
The Impact of Rhythmic Physical Activity on Mental Health and Quality of Life in Older Adults with and without Cognitive Impairment: A Systematic Review and Meta-Analysis

 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sources of Information
2.2. Search Strategy
2.3. Eligibility Criteria
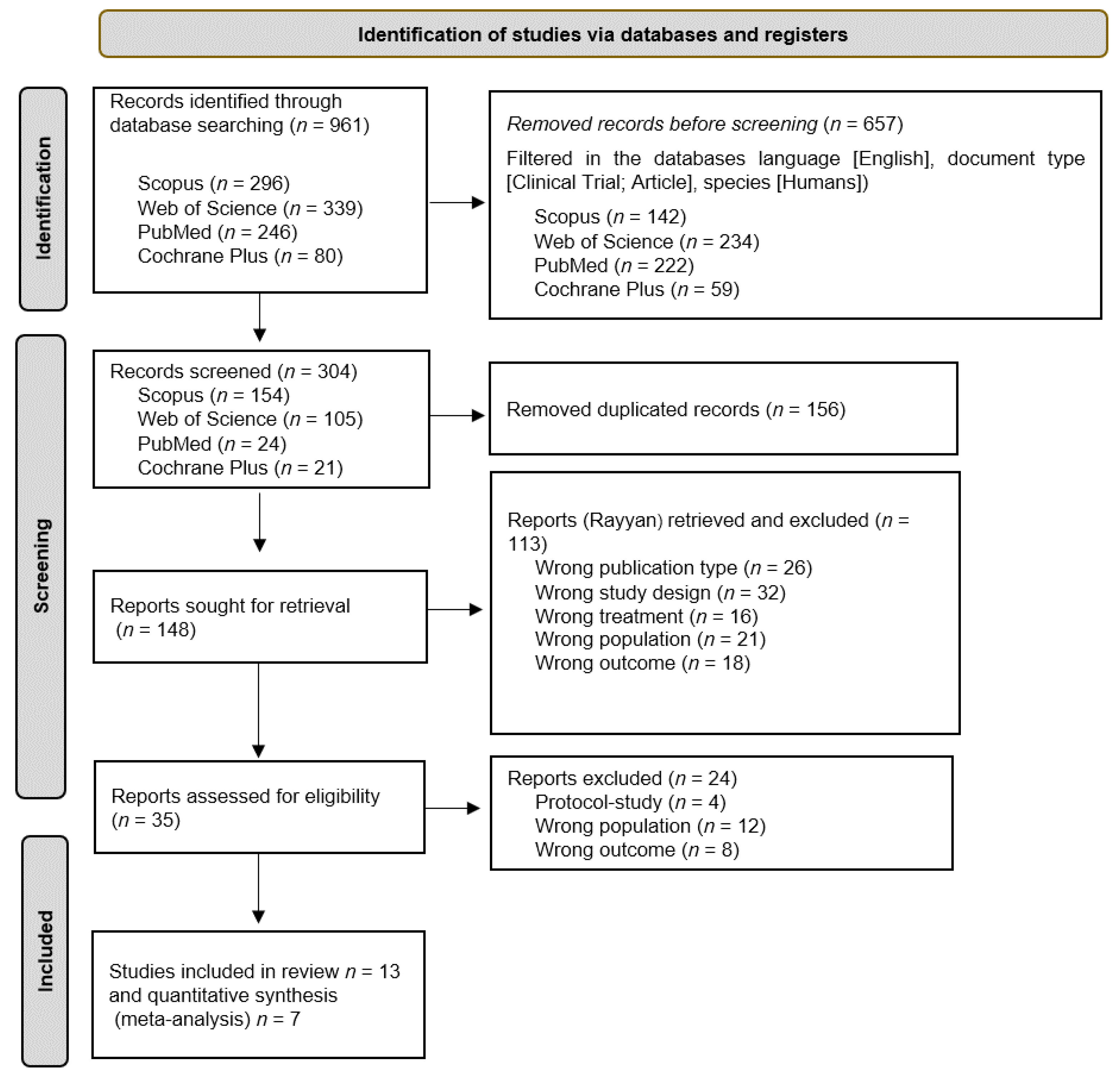
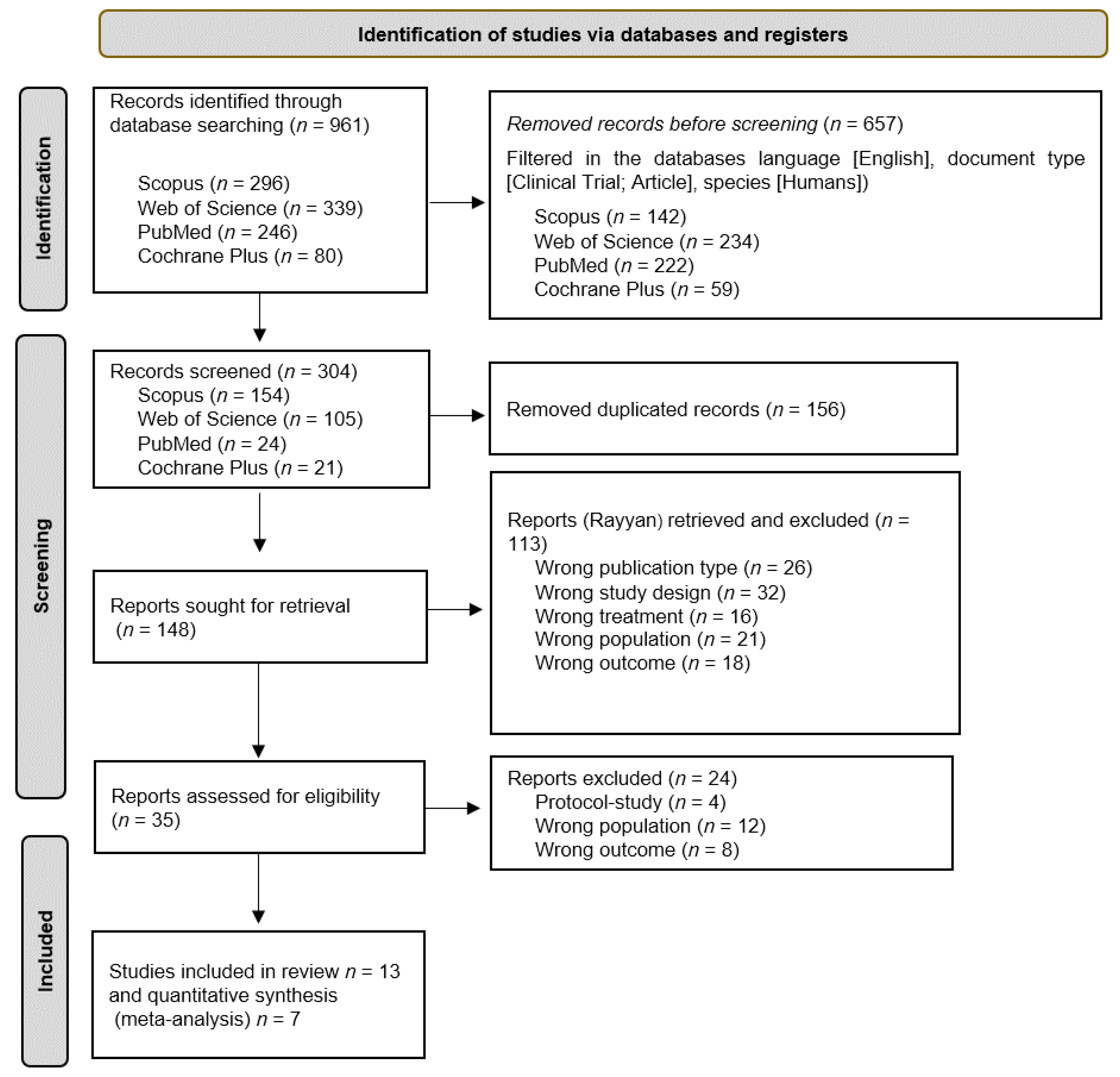
2.4. Study Selection Process
2.5. Data Extraction
2.6. Methodological Quality Assessment
2.7. Analytical Decisions of the Meta-Analysis
3. Results
3.1. Methodology Quality
3.2. Study Characteristics
3.3. Study Results
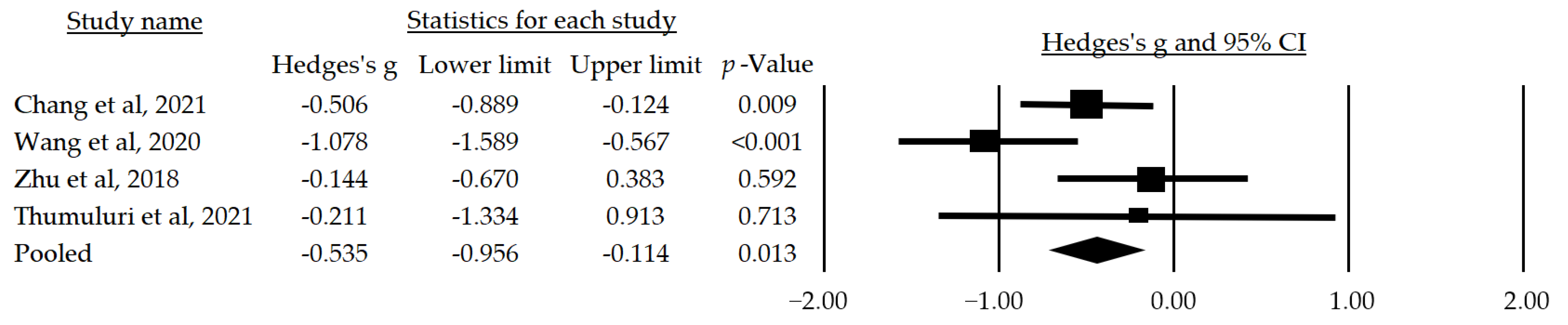
3.4. Meta-Analysis
3.4.1. Depression
3.4.2. Anxiety
3.5. Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crimmins, E.M. Lifespan and Healthspan: Past, Present, and Promise. Gerontologist 2015, 55, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef]
- Aretouli, E.; Brandt, J. Everyday functioning in mild cognitive impairment and its relationship with executive cognition. Int. J. Geriatr. Psychiatry 2010, 25, 224–233. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Evidence Profile: Cognitive Impairment. 2017. Available online: https://www.who.int/ageing/health-systems/icope/evidence-centre/ICOPE-evidence-profile-cognitive.pdf?ua=1 (accessed on 21 July 2023).
- World Health Organization. Global Status Report on the Public Health Response to Dementia; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Alzheimer’s Association. 2019 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2019, 15, 321–387. [Google Scholar] [CrossRef]
- Knopman, D.S.; Petersen, R.C. Mild cognitive impairment and mild dementia: A clinical perspective. Mayo Clin. Proc. 2014, 89, 1452–1459. [Google Scholar] [CrossRef]
- Wiels, W.A.; Wittens, M.M.; Zeeuws, D.; Baeken, C.; Engelborghs, S. Neuropsychiatric symptoms in mild cognitive impairment and dementia due to AD: Relation with disease stage and cognitive deficits. Front. Psychiatry 2021, 12, 707580. [Google Scholar] [CrossRef]
- Lim, Y.Y.; Kong, J.; Maruff, P.; Jaeger, J.; Huang, E.; Ratti, E. Longitudinal cognitive decline in patients with mild cognitive impairment or dementia due to alzheimer’s disease. J. Prev. Alzheimer’s Dis. 2022, 9, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Karkou, V.; Meekums, B. Dance movement therapy for dementia. Cochrane Database Syst. Rev. 2017, 2, Cd011022. [Google Scholar] [CrossRef]
- Möhler, R.; Renom, A.; Renom, H.; Meyer, G. Personally tailored activities for improving psychosocial outcomes for people with dementia in community settings. Cochrane Database Syst. Rev. 2020, 8, 1465–1858. [Google Scholar] [CrossRef]
- Shaji, K.S.; George, R.K.; Prince, M.J.; Jacob, K.S. Behavioral symptoms and caregiver burden in dementia. Indian J. Psychiatry 2009, 51, 45. [Google Scholar] [CrossRef]
