

Public Knowledge about Dementia in Poland—A Survey Study


Abstract
:1. Introduction
2. Materials and Methods
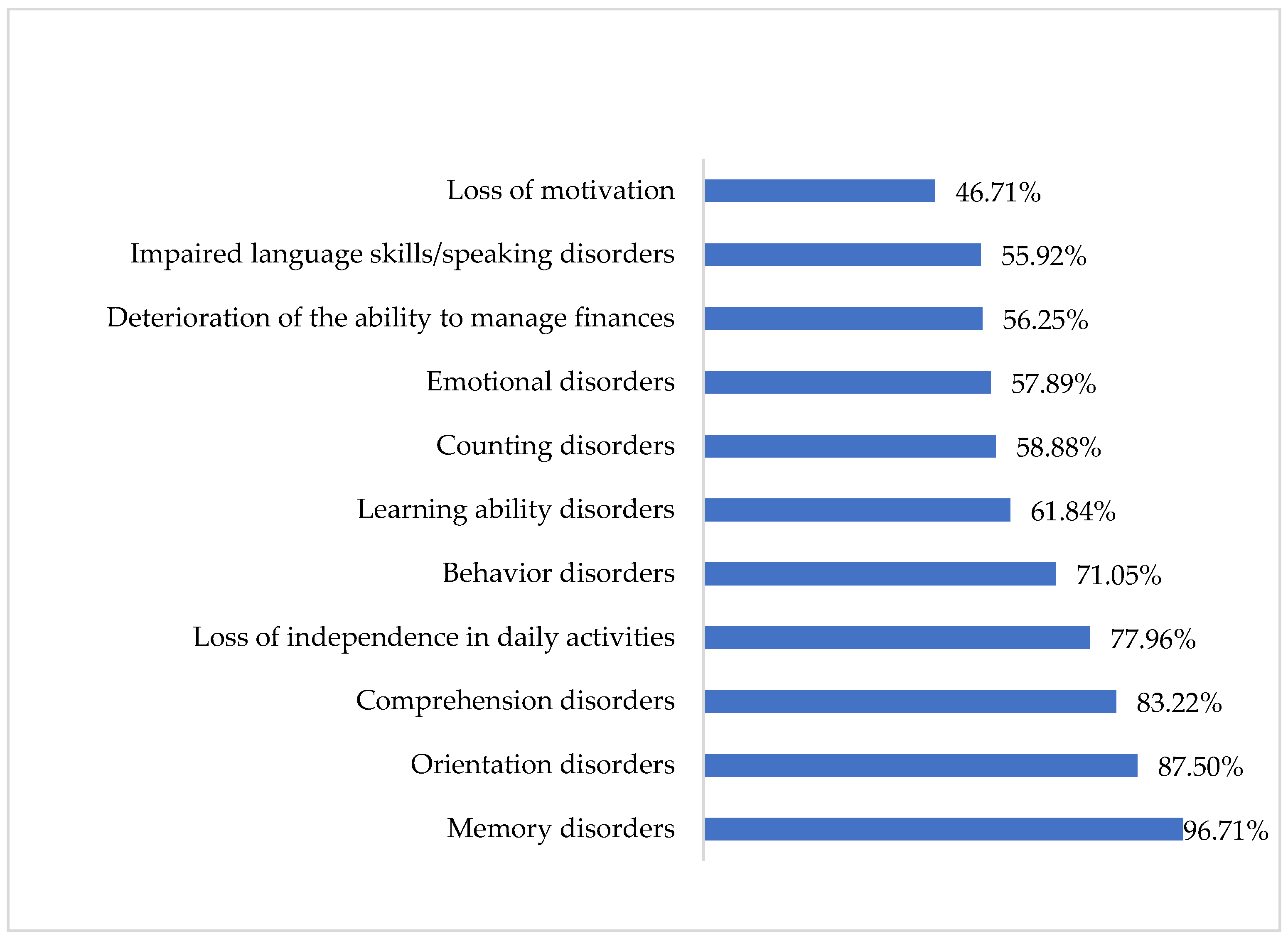
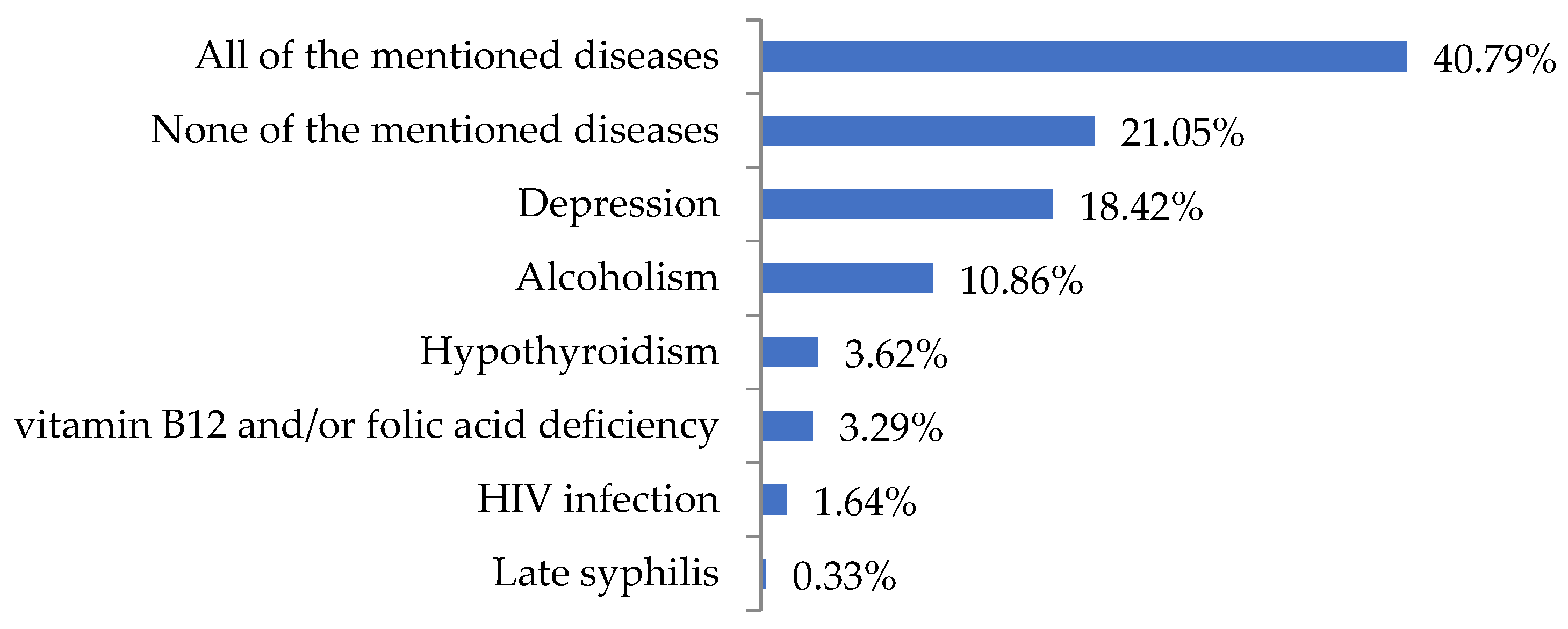
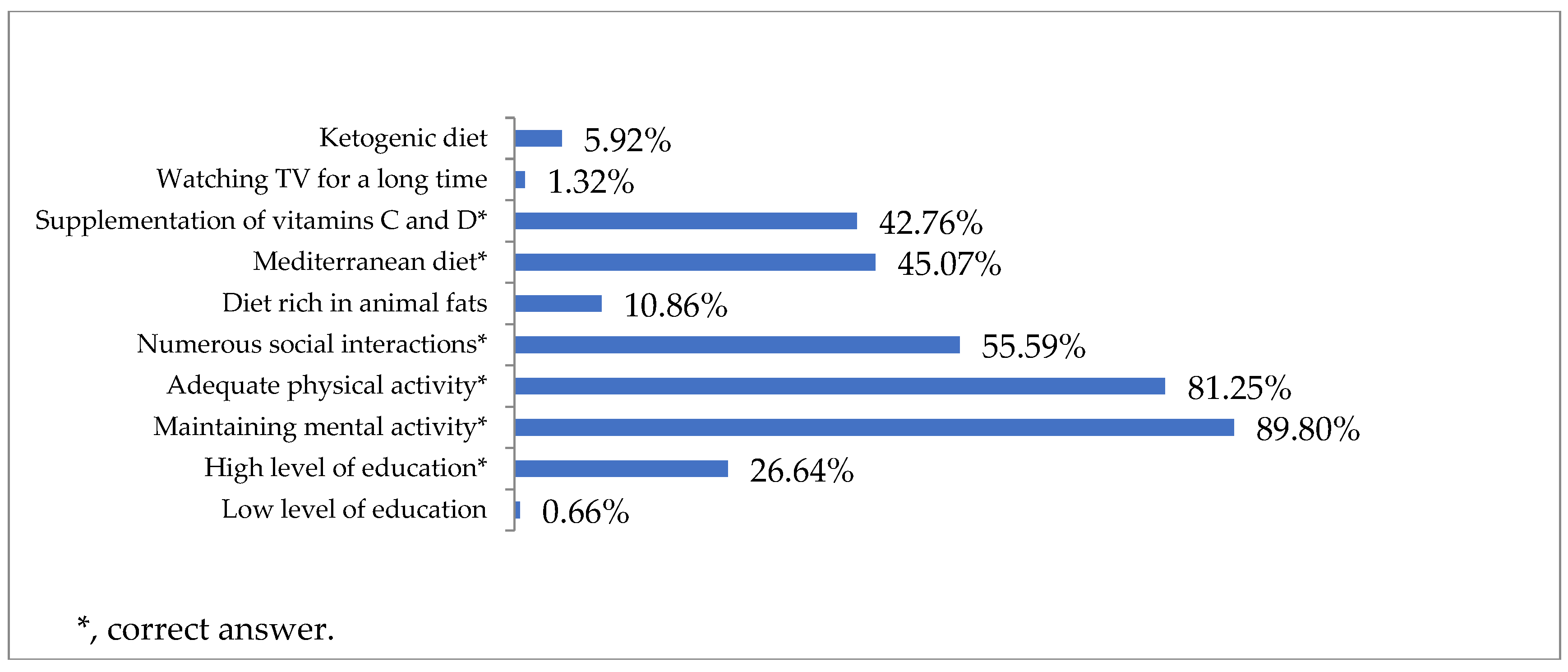
3. Results
4. Discussion
5. Limitation of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Dementia Forecasting Collaborators. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, 105–125. [Google Scholar] [CrossRef]
- Annear, M.J.; Toye, C.; Elliott, K.E.J.; McInerney, F.; Eccleston, C.; Robinson, A. Dementia knowledge assessment scale (DKAS): Confirmatory factor analysis and comparative subscale scores among an international cohort. BMC Geriatr. 2017, 17, 168. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Status Report on the Public Health Response to Dementia; World Health Organization: Geneva, Switzerland, 2021; pp. 19–48. [Google Scholar]
- Felstead, C.; Perkins, L.; Stott, J.; Hui, E.K.; Spector, A. A systematic literature review of group-based training interventions for informal carers: Impact on the behavioural and psychological symptoms of dementia (BPSD). Aging Ment. Health 2022, 27, 1246–1255. [Google Scholar] [CrossRef] [PubMed]
- Cerejeira, J.; Lagarto, L.; Mukaetova-Ladinska, E. Behavioral and psychological symptoms of dementia. Front. Neurol. 2012, 3, 73. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Regional Health-Europe. Challenges for addressing dementia. Lancet Reg. Health Eur. 2022, 20, 100504. [Google Scholar] [CrossRef] [PubMed]
- Alzheimer Europe. Dementia in Europe Yearbook 2019. Estimating the Prevalence of Dementia in Europe; Alzheimer Europe: Luxembourg, 2020; pp. 9–16. [Google Scholar]
- Wu, Y.T.; Beiser, A.; Breteler, M.; Fratiglioni, L.; Helmer, C.; Hendrie, H.C.; Honda, H.; Ikram, M.A.; Langa, K.M.; Lobo, A.; et al. The changing prevalence and incidence of dementia over time—Current evidence. Nat. Rev. Neurol. 2017, 13, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef]
