

Enhancing Intraoral Scanning Accuracy: From the Influencing Factors to a Procedural Guideline

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy and Selection Criteria
2.2. Registration
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
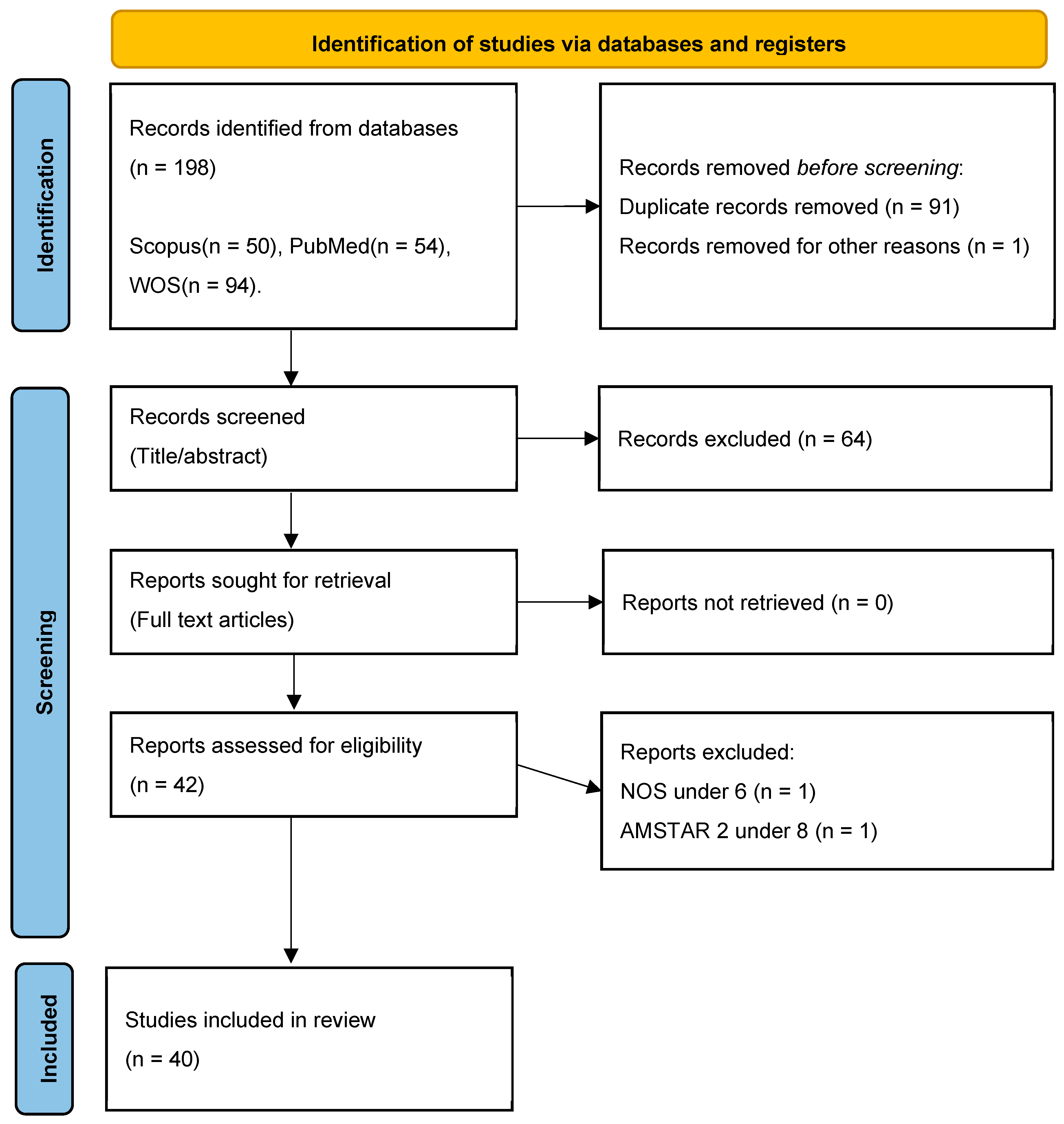
3.1. Databases Research Results and Validity of Data Extraction Assessment
3.2. Literature Findings
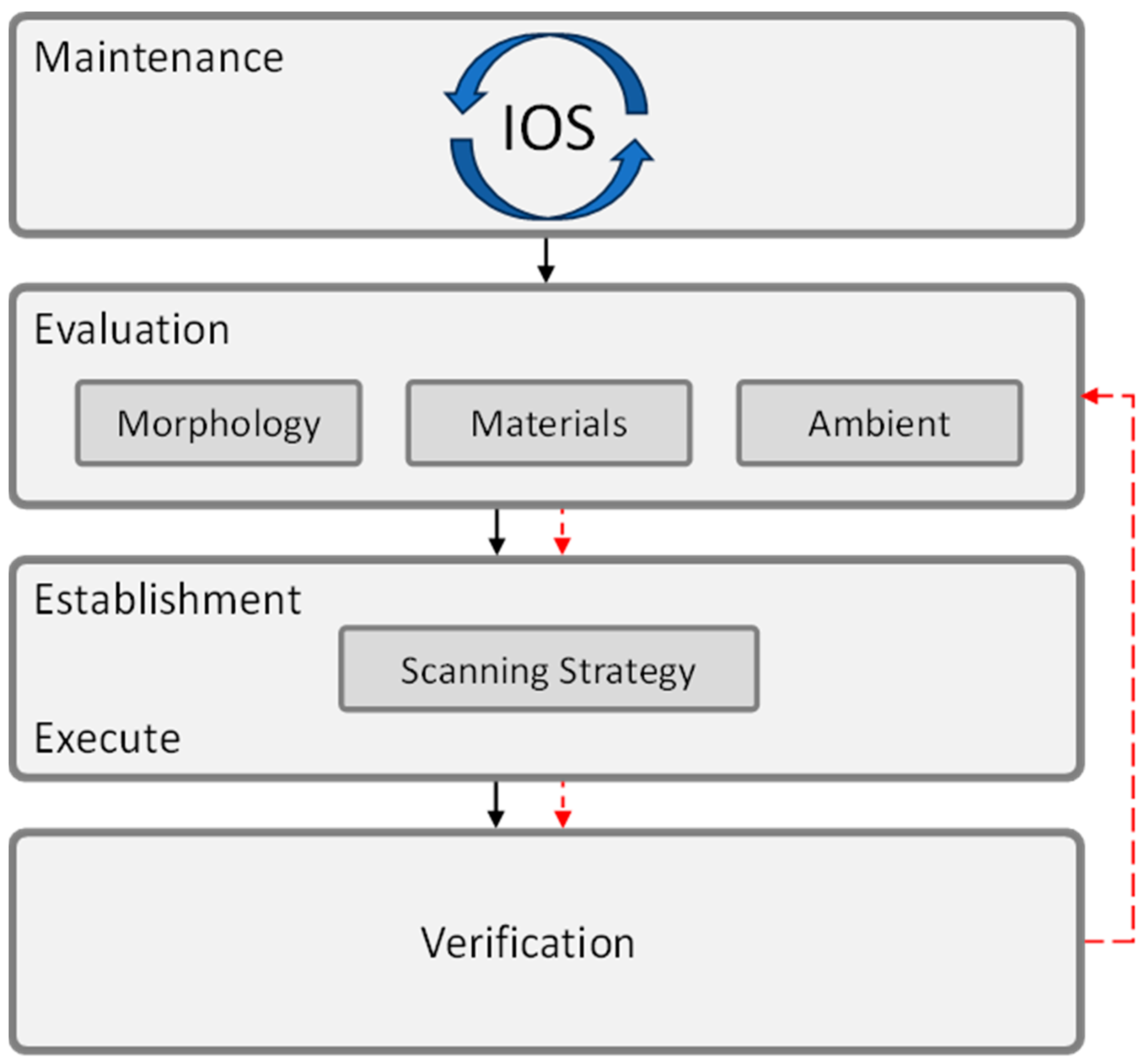
- IOS—characteristics and maintenance—this includes the inherent features of the IOS device, its pre-scanning preparation, and ongoing maintenance protocols.
- Intraoral morphology—this category includes the anatomical characteristics of the oral cavity and dentition.
- Intraoral materials—this refers to the presence of various materials within the oral cavity, such as restorative or implant scan body materials.
- Ambient conditions—this category encompasses the environmental conditions under which the scanning procedure is performed, including wetness, lighting, and temperature.
- Scanning strategy—this refers to the specific techniques and approaches employed by the operator during the scanning process.