- Krishnamoorthy, A.; Anderson, D. Managing challenging behaviour in older adults with dementia. Prog. Neurol. Psychiatry 2011, 15, 20–26. [Google Scholar] [CrossRef]
- Bell, G.; Singham, T.; Saunders, R.; John, A.; Stott, J. Positive psychological constructs and association with reduced risk of mild cognitive impairment and dementia in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2022, 77, 101594. [Google Scholar] [CrossRef] [PubMed]
- Marchant, N.L.; Lovland, L.R.; Jones, R.; Pichet Binette, A.; Gonneaud, J.; Arenaza-Urquijo, E.M.; Chételat, G.; Villeneuve, S.; PREVENT-AD Research Group. Repetitive negative thinking is associated with amyloid, tau, and cognitive decline. Alzheimer’s Dement. 2020, 16, 1054–1064. [Google Scholar] [CrossRef] [PubMed]
- Borglin, G.; Jakobsson, U.; Edberg, A.-K.; Hallberg, I.R. Older people in Sweden with various degrees of present quality of life: Their health, social support, everyday activities and sense of coherence. Health Soc. Care Community 2006, 14, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, C.; Benson, G.S.; Antonenko, D.; Horn, N.; Köbe, T.; Klimecki, O.; Sommer, W.; Wirth, M.; Flöel, A. Negative affective burden is associated with higher resting-state functional connectivity in subjective cognitive decline. Sci. Rep. 2022, 12, 6212. [Google Scholar] [CrossRef]
- Terracciano, A.; Stephan, Y.; Luchetti, M.; Albanese, E.; Sutin, A.R. Personality traits and risk of cognitive impairment and dementia. J. Psychiatr. Res. 2017, 89, 22–27. [Google Scholar] [CrossRef]
- Flicker, L.; Lautenschlager, N.T.; Almeida, O.P. Healthy mental ageing. Br. Menopause Soc. J. 2006, 12, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; James, P.; Zevon, E.S.; Trudel-Fitzgerald, C.; Kubzansky, L.D.; Grodstein, F. Optimism and healthy aging in women and men. Am. J. Epidemiol. 2019, 188, 1084–1091. [Google Scholar] [CrossRef]
- Cohen, R.; Bavishi, C.; Rozanski, A. Purpose in life and its relationship to all-cause mortality and cardiovascular events: A meta-analysis. Psychosom. Med. 2016, 78, 122–133. [Google Scholar] [CrossRef]
- Martín-María, N.; Miret, M.; Caballero, F.F.; Rico-Uribe, L.A.; Steptoe, A.; Chatterji, S.; Ayuso-Mateos, J.L. The impact of subjective well-being on mortality: A meta-analysis of longitudinal studies in the general population. Psychosom. Med. 2017, 79, 565–575. [Google Scholar] [CrossRef]
- Demnitz-King, H.; Gonneaud, J.; Klimecki, O.M.; Chocat, A.; Collette, F.; Dautricourt, S.; Jessen, F.; Krolak-Salmon, P.; Lutz, A.; Morse, R.M.; et al. Association of self-reflection with cognition and brain health in cognitively unimpaired older adults. Neurology 2022, 99, e1422–e1431. [Google Scholar] [CrossRef] [PubMed]