- Gao, S.; Burney, H.N.; Callahan, C.M.; Purnell, C.E.; Hendrie, H.C. Incidence of dementia and Alzheimer disease over time: A meta-analysis. J. Am. Geriatr. Soc. 2019, 67, 1361–1369. [Google Scholar] [CrossRef]
- Matthews, F.E.; Stephan, B.C.; Robinson, L.; Jagger, C.; Barnes, L.E.; Arthur, A.; Brayne, C.; Comas-Herrera, A.; Wittenberg, R.; Dening, T.; et al. A two decade dementia incidence comparison from the Cognitive Function and Ageing Studies I and II. Nat. Commun. 2016, 7, 11398. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Dugravot, A.; Shipley, M.; Brunner, E.J.; Elbaz, A.; Sabia, S.; Kivimaki, M. Obesity trajectories and risk of dementia: 28 years of follow-up in the Whitehall II Study. Alzheimer’s Dement. 2018, 14, 178–186. [Google Scholar] [CrossRef]
- Lee, C.M.; Woodward, M.; Batty, G.D.; Beiser, A.S.; Bell, S.; Berr, C.; Bjertness, E.; Chalmers, J.; Clarke, R.; Dartigues, J.; et al. Association of anthropometry and weight change with risk of dementia and its major subtypes: A meta-analysis consisting 2.8 million adults with 57294 cases of dementia. Obes. Rev. 2020, 21, e12989. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- Ghahremani, M.; Smith, E.E.; Chen, H.-Y.; Creese, B.; Goodarzi, Z.; Ismail, Z. Vitamin D supplementation and incident dementia: Effects of sex, APOE, and baseline cognitive status. Alzheimer’s Dement. 2023, 15, e12404. [Google Scholar] [CrossRef] [PubMed]
- Ismail, Z.; Black, S.E.; Camicioli, R.; Chertkow, H.; Herrmann, N.; Laforce, R.; Montero-Odasso, M.; Rockwood, K.; Rosa-Neto, P.; Seitz, D.; et al. Recommendations of the 5th Canadian Consensus Conference on the diagnosis and treatment of dementia. Alzheimer’s Dement. 2020, 16, 1182–1195. [Google Scholar] [CrossRef] [PubMed]
- Sanderson-Cimino, M.; Elman, J.A.; Tu, X.M.; Gross, A.L.; Panizzon, M.S.; Gustavson, D.E.; Bondi, M.W.; Edmonds, E.C.; Eglit, G.M.; Eppig, J.S.; et al. Cognitive practice effects delay diagnosis of MCI: Implications for clinical trials. Alzheimer’s Dement. 2022, 8, e12228. [Google Scholar] [CrossRef]