4. Discussion
4.1. IOS—Characteristics and Maintenance
4.1.1. Software Versions and Updates
4.1.2. Scan Resolution
4.1.3. Size of the Scanner Head
4.1.4. Custom Abutment Library Data
4.1.5. Calibration
4.2. Intraoral Morphology
4.2.1. Crowding and Inclination of Teeth
4.2.2. Edentulous Condition
4.2.3. Palatal Morphologies
4.2.4. Inter-Tooth Distance
4.2.5. Inter-Implant Distance
4.2.6. Implant Position
4.2.7. Implant Depth
4.2.8. Implant Angulation
4.2.9. Implant Scan Body Fit
4.2.10. Implant Scan Body Bevel Location
4.2.11. Implant Scan Body Design
4.2.12. Implant Scan Body Retention System
4.2.13. Implant Scan Body Splinting Techniques
4.2.14. Proximal Axial Wall Height (Height of the Prepared Tooth)
4.2.15. Inlay Preparation Design
4.2.16. Location of the Scanned Area
4.2.17. Arch Width
4.2.18. Limited Mouth Opening
4.3. Intraoral Materials
4.3.1. Material
4.3.2. Material of the Bracket
4.3.3. Translucency of the Materials
4.3.4. Tooth Preparation Finishing Procedure
4.3.5. Tooth Color
4.4. Ambient Conditions
4.4.1. Lighting Conditions
4.4.2. Humidity
4.4.3. Ambient Temperature
4.5. Scanning Strategy
4.5.1. Scanning Strategy
4.5.2. Scanning Origin
4.5.3. Scanning Distance
4.5.4. Scanned Arch
4.5.5. Landmarks
4.5.6. Scanning Sequence
4.5.7. Scanning Pattern
4.5.8. Scanning Height
4.5.9. Scanning Speed
4.5.10. Scanning-Aid
4.5.11. Scanning Protocol
4.5.12. Experience of the Operator (Training and Age)
4.5.13. Patient Preparation
4.5.14. Limitations
4.5.15. Procedural Guideline Proposal
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martínez-Rodríguez, C.; Patricia, J.-P.; Ricardo, O.-A.; Alejandro, I.-L. Personalized dental medicine: Impact of intraoral and extraoral clinical variables on the precision and efficiency of intraoral scanning. J. Pers. Med. 2020, 10, 92. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Jiang, P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans—Part 1: Influence of ambient scanning light conditions on the accuracy (trueness and precision) of different intraoral scanners. J. Prosthet. Dent. 2020, 124, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Polo, M.; Álvarez, F.; Ortega, R.; Gómez-Polo, C.; Barmak, A.B.; Kois, J.C.; Revilla-León, M. Influence of the implant scan body bevel location, implant angulation and position on intraoral scanning accuracy: An in vitro study. J. Dent. 2022, 121, 104122. [Google Scholar] [CrossRef]
- Revilla-León, M.; Cascos-Sánchez, R.; Barmak, A.B.; Kois, J.C.; Gómez-Polo, M. The effect of different tooth preparation finishing procedures and immediate dentin sealing on the scanning accuracy of different intraoral scanners. J. Dent. 2023, 130, 104431. [Google Scholar] [CrossRef]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, R.; Galli, M.; Chen, Z.; Mendonça, G.; Meirelles, L.; Wang, H.-L.; Chan, H.-L. Intraoral scanning reduces procedure time and improves patient comfort in fixed prosthodontics and implant dentistry: A systematic review. Clin. Oral Investig. 2021, 25, 6517–6531. [Google Scholar] [CrossRef]
- Negucioiu, M.; Buduru, S.; Coman, D.; Condor, A.-M.; Berar, A.; Condor, D.; Buduru, R.; Kui, A. Digital Impressions Versus Traditional Impressions: An Overview on Accuracy, Time and Patient Preferences. Rom. J. Oral Rehabil. 2024, 16. [Google Scholar] [CrossRef]
- Novac, A.C.; Pop, D.M.; Tănase, A.; Zaharia, C.; Crăciunescu, E.L.; Romînu, M.; Negruțiu, M.L.; Duma, V.-F.; Sinescu, C. The Advantages of the Implementation of Digital Flow in the Working Time Management of Dental Prostheses Restorations. Rom. J. Oral Rehabil. 2023, 15. [Google Scholar]
- Jin, G.; Kim, J.-E.; Nam, N.-E.; Shin, S.-H.; Shim, J.-S. Accuracy improvement of intraoral scanning and buccal bite registration using healing abutment as landmarks: An in vitro study. Appl. Sci. 2021, 11, 318. [Google Scholar] [CrossRef]
- Thomas, A.A.; Jain, R.K. Influence of Operator Experience on Scanning Time and Accuracy with Two Different Intraoral Scanners—A Prospective Clinical Trial. Turk. J. Orthod. 2023, 36, 10–14. [Google Scholar] [CrossRef]
- Kihara, H.; Hatakeyama, W.; Komine, F.; Takafuji, K.; Takahashi, T.; Yokota, J.; Oriso, K.; Kondo, H. Accuracy and practicality of intraoral scanner in dentistry: A literature review. J. Prosthodont. Res. 2020, 64, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.-H.; Mangal, U.; Nam, N.-E.; Choi, S.-H.; Shim, J.-S.; Kim, J.-E. A comparison of accuracy of different dental restorative materials between intraoral scanning and conventional impression-taking: An in vitro study. Materials 2021, 14, 2060. [Google Scholar] [CrossRef]
- Resnick, C.M.; Doyle, M.; Calabrese, C.E.; Sanchez, K.; Padwa, B.L. Is It Cost Effective to Add an Intraoral Scanner to an Oral and Maxillofacial Surgery Practice? J. Oral Maxillofac. Surg. 2019, 77, 1687–1694. [Google Scholar] [CrossRef]
- Suese, K. Progress in digital dentistry: The practical use of intraoral scanners. Dent. Mater. J. 2020, 39, 52–56. [Google Scholar] [CrossRef]
- Shimizu, T.; Tasaka, A.; Wadachi, J.; Yamashita, S. A new proposal for improving the accuracy of intraoral scanning for partially edentulous residual ridge. J. Prosthodont. Res. 2023, 67, 246–254. [Google Scholar] [CrossRef]
- Eggmann, F.; Blatz, M.B. Recent Advances in Intraoral Scanners. J. Dent. Res. 2024, 103, 1349–1357. [Google Scholar] [CrossRef]
- Schimmel, M.; Akino, N.; Srinivasan, M.; Wittneben, J.-G.; Yilmaz, B.; Abou-Ayash, S. Accuracy of intraoral scanning in completely and partially edentulous maxillary and mandibular jaws: An in vitro analysis. Clin. Oral Investig. 2021, 25, 1839–1847. [Google Scholar] [CrossRef]
- Christopoulou, I.; Kaklamanos, E.G.; Makrygiannakis, M.A.; Bitsanis, I.; Perlea, P.; Tsolakis, A.I. Intraoral Scanners in Orthodontics: A Critical Review. Int. J. Environ. Res. Public Health 2022, 19, 1407. [Google Scholar] [CrossRef]
- Revilla-Leon, M.; Frazier, K.; Da Costa, J.B.; Kumar, P.; Duong, M.-L.; Khajotia, S.; Urquhart, O. Intraoral scanners. J. Am. Dent. Assoc. 2021, 152, 669–670.e2. [Google Scholar] [CrossRef]
- Forna, N.; Cretu, C.; Topoliceanu, C.; Agop-Forna, D. Digital Systems Predictible for Success in Dental Medicine. Publ. House Rom. Acad. 2023, 25, 77–85. [Google Scholar]
- Russo, L.L.; Caradonna, G.; Troiano, G.; Salamini, A.; Guida, L.; Ciavarella, D. Three-dimensional differences between intraoral scans and conventional impressions of edentulous jaws: A clinical study. J. Prosthet. Dent. 2020, 123, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Ferrari Cagidiaco, E.; Zarone, F.; Discepoli, N.; Joda, T.; Ferrari, M. Analysis of The Reproducibility of Subgingival Vertical Margins Using Intraoral Optical Scanning (IOS): A Randomized Controlled Pilot Trial. J. Clin. Med. 2021, 10, 941. [Google Scholar] [CrossRef]