- Herrman, H.; Saxena, S.; Moodie, R. Promoting Mental Health: Concepts, Emerging Evidence, Practice: A Report of the World Health Organization, Department of Mental Health and Substance Abuse in Collaboration with the Victorian Health Promotion Foundation and the University of Melbourne; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Kempermann, G. Embodied prevention. Front. Psychol. 2022, 13, 841393. [Google Scholar] [CrossRef] [PubMed]
- de Witte, M.; Orkibi, H.; Zarate, R.; Karkou, V.; Sajnani, N.; Malhotra, B.; Ho, R.T.H.; Kaimal, G.; Baker, F.A.; Koch, S.C. From therapeutic factors to mechanisms of change in the creative arts therapies: A scoping review. Front. Psychol. 2021, 12, 2525. [Google Scholar] [CrossRef] [PubMed]
- Basso, J.C.; Satyal, M.K.; Rugh, R. Dance on the brain: Enhancing intra- and inter-brain synchrony. Front. Hum. Neurosci. 2021, 14, 586. [Google Scholar] [CrossRef] [PubMed]
- Hewston, P.; Kennedy, C.C.; Borhan, S.; Merom, D.; Santaguida, P.; Ioannidis, G.; Marr, S.; Santesso, N.; Thabane, L.; Bray, S.; et al. Effects of dance on cognitive function in older adults: A systematic review and meta-analysis. Age Ageing 2020, 50, 1084–1092. [Google Scholar] [CrossRef]
- Meng, X.; Li, G.; Jia, Y.; Liu, Y.; Shang, B.; Liu, P.; Bao, X.; Chen, L. Effects of dance intervention on global cognition, executive function and memory of older adults: A meta-analysis and systematic review. Aging Clin. Exp. Res. 2020, 32, 7–19. [Google Scholar] [CrossRef]
- Liu, X.; Shen, P.-L.; Tsai, Y.-S. Dance intervention effects on physical function in healthy older adults: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2021, 33, 253–263. [Google Scholar] [CrossRef]
- Mattle, M.; Chocano-Bedoya, P.O.; Fischbacher, M.; Meyer, U.; Abderhalden, L.A.; Lang, W.; Mansky, R.; Kressig, R.W.; Steurer, J.; Orav, E.J.; et al. Association of dance-based mind-motor activities with falls and physical function among healthy older adults: A systematic review and meta-analysis. JAMA Netw. Open 2020, 3, e2017688. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Chang, J.; Chen, Y.; Liu, C.; Yong, L.; Yang, M.; Zhu, W.; Wang, J.; Yan, J. Effect of square dance exercise on older women with mild mental disorders. Front. Psychiatry 2021, 12, 699778. [Google Scholar] [CrossRef]
- Cheung, D.S.K.; Lai, C.K.Y.; Wong, F.K.Y.; Leung, M.C.P. The effects of the music-with-movement intervention on the cognitive functions of people with moderate dementia: A randomized controlled trial. Aging Ment. Health 2018, 22, 306–315. [Google Scholar] [CrossRef]
- Lazarou, I.; Parastatidis, T.; Tsolaki, A.; Gkioka, M.; Karakostas, A.; Douka, S.; Tsolaki, M. International ballroom dancing against neurodegeneration: A randomized controlled trial in greek community-dwelling elders with mild cognitive impairment. Am. J. Alzheimer’s Dis. Other Dement. 2017, 32, 489–499. [Google Scholar] [CrossRef]