- Moreno-Morales, C.; Calero, R.; Moreno-Morales, P.; Pintado, C. Music Therapy in the Treatment of Dementia: A Systematic Review and Meta-Analysis. Front. Med. 2020, 7, 160. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.-J.; Lee, D.Y.; Sung, M.R. Public Knowledge about Dementia in South Korea: A Community-Based Cross-Sectional Survey. Int. Psychogeriatr. 2015, 27, 463–469. [Google Scholar] [CrossRef]
- Smith, B.J.; Ali, S.; Quach, H. Public knowledge and beliefs about dementia risk reduction: A national survey of Australians. BMC Public Health 2014, 14, 661. [Google Scholar] [CrossRef]
- Glynn, R.W.; Shelley, E.; Lawlor, B.A. Public knowledge and understanding of dementia—Evidence from a national survey in Ireland. Age Ageing 2017, 46, 865–869. [Google Scholar] [CrossRef]
- Kjelvik, G.; Rokstad, A.M.M.; Stuebs, J.; Thingstad, P.; Deckers, K.; Köhler, S.; Selbæk, G. Public knowledge about dementia risk reduction in Norway. BMC Public Health 2022, 22, 2046. [Google Scholar] [CrossRef]
- Leszko, M.; Carpenter, B.D. Reliability and Validity of the Polish Version of the Alzheimer’s Disease Knowledge Scale. Dement. Geriatr. Cogn. Disord. 2021, 50, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, T.R.; Waldemar, G. Knowledge and perceptions of dementia and Alzheimer’s disease in four ethnic groups in Copenhagen, Denmark. Int. J. Geriatr. Psychiatry 2016, 31, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Leong, S.-M.; Che, S.-L.; Van, I.-K.; Chuang, Y.-C. Comparisons of Dementia Knowledge and Attitudes among the Youth and Older Adults: Insights from the Construal Level Theory Perspective. Int. J. Environ. Res. Public Health 2022, 19, 1928. [Google Scholar] [CrossRef] [PubMed]
- Keller, M.; McCleskey, S.; Mays, A.; Sarkisian, C. 41896 Surveying knowledge of quality of dementia care among Latino caregivers. J. Clin. Transl. Sci. 2021, 5, 85. [Google Scholar] [CrossRef]