- Rasaie, V.; Abduo, J.; Hashemi, S. Accuracy of Intraoral Scanners for Recording the Denture Bearing Areas: A Systematic Review. J. Prosthodont. 2021, 30, 520–539. [Google Scholar] [CrossRef]
- Ye, J.R.; Park, S.H.; Lee, H.; Hong, S.-J.; Chae, Y.K.; Lee, K.E.; Lee, H.-S.; Choi, S.C.; Nam, O.H. Influence of limited mouth opening in children on intraoral scanning accuracy: An in vitro study. Int. J. Paediatr. Dent. 2024, 34, 755–763. [Google Scholar] [CrossRef]
- Aswani, K.; Wankhade, S.; Khalikar, A.; Deogade, S. Accuracy of an intraoral digital impression: A review. J. Indian. Prosthodont. Soc. 2020, 20, 27–37. [Google Scholar] [CrossRef]
- Ashraf, Y.; Sabet, A.; Hamdy, A.; Ebeid, K. Influence of Preparation Type and Tooth Geometry on the Accuracy of Different Intraoral Scanners. J. Prosthodont. 2020, 29, 800–804. [Google Scholar] [CrossRef]
- Shin, S.-H.; Yu, H.-S.; Cha, J.-Y.; Kwon, J.-S.; Hwang, C.-J. Scanning accuracy of bracket features and slot base angle in different bracket materials by four intraoral scanners: An in vitro study. Materials 2021, 14, 365. [Google Scholar] [CrossRef]
- Park, Y.; Kim, J.-H.; Park, J.-K.; Son, S.-A. Scanning accuracy of an intraoral scanner according to different inlay preparation designs. BMC Oral Health 2023, 23, 515. [Google Scholar] [CrossRef]
- Pilecco, R.O.; Dapieve, K.S.; Baldi, A.; Valandro, L.F.; Scotti, N.; Pereira, G.K.R. Comparing the accuracy of distinct scanning systems and their impact on marginal/internal adaptation of tooth-supported indirect restorations. A scoping review. J. Mech. Behav. Biomed. Mater. 2023, 144, 105975. [Google Scholar] [CrossRef]
- Revilla-León, M.; Fry, E.; Zeitler, J.M.; Li, J.; Barmak, A.B.; Kois, J.C.; Pérez-Barquero, J.A. Influence of apical finish line location of tooth preparations on the scanning accuracy of intraoral scanners with various focal lengths and scanning technologies. J. Prosthet. Dent. 2024. [Google Scholar] [CrossRef]
- Ciocan, L.T.; Vasilescu, V.G.; Răuță, S.-A.; Pantea, M.; Pițuru, S.-M.; Imre, M. Comparative Analysis of Four Different Intraoral Scanners: An In Vitro Study. Diagnostics 2024, 14, 1453. [Google Scholar] [CrossRef] [PubMed]
- Alkadi, L. A Comprehensive Review of Factors That Influence the Accuracy of Intraoral Scanners. Diagnostics 2023, 13, 3291. [Google Scholar] [CrossRef] [PubMed]
- Hardan, L.; Bourgi, R.; Lukomska-Szymanska, M.; Hernández-Cabanillas, J.C.; Zamarripa-Calderón, J.E.; Jorquera, G.; Ghishan, S.; Cuevas-Suárez, C.E. Effect of scanning strategies on the accuracy of digital intraoral scanners: A meta-analysis of in vitro studies. J. Adv. Prosthodont. 2023, 15, 315–332. [Google Scholar] [CrossRef]
- Shah, N.; Thakur, M.; Gill, S.; Shetty, O.; Alqahtani, N.M.; Al-Qarni, M.A.; Alqahtani, S.M.; Elagib, M.F.A.; Chaturvedi, S. Validation of Digital Impressions’ Accuracy Obtained Using Intraoral and Extraoral Scanners: A Systematic Review. J. Clin. Med. 2023, 12, 5833. [Google Scholar] [CrossRef]
- Angelone, F.; Ponsiglione, A.M.; Ricciardi, C.; Cesarelli, G.; Sansone, M.; Amato, F. Diagnostic Applications of Intraoral Scanners: A Systematic Review. J. Imaging 2023, 9, 134. [Google Scholar] [CrossRef]
- Abduo, J. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar] [CrossRef]
- Diker, B.; Tak, Ö. Comparing the accuracy of six intraoral scanners on prepared teeth and effect of scanning sequence. J. Adv. Prosthodont. 2020, 12, 299–306. [Google Scholar] [CrossRef]
- Schmidt, A.; Klussmann, L.; Wöstmann, B.; Schlenz, M.A. Accuracy of Digital and Conventional Full-Arch Impressions in Patients: An Update. J. Clin. Med. 2020, 9, 688. [Google Scholar] [CrossRef]
- Al-Hassiny, A.; Végh, D.; Bányai, D.; Végh, Á.; Géczi, Z.; Borbély, J.; Hermann, P.; Hegedüs, T. User Experience of Intraoral Scanners in Dentistry: Transnational Questionnaire Study. Int. Dent. J. 2023, 73, 754–759. [Google Scholar] [CrossRef]
- ISO 5725-1:2023 (en); Accuracy (Trueness and Precision) of Measurement Methods and Results—Part 1: General Principles and Definitions. International Organization for Standardization: Geneva, Switzerland, 2024.
- Anh, J.-W.; Park, J.-M.; Chun, Y.-S.; Kim, M.; Kim, M. A comparison of the precision of three-dimensional images acquired by 2 digital intraoral scanners: Effects of tooth irregularity and scanning direction. Korean J. Orthod. 2016, 46, 3–12. [Google Scholar] [CrossRef]
- Zimmermann, M.; Ender, A.; Mehl, A. Local accuracy of actual intraoral scanning systems for single-tooth preparations in vitro. J. Am. Dent. Assoc. 2020, 151, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.-C.; Fages, M.; Ducret, M. Intraoral Scanner Technologies: A Review to Make a Successful Impression. J. Healthc. Eng. 2017, 2017, 8427595. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Vazouras, K.; Chen, Y.; Kotina, E.; Natto, Z.; Kang, K.; Chochlidakis, K. Digital vs Conventional Implant Impressions: A Systematic Review and Meta-Analysis. J. Prosthodont. 2020, 29, 660–678. [Google Scholar] [CrossRef]
- Gallardo, Y.R.; Bohner, L.; Tortamano, P.; Pigozzo, M.N.; Laganá, D.C.; Sesma, N. Patient outcomes and procedure working time for digital versus conventional impressions: A systematic review. J. Prosthet. Dent. 2018, 119, 214–219. [Google Scholar] [CrossRef]
- Giachetti, L.; Sarti, C.; Cinelli, F.; Russo, D. Accuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical Studies. Int. J. Prosthodont. 2020, 33, 192–201. [Google Scholar] [CrossRef]
- Gómez-Polo, M.; Donmez, M.B.; Çakmak, G.; Yilmaz, B.; Revilla-León, M. Influence of implant scan body design (height, diameter, geometry, material, and retention system) on intraoral scanning accuracy: A systematic review. J. Prosthodont. 2023, 32, 165–180. [Google Scholar] [CrossRef]
- Revilla-León, M.; Lanis, A.; Yilmaz, B.; Kois, J.C.; Gallucci, G.O. Intraoral digital implant scans: Parameters to improve accuracy. J. Prosthodont. 2023, 32, 150–164. [Google Scholar] [CrossRef]
- Kahale, L.A.; Elkhoury, R.; El Mikati, I.; Pardo-Hernandez, H.; Khamis, A.M.; Schünemann, H.J.; Haddaway, N.R.; Akl, E.A. Tailored PRISMA 2020 flow diagrams for living systematic reviews: A methodological survey and a proposal. F1000Res 2021, 10, 192. [Google Scholar] [CrossRef]
- Carcassi, F.; Sbardolini, G. Assertion, denial, and the evolution of Boolean operators. Mind Lang. 2023, 38, 1187–1207. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Ottawa Hospital Research Institute. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 March 2024).