- Ho, R.T.H.; Fong, T.C.T.; Chan, W.C.; Kwan, J.S.K.; Chiu, P.K.C.; Yau, J.C.Y.; Lam, L.C.W. Psychophysiological effects of dance movement therapy and physical exercise on older adults with mild dementia: A randomized controlled trial. J. Gerontol. Ser. B 2018, 75, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Adam, D.; Ramli, A.; Shahar, S. Effectiveness of a combined dance and relaxation intervention on reducing anxiety and depression and improving quality of life among the cognitively impaired elderly. Sultan Qaboos Univ. Med. J. 2016, 16, e47–e53. [Google Scholar] [CrossRef] [PubMed]
- Bisbe, M.; Fuente-Vidal, A.; López, E.; Moreno, M.; Naya, M.; de Benetti, C.; Milà, R.; Bruna, O.; Boada, M.; Alegret, M. Comparative cognitive effects of choreographed exercise and multimodal physical therapy in older adults with amnestic mild cognitive impairment: Randomized clinical trial. J. Alzheimer’s Dis. JAD 2020, 73, 769–783. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yin, H.; Meng, X.; Shang, B.; Meng, Q.; Zheng, L.; Wang, L.; Chen, L. Effects of Chinese square dancing on older adults with mild cognitive impairment. Geriatr. Nurs. 2020, 41, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Tolea, M.I.; Sherman, D.; Rosenfeld, A.; Arcay, V.; Lopes, Y.; Galvin, J.E. Feasibility of conducting nonpharmacological interventions to manage dementia symptoms in community-dwelling older adults: A cluster randomized controlled trial. Am. J. Alzheimer’s Dis. Other Dement. 2020, 35, 1533317519872635. [Google Scholar] [CrossRef]
- Esmail, A.; Vrinceanu, T.; Lussier, M.; Predovan, D.; Berryman, N.; Houle, J.; Karelis, A.; Grenier, S.; Minh Vu, T.T.; Villalpando, J.M.; et al. Effects of dance/movement training vs. aerobic exercise training on cognition, physical fitness and quality of life in older adults: A randomized controlled trial. J. Bodyw. Mov. Ther. 2020, 24, 212–220. [Google Scholar] [CrossRef]
- Hars, M.; Herrmann, F.R.; Gold, G.; Rizzoli, R.; Trombetti, A. Effect of music-based multitask training on cognition and mood in older adults. Age Ageing 2014, 43, 196–200. [Google Scholar] [CrossRef]
- Liao, S.J.; Tan, M.P.; Chong, M.C.; Chua, Y.P. The impact of combined music and tai chi on depressive symptoms among community-dwelling older persons: A cluster randomized controlled trial. Issues Ment. Health Nurs. 2018, 39, 398–402. [Google Scholar] [CrossRef]
- Zhu, Y.; Wu, H.; Qi, M.; Wang, S.; Zhang, Q.; Zhou, L.; Wang, S.; Wang, W.; Wu, T.; Xiao, M.; et al. Effects of a specially designed aerobic dance routine on mild cognitive impairment. Clin. Interv. Aging 2018, 13, 1691–1700. [Google Scholar] [CrossRef] [PubMed]
- Thumuluri, D.; Lyday, R.; Babcock, P.; Ip, E.H.; Kraft, R.A.; Laurienti, P.J.; Barnstaple, R.; Soriano, C.T.; Hugenschmidt, C.E. Improvisational movement to improve quality of life in older adults with early-stage dementia: A pilot study. Front. Sports Act. Living 2021, 3, 796101. [Google Scholar] [CrossRef] [PubMed]
