
Unraveling the Complex Nexus of Human Papillomavirus (HPV) in Extragenital Keratinocyte Skin Tumors: A Comprehensive Analysis of Bowen’s Disease and In Situ Squamous-Cell Carcinoma

 , ,
, ,  ,
, 

Abstract
1. Introduction
1.1. Overview of Human Papillomavirus (HPV)
1.2. The Role of HPV in Skin Cancers
1.3. Immunosuppression and HPV: A Common Factor for Keratinocyte Skin Cancer Development?
1.4. Prognostic Role, Emerging Therapies, and Future Perspective on HPV
1.5. Is There a Role of HPV in Bowen’s Disease and In Situ SCC?
2. Patients and Methods
Statistical Analysis
3. Results
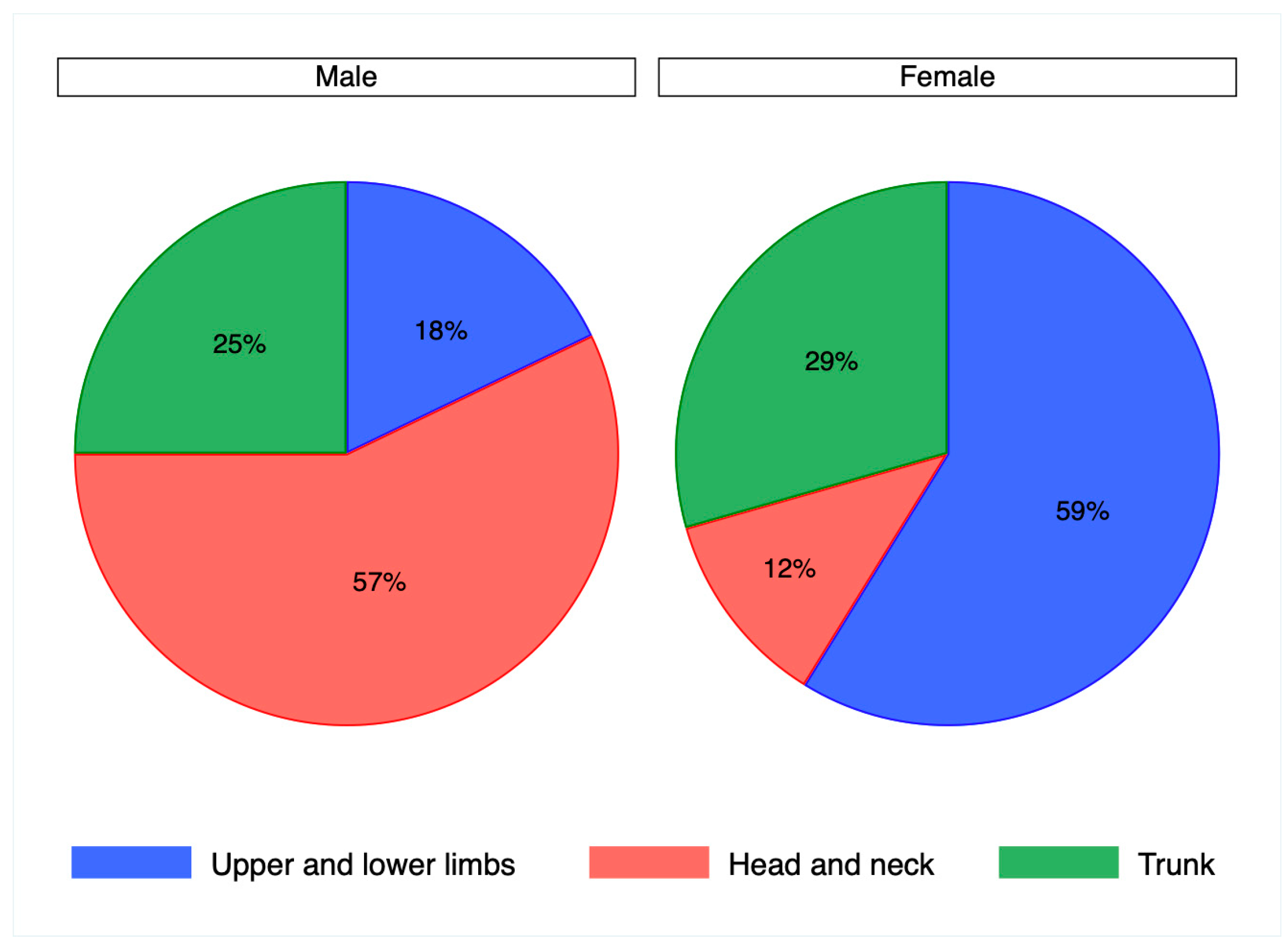
3.1. Demographical Data
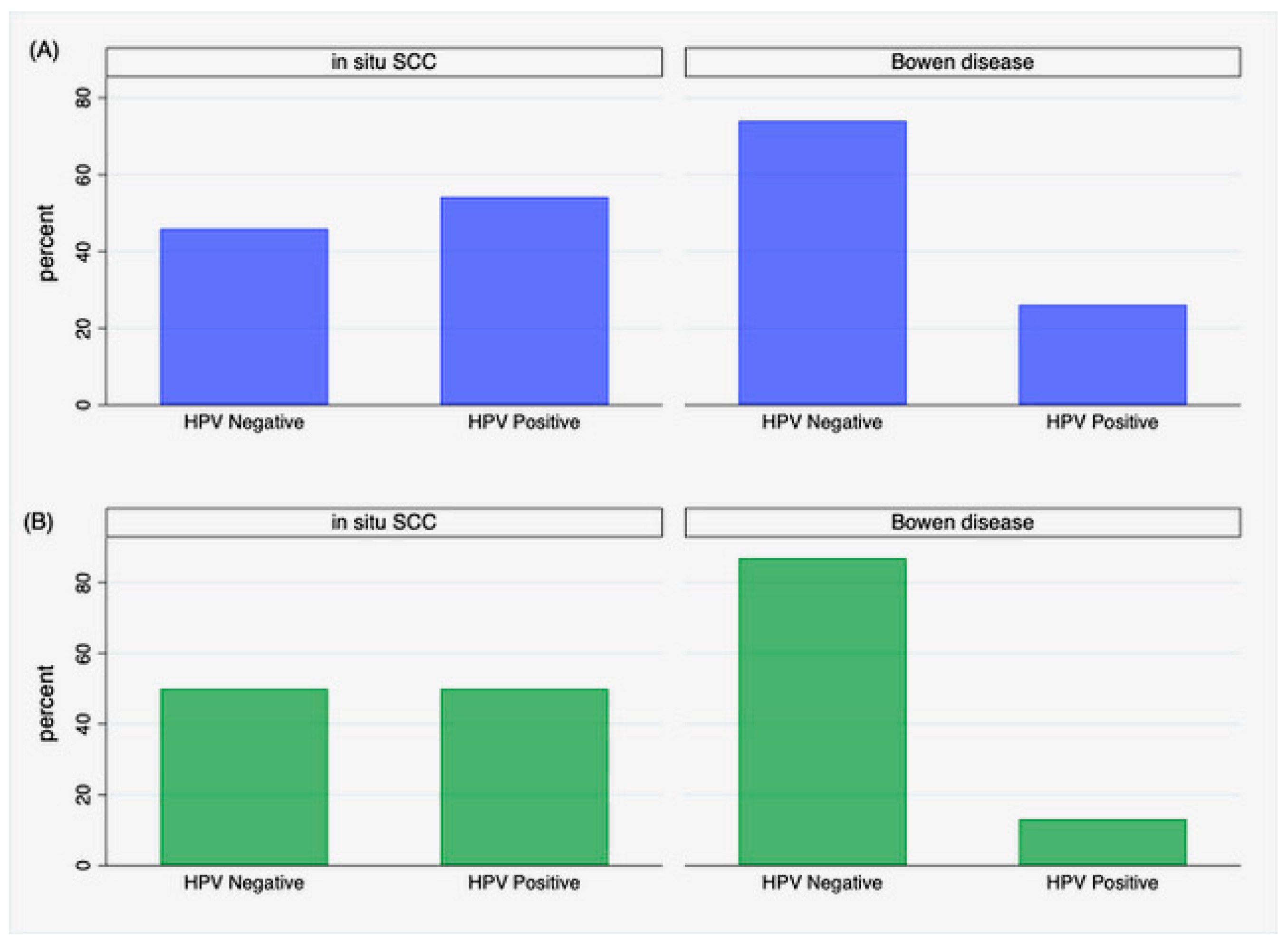
3.2. HPV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neagu, N.; Dianzani, C.; Venuti, A.; Bonin, S.; Voidăzan, S.; Zalaudek, I.; Conforti, C. The role of HPV in keratinocyte skin cancer development: A systematic review. J. Eur. Acad. Dermatol. Venereol. 2023, 37, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, M.; Baharzadeh, F.; Almasi, A.; Sadeghi, M. A Systematic Review and Meta-Analysis: Evaluation of the β-Human Papillomavirus in Immunosuppressed Individuals with Cutaneous Squamous Cell Carcinoma. Biomedicine 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Nindl, I.; Gottschling, M.; Stockfleth, E. Human papillomaviruses and non-melanoma skin cancer: Basic virology and clinical manifes-tations. Dis. Markers 2007, 23, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Waterboer, T.; Abeni, D.; Sampogna, F.; Rother, A.; Masini, C.; Sehr, P.; Michael, K.; Pawlita, M. Serological association of beta and gamma human papillomaviruses with squamous cell carcinoma of the skin. Br. J. Dermatol. 2008, 159, 457–459. [Google Scholar] [CrossRef] [PubMed]
- Farzan, S.F.; Waterboer, T.; Gui, J.; Nelson, H.H.; Li, Z.; Michael, K.M.; Perry, A.E.; Spencer, S.K.; Demidenko, E.; Green, A.C.; et al. Cutaneous alpha, beta and gamma human papillomaviruses in relation to squamous cell carcinoma of the skin: A population-based study. Int. J. Cancer 2013, 133, 1713–1720. [Google Scholar] [CrossRef] [PubMed]
