

Whole-Body Cryotherapy Alters Circulating MicroRNA Profile in Postmenopausal Women

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
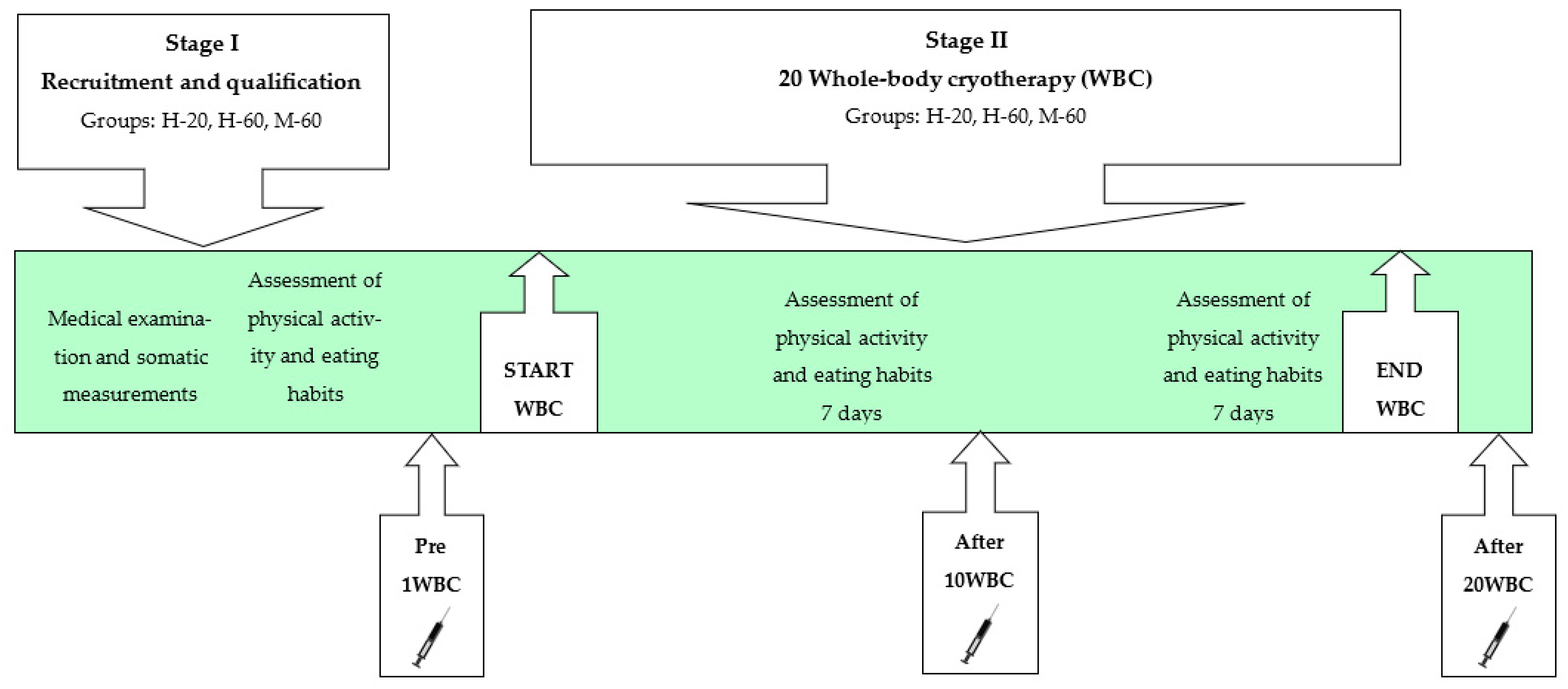
2.1. Study Design
- H-20—young healthy women, n = 19;
- H-60—healthy postmenopausal women, n = 18;
- M-60—postmenopausal women diagnosed with MetS, n = 18.
2.2. Qualification of Participants
2.2.1. Medical Examination
- WC (waist circumference) > 88 cm;
- FBG > 5.6 mmol/L;
- HDL-C < 1.3 mmol/L;
- TG > 1.7 mmol/L;
- SBP ≥ 130 mmHg or DBP ≥ 85 mmHg or antihypertensive therapy [1].
