Invasive and Innovative Management of Prosthesis Infections in Endoscopic-Assisted Breast Reconstruction. Aesth Plast. Surg. 2024, 48, 266–272. [Google Scholar] [CrossRef]
- Ok, S.; Yoon, S.M.; Choi, S. Intuitive and Minimally Invasive Surgical Technique for Comminuted Mid-Shaft Clavicle Fractures: Fixation with an Anterior Mini Plate and Superior Locking Compression Plate. J. Clin. Med. 2025, 14, 999. [Google Scholar] [CrossRef]
- Scaglioni, M.F.; Martini, F.; Meroni, M. Present and Future of Autologous Breast Reconstruction: Advancing Techniques to Minimize Morbidity and Complications, Enhancing Quality of Life and Patient Satisfaction. J. Clin. Med. 2025, 14, 2599. [Google Scholar] [CrossRef]
- Sulamanidze, G.; Albina, K.; Sulamanidze, K.; Sulamanidze, M.; Samizadeh, S. Thread Lifting: Treatment Procedure. In Thread Lifting Techniques for Facial Rejuvenation and Recontouring; Samizadeh, S., Ed.; Springer International Publishing: Cham, Switzerland, 2024; pp. 269–279. [Google Scholar]
- Halepas, S.; Chen, X.J.; Ferneini, E.M. Thread-Lift Sutures: Anatomy, Technique, and Review of Current Literature. J. Oral Maxillofac. Surg. 2020, 78, 813–820. [Google Scholar] [CrossRef]
- Hyakusoku, H.; Ogawa, R.; Ono, S.; Ishii, N.; Hirakawa, K. Complications after Autologous Fat Injection to the Breast. Plast. Reconstr. Surg. 2009, 123, 360–370. [Google Scholar] [CrossRef]
- Zheng, D.-N.; Li, Q.-F.; Lei, H.; Zheng, S.-W.; Xie, Y.-Z.; Xu, Q.-H.; Yun, X.; Pu, L.L.Q. Autologous fat grafting to the breast for cosmetic enhancement: Experience in 66 patients with long-term follow up. J. Plast. Reconstr. Aesthetic Surg. 2008, 61, 792–798. [Google Scholar] [CrossRef]
- Bartella, L.; Smith, C.S.; Dershaw, D.D.; Liberman, L. Imaging Breast Cancer. Radiol. Clin. N Am. 2007, 45, 45–67. [Google Scholar] [CrossRef] [PubMed]
- Brandner, D.M.; Cai, X.; Foiret, J.; Ferrara, K.W.; Zagar, B.G. Estimation of Tissue Attenuation from Ultrasonic B-Mode Images—Spectral-Log-Difference and Method-of-Moments Algorithms Compared. Sensors 2021, 21, 2548. [Google Scholar] [CrossRef]
- Bogdan, R.-G.; Helgiu, A.; Cimpean, A.-M.; Ichim, C.; Todor, S.B.; Iliescu-Glaja, M.; Bodea, I.C.; Crainiceanu, Z.P. Assessing Fat Grafting in Breast Surgery: A Narrative Review of Evaluation Techniques. J. Clin. Med. 2024, 13, 7209. [Google Scholar] [CrossRef] [PubMed]
- Catalano, O.; Fusco, R.; De Muzio, F.; Simonetti, I.; Palumbo, P.; Bruno, F.; Borgheresi, A.; Agostini, A.; Gabelloni, M.; Varelli, C.; et al. Recent Advances in Ultrasound Breast Imaging: From Industry to Clinical Practice. Diagnostics 2023, 13, 980. [Google Scholar] [CrossRef]
- Lee, M.Y.; Kim, Y.J.; Kim, Y.S.; Roh, T.S.; Yun, I.S. Demographic review of aesthetic surgery for patients with facial palsy. Arch. Craniofacial Surg. 2024, 25, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Byun, I.H.; Jung, J.E.; Shin, I.S.; Hoon Park, S. Periareolar augmentation mastopexy: Finding the aesthetic level of breast lifting. J. Cutan. Aesthetic Surg. 2023, 16, 286–291. [Google Scholar] [CrossRef]
- Alshoabi, S.A.; Alareqi, A.A.; Gameraddin, M.; Gareeballah, A.; Alsultan, K.D.; Alzain, A.F. Efficacy of ultrasonography and mammography in detecting features of breast cancer. J. Fam. Med. Prim. Care 2025, 14, 341–347. [Google Scholar] [CrossRef]
- Hong, G.; Park, S.Y.; Yi, K. Revolutionizing thread lifting: Evolution and techniques in facial rejuvenation. J. Cosmet. Dermatol. 2024, 23, 2537–2542. [Google Scholar] [CrossRef]