- Savović, J.; Jones, H.E.; Altman, D.G.; Harris, R.J.; Jüni, P.; Pildal, J.; Als-Nielsen, B.; Balk, E.M.; Gluud, C.; Gluud, L.L.; et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Ann. Intern. Med. 2012, 157, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Hidaka, B.H. Depression as a disease of modernity: Explanations for increasing prevalence. J. Affect. Disord. 2012, 140, 205–214. [Google Scholar] [CrossRef]
- Koch, S.C.; Riege, R.F.F.; Tisborn, K.; Biondo, J.; Martin, L.; Beelmann, A. Effects of dance movement therapy and dance on health-related psychological outcomes. a meta-analysis update. Front. Psychol. 2019, 10, 1806. [Google Scholar] [CrossRef]
- Kiepe, M.-S.; Stöckigt, B.; Keil, T. Effects of dance therapy and ballroom dances on physical and mental illnesses: A systematic review. Arts Psychother. 2012, 39, 404–411. [Google Scholar] [CrossRef]
- Robinson, O.; Vytal, K.; Cornwell, B.; Grillon, C. The impact of anxiety upon cognition: Perspectives from human threat of shock studies. Front. Hum. Neurosci. 2013, 7, 203. [Google Scholar] [CrossRef]
- Shao, S. Intervention effect of dance therapy based on the satir model on the mental health of adolescents during the COVID-19 epidemic. Psychiatr. Danub. 2021, 33, 411–417. [Google Scholar] [CrossRef]
- Salihu, D.; Wong, E.M.L.; Kwan, R.Y.C. Effects of an african circle dance programme on internally displaced persons with depressive symptoms: A quasi-experimental study. Int. J. Environ. Res. Public Health 2021, 18, 843. [Google Scholar] [CrossRef]
- Bennett, C.G.; Fox, H.; McLain, M.; Medina-Pacheco, C. Impacts of dance on agitation and anxiety among persons living with dementia: An integrative review. Geriatr. Nurs. 2021, 42, 181–187. [Google Scholar] [CrossRef]
- Rosenberg, P.B.; Lyketsos, C. Mild cognitive impairment: Searching for the prodrome of Alzheimer’s disease. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2008, 7, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Somme, J.; Fernández-Martínez, M.; Molano, A.; Zarranz, J.J. Neuropsychiatric symptoms in amnestic mild cognitive impairment: Increased risk and faster progression to dementia. Curr. Alzheimer Res. 2013, 10, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yin, H.; Jia, Y.; Zhao, L.; Wang, L.; Chen, L. Effects of mind-body exercise on cognitive function in older adults with cognitive impairment: A systematic review and meta-analysis. J. Nerv. Ment. Dis. 2018, 206, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Yi, Q.; Zheng, X.; Cui, S.; Chen, B.; Lu, L.; Tang, C. Effects of mind-body exercises on cognitive function in older adults: A meta-analysis. J. Am. Geriatr. Soc. 2019, 67, 749–758. [Google Scholar] [CrossRef]
- Kwak, Y.T.; Yang, Y.; Koo, M.S. Anxiety in Dementia. Dement. Neurocognitive Disord. 2017, 16, 33–39. [Google Scholar] [CrossRef]