2.2.2. Assessment of Physical Activity and Eating Habits
2.2.3. Participants
2.3. Somatic Measurements and Body Composition Assessment
2.4. Whole-Body Cryotherapy
2.5. Blood Collection
2.6. miRNA Expression Analysis
2.6.1. miRNA Isolation and Quality Control of RNA
2.6.2. Reverse Transcription
2.6.3. Real-Time Quantitative PCR
2.7. Fasting Blood Glucose and Lipid Profile Analysis
2.8. Statistical Analysis
2.9. Bioinformatic Analysis
3. Results
3.1. Characteristics of the Study Participants
3.1.1. Somatic Build
3.1.2. Diagnostics in Metabolic Syndrome
3.1.3. Blood Morphology
3.1.4. Other Metabolic Markers
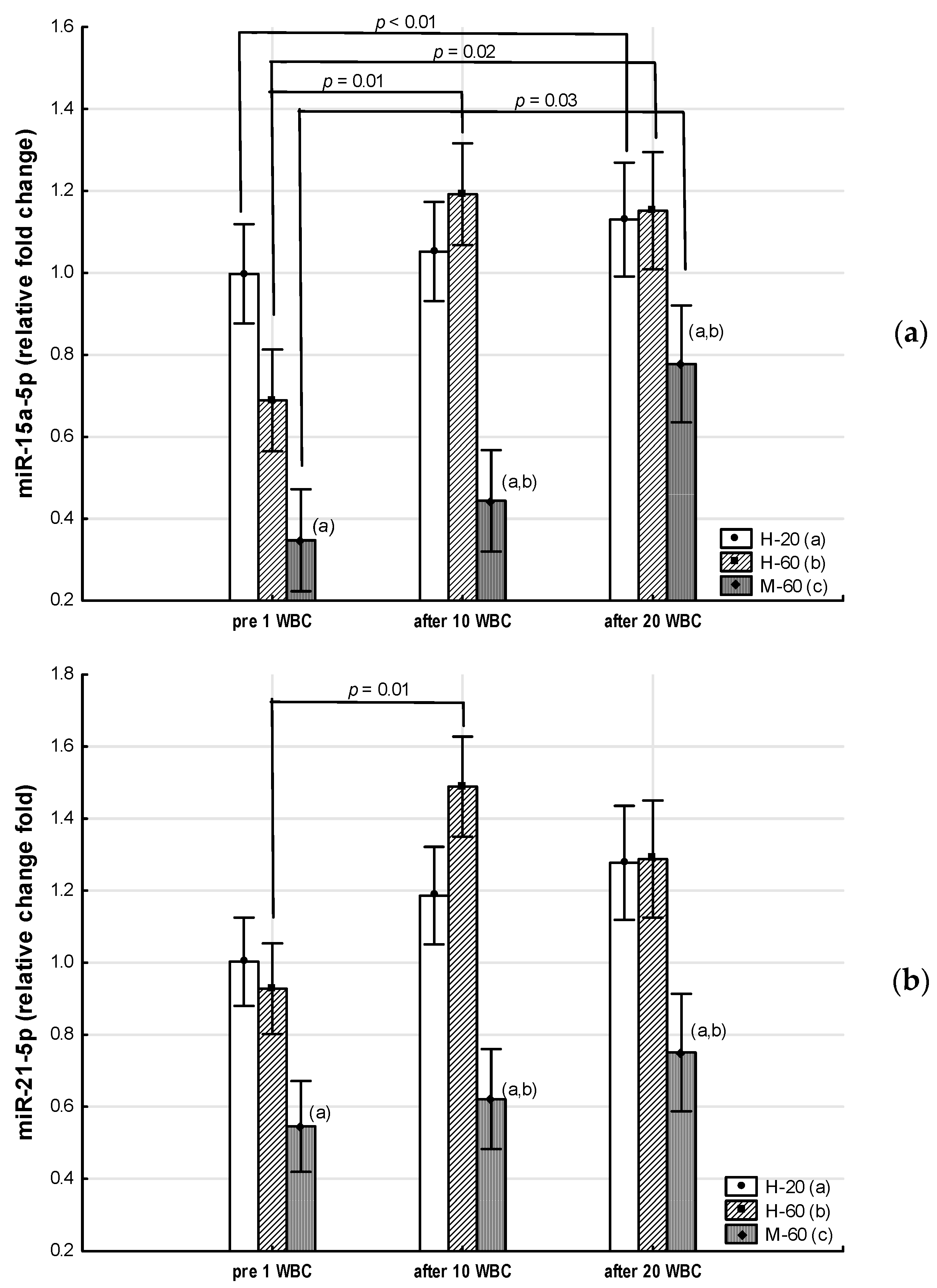
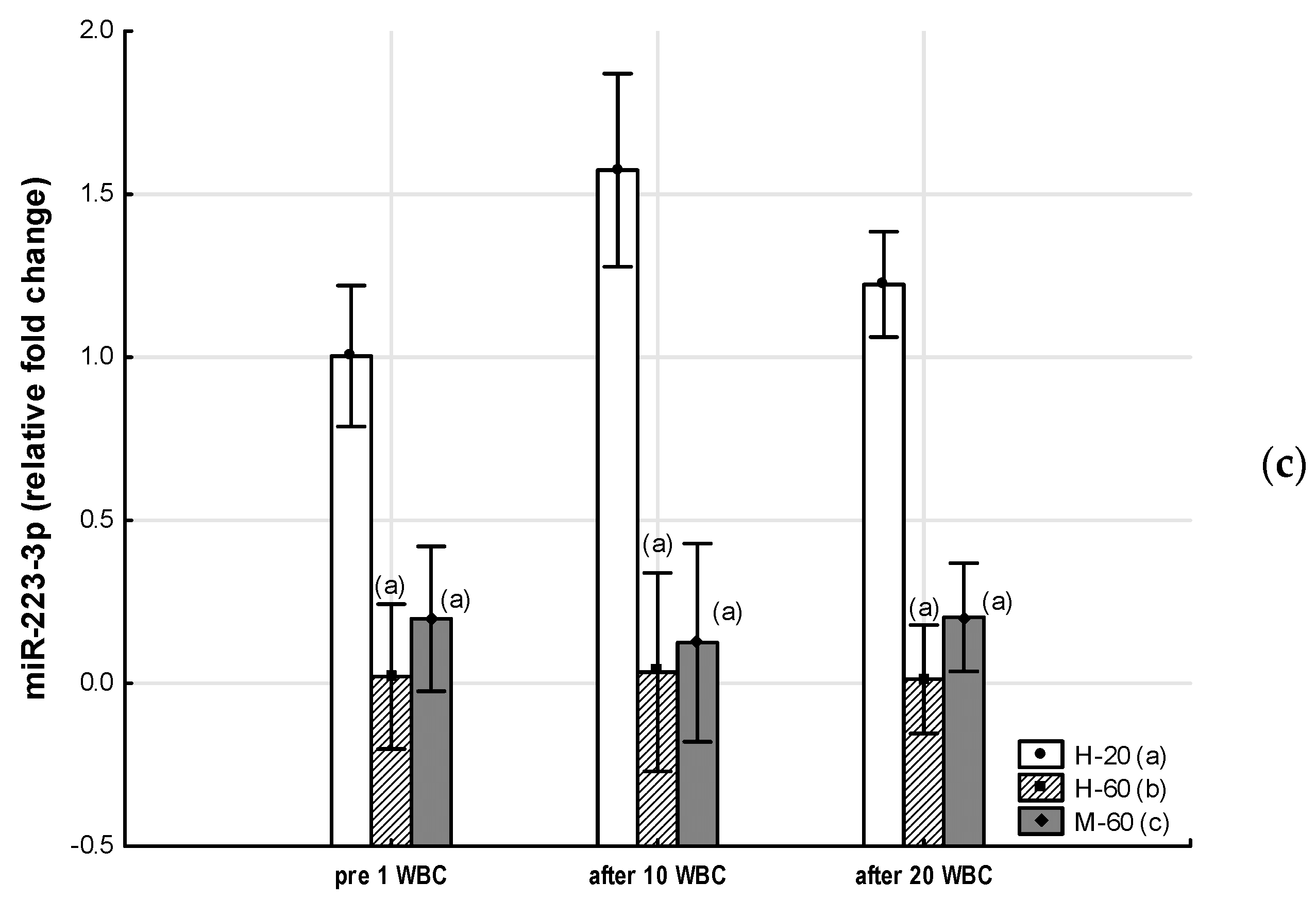
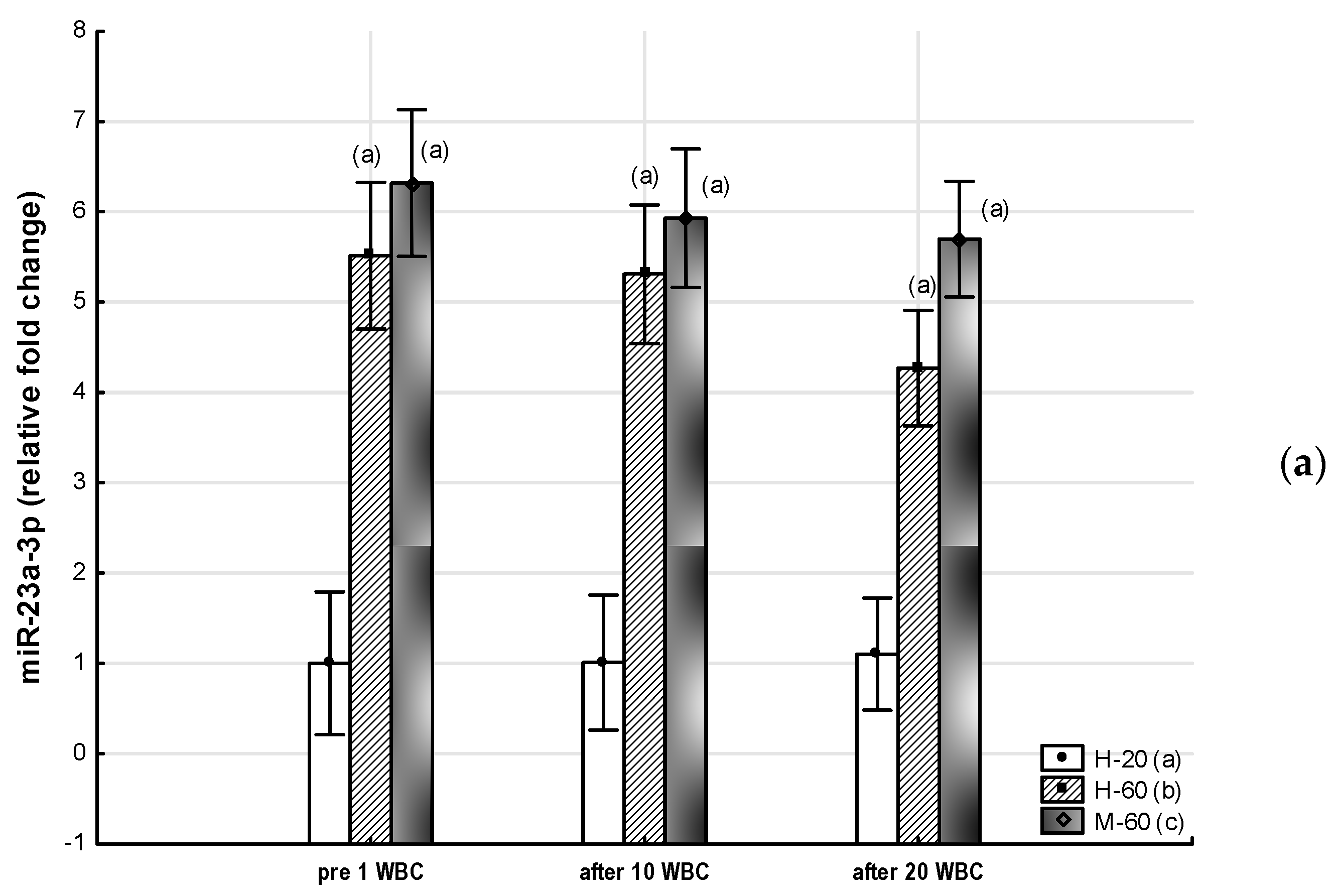
3.2. Expression of Selected miRNAs
3.2.1. Group Comparison
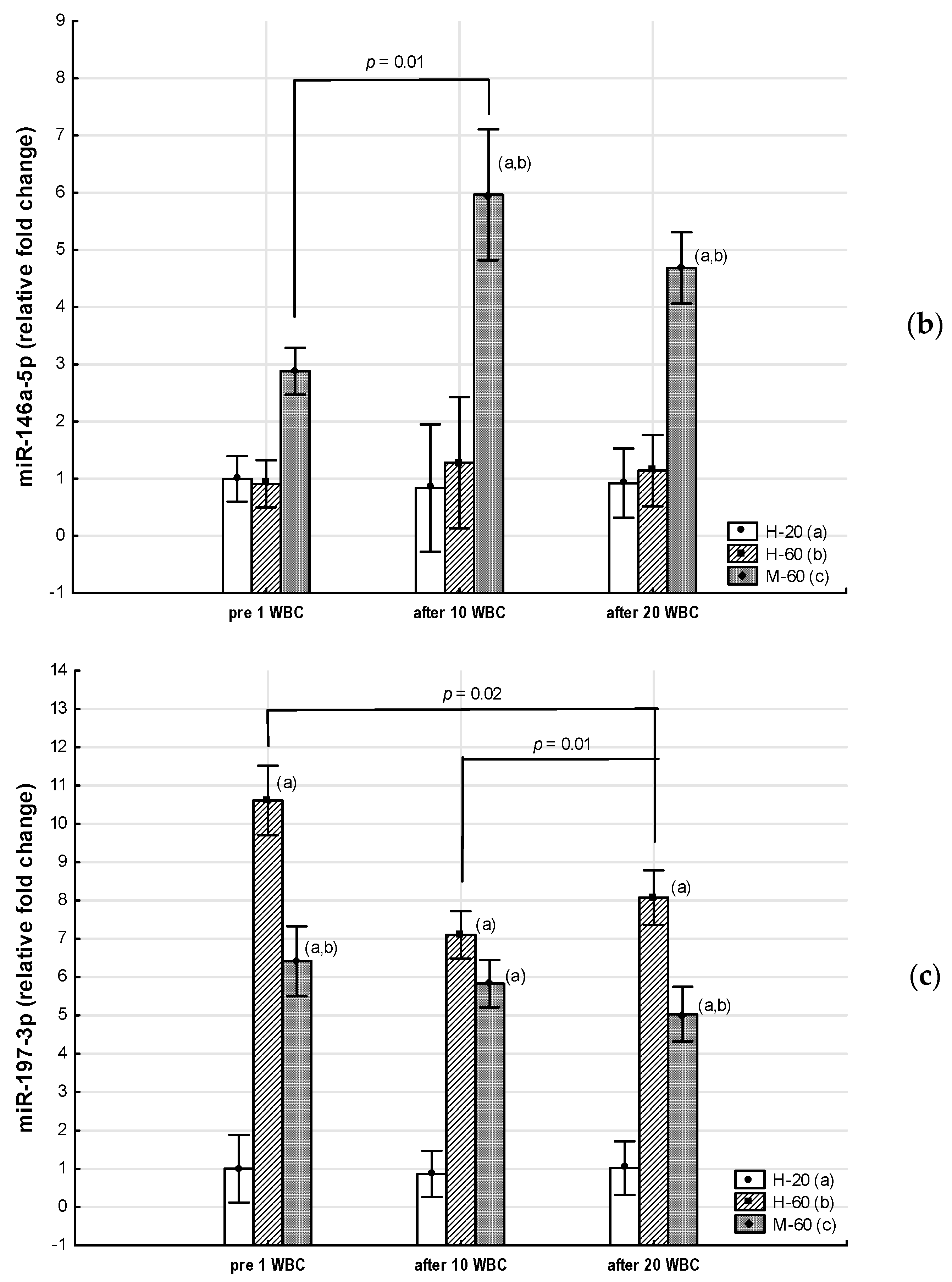
3.2.2. Effects of Whole-Body Cryotherapy
3.2.3. Inter-Group Comparison Regarding Effects of Whole-Body Cryotherapy
3.3. Metabolic Changes