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Braian, M.; Wennerberg, A. Trueness and precision of 5 intraoral scanners for scanning edentulous and dentate complete-arch mandibular casts: A comparative in vitro study. J. Prosthet. Dent. 2019, 122, 129–136.e2. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Subramanian, S.G.; Özcan, M.; Krishnamurthy, V.R. Clinical Study of the Influence of Ambient Light Scanning Conditions on the Accuracy (Trueness and Precision) of an Intraoral Scanner. J. Prosthodont. 2020, 29, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Motel, C.; Kirchner, E.; Adler, W.; Wichmann, M.; Matta, R.E. Impact of Different Scan Bodies and Scan Strategies on the Accuracy of Digital Implant Impressions Assessed with an Intraoral Scanner: An In Vitro Study. J. Prosthodont. 2020, 29, 309–314. [Google Scholar] [CrossRef]
- Moon, Y.-G.; Lee, K.-M. Comparison of the accuracy of intraoral scans between complete-arch scan and quadrant scan. Prog. Orthod. 2020, 21, 36. [Google Scholar] [CrossRef]
- Jivanescu, A.; Faur, A.-B.; Rotar, R.N. Can Dental Office Lighting Intensity Conditions Influence the Accuracy of Intraoral Scanning? Scanning 2021, 2021, 9980590. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Kim, J.-E.; Nam, N.-E.; Shin, S.-H.; Lim, J.-H.; Lee, K.-W.; Shim, J.-S. Influence of edentulous conditions on intraoral scanning accuracy of virtual interocclusal record in quadrant scan. Appl. Sci. 2021, 11, 1489. [Google Scholar] [CrossRef]
- Oh, H.-S.; Lim, Y.-J.; Kim, B.; Kim, M.-J.; Kwon, H.-B.; Baek, Y.-W. Influence of scanning-aid materials on the accuracy and time efficiency of intraoral scanners for full-arch digital scanning: An in vitro study. Materials 2021, 14, 2340. [Google Scholar] [CrossRef]
- Gavounelis, N.A.; Gogola, C.-M.C.; Halazonetis, D.J. The Effect of Scanning Strategy on Intraoral Scanner’s Accuracy. Dent. J. 2022, 10, 123. [Google Scholar] [CrossRef]
- Kim, E.-Y.; Wada, J.; Sakamoto, K.; Ishioka, Y.; Arai, Y.; Murakami, N.; Yamazaki, T.; Hayama, H.; Utsumi, M.; Inukai, S.; et al. Effect of Scanning Origin Location on Data Accuracy of Abutment Teeth Region in Digital Impression Acquired Using Intraoral Scanner for Removable Partial Denture: A Preliminary In Vitro Study. J. Clin. Med. 2022, 11, 7392. [Google Scholar] [CrossRef]
- Rotar, R.N.; Faur, A.B.; Pop, D.; Jivanescu, A. Scanning Distance Influence on the Intraoral Scanning Accuracy—An In Vitro Study. Materials 2022, 15, 3061. [Google Scholar] [CrossRef]
- Mai, H.Y.; Mai, H.-N.; Lee, C.-H.; Lee, K.-B.; Kim, S.-Y.; Lee, J.-M.; Lee, K.-W.; Lee, D.-H. Impact of scanning strategy on the accuracy of complete-arch intraoral scans: A preliminary study on segmental scans and merge methods. J. Adv. Prosthodont. 2022, 14, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Agustín-Panadero, R.; Moreno, D.M.; Pérez-Barquero, J.A.; Fernández-Estevan, L.; Gómez-Polo, M.; Revilla-León, M. Influence of type of restorative materials and surface wetness conditions on intraoral scanning accuracy. J. Dent. 2023, 134, 104521. [Google Scholar] [CrossRef]
- Chang, I.-C.; Hung, C.-C.; Du, J.-K.; Liu, C.-T.; Lai, P.-L.; Lan, T.-H. Accuracy of intraoral scanning methods for maxillary Kennedy class I arch. J. Dent. Sci. 2023, 18, 747–753. [Google Scholar] [CrossRef]
- Cho, J.-H.; Han, J.-S.; Yoon, H.-I. Effect of translucency of CAD-CAM ceramic restorative materials and scanning aid conditions on the accuracy of intraoral scans. J. Dent. Sci. 2023, 18, 1212–1218. [Google Scholar] [CrossRef]
- Elter, B.; Tak, Ö. Effect of substrate adjacent to the scan region on the trueness of four intraoral scanners: An in vitro study. J. Dent. 2023, 138, 104729. [Google Scholar] [CrossRef]
- Zarauz, C.; Pradíes, G.J.; Chebib, N.; Dönmez, M.B.; Karasan, D.; Sailer, I. Influence of age, training, intraoral scanner, and software version on the scan accuracy of inexperienced operators. J. Prosthodont. 2023, 32, 135–141. [Google Scholar] [CrossRef]
- Sorrentino, R.; Ruggiero, G.; Leone, R.; Di Mauro, M.I.; Cagidiaco, E.F.; Joda, T.; Lo Russo, L.; Zarone, F. Influence of different palatal morphologies on the accuracy of intraoral scanning of the edentulous maxilla: A three-dimensional analysis. J. Prosthodont. Res. 2024, 68, 634–642. [Google Scholar] [CrossRef]
- Karakuzu, M.; Öztürk, C.; Karakuzu, Z.B.; Zortuk, M. The effects of different lighting conditions on the accuracy of intraoral scanning. J. Adv. Prosthodont. 2024, 16, 311. [Google Scholar] [CrossRef]
- Jamjoom, F.Z.; Aldghim, A.; Aldibasi, O.; Yilmaz, B. Impact of intraoral scanner, scanning strategy, and scanned arch on the scan accuracy of edentulous arches: An in vitro study. J. Prosthet. Dent. 2024, 131, 1218–1225. [Google Scholar] [CrossRef]
- Zhou, Y.; Fu, L.; Zhang, Z.; Tang, X. Effect of tooth color on the accuracy of intraoral complete arch scanning under different light conditions using a zirconia restoration model. J. Prosthet. Dent. 2024, 131, 145.e1–145.e8. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Son, K.; Bihn, S.K.; Lee, K.-B. Effect of the Inter-Tooth Distance and Proximal Axial Wall Height of Prepared Teeth on the Scanning Accuracy of Intraoral Scanners. J. Funct. Biomater. 2024, 15, 115. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-T.; Chen, J.-H.; Du, J.-K.; Hung, C.-C.; Lan, T.-H. Accuracy comparison of scan segmental sequential ranges with two intraoral scanners for maxilla and mandible. J. Dent. Sci. 2024, 19, 466–472. [Google Scholar] [CrossRef]
- Choi, E.-J.; Ko, K.-H.; Huh, Y.-H.; Park, C.-J.; Cho, L.-R. Effect of scan path on accuracy of complete arch intraoral scan. J. Adv. Prosthodont. 2024, 16, 319. [Google Scholar] [CrossRef]
- Gehrke, P.; Rashidpour, M.; Sader, R.; Weigl, P. A systematic review of factors impacting intraoral scanning accuracy in implant dentistry with emphasis on scan bodies. Int. J. Implant. Dent. 2024, 10, 20. [Google Scholar] [CrossRef]
- Jamjoom, F.Z.; Aldghim, A.; Aldibasi, O.; Yilmaz, B. In vitro evaluation of the impact of intraoral scanner, scanning aids, and the scanned arch on the scan accuracy of edentulous arches. J. Prosthodont. 2024. Early View. [Google Scholar] [CrossRef]
- Revilla-León, M.; Smith, Z.; Methani, M.M.; Zandinejad, A.; Özcan, M. Influence of scan body design on accuracy of the implant position as transferred to a virtual definitive implant cast. J. Prosthet. Dent. 2021, 125, 918–923. [Google Scholar] [CrossRef]
- Schmalzl, J.; Róth, I.; Borbély, J.; Hermann, P.; Vecsei, B. The impact of software updates on accuracy of intraoral scanners. BMC Oral Health 2023, 23, 219. [Google Scholar] [CrossRef]
- Vág, J.; Renne, W.; Revell, G.; Ludlow, M.; Mennito, A.; Teich, S.T.; Gutmacher, Z. The effect of software updates on the trueness and precision of intraoral scanners. Quintessence Int. 2021, 52, 636–644. [Google Scholar] [CrossRef]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Effect of Software Version on the Accuracy of an Intraoral Scanning Device. Int. J. Prosthodont. 2018, 31, 375–376. [Google Scholar] [CrossRef]
- Shim, J.S.; Lee, J.S.; Lee, J.Y.; Choi, Y.J.; Shin, S.W.; Ryu, J.J. Effect of software version and parameter settings on the marginal and internal adaptation of crowns fabricated with the CAD/CAM system. J. Appl. Oral. Sci. 2015, 23, 515–522. [Google Scholar] [CrossRef]
- Fages, M.; Carayon, D.; Desoutter, A.; Benmoumen, I.; Bouchiha, K.; Subsol, G.; Cuisinier, F. Unified protocol to evaluate intraoral scanner resolution, trueness and precision: The RTP-protocol. Metrol. Meas. Syst. 2024, 31, 73–83. [Google Scholar]
- Chiu, A.; Chen, Y.-W.; Hayashi, J.; Sadr, A. Accuracy of CAD/CAM Digital Impressions with Different Intraoral Scanner Parameters. Sensors 2020, 20, 1157. [Google Scholar] [CrossRef] [PubMed]
- Medina-Sotomayor, P.; Pascual-Moscardó, A.; Camps, I. Relationship between resolution and accuracy of four intraoral scanners in complete-arch impressions. J. Clin. Exp. Dent. 2018, 10, e361–e366. [Google Scholar] [CrossRef]