- van Leeuwen, K.M.; van Loon, M.S.; van Nes, F.A.; Bosmans, J.E.; de Vet, H.C.W.; Ket, J.C.F.; Widdershoven, G.A.M.; Ostelo, R.W.J.G. What does quality of life mean to older adults? A thematic synthesis. PLoS ONE 2019, 14, e0213263. [Google Scholar] [CrossRef]
- Ma, C.; Li, M.; Li, R.; Wu, C. The effect of rhythmic movement on physical and cognitive functions among cognitively healthy older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2023, 104, 104837. [Google Scholar] [CrossRef]
- Fatkulina, N.; Hendrixson, V.; Rauckiene-Michealsson, A.; Kievisiene, J.; Razbadauskas, A.; Agostinis Sobrinho, C. Dance/movement therapy as an intervention in breast cancer patients: A systematic review. Evid.-Based Complement. Altern. Med. eCAM 2021, 2021, 4989282. [Google Scholar] [CrossRef]
- Lötzke, D.; Ostermann, T.; Büssing, A. Argentine tango in parkinson disease—a systematic review and meta-analysis. BMC Neurol. 2015, 15, 226. [Google Scholar] [CrossRef]
- Wu, C.C.; Xiong, H.Y.; Zheng, J.J.; Wang, X.Q. Dance movement therapy for neurodegenerative diseases: A systematic review. Front. Aging Neurosci. 2022, 14, 975711. [Google Scholar] [CrossRef]
- Carapellotti, A.M.; Stevenson, R.; Doumas, M. The efficacy of dance for improving motor impairments, non-motor symptoms, and quality of life in parkinson’s disease: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0236820. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authorship | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chang et al., 2021 [33] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 6 |
| Cheung et al., 2016 [34] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Lazarou et al., 2017 [35] | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 6 |
| Ho et al., 2018 [36] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 6 |
| Adam, Ramli, and Shahar, 2016 [37] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 4 |
| Bisbe et al., 2020 [38] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Wang et al., 2020 [39] | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 5 |
| Park et al., 2020 [40] | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Esmail et al., 2019 [41] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7 |
| Hars et al., 2013 [42] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 6 |
| Liao et al., 2018 [43] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 5 |
| Zhu et al., 2018 [44] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7 |
| Thumuluri et al., 2021 [45] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| Author and Year | Cognitive Impairment | Sex | Sample CG/IG | Control Group | Intervention Group | Measuring Instrument | Assessments | Values | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Age | Intervention | Intervention Parameters | ||||||||