3.3.1. Group Comparison
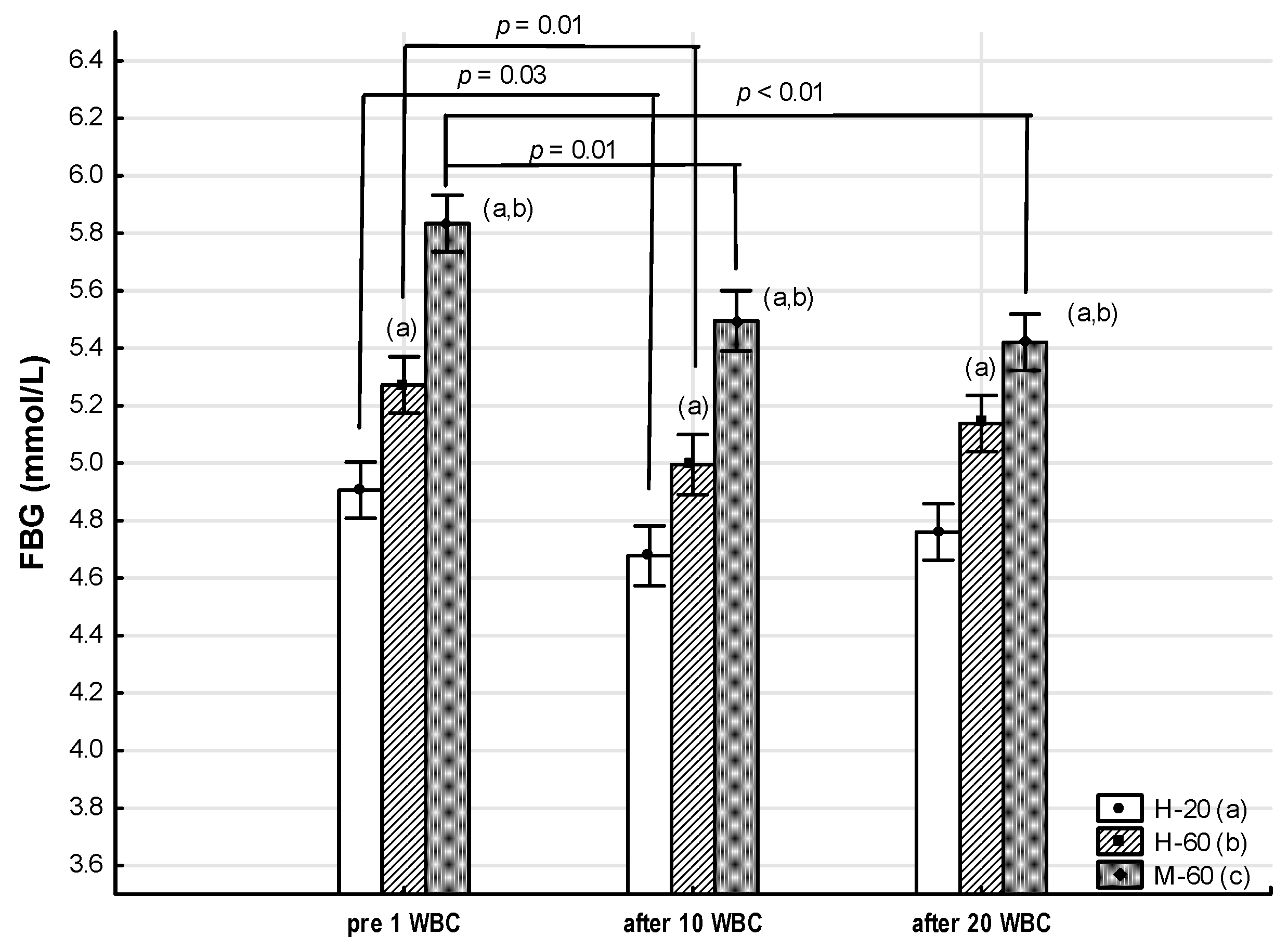
3.3.2. Effects of Whole-Body Cryotherapy
3.3.3. Inter-Group Comparison Regarding Effects of Whole-Body Cryotherapy
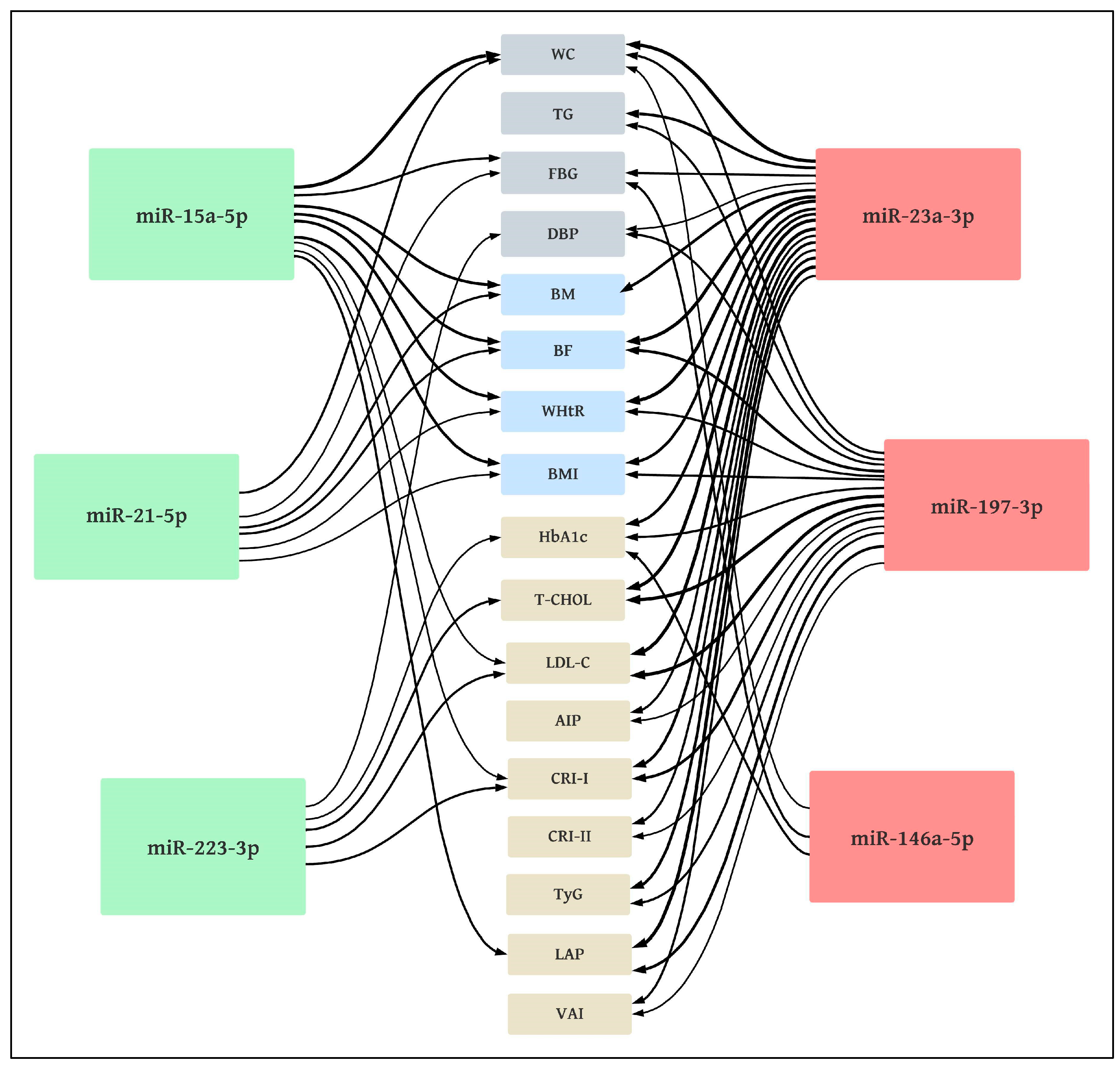
3.4. Correlations between miRNA Expression and Clinically Studied Variables of Metabolic Syndrome as Well as Other Somatic and Metabolic Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Fahed, G.; Aoun, L.; Bou Zerdan, M.; Allam, S.; Bou Zerdan, M.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int. J. Mol. Sci. 2022, 23, 786. [Google Scholar] [CrossRef] [PubMed]
- Vishram, J.K.K.; Borglykke, A.; Andreasen, A.H.; Jeppesen, J.; Ibsen, H.; Jørgensen, T.; Palmieri, L.; Giampaoli, S.; Donfrancesco, C.; Kee, F.; et al. Impact of Age and Gender on the Prevalence and Prognostic Importance of the Metabolic Syndrome and Its Components in Europeans. The MORGAM Prospective Cohort Project. PLoS ONE 2014, 9, e107294. [Google Scholar] [CrossRef] [PubMed]