- Švajdler, M., Jr.; Mezencev, R.; Kašpírková, J.; Kacerovská, D.; Kazakov, D.V.; Ondič, O.; Michal, M. Human papillomavirus infection and p16 expression in the immunocompetent patients with extragenital/extraungual Bowen's disease. Diagn Pathol. 2016, 11, 53. [Google Scholar] [CrossRef]
- Conforti, C.; Paolini, F.; Venuti, A.; Dianzani, C.; Zalaudek, I. The detection rate of human papillomavirus in well-differentiated squamous cell carcinoma and keratoacanthoma: Is there new evidence for a viral pathogenesis of keratoacanthoma? Br. J. Dermatol. 2019, 181, 1309–1311. [Google Scholar] [CrossRef] [PubMed]
- Conforti, C.; Giuffrida, R.; Pizzichetta, M.; Di Meo, N.; Magaton-Rizzi, G.; Zalaudek, I. Integrating the concept of field cancerization in the classification and risk assessment of cutaneous squamous cell carcinoma: Proposal for a new classification and terminology of keratinocyte skin cancer. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e327–e330. [Google Scholar] [CrossRef]
- Elder, D.; Massi, D.; Scolyer, R.A. WHO Classification of Skin Tumors, 4th ed.; WHO: Geneva, Switzerland, 2018; Volume 11. [Google Scholar]
- Oyervides-Muñoz, M.A.; Pérez-Maya, A.A.; Rodríguez-Gutiérrez, H.F.; Gómez-Macias, G.S.; Fajardo-Ramírez, O.R.; Treviño, V.; Barrera-Saldaña, H.A.; Garza-Rodríguez, M.L. Understanding the HPV integration and its progression to cervical cancer. Infect. Genet. Evol. 2018, 61, 134–144. [Google Scholar] [CrossRef]
- Burd, E.M. Human papillomavirus and cervical cancer. Clin. Microbiol. Rev. 2003, 16, 1–17. [Google Scholar] [CrossRef]
- Đukić, A.; Lulić, L.; Thomas, M.; Skelin, J.; Bennett Saidu, N.E.; Grce, M.; Banks, L.; Tomaić, V. HPV Oncoproteins and the Ubiquitin Proteasome System: A Signature of Malignancy? Pathogens 2020, 9, 133. [Google Scholar] [CrossRef] [PubMed]
- Scheffner, M.; Werness, B.A.; Huibregtse, J.M.; Levine, A.J.; Howley, P.M. The E6 oncoprotein encoded by human papillomavirus types 16 and 18 promotes the degradation of p53. Cell 1990, 63, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Zapien, D.; Ruiz, F.X.; Poirson, J.; Mitschler, A.; Ramirez, J.; Forster, A.; Cousido-Siah, A.; Masson, M.; Vande Pol, S.; Podjarny, A.; et al. Structure of the