- An, H.; Langas, E.E.; Gill, A.S. Effect of scanning speed, scanning pattern, and tip size on the accuracy of intraoral digital scans. J. Prosthet. Dent. 2024, 131, 1160–1167. [Google Scholar] [CrossRef]
- Hayama, H.; Fueki, K.; Wadachi, J.; Wakabayashi, N. Trueness and precision of digital impressions obtained using an intraoral scanner with different head size in the partially edentulous mandible. J. Prosthodont. Res. 2018, 62, 347–352. [Google Scholar] [CrossRef]
- Baek, Y.-W.; Lim, Y.-J.; Kim, M.-J.; Kwon, H.-B. Effect of custom abutment data superimposition on the accuracy of implant abutment level scanning: An in vitro study. J. Prosthet. Dent. 2024, 131, 1208–1217. [Google Scholar] [CrossRef]
- Kim, J.-E.; Park, J.-H.; Moon, H.-S.; Shim, J.-S. Simplified digital workflow for dental implant restoration on a stock abutment using an intraoral scanner: A dental technique. J. Prosthet. Dent. 2017, 118, 268–272. [Google Scholar] [CrossRef]
- Cho, W.-T.; Bae, E.-B.; Ahn, J.-J.; Huh, J.-B. Cordless digital workflow for scanning implant-supported prostheses at the abutment level: A dental technique. J. Prosthet. Dent. 2020, 124, 428–430. [Google Scholar] [CrossRef]
- Lin, W.-S.; Harris, B.T.; Morton, D. The use of a scannable impression coping and digital impression technique to fabricate a customized anatomic abutment and zirconia restoration in the esthetic zone. J. Prosthet. Dent. 2013, 109, 187–191. [Google Scholar] [CrossRef]
- Revilla-León, M.; Gohil, A.; Barmak, A.B.; Gómez-Polo, M.; Pérez-Barquero, J.A.; Att, W.; Kois, J.C. Influence of ambient temperature changes on intraoral scanning accuracy. J. Prosthet. Dent. 2023, 130, 755–760. [Google Scholar] [CrossRef]
- Ruggiero, G.; Leone, R.; Sorrentino, R.; Zarone, F. In silico analysis and accuracy of different palatal morphologies using intraoral scanner system. J. Dent. 2024, 147, 105173. [Google Scholar] [CrossRef]
- Gan, N.; Xiong, Y.; Jiao, T. Accuracy of Intraoral Digital Impressions for Whole Upper Jaws, Including Full Dentitions and Palatal Soft Tissues. PLoS ONE 2016, 11, e0158800. [Google Scholar] [CrossRef] [PubMed]
- Zarone, F.; Ruggiero, G.; Ferrari, M.; Mangano, F.; Joda, T.; Sorrentino, R. Comparison of different intraoral scanning techniques on the completely edentulous maxilla: An in vitro 3-dimensional comparative analysis. J. Prosthet. Dent. 2020, 124, 762.e1–762.e8. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.-Y.; Son, K.; Lee, K.-B. Effect of distance between the abutment and the adjacent teeth on intraoral scanning: An in vitro study. J. Prosthet. Dent. 2021, 125, 911–917. [Google Scholar] [CrossRef]
- Gómez-Polo, M.; Ortega, R.; Sallorenzo, A.; Agustín-Panadero, R.; Barmak, A.B.; Kois, J.C.; Revilla-León, M. Influence of the surface humidity, implant angulation, and interimplant distance on the accuracy and scanning time of complete-arch implant scans. J. Dent. 2022, 127, 104307. [Google Scholar] [CrossRef]
- Abduo, J.; Laskey, D. Effect of preparation type on the accuracy of different intraoral scanners: An in vitro study at different levels of accuracy evaluation. J. Esthet. Restor. Dent. 2022, 34, 1221–1229. [Google Scholar] [CrossRef]
- Garcia-Gomez, S.; Maneiro-Lojo, J.; Alonso Pérez-Barquero, J.; Kois, J.C.; Fernandez-Estevan, L.; Revilla-León, M. Influence of interdental space and operator experience on the accuracy, scanning time, and number of photograms of veneer preparations digitized by using an intraoral scanner. J. Prosthet. Dent. 2025, S0022391325001076. [Google Scholar] [CrossRef]
- Tan, M.; Yee, S.; Wong, K.; Tan, Y.; Tan, K. Comparison of Three-Dimensional Accuracy of Digital and Conventional Implant Impressions: Effect of Interimplant Distance in an Edentulous Arch. Int. J. Oral Maxillofac. Implant. 2019, 34, 366–380. [Google Scholar] [CrossRef]
- Desoutter, A.; Subsol, G.; Fargier, E.; Sorgius, A.; Tassery, H.; Fages, M.; Cuisinier, F. New method to analyze resolution acquisition for intraoral scanners. Metrol. Meas. Syst. 2021, 29, 391–404. [Google Scholar] [CrossRef]
- Azevedo, L.; Marques, T.; Karasan, D.; Fehmer, V.; Sailer, I.; Correia, A.; Gómez Polo, M. Influence of Implant ScanBody Material and Intraoral Scanners on the Accuracy of Complete-Arch Digital Implant Impressions. Int. J. Prosthodont. 2024, 37, 575–582. [Google Scholar] [CrossRef]
- Thanasrisuebwong, P.; Kulchotirat, T.; Anunmana, C. Effects of inter-implant distance on the accuracy of intraoral scanner: An in vitro study. J. Adv. Prosthodont. 2021, 13, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Laohverapanich, K.; Luangchana, P.; Anunmana, C.; Pornprasertsuk-Damrongsri, S. Different Implant Subgingival Depth Affects the Trueness and Precision of the 3D Dental Implant Position: A Comparative in Vitro Study Among Five Digital Scanners and a Conventional Technique. Int. J. Oral. Maxillofac. Implant. 2021, 36, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Sequeira, V.; Harper, M.T.; Lilly, C.L.; Bryington, M.S. Accuracy of Digital Impressions at Varying Implant Depths: An In Vitro Study. J. Prosthodont. 2023, 32, 54–61. [Google Scholar] [CrossRef]
- Arcuri, L.; Pozzi, A.; Lio, F.; Rompen, E.; Zechner, W.; Nardi, A. Influence of implant scanbody material, position and operator on the accuracy of digital impression for complete-arch: A randomized in vitro trial. J. Prosthodont. Res. 2020, 64, 128–136. [Google Scholar] [CrossRef]
- Stimmelmayr, M.; Güth, J.-F.; Erdelt, K.; Edelhoff, D.; Beuer, F. Digital evaluation of the reproducibility of implant scanbody fit—An in vitro study. Clin. Oral Investig. 2012, 16, 851–856. [Google Scholar] [CrossRef]
- Huang, R.; Liu, Y.; Huang, B.; Zhou, F.; Chen, Z.; Li, Z. Improved accuracy of digital implant impressions with newly designed scan bodies: An in vivo evaluation in beagle dogs. BMC Oral Health 2021, 21, 623. [Google Scholar] [CrossRef]
- D’haese, R.; Vrombaut, T.; Roeykens, H.; Vandeweghe, S. In Vitro Accuracy of Digital and Conventional Impressions for Full-Arch Implant-Supported Prostheses. JCM 2022, 11, 594. [Google Scholar] [CrossRef]
- Michelinakis, G.; Apostolakis, D.; Kamposiora, P.; Papavasiliou, G.; Özcan, M. The direct digital workflow in fixed implant prosthodontics: A narrative review. BMC Oral Health 2021, 21, 37. [Google Scholar] [CrossRef]
- Schmidt, A.; Billig, J.-W.; Schlenz, M.A.; Rehmann, P.; Wöstmann, B. Influence of the Accuracy of Intraoral Scanbodies on Implant Position: Differences in Manufacturing Tolerances. Int. J. Prosthodont. 2019, 32, 430–432. [Google Scholar] [CrossRef]
- Arcuri, L.; Lio, F.; Campana, V.; Mazzetti, V.; Federici, F.R.; Nardi, A.; Galli, M. Influence of Implant Scanbody Wear on the Accuracy of Digital Impression for Complete-Arch: A Randomized In Vitro Trial. Materials 2022, 15, 927. [Google Scholar] [CrossRef]
- Zhang, T.; Yang, B.; Ge, R.; Zhang, C.; Zhang, H.; Wang, Y. Effect of a Novel ‘Scan Body’ on the In Vitro Scanning Accuracy of Full-Arch Implant Impressions. Int. Dent. J. 2024, 74, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Fluegge, T.; Att, W.; Metzger, M.; Nelson, K. A Novel Method to Evaluate Precision of Optical Implant Impressions with Commercial Scan Bodies—An Experimental Approach. J. Prosthodont. 2017, 26, 34–41. [Google Scholar] [CrossRef]
- Mizumoto, R.M.; Yilmaz, B. Intraoral scan bodies in implant dentistry: A systematic review. J. Prosthet. Dent. 2018, 120, 343–352. [Google Scholar] [CrossRef]
- Pachiou, A.; Zervou, E.; Tsirogiannis, P.; Sykaras, N.; Tortopidis, D.; Kourtis, S. Characteristics of intraoral scan bodies and their influence on impression accuracy: A systematic review. J. Esthet. Restor. Dent. 2023, 35, 1205–1217. [Google Scholar] [CrossRef]
- Lawand, G.; Ismail, Y.; Revilla-León, M.; Tohme, H. Effect of implant scan body geometric modifications on the trueness and scanning time of complete arch intraoral implant digital scans: An in vitro study. J. Prosthet. Dent. 2024, 131, 1189–1197. [Google Scholar] [CrossRef]