| Chang et al., 2021 [33] | Mild mental disorder | F: 100% | 47/62 | Liberal daily lifestyle | 76.56 ± 3.60 | Square dance exercise | I: 100–140 beats per min F: 3 times/week #S: 54 sessions D: 30 min | GDS-15 | T0: baseline T1: 9 weeks T2: 5 months | T0: 4.97 ± 1.41 T1: 4.55 ± 1.17 T2: 4.31 ± 1.14 * |
| Cheung et al., 2016 [34] | Moderate dementia | M: 25.9% F: 74.1% | 53/58 | Social activities | 85.71 ± 6.68 | Music-with-movement intervention | I: not reported F: 2 times/week #S: 12 sessions D: 30 min | GDS-15 | T0: baseline T1: 6 weeks T2: 3 months | T0: 5.99 ± 3.57 T1: Not reported * T2: Not reported |
| Lazarou et al., 2017 [35] | Mild cognitive impairment | M: 21.7% F: 78.3% | 63/66 | Usual care | 65.89 ± 10.76 | International ballroom dancing | I: not reported F: 2 times/week #S: 80 sessions D: 60 min | BDI | T0: baseline T1: 10 months | BDI T0: 10.68 ± 5.89 T1: 8.27 ± 4.55 * |
| Ho et al., 2018 [36] | Mild dementia | M: 19% F: 81% | 68/69 | Waitlist control | 79.4 ± 7.6 | Dance movement therapy | I: moderate intensity F: 2 times/week #S: 24 sessions D: 60 min | GDS-15 | T0: baseline T1: 3 months T2: 6 months T3: 12 months | GDS-15 T0: 0.8 ± 1.1 T1: 0.6 ± 0.9 * T2: 0.7 ± 1.0 T3: 0.7 ± 1.0 |
| Adam, Ramli, and Shahar, 2016 [37] | Cognitively impaired elderly patients | M: 47.7% F: 52.3% | 40/44 | Relaxation exercises | 70.3 ± 6.7 | Combined dance and relaxation | I: not reported F: 2 times/week #S: 12 sessions D: 60 min | HADS | T0: baseline T1: 3 weeks T2: 6 weeks | HADS Depression T0: 7.6 ± 3.1 T1: 5.3 ± 3.0 T2: 3.7 ± 2.7 * Anxiety T0: 7.5 ± 3.5 T1: 6.1 ± 3.6 T2: 4.4 ± 2.7 * |
| Bisbe et al., 2020 [38] | Mild cognitive impairment | M: 52.9% F: 47.1% | 14/17 | Physical therapy | 72.88 ± 5.60 | Choreographed exercise | I: light-to-moderate F: 2 times/week #S: 24 sessions D: 60 min | HADS | T0: baseline T1: 3 months | HADS Depression T0: 6.59 ± 3.00 T1: 6.00 ± 3.43 Anxiety T0: 8.65 ± 4.18 T1: 8.82 ± 3.25 |
| Wang et al., 2020 [39] | Mild cognitive impairment | M: 21.2% F: 78.8% | 33/33 | Usual lifestyle | 81.06 ± 5.17 | Chinese square dancing | I: moderate F: 3 times/week #S: 36 sessions D: 40 min | GDS-15 | T0: baseline T1: 6 weeks T2: 3 months | T0: 4.88 ± 2.85 T1: 3.48 ± 2.32 T2: 2.61 ± 1.71 * |
| Park et al., 2020 [40] | Dementia | M: 58.1% F: 41.9% | 11/10 | Chair exercise | 84.3 ± 7.7 | Music intervention | I: not reported F: 2 times/week #S: 24 sessions D: 45 min | HADS | T0: baseline T1: 6 weeks T2: 3 months | HADS Depression T0: 9.40 ± 4.09 T1: 11.80 ± 4.10 T2: 12.30 ± 4.76 Anxiety T0: 5.40 ± 2.63 T1: 4.90 ± 3.54 T2: 7.89 ± 3.18 |
| Esmail et al., 2019 [41] | Without cognitive impairment | M: 33.3% F: 66.7% | 14/12 | Usual care | 68.08 ± 7.59 | Dance/movement training | I: moderate F: 3 times/week #S: 36 sessions D: 60 min | STAI | T0: baseline T1: 3 months | STAI-State T0: 0.09 ± 0.86 T1: −0.11 ± 1.25 * STAI-Trait T0: 0.07 ± 1.09 T1: 0.16 ± 1.09 |