E6/E6AP/p53 complex required for HPV-mediated degradation of p53. Nature 2016, 529, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.E.; Cantalupo, P.G.; Pipas, J.M. Identification of Head and Neck Cancer Subtypes Based on Human Papillomavirus Presence and E2F-Regulated Gene Expression. mSphere 2018, 3, e00580-17. [Google Scholar] [CrossRef] [PubMed]
- Galloway, D.A.; Laimins, L.A. Human papillomaviruses: Shared and distinct pathways for pathogenesis. Curr. Opin. Virol. 2015, 14, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Balaji, D.; Kalarani, I.B.; Mohammed, V.; Veerabathiran, R. Potential role of human papillomavirus proteins associated with the development of cancer. Virusdisease 2022, 33, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Balasubramaniam, S.D.; Balakrishnan, V.; Oon, C.E.; Kaur, G. Key Molecular Events in Cervical Cancer Development. Medicina 2019, 55, 384. [Google Scholar] [CrossRef] [PubMed]
- de Sanjosé, S.; Brotons, M.; Pavón, M.A. The natural history of human papillomavirus infection. Best Pract. Res. Clin. Obs. Gynaecol. 2018, 47, 2–13. [Google Scholar] [CrossRef]
- Nishimura, A.; Ono, T.; Ishimoto, A.; Dowhanick, J.J.; Frizzell, M.A.; Howley, P.M.; Sakai, H. Mechanisms of human papillomavirus E2-mediated repression of viral oncogene expression and cervical cancer cell growth inhibition. J. Virol. 2000, 74, 3752–3760. [Google Scholar] [CrossRef]
- Chitsike, L.; Yuan, C.H.; Roy, A.; Boyle, K.; Duerksen-Hughes, P.J. A high-content AlphaScreen™ identifies E6-specific small molecule inhibitors as potential therapeutics for HPV+ head and neck squamous cell carcinomas. Oncotarget 2021, 12, 549–561. [Google Scholar] [CrossRef]
- Hu, Z.; Ding, W.; Zhu, D.; Yu, L.; Jiang, X.; Wang, X.; Zhang, C.; Wang, L.; Ji, T.; Liu, D.; et al. TALEN-mediated targeting of HPV oncogenes ameliorates HPV-related cervical malignancy. J. Clin. Investig. 2015, 125, 425–436. [Google Scholar] [CrossRef]
- Brianti, P.; De Flammineis, E.; Mercuri, S.R. Review of HPV-related diseases and cancers. New Microbiol. 2017, 40, 80–85. [Google Scholar] [PubMed]