- Robinson, A.; Eccleston, C.; Annear, M.; Elliott, K.-E.; Andrews, S.; Stirling, C.; Ashby, M.; Donohue, C.; Banks, S.; Toye, C.; et al. Who Knows, who Cares? Dementia Knowledge among Nurses, Care Workers, and Family members of People Living with Dementia. J. Palliat. Care 2014, 30, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Jones, C.; Wu, M.-L.; Moyle, W. Healthcare professionals’ dementia knowledge and attitudes towards dementia care and family carers’ perceptions of dementia care in China: An integrative review. J. Clin. Nurs. 2020, 31, 1753–1775. [Google Scholar] [CrossRef]
- Wang, M.; Xu, X.; Huang, Y.; Shao, S.; Chen, X.; Li, J.; Du, J. Knowledge, attitudes and skills of dementia care in general practice: A cross-sectional study in primary health settings in Beijing, China. BMC Fam. Pract. 2020, 21, 89. [Google Scholar] [CrossRef]
- Annear, M.J. Knowledge of Dementia Among the Australian Health Workforce: A National Online Survey. J. Appl. Gerontol. 2020, 39, 62–73. [Google Scholar] [CrossRef]
- Eichler, T.; Thyrian, J.R.; Hertel, J.; Köhler, L.; Wucherer, D.; Dreier, A.; Michalowsky, B.; Teipel, S.; Hoffmann, W. Rates of formal diagnosis in people screened positive for dementia in primary care: Results of the DelpHi-Trial. J. Alzheimer’s Dis. 2014, 42, 451–458. [Google Scholar] [CrossRef]
- Wilcock, J.; Iliffe, S.; Turner, S.; Bryans, M.; O’Carroll, R.; Keady, J.; Levin, E.; Downs, M. Concordance with clinical practice guidelines for dementia in general practice. Aging Ment. Health 2009, 13, 155–161. [Google Scholar] [CrossRef]
- Polacsek, M.; Goh, A.; Malta, S.; Hallam, B.; Gahan, L.; Cooper, C.; Low, L.; Livingston, G.; Panayiotou, A.; Loi, S.; et al. ‘I know they are not trained in dementia’: Addressing the need for specialist dementia training for home care workers. Health Soc. Care Community 2020, 28, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.A.; Hur, H.K. Formal Nursing Home Caregivers’ Dementia Knowledge, Empathy, and Burden of Care from Behavioral and Psychological Symptoms of Dementia. J. Korean Gerontol. Nurs. 2020, 22, 216–225. [Google Scholar] [CrossRef]