- Alvarez, C.; Domínguez, P.; Jiménez-Castellanos, E.; Arroyo, G.; Orozco, A. How the geometry of the scan body affects the accuracy of digital impressions in implant supported prosthesis. In vitro study. J. Clin. Exp. Dent. 2022, 14, e1008–e1014. [Google Scholar] [CrossRef]
- Gómez-Polo, M.; Sallorenzo, A.; Ortega, R.; Gómez-Polo, C.; Barmak, A.B.; Att, W.; Revilla-León, M. Influence of implant angulation and clinical implant scan body height on the accuracy of complete arch intraoral digital scans. J. Prosthet. Dent. 2024, 131, 119–127. [Google Scholar] [CrossRef]
- Althubaitiy, R.; Sambrook, R.; Weisbloom, M.; Petridis, H. The Accuracy of Digital Implant Impressions when Using and Varying the Material and Diameter of the Dental Implant Scan Bodies. Eur. J. Prosthodont. Restor. Dent. 2022, 30, 305–313. [Google Scholar]
- Gama, L.T.; Bezerra, A.P.; Schimmel, M.; Rodrigues Garcia, R.C.M.; de Luca Canto, G.; Gonçalves, T.M.S.V. Clinical performance of polymer frameworks in dental prostheses: A systematic review. J. Prosthet. Dent. 2024, 131, 579–590. [Google Scholar] [CrossRef]
- Shetty, P.S.; Gangurde, A.P.; Chauhan, M.R.; Jaiswal, N.V.; Salian, P.R.; Singh, V. Accuracy of the digital implant impression with splinted and non-splinted intraoral scan bodies: A systematic review. J. Indian Prosthodont. Soc. 2025, 25, 3–12. [Google Scholar] [CrossRef]
- Iturrate, M.; Minguez, R.; Pradies, G.; Solaberrieta, E. Obtaining reliable intraoral digital scans for an implant-supported complete-arch prosthesis: A dental technique. J. Prosthet. Dent. 2019, 121, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, R.M.; Yilmaz, B.; McGlumphy, E.A.; Seidt, J.; Johnston, W.M. Accuracy of different digital scanning techniques and scan bodies for complete-arch implant-supported prostheses. J. Prosthet. Dent. 2020, 123, 96–104. [Google Scholar] [CrossRef]
- Llansana, F.; Guirao, S.; Kois, J.C.; Revilla-León, M. Calibrated splinting framework for complete arch intraoral implant digital scans manufactured by combining milled and additively manufacturing technologies: A dental technique. J. Prosthet. Dent. 2024, 132, 680–686. [Google Scholar] [CrossRef]
- Retana, L.; Nejat, A.H.; Pozzi, A. Effect of splinting scan bodies on trueness of complete-arch implant impression using different intraoral scanners: An in vitro study. Int. J. Comput. Dent. 2023, 26, 19–28. [Google Scholar] [CrossRef]
- Paratelli, A.; Vania, S.; Gómez-Polo, C.; Ortega, R.; Revilla-León, M.; Gómez-Polo, M. Techniques to improve the accuracy of complete arch implant intraoral digital scans: A systematic review. J. Prosthet. Dent. 2023, 129, 844–854. [Google Scholar] [CrossRef]
- Bader Eddin, M.B.; Önöral, Ö. Influence of splinting scan bodies or incorporating three-dimensionally printed scan aids on the trueness of complete arch digital scans. J. Prosthet. Dent. 2024, 132, 828.e1–828.e12. [Google Scholar] [CrossRef]
- Denneulin, T.; Rignon-Bret, C.; Ravalec, G.; Tapie, L.; Bouter, D.; Wulfman, C. Accuracy of Complete-Arch Implant Digital Scans: Effect of Scanning Protocol, Number of Implants, and Scan Body Splinting. Int. J. Prosthodont. 2023, 36, 219–227. [Google Scholar] [CrossRef]
- Cheng, J.; Zhang, H.; Liu, H.; Li, J.; Wang, H.-L.; Tao, X. Accuracy of edentulous full-arch implant impression: An in vitro comparison between conventional impression, intraoral scan with and without splinting, and photogrammetry. Clin. Oral Implant. Res. 2024, 35, 560–572. [Google Scholar] [CrossRef]
- Ali, K.; Alzaid, A.A.; Suprono, M.S.; Garbacea, A.; Savignano, R.; Kattadiyil, M.T. Evaluating the effects of splinting implant scan bodies intraorally on the trueness of complete arch digital scans: A clinical study. J. Prosthet. Dent. 2024, 132, 781.e1–781.e7. [Google Scholar] [CrossRef]
- Treesh, J.C.; Liacouras, P.C.; Taft, R.M.; Brooks, D.I.; Raiciulescu, S.; Ellert, D.O.; Grant, G.T.; Ye, L. Complete-arch accuracy of intraoral scanners. J. Prosthet. Dent. 2018, 120, 382–388. [Google Scholar] [CrossRef]
- Pellitteri, F.; Albertini, P.; Vogrig, A.; Spedicato, G.A.; Siciliani, G.; Lombardo, L. Comparative analysis of intraoral scanners accuracy using 3D software: An in vivo study. Prog. Orthod. 2022, 23, 21. [Google Scholar] [CrossRef]
- Kim, M.-K.; Kim, J.-M.; Lee, Y.-M.; Lim, Y.-J.; Lee, S.-P. The effect of scanning distance on the accuracy of intra-oral scanners used in dentistry. Clin. Anat. 2019, 32, 430–438. [Google Scholar] [CrossRef]
- Kaewbuasa, N.; Ongthiemsak, C. Effect of different arch widths on the accuracy of three intraoral scanners. J. Adv. Prosthodont. 2021, 13, 205–215. [Google Scholar] [CrossRef]
- Osnes, C.; Caplan, J.; Ferrari, M.; Keeling, A. Investigating three methods of assessing the clinically relevant trueness of two intraoral scanners. J. Osseointegration 2021, 13, 29–34. [Google Scholar] [CrossRef]
- Li, H.; Lyu, P.; Wang, Y.; Sun, Y. Influence of object translucency on the scanning accuracy of a powder-free intraoral scanner: A laboratory study. J. Prosthet. Dent. 2017, 117, 93–101. [Google Scholar] [CrossRef]
- González de Villaumbrosia, P.; Martínez-Rus, F.; García-Orejas, A.; Salido, M.P.; Pradíes, G. In vitro comparison of the accuracy (trueness and precision) of six extraoral dental scanners with different scanning technologies. J. Prosthet. Dent. 2016, 116, 543–550.e1. [Google Scholar] [CrossRef]
- Bocklet, C.; Renne, W.; Mennito, A.; Bacro, T.; Latham, J.; Evans, Z.; Ludlow, M.; Kelly, A.; Nash, J. Effect of scan substrates on accuracy of 7 intraoral digital impression systems using human maxilla model. Orthod. Craniofacial Res. 2019, 22, 168–174. [Google Scholar] [CrossRef]
- Nedelcu, R.G.; Persson, A.S.K. Scanning accuracy and precision in 4 intraoral scanners: An in vitro comparison based on 3-dimensional analysis. J. Prosthet. Dent. 2014, 112, 1461–1471. [Google Scholar] [CrossRef]
- Güth, J.-F.; Runkel, C.; Beuer, F.; Stimmelmayr, M.; Edelhoff, D.; Keul, C. Accuracy of five intraoral scanners compared to indirect digitalization. Clin. Oral Investig. 2017, 21, 1445–1455. [Google Scholar] [CrossRef]
- Oh, K.C.; Park, J.; Moon, H.S. Effects of Scanning Strategy and Scanner Type on the Accuracy of Intraoral Scans: A New Approach for Assessing the Accuracy of Scanned Data. J. Prosthodont. 2020, 29, 518–523. [Google Scholar] [CrossRef]
- Pattamavilai, S.; Ongthiemsak, C. Accuracy of intraoral scanners in different complete arch scan patterns. J. Prosthet. Dent. 2024, 131, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Wesemann, C.; Kienbaum, H.; Thun, M.; Spies, B.C.; Beuer, F.; Bumann, A. Does ambient light affect the accuracy and scanning time of intraoral scans? J. Prosthet. Dent. 2021, 125, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Ender, A.; Joda, T.; Katsoulis, J. Impact of digital intraoral scan strategies on the impression accuracy using the TRIOS Pod scanner. Quintessence Int. 2016, 47, 343–349. [Google Scholar] [CrossRef]
- Nagy, Z.; Simon, B.; Mennito, A.; Evans, Z.; Renne, W.; Vág, J. Comparing the trueness of seven intraoral scanners and a physical impression on dentate human maxilla by a novel method. BMC Oral Health 2020, 20, 97. [Google Scholar] [CrossRef]
- Mizumoto, R.M.; Alp, G.; Özcan, M.; Yilmaz, B. The effect of scanning the palate and scan body position on the accuracy of complete-arch implant scans. Clin. Implant. Dent. Relat. Res. 2019, 21, 987–994. [Google Scholar] [CrossRef]
- Latham, J.; Ludlow, M.; Mennito, A.; Kelly, A.; Evans, Z.; Renne, W. Effect of scan pattern on complete-arch scans with 4 digital scanners. J. Prosthet. Dent. 2020, 123, 85–95. [Google Scholar] [CrossRef]
- Button, H.; Kois, J.C.; Barmak, A.B.; Zeitler, J.M.; Rutkunas, V.; Revilla-León, M. Scanning accuracy and scanning area discrepancies of intraoral digital scans acquired at varying scanning distances and angulations among 4 different intraoral scanners. J. Prosthet. Dent. 2024, 132, 1044–1060. [Google Scholar] [CrossRef]