| Hars et al., 2013 [42] | Without cognitive impairment | M: 3% F: 97% | 68/66 | Waitlist control | 75 ± 8 | Music-based multitask training | I: not reported F: 1 time/week #S: 25 sessions D: 60 min | HADS | T0: baseline T1: 6 months | HADS Depression T0: 6.59 ± 3.00 T1: 6.00 ± 3.43 Anxiety T0: 8.65 ± 4.18 T1: 8.82 ± 3.25 * |
| Liao et al., 2018 [43] | Without cognitive impairment | M: 38.3% F: 61.7% | 52/55 | Routine health education | 71.79 ± 7.7 | Combined music and Tai Chi | I: moderate F: 3 times/week #S: 36 sessions D: 50 min | GDS-15 | T0: baseline T1: 1 month T2: 2 months T3: 3 months | T0: 15.8 ± 4.4 T1: 14.8 ± 4.4 T2: 14.2 ± 4.5 T3: 13.3 ± 4.3 * |
| Zhu et al., 2018 [44] | Mild cognitive impairment | M: 48.3% F: 51.7% | 31/29 | Usual care | 70.3 ± 6.7 | Aerobic dance routine | I: moderate F: 3 times/week #S: 36 sessions D: 35 min | GDS-15 | T0: baseline T1: 3 months T2: 6 months | T0: 12.3 ± 7.2 T1: 10.4 ± 6.0 T2: 10.2 ± 7.0 |
| Thumuluri et al., 2021 [45] | Early-stage dementia | M: 20% F: 80% | 5/5 | Usual care | 74.15 ± 8.28 | Improvisational movement | I: not reported F: 2 times/week #S: 16 sessions D: 60 min | GDS-15 | T0: baseline T1: 2 months | T0: 1.2 ± 1.64 T1: 1.8 ± 1.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Alcalá, M.; Aibar-Almazán, A.; Afanador-Restrepo, D.F.; Carcelén-Fraile, M.d.C.; Achalandabaso-Ochoa, A.; Castellote-Caballero, Y.; Hita-Contreras, F. The Impact of Rhythmic Physical Activity on Mental Health and Quality of Life in Older Adults with and without Cognitive Impairment: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 7084. https://doi.org/10.3390/jcm12227084
Sánchez-Alcalá M, Aibar-Almazán A, Afanador-Restrepo DF, Carcelén-Fraile MdC, Achalandabaso-Ochoa A, Castellote-Caballero Y, Hita-Contreras F. The Impact of Rhythmic Physical Activity on Mental Health and Quality of Life in Older Adults with and without Cognitive Impairment: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(22):7084. https://doi.org/10.3390/jcm12227084
Chicago/Turabian StyleSánchez-Alcalá, Marcelina, Agustín Aibar-Almazán, Diego Fernando Afanador-Restrepo, María del Carmen Carcelén-Fraile, Alexander Achalandabaso-Ochoa, Yolanda Castellote-Caballero, and Fidel Hita-Contreras. 2023. "The Impact of Rhythmic Physical Activity on Mental Health and Quality of Life in Older Adults with and without Cognitive Impairment: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 22: 7084. https://doi.org/10.3390/jcm12227084
APA StyleSánchez-Alcalá, M., Aibar-Almazán, A., Afanador-Restrepo, D. F., Carcelén-Fraile, M. d. C., Achalandabaso-Ochoa, A., Castellote-Caballero, Y., & Hita-Contreras, F. (2023). The Impact of Rhythmic Physical Activity on Mental Health and Quality of Life in Older Adults with and without Cognitive Impairment: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(22), 7084. https://doi.org/10.3390/jcm12227084