- Zülke, A.E.; Luppa, M.; Köhler, S.; Riedel-Heller, S.G. Knowledge of risk and protective factors for dementia in older German adults A population-based survey on risk and protective factors for dementia and internet-based brain health interventions. PLoS ONE 2022, 17, e0277037. [Google Scholar] [CrossRef] [PubMed]
- Rosato, M.; Leavey, G.; Cooper, J.; De Cock, P.; Devine, P. Factors associated with public knowledge of and attitudes to dementia: A cross-sectional study. PLoS ONE 2019, 14, e0210543. [Google Scholar] [CrossRef] [PubMed]
- The Wicking Dementia Research and Education Centre; University of Tasmania: Hobart, Australia, 2023; Available online: https://mooc.utas.edu.au/ (accessed on 1 August 2023).
- Eccleston, C.; Doherty, K.; Bindoff, A.; Robinson, A.; Vickers, J.; McInerney, F. Building dementia knowledge globally through the Understanding Dementia Massive Open Online Course (MOOC). Npj Sci. Learn. 2019, 4, 3. [Google Scholar] [CrossRef]
- Su, H.F.; Koo, M.; Lee, W.L.; Sung, H.-C.; Lee, R.-P.; Liu, W.-I. A dementia care training using mobile e-learning with mentoring support for home care workers: A controlled study. BMC Geriatr. 2021, 21, 126. [Google Scholar] [CrossRef]
- Nguyen, B.; Woo, B. Sharing is caring: WhatsApp as a method of disseminating dementia knowledge to elderly Chinese Americans. Int. Psychogeriatr. 2020, 32, 281–282. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean Age, X ± SD | 34 ± 12.82 |
| Gender, n (%) | |
| Women | 236 (77.63) |
| Men | 68 (22.37) |
| Level of education, n (%) | |
| Primary | 2 (0.66) |
| Vocational | 6 (1.97) |
| Secondary | 114 (37.5) |
| Higher | 182 (59.87) |
| Place of residence, n (%) | |
| Rural | 36 (11.85) |
| Urban, city under 100,000 inhabitants | 100 (32.89) |
| Urban, city from 100 to 500,000 inhabitants | 110 (36.18) |
| Urban, city with over 500,000 inhabitants | 58 (19.08) |
| Province, n (%) | |
| Lower Silesia | 14 (4.6) |
| Kuyavian-Pomerania | 3 (0.99) |
| Lodz Province | 8 (2.63) |
| Lublin Province | 10 (3.29) |
| Lubusz Province | 5 (1.64) |
| Lesser Poland | 19 (6.25) |