- Amornvit, P.; Rokaya, D.; Sanohkan, S. Comparison of Accuracy of Current Ten Intraoral Scanners. BioMed Res. Int. 2021, 2021, 2673040. [Google Scholar] [CrossRef]
- Gómez-Polo, M.; Álvarez, F.; Ortega, R.; Gómez-Polo, C.; Barmak, A.B.; Kois, J.C.; Revilla-León, M. Corrigendum to ‘Influence of the implant scan body bevel location, implant angulation and position on intraoral scanning accuracy: An in vitro study’ [Journal of Dentistry volume 121 (2022) 104122]. J. Dent. 2022, 126, 104274. [Google Scholar] [CrossRef]
- Rotaru, C.; Bica, E.A.; Butnărașu, C.; Săndulescu, M. Three-Dimensional Scanning Accuracy of Intraoral Scanners for Dental Implant Scan Bodies—An Original Study. Medicina 2023, 59, 2037. [Google Scholar] [CrossRef]
- Blatz, M.B.; Conejo, J. The Current State of Chairside Digital Dentistry and Materials. Dent. Clin. N. Am. 2019, 63, 175–197. [Google Scholar] [CrossRef]
- Saini, R.S.; Alshadidi, A.A.F.; Rakhra, J.; Aldosari, L.I.N.; Hassan, S.A.B.; Quadri, S.A.; Madhav, V.N.V.; Avetisyan, A.; Heboyan, A. Text mining analysis of scientific literature on digital intraoral scanners in dentistry: Bibliometric analysis. Digit. Health 2024, 10, 20552076241260837. [Google Scholar] [CrossRef]
- Dönmez, M.B.; Çakmak, G.; Schimmel, M.; Bayadse, M.; Yilmaz, B.; Abou-Ayash, S. Scan accuracy of recently introduced wireless intraoral scanners in different fixed partial denture situations. J. Dent. 2025, 153, 105558. [Google Scholar] [CrossRef]
- Ghadirifard, M.; Eisaei, M.; Hakimaneh, S.M.; Bafandeh, M.A.; Shayegh, S.S. In Vitro Evaluation of the Effect of Scanning Strategy on the Accuracy of Intraoral Scanners: In Vitro Evaluation of the Effect of Scanning Strategy on the Accuracy of Intraoral Scanners. Galen. Med. J. 2024, 13, e3748. [Google Scholar] [CrossRef]
- Lee, H.J.; Oh, K.C. Accuracy of Motion Trajectory Achieved with an Intraoral Scanner: An In Vitro Study with a Proof-of-Concept. Diagnostics 2024, 14, 2713. [Google Scholar] [CrossRef]
- Pozzi, A. The Accuracy of Stereophotogrammetry for Complete-Arch Digital Implant Impression In Vitro and In Vivo. Ph.D. Thesis, Szegedi Tudományegyetem, Szeged, Hungary, 2023; p. 11917. [Google Scholar]
- Pozzi, A.; Agliardi, E.; Lio, F.; Nagy, K.; Nardi, A.; Arcuri, L. Accuracy of intraoral optical scan versus stereophotogrammetry for complete-arch digital implant impression: An in vitro study. J. Prosthodont. Res. 2023, 68, 172–180. [Google Scholar] [CrossRef]
- Kalyan, V.A.; Reddy, T.V.K.; Venkatesh, V.; Kunhikannan, S. Unlocking the Future of Dentistry with Intraoral Scanners. In Science and Technology: Developments and Applications; Jakóbczak, D.J., Ed.; BP International: Hong Kong, China, 2025; Volume 2, pp. 92–107. ISBN 978-93-48859-29-7. [Google Scholar]
- Hamilton, A.; Negreiros, W.M.; Jain, S.; Finkelman, M.; Gallucci, G.O. Influence of scanning protocol on the accuracy of complete-arch digital implant scans: An in vitro study. Clin. Oral Implant. Res. 2024, 35, 641–651. [Google Scholar] [CrossRef]
- Nelwan, S.C.; Karuniadewi, A.A.S.; Nowwarote, N.; Dewi, A.M.; Prayogo, R.D. Accuracy of Digital Intraoral Scans Three-dimensional Surface Analysis Compared with Plaster Models Dental Measurement in Mixed Dentition. Int. J. Clin. Pediatr. Dent. 2025, 17, 1363–1369. [Google Scholar] [CrossRef]
- Pesce, P.; Nicolini, P.; Caponio, V.C.A.; Zecca, P.A.; Canullo, L.; Isola, G.; Baldi, D.; De Angelis, N.; Menini, M. Accuracy of Full-Arch Intraoral Scans Versus Conventional Impression: A Systematic Review with a Meta-Analysis and a Proposal to Standardise the Analysis of the Accuracy. J. Clin. Med. 2024, 14, 71. [Google Scholar] [CrossRef]
- Meshni, A.A.; Jain, S.; Osaysi, H.N.M.; Hezam, K.N.; Adlan, S.S.G. The Comparison of Accuracy of Post Space Digital Impressions Made by Three Different Intraoral Scanners: An In Vitro Study. Diagnostics 2024, 14, 2893. [Google Scholar] [CrossRef]
- Sorrentino, R.; Ruggiero, G.; Leone, R.; Cagidiaco, E.F.; Mauro, M.I.D.; Ferrari, M.; Zarone, F. Trueness and precision of an intraoral scanner on abutments with subgingival vertical margins: An in vitro study. J. Dent. 2024, 144, 104943. [Google Scholar] [CrossRef] [PubMed]
- Rafla, K.A.; Sherif, R.M.; Ghanem, L. Accuracy of Two Digital Scanners (Intraoral, Extraoral) Compared to Conventional Impression Using Implant with Different Angulations (Zero, 15°,25°) “In-Vitro Study”. J. Fundam. Clin. Res. 2024, 4, 172–188. [Google Scholar] [CrossRef]
- Cui, X.; Liu, Y.; Zhang, R.; Wang, X. Accuracy of intraoral versus desktop scanners used in digitizing polyvinyl siloxane impression for fabricating a CAD-CAM customized post and core. J. Prosthodont. 2024, 34, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.; Kim, J.-H.; Park, J.-K.; Son, S.-A. Evaluating the accuracy of CEREC intraoral scanners for inlay restorations: Impact of adjacent tooth materials. BMC Oral Health 2024, 24, 1033. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Author | Criterion 1 | Criterion 2 | Criterion 3 | Criterion 4 | Criterion 5 | Criterion 6 | Criterion 7 | Criterion 8 | Criterion 9 | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Braian M. et al. [53] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Revilla-León M. et al. [54] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Revilla-León M. et al. [2] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Martínez-Rodríguez C. et al. [1] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Diker B. and Tak Ö. [37] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Motel C. et al. [55] | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Moon Y.-G. and Lee K.-M. [56] | 1 | x | 1 | x | 1 | 1 | 1 | 1 | 1 | 7 |
| Schimmel M. et al. [17] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Jivanescu A. et al. [57] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Jin G. et al. [9] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Lee Y.-C. et al. [58] | 1 | x | 1 | 1 | 1 | 1 | 1 | x | 1 | 7 |
| Shin S.-H. et al. [27] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Lim J.-H. et al. [12] | 1 | x | 1 | 1 | 1 | 1 | 1 | x | 1 | 7 |
| Oh H.-S. et al. [59] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Gómez-Polo M. et al. [3] | 1 | 1 | 1 | 1 | x | 1 | 1 | 1 | 1 | 8 |
| Gavounelis N.A. et al. [60] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Kim E.-Y. et al. [61] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Rotar R.N. et al. [62] | 1 | 1 | 1 | 1 | 1 | x | 1 | 1 | 1 | 8 |
| Mai H.Y. et al. [63] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Revilla-León M. et al. [48] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Agustín-Panadero R. et al. [64] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Chang I.-C. et al. [65] | 1 | x | 1 | x | 1 | 1 | 1 | 1 | 1 | 7 |
| Cho J.-H. et al. [66] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Park Y. et al. [28] | 1 | x | 1 | 1 | x | 1 | 1 | 1 | 1 | 7 |
| Shimizu T. et al. [15] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Thomas A.A. and Jain R.K. [10] | 1 | 1 | 1 | x | 1 | 1 | 1 | 1 | 1 | 8 |
| Elter B. and Tak Ö. [67] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Zarauz C. et al. [68] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Sorrentino R. et al. [69] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Karakuzu M. et al. [70] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Jamjoom, F.Z. et al. [71] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Zhou Y. et al. [72] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Ye J.R. and Jain R.K. [24] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | x | 1 | 8 |
| Jamjoom F.Z. et al. [71] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Kim S.-Y. et al. [73] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Liu C.-T. et al. [74] | 1 | x | 1 | x | 1 | 1 | 1 | 1 | 1 | 7 |
| Choi E.-J. et al. [75] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Author (Citation) | C1 | C 2 | C3 | C 4 | C 5 | C 6 | C 7 | C 8 | C9 | C 10 | C 11 | C 12 | C 13 | C 14 | C 15 | C 16 | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hardan L. et al. [33] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 14 |