- Gordon, R. Skin cancer: An overview of epidemiology and risk factors. Semin. Oncol. Nurs. 2013, 29, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Bouwes Bavinck, J.N.; Neale, R.E.; Abeni, D.; Euvrard, S.; Green, A.C.; Harwood, C.A.; de Koning, M.N.; Naldi, L.; Nindl, I.; Pawlita, M.; et al. Multicenter study of the association between betapapillomavirus infection and cutaneous squamous cell carcinoma. Cancer Res. 2010, 70, 9777–9786. [Google Scholar] [CrossRef]
- Tampa, M.; Mitran, C.I.; Mitran, M.I.; Nicolae, I.; Dumitru, A.; Matei, C.; Manolescu, L.; Popa, G.L.; Caruntu, C.; Georgescu, S.R. The Role of Beta HPV Types and HPV-Associated Inflammatory Processes in Cutaneous Squamous Cell Carcinoma. J. Immunol. Res. 2020, 2020, 5701639. [Google Scholar] [CrossRef]
- Garolla, A.; Graziani, A.; Grande, G.; Ortolani, C.; Ferlin, A. HPV-related diseases in male patients: An underestimated conundrum. J. Endocrinol. Investig. 2023, 47, 261–274. [Google Scholar] [CrossRef]
- Baek, Y.S.; Jeon, J.; Kim, A.; Song, H.J.; Kim, C. Human papillomavirus is more frequently detected in the pelvic than non-pelvic area in patients with squamous cell carcinoma in situ (Bowen’s disease). Eur. J. Dermatol. 2020, 30, 111–118. [Google Scholar] [CrossRef]
- Zakrzewska, K.; Regalbuto, E.; Pierucci, F.; Arvia, R.; Mazzoli, S.; Gori, A.; de Giorgi, V. Pattern of HPV infection in basal cell carcinoma and in perilesional skin biopsies from immunocompetent patients. Virol. J. 2012, 9, 309. [Google Scholar] [CrossRef] [PubMed]
- Ciccarese, G.; Drago, F.; Broccolo, F.; Pastorino, A.; Pizzatti, L.; Atzori, L.; Pilloni, L.; Santinelli, D.; Urbani, A.; Parodi, A.; et al. Oncoviruses and melanomas: A retrospective study and literature review. J. Med. Virol. 2023, 95, e27924. [Google Scholar] [CrossRef]
- Snoeck, R.; Andrei, G.; De Clercq, E. Cidofovir in the treatment of HPV-associated lesions. Verh. K Acad. Geneeskd. Belg. 2001, 63, 93–120; discussion 120–122. [Google Scholar] [PubMed]
- Del Mistro, A.; Chieco Bianchi, L. HPV-related neoplasias in HIV-infected individuals. Eur. J. Cancer 2001, 37, 1227–1235. [Google Scholar] [CrossRef]
- Reusser, N.M.; Downing, C.; Guidry, J.; Tyring, S.K. HPV Carcinomas in Immunocompromised Patients. J. Clin. Med. 2015, 4, 260–281. [Google Scholar] [CrossRef] [PubMed]