- Katsika, L.; Boureka, E.; Kalogiannidis, I.; Tsakiridis, I.; Tirodimos, I.; Lallas, K.; Tsimtsiou, Z.; Dagklis, T. Screening for Breast Cancer: A Comparative Review of Guidelines. Life 2024, 14, 777. [Google Scholar] [CrossRef]
- Provencher, L.; Hogue, J.C.; Desbiens, C.; Poirier, B.; Poirier, E.; Boudreau, D.; Joyal, M.; Diorio, C.; Duchesne, N.; Chiquette, J. Is Clinical Breast Examination Important for Breast Cancer Detection? Curr. Oncol. 2016, 23, 332–339. [Google Scholar] [CrossRef]
- Mahraoui, A.; Goslings, J.C.; Kluijfhout, W.P. The Added Value of Sterility in Minor Surgical Procedures in Preventing Infection: A Systematic Review. Healthcare 2024, 12, 2101. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, C.E.; Venuto, R.; Tripodi, P.; Bartucciotto, L.; Ventura Spagnolo, E.; Nirta, A.; Genovese, G.; La Spina, I.; Sortino, S.; Nicita, A.; et al. From Guidelines to Action: Tackling Risk Factors for Surgical Site Infections. Antibiotics 2025, 14, 40. [Google Scholar] [CrossRef]
- Silva, A.; Mourão, J.; Vale, N. A Review of the Lidocaine in the Perioperative Period. J. Pers. Med. 2023, 13, 1699. [Google Scholar] [CrossRef]
- Stamenkovic, D.M.; Bezmarevic, M.; Bojic, S.; Unic-Stojanovic, D.; Stojkovic, D.; Slavkovic, D.Z.; Bancevic, V.; Maric, N.; Karanikolas, M. Updates on Wound Infiltration Use for Postoperative Pain Management: A Narrative Review. J. Clin. Med. 2021, 10, 4659. [Google Scholar] [CrossRef] [PubMed]
- Bertossi, D.; Botti, G.; Gualdi, A.; Fundarò, P.; Nocini, R.; Pirayesh, A.; Van Der Lei, B. Effectiveness, Longevity, and Complications of Facelift by Barbed Suture Insertion. Aesthetic Surg. J. 2019, 39, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Hong, W.; Chen, I.C.; Su, C.Y.; Perng, C.K.; Ma, H.; Fang, H.W. Evaluating Pull-Out Strength of Barbed Suture In Vitro by Using Porcine Tissue and Polydimethylsiloxane (PDMS). Polymers 2022, 14, 2170. [Google Scholar] [CrossRef]
- Căiță, G.A.; Voiță-Mekeres, F.; Bodog, F.; Vieriu, C.M.; Varga, D.M.; Racoviță, M.; Szilagyi, G.; Manole, F. The Bee Cosmetic Surgery Scale—A Clinical Tool for Assessing the Psychopathological, Psychosocial, and Decision-Making Factors Involved in Accepting Cosmetic Procedures. Cosmetics 2024, 11, 176. [Google Scholar] [CrossRef]
- Skwirczyńska, E.; Piotrowiak, M.; Ostrowski, M.; Wróblewski, O.; Tejchman, K.; Kwiatkowski, S.; Cymbaluk-Płoska, A. Welfare and Self-Assessment in Patients after Aesthetic and Reconstructive Treatments. Int. J. Environ. Res. Public Health 2022, 19, 11238. [Google Scholar] [CrossRef]
- Carter, P.; Gee, M.; McIlhone, H.; Lally, H.; Lawson, R. Comparing manual and computational approaches to theme identification in online forums: A case study of a sex work special interest community. Methods Psychol. 2021, 5, 100065. [Google Scholar] [CrossRef]
- Cheng, M.; Janzekovic, J.; Finze, R.; Mohseni, M.; Saifzadeh, S.; Savi, F.M.; Ung, O.; Wagels, M.; Hutmacher, D.W. Conceptualizing Scaffold Guided Breast Tissue Regeneration in a Preclinical Large Animal Model. Bioengineering 2024, 11, 593. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Liu, Y.X.; Chen, P.Y.; Fang, H.W. Zigzag Barbed Polydioxanone Thread Implantation and Evaluation Using Polydimethylsiloxane Model to Simulate Thread Migration in Tissue. Polymers 2024, 16, 1785. [Google Scholar] [CrossRef]