| Masovia | 28 (9.21) |
| Opole Province | 10 (3.29) |
| Subcarpathian Province | 22 (7.24) |
| Podlasie Province | 1 (0.33) |
| Pomerania | 2 (0.66) |
| Silesia | 157 (51.64) |
| Holly Cross Province | 3 (0.99) |
| Greater Poland | 14 (4.61) |
| West Pomeranian | 8 (2.63) |
| Warmia-Masuria | 0 (0.00) |
| Do you study/work in the medical/medical-related industry? | |
| Yes | 117 (38.49) |
| No | 187 (61.51) |
| Have you ever heard or read about dementia/dementia syndromes? | |
| Yes | 276 (90.79) |
| No | 18 (5.92) |
| I do not know | 10 (3.29) |
| Is there a history of dementia in your family? | |
| Yes | 133 (43.75) |
| No | 128 (42.11) |
| I do not know | 43 (14.14) |
| Are you a person who has cared for or is currently caring for someone with dementia? | |
| Yes | 71 (23.36) |
| No | 233 (76.64) |
| % of Maximum Score (23.6 Points) | p-Value * | |
|---|---|---|
| Total | 71.81% | |
| Gender | ||
| Women | 72.54% | |
| Men | 69.69% | 0.089 |
| Do you study/work in the medical/medical-related industry? | ||
| Yes | 76.60% | |
| No | 67.99% | 0.0001 |
| Have you ever heard or read about dementia/dementia syndromes? | ||
| Yes | 72.06% | |
| No | 61.25% | 0.0001 |
| Is there a history of dementia in your family? | ||
| Yes | 72.00% | |
| No | 70.88% | 0.429 |
| Are you a person who has cared for or is currently caring for someone with dementia? | ||
| Yes | 71.19% | |
| No | 71.34% | 0.925 |
| Question | Answers, n (%) | ||
|---|---|---|---|
| True | False | ||
| 1 | Dementia is a natural condition of the aging process. | 136 (44.74) | * 168 (55.26) |
| 2 | Dementia is the result of changes in the brain. | * 300 (98.68) | 4 (1.32) |
| 3 | The most common type of dementia is Alzheimer’s disease. | * 204 (67.11) | 100 (32.89) |
| 4 | Dementia is curable in most cases. | 16 (5.26) | * 288 (94.74) |
| 5 | Dementia mainly affects people over 60 years old. | * 235 (77.30) | 69 (22.70) |
| 6 | It is possible to develop dementia in middle age. | * 268 (88.16) | 36 (11.84) |