- Horsley, A.; Al-Aloul, M. HPV-associated complications post lung transplantation: Why prevention is better than ‘no’ cure. Thorax 2022, 77, 539. [Google Scholar] [CrossRef] [PubMed]
- Savani, B.N.; Goodman, S.; Barrett, A.J. Can routine posttransplant HPV vaccination prevent commonly occurring epithelial cancers after allogeneic stem cell transplantation? Clin. Cancer Res. 2009, 15, 2219–2221. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lindelöf, B.; Sigurgeirsson, B.; Gäbel, H.; Stern, R. Incidence of skin cancer in 5356 patients following organ transplantation. Br. J. Dermatol. 2000, 143, 513–519. [Google Scholar] [PubMed]
- Joo, Y.H.; Lee, Y.S.; Cho, K.J.; Park, J.O.; Nam, I.C.; Kim, C.S.; Kim, S.Y.; Kim, M.S. Characteristics and prognostic implications of high-risk HPV-associated hypopharyngeal cancers. PLoS ONE 2013, 8, e78718. [Google Scholar] [CrossRef]
- Giannella, L.; Di Giuseppe, J.; Delli Carpini, G.; Grelloni, C.; Fichera, M.; Sartini, G.; Caimmi, S.; Natalini, L.; Ciavattini, A. HPV-Negative Adenocarcinomas of the Uterine Cervix: From Molecular Characterization to Clinical Implications. Int. J. Mol. Sci. 2022, 23, 15022. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, P.; Hong, S.; Kono, T.; Hoover, P.; Laimins, L. Topoisomerase 2β Induces DNA Breaks To Regulate Human Papillomavirus Replication. mBio 2021, 12, e00005-21. [Google Scholar] [CrossRef] [PubMed]
- Donmez, H.G.; Tanacan, A.; Unal, C.; Fadiloglu, E.; Onder, S.C.; Portakal, O.; Beksac, M.S. Human papillomavirus infection and autoimmune disorders: A tertiary center experience. Pathog Dis. 2019, 77, ftz028. [Google Scholar] [CrossRef]
- Mii, S.; Amoh, Y.; Tanabe, K.; Kitasato, H.; Sato, Y.; Katsuoka, K. Nestin expression in Bowen's disease and Bowen’s carcinoma associated with human papillomavirus. Eur. J. Dermatol. 2011, 21, 515–519. [Google Scholar] [CrossRef]
- Rodust, P.M.; Stockfleth, E.; Ulrich, C.; Leverkus, M.; Eberle, J. UV-induced squamous cell carcinoma—A role for antiapoptotic signalling pathways. Br. J. Dermatol. 2009, 161 (Suppl. S3), 107–115. [Google Scholar] [CrossRef] [PubMed]