- Jwa, S.-J.; Won, J.-M.; Kim, D.-H.; Kim, K.-B.; Lee, J.-B.; Heo, M.; Shim, K.-S.; Jo, H.-S.; Lee, W.-J.; Roh, T.-S.; et al. Breast Tissue Restoration after the Partial Mastectomy Using Polycaprolactone Scaffold. Polymers 2022, 14, 3817. [Google Scholar] [CrossRef] [PubMed]
- Cuomo, R. Submuscular and Pre-pectoral ADM Assisted Immediate Breast Reconstruction: A Literature Review. Medicina 2020, 56, 256. [Google Scholar] [CrossRef]
- Suh, D.H.; Jang, H.W.; Lee, S.J.; Lee, W.S.; Ryu, H.J. Outcomes of Polydioxanone Knotless Thread Lifting for Facial Rejuvenation. Dermatol. Surg. 2015, 41, 720–725. [Google Scholar] [CrossRef]
- Matarasso, A.; Paul, M.D. Barbed Sutures in Aesthetic Plastic Surgery: Evolution of Thought and Process. Aesthetic Surg. J. 2013, 33 (Suppl. S3), 17S–31S. [Google Scholar] [CrossRef] [PubMed]
- Baig, M.N.; Yousaf, I.; Galbraith, J.G.; Din, R. Absorbable Polydioxanone (PDS) suture provides fewer wound complications than polyester (ethibond) suture in acute Tendo-Achilles rupture repair. Ir. Med. J. 2017, 110, 566. [Google Scholar] [PubMed]
- Dayan, S. Aesthetic evolution drives birth of minimally invasive surgery subgroup. J. Cosmet. Dermatol. 2019, 18, 1182–1185. [Google Scholar] [CrossRef]
- Aladari, N.; Palaghia, M.M.; Trofin, A.-M.; Cojocaru, E.; Ungureanu, C.; Ianole, V.; Morosan, E.; Budacu, C.C.; Motruc, T.C.; Pertea, M.; et al. Reducing Capsular Contracture Formation in Breast Augmentation with Silicone Implants: Experimental Study on Rats. Appl. Sci. 2022, 12, 4056. [Google Scholar] [CrossRef]
- Dini, G.M.; Milani, J.; Albuquerque, L.G.; Oliveira, M.F.D.; Santos Filho, I.D.D.A.O.; Iurk, L.K.; Ferreira, L.M. Breast augmentation via the abdominoplasty incision approach: A prospective study of 100 cases. Rev. Bras. Cir. Plást 2013, 28, 105–113. [Google Scholar] [CrossRef]
- Trovato, F.; Ceccarelli, S.; Michelini, S.; Vespasiani, G.; Guida, S.; Galadari, H.I.; Nisticò, S.P.; Colonna, L.; Pellacani, G. Advancements in Regenerative Medicine for Aesthetic Dermatology: A Comprehensive Review and Future Trends. Cosmetics 2024, 11, 49. [Google Scholar] [CrossRef]
- Vindigni, V.; Marena, F.; Zanettin, C.; Bassetto, F. Breast Reconstruction: The Oncoplastic Approach. J. Clin. Med. 2024, 13, 4718. [Google Scholar] [CrossRef] [PubMed]
- Viscardi, J.A.; Oranges, C.M.; Schaefer, D.J.; Kalbermatten, D.F. Reduction Mammoplasty: A Ten-Year Retrospective Review of the Omega Resection Pattern Technique. J. Clin. Med. 2021, 10, 4418. [Google Scholar] [CrossRef]
- Sulamanidze, M.; Sulamanidze, G.; Sulamanidze, K. Mastopexy—How to Reach Consistent Results—New Methods. In Miniinvasive Face and Body Lifts—Closed Suture Lifts or Barbed Thread Lifts; Serdev, N., Ed.; InTech: Houston, TX, USA, 2013. [Google Scholar]
- Balch, C.R. The Central Mound Technique for Reduction Mammaplasty. Plast. Reconstr. Surg. 1981, 67, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Hester, T.R.; Bostwick, J.; Miller, L.; Cunningham, S.J. Breast Reduction Utilizing the Maximally Vascularized Central Breast Pedicle. Plast. Reconstr. Surg. 1985, 76, 890–898. [Google Scholar] [CrossRef] [PubMed]
- See, M.H. Central pedicle reduction mammoplasty: A reliable technique. Gland. Surg. 2014, 3, 51. [Google Scholar]
- Würinger, E.; Mader, N.; Posch, E.; Holle, J. Nerve and Vessel Supplying Ligamentous Suspension of the Mammary Gland. Plast. Reconstr. Surg. 1998, 101, 1486–1493. [Google Scholar] [CrossRef]