- Amini, M.; Zayeri, F.; Salehi, M. Trend analysis of cardiovascular disease mortality, incidence, and mortality-to-incidence ratio: Results from global burden of disease study 2017. BMC Public Health 2021, 21, 401. [Google Scholar] [CrossRef]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Kyu, H.H.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- Mathers, C.D.; Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef]
- Starzak, M.; Stanek, A.; Jakubiak, G.K.; Cholewka, A.; Cieślar, G. Arterial Stiffness Assessment by Pulse Wave Velocity in Patients with Metabolic Syndrome and Its Components: Is It a Useful Tool in Clinical Practice? Int. J. Environ. Res. Public Health 2022, 19, 10368. [Google Scholar] [CrossRef]
- Myers, J.; Kokkinos, P.; Nyelin, E. Physical Activity, Cardiorespiratory Fitness, and the Metabolic Syndrome. Nutrients 2019, 11, 1652. [Google Scholar] [CrossRef]
- Kantorowicz, M.; Szymura, J.; Szygula, Z.; Kusmierczyk, J.; Maciejczyk, M.; Wiecek, M. Nordic Walking at Maximal Fat Oxidation Intensity Decreases Circulating Asprosin and Visceral Obesity in Women With Metabolic Disorders. Front. Physiol. 2021, 12, 726783. [Google Scholar] [CrossRef]
- Castro-Barquero, S.; Ruiz-León, A.M.; Sierra-Pérez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [Google Scholar] [CrossRef] [PubMed]
- Stanek, A.; Grygiel-Górniak, B.; Brożyna-Tkaczyk, K.; Myśliński, W.; Cholewka, A.; Zolghadri, S. The Influence of Dietary Interventions on Arterial Stiffness in Overweight and Obese Subjects. Nutrients 2023, 15, 1440. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, G.; Ziemann, E.; Banfi, G. Whole-Body Cryotherapy: Possible Application in Obesity and Diabesity. In Rehabilitation Interventions in the Patient with Obesity; Capodaglio, P., Ed.; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Fontana, J.M.; Bozgeyik, S.; Gobbi, M.; Piterà, P.; Giusti, E.M.; Dugué, B.; Lombardi, G.; Capodaglio, P. Whole-body cryostimulation in obesity. A scoping review. J. Therm. Biol. 2022, 106, 103250. [Google Scholar] [CrossRef] [PubMed]