- Conforti, C.; Bonin, S.; Coscarella, G.; Nardon, E.; Perrella, E.; Alessandri-Bonetti, M.; Neagu, N.; Toffoli, L.; Zalaudek, I.; Dianzani, C. The role of cutaneous human-papillomavirus (HPV) infection in situ squamous cell carcinoma: A pilot study. Ital. J. Dermatol. Venerol. 2023, 158, 157–158. [Google Scholar] [CrossRef] [PubMed]
- Conforti, C.; Dianzani, C.; Bonin, S.; Nardon, E.; Giuffrida, R.; Di Meo, N.; Zalaudek, I. Extragenital/extraungueal Bowen disease arising in the absence of field cancerization is not associated with human papillomavirus infection: Results from a pilot study. Australas. J. Dermatol. 2020, 61, e484–e486. [Google Scholar] [CrossRef] [PubMed]
- Bolatti, E.M.; Hošnjak, L.; Chouhy, D.; Re-Louhau, M.F.; Casal, P.E.; Bottai, H.; Kocjan, B.J.; Stella, E.J.; Gorosito, M.D.; Sanchez, A.; et al. High prevalence of Gammapapillomaviruses (Gamma-PVs) in pre-malignant cutaneous lesions of immunocompetent individuals using a new broad-spectrum primer system, and identification of HPV210, a novel Gamma-PV type. Virology 2018, 525, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Flores-Miramontes, M.G.; Torres-Reyes, L.A.; Alvarado-Ruíz, L.; Romero-Martínez, S.A.; Ramírez-Rodríguez, V.; Balderas-Peña, L.M.A.; Vallejo-Ruíz, V.; Piña-Sánchez, P.; Cortés-Gutiérrez, E.I.; Jave-Suárez, L.F.; et al. Human papillomavirus genotyping by Linear Array and Next-Generation Sequencing in cervical samples from Western Mexico. Virol. J. 2015, 12, 161. [Google Scholar] [CrossRef] [PubMed]
- Wenande, E.; Bech-Thomsen, N.; Togsverd-Bo, K.; Haedersdal, M. Off-Label 9-Valent Human Papillomavirus Vaccination for Actinic Keratosis: A Case Series. Case Rep. Dermatol. 2021, 13, 457–463. [Google Scholar] [CrossRef]
- Norval, M. The mechanisms and consequences of ultraviolet-induced immunosuppression. Prog. Biophys. Mol. Biol. 2006, 92, 108–118. [Google Scholar] [CrossRef]
- Yonekura, S.; Egawa, G.; Komori, T.; Kabashima, K. Multiple Bowen’s disease on the finger associated with human papillomavirus type 34. Ski. Health Dis 2023, 3, e238. [Google Scholar] [CrossRef]