- Cho, B.C.; Yang, J.D.; Baik, B.S. Periareolar reduction mammoplasty using an inferior dermal pedicle or a central pedicle. J. Plast. Reconstr. Aesthetic Surg. 2008, 61, 275–281. [Google Scholar] [CrossRef]
- Datta, G.; Carlucci, S. Selective Breast Reduction: A Personal Approach with a Central-Superior Pedicle. Plast. Reconstr. Surg. 2009, 123, 433–442. [Google Scholar] [CrossRef]
- Bayramiçli, M. The Central Pillar Technique: A New Septum-Based Pedicle Design for Reduction Mammaplasty. Aesthetic Surg. J. 2012, 32, 578–590. [Google Scholar] [CrossRef]
- Cho, M.J.; Schroeder, M.; Flores Garcia, J.; Royfman, A.; Moreira, A. The Current State of the Art in Autologous Breast Reconstruction: A Review and Modern/Future Approaches. J. Clin. Med. 2025, 14, 1543. [Google Scholar] [CrossRef]
- Park, J.H.; Park, J.U.; Chang, H. Advances in Biomaterials for Breast Reconstruction. Appl. Sci. 2021, 11, 7493. [Google Scholar] [CrossRef]
- Nambi Gowri, K.; King, M.W. A Review of Barbed Sutures—Evolution, Applications and Clinical Significance. Bioengineering 2023, 10, 419. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Yu, J.; Yu, X.; Zhang, Y.; Men, Z. Study on Bionic Design and Tissue Manipulation of Breast Interventional Robot. Sensors 2024, 24, 6408. [Google Scholar] [CrossRef]
- Chang, E.I. Advances in Microsurgical Treatment Options to Optimize Autologous Free Flap Breast Reconstruction. J. Clin. Med. 2024, 13, 5672. [Google Scholar] [CrossRef]
- Trinh, T.-T.T.; Chien, P.N.; Le, L.T.T.; Ngan-Giang, N.; Nga, P.T.; Nam, S.-Y.; Heo, C.-Y. An Assessment of the Effectiveness and Safety of ULTRACOL100 as a Device for Restoring Skin in the Nasolabial Fold Region. Cosmetics 2023, 11, 4. [Google Scholar] [CrossRef]
- Kim, D.M.; Baek, S.-W.; Park, J.M.; Kim, D.-S.; Lee, S.; Lee, J.-K.; Park, C.G.; Han, D.K. Multifunctional PDO Thread Coated with Mg(OH)2/ZnO Nanoparticles and Asiaticoside for Improved Facial Lifting. Pharmaceutics 2023, 15, 2220. [Google Scholar] [CrossRef]
- Lee, S.; Moon, H.W.; Lee, S.J.; Cho, J.C. Development and Characterization of PEGylated Poly D,L-Lactic Acid Nanoparticles for Skin Rejuvenation. Nanomaterials 2025, 15, 470. [Google Scholar] [CrossRef]
- Shin, J.J.; Park, T.J.; Kim, B.Y.; Kim, C.M.; Suh, D.H.; Lee, S.J.; Moon, H.-R.; Ryu, H.J. Comparative effects of various absorbable threads in a rat model. J. Cosmet. Laser Ther. 2019, 21, 158–162. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Grade | Nipple Position Relative to Inframammary Fold | Glandular Contour Characteristics | Clinical Notes |
|---|---|---|---|
| Grade I | At the level of or ≤1 cm below the IMF | Nipple is still above the lower contour of the breast mound | Mild ptosis, often aesthetic concern only |
| Grade II | >1 cm below the IMF but still above the lower contour of the breast | Nipple lies midway between the IMF and the inferior breast contour | Moderate ptosis, frequently an indication for surgical correction |
| Grade III | At or below the lowest point of the breast mound | Nipple points downward, typically at the lowest point of the gland | Severe ptosis, requires full surgical mastopexy |
| Pseudoptosis | At or above the IMF | Glandular tissue descends below IMF while nipple remains in normal position | Often post-lactational or post-weight loss, not true ptosis |
| Bottoming Out | Nipple remains elevated | Breast parenchyma has migrated below IMF | Often seen post-surgery (augmentation/reduction), may need revision |