| Revilla-León M. et al. [4] | 1 | x | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | x | 1 | 1 | 1 | x | 1 | 13 |
| Gehrke P. et al. [76] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | x | x | 1 | 1 | 1 | x | 1 | 13 |
| No. | Authors | Year | Vivo/ Vitro | Factors |
|---|---|---|---|---|
| 1. | Braian M. et al. [53] | 2019 | Vitro | Scanning distance |
| 2. | Revilla-León M. et al. [54] | 2020 | Vivo | Lighting conditions |
| 3. | Diker B. and Tak Ö. [37] | 2020 | Vitro | Scanning sequence |
| 4. | Revilla-León M. et al. [2] | 2020 | Vitro | Lighting conditions |
| 5. | Martínez-Rodríguez C. et al. [1] | 2020 | Vitro | Lighting conditions |
| Surface material | ||||
| Crowding of teeth | ||||
| Inclination of teeth | ||||
| 6. | Motel C. et al. [55] | 2020 | Vitro | Scanning strategy |
| Implant scan body (design) | ||||
| 7. | Moon Y.-G. and Lee K.-M. [56] | 2020 | Vivo | Scanning distance |
| 8. | Lim J.-H. et al. [12] | 2021 | Vitro | Translucency of the materials |
| 9. | Jin G. et al. [9] | 2021 | Vitro | Healing abutments as landmarks |
| Number of missing teeth (edentulous condition) | ||||
| 10. | Schimmel M. et al. [17] | 2021 | Vitro | The experience of the operator |
| 11. | Jivanescu A. et al. [57] | 2021 | Vitro | Lighting conditions |
| 12. | Lee Y.-C. et al. [58] | 2021 | Vitro | Edentulous condition |
| 13. | Oh H.-S. et al. [59] | 2021 | Vitro | Scanning-aid materials |
| 14. | Shin S.-H. et al. [27] | 2021 | Vitro | Material of the bracket |
| 15. | Kim E.-Y. et al. [61] | 2022 | Vitro | Scanning origin |
| 16. | Mai H.Y. et al. [63] | 2022 | Vitro | Scanning strategy |
| 17. | Gómez-Polo M. et al. [3] | 2022 | Vitro | Implant scan body bevel location |
| Implant angulation | ||||
| Implant position | ||||
| 18. | Rotar R.N. et al. [62] | 2022 | Vitro | Scanning distance (height) |
| 19. | Gavounelis N.A. et al. [60] | 2022 | Vitro | Scanning strategy |
| 20. | Shimizu T. et al. [15] | 2023 | Vitro | Landmarks |
| 21. | Elter B. and Tak Ö. [67] | 2023 | Vitro | Adjacent substrate (material) |
| 22. | Revilla-León M. et al. [48] | 2023 | - | Lighting conditions |
| Scanning pattern | ||||
| Implant scan body design | ||||
| Implant scan body splinting techniques | ||||
| Arch location (scanned arch) | ||||
| Implant position | ||||
| Inter-implant distance | ||||
| Implant depth | ||||
| Implant angulation | ||||
| Interdental space (inter-tooth distance) | ||||
| 23. | Zarauz C. et al. [68] | 2023 | Vivo | Age of operator |
| Training of operator (experience) | ||||
| Software version | ||||
| 24. | Chang I.-C. et al. [65] | 2023 | Vitro | Scanning protocol |
| 25. | Hardan L. et al. [33] | 2023 | - | Scanning speed |
| Scanning pattern | ||||
| Landmarks | ||||
| Humidity | ||||
| Scanning-aid (material and agents) | ||||
| Lighting conditions | ||||
| Scanning distance | ||||
| Ambient temperature | ||||
| Software version | ||||
| Scan resolution | ||||
| Size of the scanner head | ||||
| Custom abutment library data | ||||
| 26. | Cho J.-H. et al. [66] | 2023 | Vitro | Translucency of ceramic restorative materials |
| Scanning aid | ||||
| 27. | Thomas A.A. and Jain R.K. [10] | 2023 | Vivo | The experience of the operator |
| 28. | Agustín-Panadero R. et al. [64] | 2023 | Vitro | Wetness of the surface |
| Materials | ||||
| 29. | Park Y. et al. [28] | 2023 | Vitro | Inlay preparation design |
| 30. | Revilla-León M. et al. [4] | 2023 | - | Tooth preparation finishing procedure |
| 31. | Kim S.-Y. et al. [73] | 2024 | Vitro | Inter-tooth distance |
| Proximal axial wall height | ||||
| 32. | Choi E.-J. et al. [75] | 2024 | Vitro | Scan path (scanning pattern) |
| 33. | Gehrke P. et al. [76] | 2024 | - | Implant scan body design, type of ISB |
| Implant scan body material (materials) | ||||
| Implant scan body fit | ||||
| Implant position | ||||
| Implant angulation | ||||
| Operator skill (the experience of the operator) | ||||
| Scanning strategy | ||||
| Scanning aids | ||||
| 34. | Zhou Y. et al. [72] | 2024 | Vitro | Tooth color |
| Lighting conditions | ||||
| 35. | Karakuzu M. et al. [70] | 2024 | Vitro | Lighting conditions |
| 36. | Liu C.-T. et al. [74] | 2024 | Vitro | Scanning strategy |
| 37. | Sorrentino R. et al. [69] | 2024 | Vitro | Palatal morphologies |
| 38. | Jamjoom F.Z. et al. [71] | 2024 | Vitro | Scanning strategy |
| Scanned arch | ||||
| 39. | Jamjoom F.Z. et al. [77] | 2024 | Vitro | Scanning aid (liquid-type) |
| 40. | Ye J.R. and Jain R.K. [24] | 2024 | Vitro | Limited mouth opening |
| No. | Authors | Year | Vivo/ Vitro | Factors |
|---|---|---|---|---|
| 1. | Alkadi L. [32] | 2023 | - | Location of the scanned area |
| Arch width | ||||
| Scan resolution | ||||
| Software versions and updates | ||||
| Scanner head size | ||||
| 2. | Gómez-Polo M. et al. [47] | 2023 | - | Implant scan body retention system |
| 3. | Revilla-León M. et al. [78] | 2021 | - | Implant scan body design |
| IOS—characteristics and maintenance | 1. | Software versions and updates [32,33,68] |
| 2. | Scan resolution [32,33] | |
| 3. | Size of the scanner head [32,33] | |
| 4. | Custom abutment library data [33] | |
| Intraoral morphology | 5. | Crowding of teeth [1] |
| 6. | Inclination of teeth [1] | |
| 7. | Edentulous condition [9,58] | |
| 8. | Palatal morphologies [69] | |
| 9. | Inter-tooth distance [73] | |
| 10. | Inter-implant distance [48] | |
| 11. | Implant position [3,48,76] | |
| 12. | Implant depth [48] | |
| 13. | Implant angulation [3,48,76] | |
| 14. | Implant scan body fit [76] | |
| 15. | Implant scan body bevel location [3] | |
| 16. | Implant scan body design [48,55,76,78] | |
| 17. | Implant scan body retention system [47] | |
| 18. | Implant scan body splinting techniques [48] | |
| 19. | Proximal axial wall height [73] | |
| 20. | Inlay preparation design [28] | |
| 21. | Location of the scanned area [32] | |
| 22. | Arch width [32] | |
| 23. | Limited mouth opening [24] | |
| Intraoral materials | 24. | Materials [1,27,64,67,76] |
| 25. | Translucency of the materials [12,66] | |
| 26. | Tooth preparation finishing procedure [4] | |
| 27. | Tooth color [72] | |
| Ambient conditions | 28. | Lighting conditions [1,2,33,48,54,57,70,72] |
| 29. | Humidity, wetness of the surface [33,64] | |
| 30. | Ambient temperature [33] | |
| Scanning strategy | 31. | Scanning strategy [55,60,63,71,74,76] |
| 32. | Scanning origin [61] | |
| 33. | Scanning distance [33,53] | |
| 34. | Scanned arch [48,71] | |
| 35. | Landmarks [9,15,33] | |
| 36. | Scanning sequence [37] | |
| 37. | Scanning pattern [33,48,75] | |
| 38. | Scanning height [62] | |
| 39. | Scanning speed [33] | |
| 41. | Scanning-aid [33,59,66,76,77] | |
| 42. | Scanning protocol [65] | |
| 43. | Experience of the operator (training and age) [10,17,68,76] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fratila, A.M.; Saceleanu, A.; Arcas, V.C.; Fratila, N.; Earar, K. Enhancing Intraoral Scanning Accuracy: From the Influencing Factors to a Procedural Guideline. J. Clin. Med. 2025, 14, 3562. https://doi.org/10.3390/jcm14103562
Fratila AM, Saceleanu A, Arcas VC, Fratila N, Earar K. Enhancing Intraoral Scanning Accuracy: From the Influencing Factors to a Procedural Guideline. Journal of Clinical Medicine. 2025; 14(10):3562. https://doi.org/10.3390/jcm14103562
Chicago/Turabian StyleFratila, Anca Maria, Adriana Saceleanu, Vasile Calin Arcas, Nicu Fratila, and Kamel Earar. 2025. "Enhancing Intraoral Scanning Accuracy: From the Influencing Factors to a Procedural Guideline" Journal of Clinical Medicine 14, no. 10: 3562. https://doi.org/10.3390/jcm14103562
APA StyleFratila, A. M., Saceleanu, A., Arcas, V. C., Fratila, N., & Earar, K. (2025). Enhancing Intraoral Scanning Accuracy: From the Influencing Factors to a Procedural Guideline. Journal of Clinical Medicine, 14(10), 3562. https://doi.org/10.3390/jcm14103562