- Wen, P.; Liu, H.; Xue, S.; Li, W.; Li, F.; Wang, L. Bowen disease of the nail unit associated with HPV-16 infection in a pemphigus patient following rituximab treatment. Eur. J. Dermatol. 2022, 32, 270–272. [Google Scholar]



{kind=link}
{kind=link}
| Anatomical Sites | Cases (%) | Controls (%) |
|---|---|---|
| Upper and lower limbs | 15 (32%) | 18 (53%) |
| Head and neck | 18 (38%) | 6 (18%) |
| Trunk | 12 (26%) | 10 (29%) |
| Not available | 2 (4%) | 0 (0%) |
| Total | 47 (100%) | 34 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conforti, C.; Retrosi, C.; Agozzino, M.; Dianzani, C.; Nardon, E.; Oliveri, A.; Azzalini, E.; Guida, S.; Pellacani, G.; Di Lella, G.; et al. Unraveling the Complex Nexus of Human Papillomavirus (HPV) in Extragenital Keratinocyte Skin Tumors: A Comprehensive Analysis of Bowen’s Disease and In Situ Squamous-Cell Carcinoma. J. Clin. Med. 2024, 13, 1091. https://doi.org/10.3390/jcm13041091
Conforti C, Retrosi C, Agozzino M, Dianzani C, Nardon E, Oliveri A, Azzalini E, Guida S, Pellacani G, Di Lella G, et al. Unraveling the Complex Nexus of Human Papillomavirus (HPV) in Extragenital Keratinocyte Skin Tumors: A Comprehensive Analysis of Bowen’s Disease and In Situ Squamous-Cell Carcinoma. Journal of Clinical Medicine. 2024; 13(4):1091. https://doi.org/10.3390/jcm13041091
Chicago/Turabian StyleConforti, Claudio, Chiara Retrosi, Marina Agozzino, Caterina Dianzani, Ermanno Nardon, Anselmo Oliveri, Eros Azzalini, Stefania Guida, Giovanni Pellacani, Giovanni Di Lella, and et al. 2024. "Unraveling the Complex Nexus of Human Papillomavirus (HPV) in Extragenital Keratinocyte Skin Tumors: A Comprehensive Analysis of Bowen’s Disease and In Situ Squamous-Cell Carcinoma" Journal of Clinical Medicine 13, no. 4: 1091. https://doi.org/10.3390/jcm13041091
APA StyleConforti, C., Retrosi, C., Agozzino, M., Dianzani, C., Nardon, E., Oliveri, A., Azzalini, E., Guida, S., Pellacani, G., Di Lella, G., Rongioletti, F., Zalaudek, I., & Bonin, S. (2024). Unraveling the Complex Nexus of Human Papillomavirus (HPV) in Extragenital Keratinocyte Skin Tumors: A Comprehensive Analysis of Bowen’s Disease and In Situ Squamous-Cell Carcinoma. Journal of Clinical Medicine, 13(4), 1091. https://doi.org/10.3390/jcm13041091