| Feature | Breast Thread Lift | Traditional Mastopexy |
|---|---|---|
| Level of Invasiveness | Minimally invasive (no skin excision) | Invasive (extensive skin and parenchymal excision) |
| Estimated Duration of Results | 12–24 months (depending on material and technique) | 10–15 years or longer |
| Recovery Time | 1–2 weeks | 4–6 weeks |
| Risks and Complications | Asymmetries, inflammatory reactions, thread displacement | Visible scarring, NAC necrosis, ptosis recurrence |
| Ideal Candidates | Mild to moderate ptosis (Grade I–II) | Moderate to severe ptosis (Grade II–III) |
| Anesthesia Requirement | Local anesthesia ± mild sedation | General anesthesia |
| Immediate Aesthetic Results | Subtle and natural improvement | Complete correction and structural reshaping |
| Estimated Cost | Moderate | High |
| Thread Type | Composition | Duration of Effect | Clinical Features | Tissue Support Strength | Repeated Use Considerations |
|---|---|---|---|---|---|
| PDO | Biodegradable polymer | 6–12 months | Quick collagen boost; best for early signs of skin laxity | Mild | Limited long-term data; repeated use may increase fibrosis risk |
| Poly-L-Lactic Acid (PLLA) | Biodegradable poly-L-lactic acid | 12–18 months | Sustained collagen stimulation; suitable for midface volumization | Moderate | Reuse may affect tissue quality; long-term effects unconfirmed |
| Polycaprolactone (PCL) | Biodegradable polycaprolactone | 18–24+ months | Deep structural reinforcement; extended lifting performance | Strong | Repeated use insufficiently studied; potential for delayed tissue changes |
| Silhouette Soft | Polylactic acid with molded cones | 18–24 months | Dual effect: repositioning and collagen stimulation via cones | Moderate to strong | Possible fibrotic response with multiple sessions; caution recommended |
| Barbed Sutures | Permanent synthetic fiber | Long-term/permanent | Best for significant tissue drooping; durable mechanical hold | Very strong | Not advised for repeat sessions due to chronic inflammation risk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogdan, R.G.; Helgiu, A.; Bloanca, V.A.; Ichim, C.; Todor, S.B.; Iliescu-Glaja, M.; Domnariu, H.-P.; Leonte, E.; Crainiceanu, Z.P.; Anderco, P. The Rise and Refinement of Breast Thread Lifting: A Contemporary Review. J. Clin. Med. 2025, 14, 3863. https://doi.org/10.3390/jcm14113863
Bogdan RG, Helgiu A, Bloanca VA, Ichim C, Todor SB, Iliescu-Glaja M, Domnariu H-P, Leonte E, Crainiceanu ZP, Anderco P. The Rise and Refinement of Breast Thread Lifting: A Contemporary Review. Journal of Clinical Medicine. 2025; 14(11):3863. https://doi.org/10.3390/jcm14113863
Chicago/Turabian StyleBogdan, Razvan George, Alina Helgiu, Vlad Adam Bloanca, Cristian Ichim, Samuel Bogdan Todor, Mihai Iliescu-Glaja, Horatiu-Paul Domnariu, Elisa Leonte, Zorin Petrisor Crainiceanu, and Paula Anderco. 2025. "The Rise and Refinement of Breast Thread Lifting: A Contemporary Review" Journal of Clinical Medicine 14, no. 11: 3863. https://doi.org/10.3390/jcm14113863
APA StyleBogdan, R. G., Helgiu, A., Bloanca, V. A., Ichim, C., Todor, S. B., Iliescu-Glaja, M., Domnariu, H.-P., Leonte, E., Crainiceanu, Z. P., & Anderco, P. (2025). The Rise and Refinement of Breast Thread Lifting: A Contemporary Review. Journal of Clinical Medicine, 14(11), 3863. https://doi.org/10.3390/jcm14113863