| 7 | There are known factors that increase the risk of developing dementia. | * 248 (81.58) | 56 (18.42) |
| 8 | There are known factors that reduce the risk of developing dementia. | * 246 (80.92) | 58 (19.08) |
| 9 | Communication with a person affected with advanced dementia is impossible. | 85 (27.96) | * 219 (72.04) |
| 10 | People with advanced dementia often communicate through body language. | * 205 (67.43) | 99 (32.57) |
| 11 | When in the company of a person with dementia, you should not address them directly because they will not understand what you are saying. | 23 (7.57) | * 281 (92.43) |
| 12 | The best therapy for dementia is pharmacotherapy. | * 128 (42.11) | 176 (57.89) |
| 13 | People with dementia usually have trouble making decisions. | * 276 (90.79) | 28 (9.21) |
| 14 | The symptoms of dementia occur suddenly. | 38 (12.5) | * 266 (87.50) |
| 15 | All forms of dementia are hereditary. | 12 (3.95) | * 292 (96.05) |
| 16 | The early diagnosis of dementia improves the quality of a patients’ life. | * 286 (94.08) | 18 (5.92) |
| 17 | The number of dementia cases worldwide will decrease in the coming years. | 62 (20.39) | * 242 (79.61) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skowronek, A.; Bojkowska-Otrębska, K.; Łabuz-Roszak, B. Public Knowledge about Dementia in Poland—A Survey Study. J. Clin. Med. 2023, 12, 7675. https://doi.org/10.3390/jcm12247675
Skowronek A, Bojkowska-Otrębska K, Łabuz-Roszak B. Public Knowledge about Dementia in Poland—A Survey Study. Journal of Clinical Medicine. 2023; 12(24):7675. https://doi.org/10.3390/jcm12247675
Chicago/Turabian StyleSkowronek, Alicja, Katarzyna Bojkowska-Otrębska, and Beata Łabuz-Roszak. 2023. "Public Knowledge about Dementia in Poland—A Survey Study" Journal of Clinical Medicine 12, no. 24: 7675. https://doi.org/10.3390/jcm12247675
APA StyleSkowronek, A., Bojkowska-Otrębska, K., & Łabuz-Roszak, B. (2023). Public Knowledge about Dementia in Poland—A Survey Study. Journal of Clinical Medicine, 12(24), 7675. https://doi.org/10.3390/jcm12247675