- van Beek, S.; Hashim, D.; Bengtsson, T.; Hoeks, J. Physiological and molecular mechanisms of cold-induced improvements in glucose homeostasis in humans beyond brown adipose tissue. Int. J. Obes. 2023, 47, 338–347. [Google Scholar] [CrossRef]
- Wiecek, M.; Szymura, J.; Sproull, J.; Szygula, Z. Whole-Body Cryotherapy Is an Effective Method of Reducing Abdominal Obesity in Menopausal Women with Metabolic Syndrome. J. Clin. Med. 2020, 9, 2797. [Google Scholar] [CrossRef]
- Lubkowska, A. Cryotherapy: Physiological considerations and applications to physical therapy. In Physical Therapy Perspectives in the 21st Century—Challenges and Possibilities, 1st ed.; Bettany-Saltikov, J., Ed.; Intech Europe: Rijeka, Croatia, 2012; pp. 155–176. [Google Scholar]
- Szymura, J.; Wiecek, M.; Maciejczyk, M.; Gradek, J.; Kantorowicz, M.; Szygula, Z. Unchanged erythrocyte profile after exposure to cryogenic temperatures in elder marathon runners. Front. Physiol. 2018, 9, 659. [Google Scholar] [CrossRef]
- Lubkowska, A.; Bryczkowska, I.; Szygula, Z.; Giemza, C.; Skrzek, A.; Rotter, I.; Lombardi, G.; Banfi, G. The effect of repeated whole-body cryostimulation on the HSP-70 and lipid metabolisms in healthy subjects. Physiol. Res. 2019, 68, 419–429. [Google Scholar] [CrossRef]
- Dulian, K.; Laskowski, R.; Grzywacz, T.; Kujach, S.; Flis, D.J.; Smaruj, M.; Ziemann, E. The whole body cryostimulation modifies irisin concentration and reduces inflammation in middle aged, obese men. Cryobiology 2015, 71, 398–404. [Google Scholar] [CrossRef]
- Wiecek, M.; Szymura, J.; Sproull, J.; Szygula, Z. Decreased Blood Asprosin in Hyperglycemic Menopausal Women as a Result of Whole-Body Cryotherapy Regardless of Metabolic Syndrome. J. Clin. Med. 2019, 8, 1428. [Google Scholar] [CrossRef]
- Stanek, A.; Romuk, E.; Wielkoszyński, T.; Bartuś, S.; Cieślar, G.; Cholewka, A. Decreased Lipid Profile and Oxidative Stress in Healthy Subjects Who Underwent Whole-Body Cryotherapy in Closed Cryochamber with Subsequent Kinesiotherapy. Oxid. Med. Cell. Longev. 2019, 2019, 7524878. [Google Scholar] [CrossRef]
- Stanek, A.; Wielkoszyński, T.; Bartuś, S.; Cholewka, A. Whole-Body Cryostimulation Improves Inflammatory Endothelium Parameters and Decreases Oxidative Stress in Healthy Subjects. Antioxidants 2020, 9, 1308. [Google Scholar] [CrossRef]
- Agbu, P.; Carthew, R.W. MicroRNA-mediated regulation of glucose and lipid metabolism. Nat. Rev. Mol. Cell Biol. 2021, 22, 425–438. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, J. Circulating MicroRNAs: Potential and Emerging Biomarkers for Diagnosis of Cardiovascular and Cerebrovascular Diseases. BioMed Res. Int. 2015, 2015, 730535. [Google Scholar] [CrossRef]
- Párrizas, M.; Novials, A. Circulating microRNAs as biomarkers for metabolic disease. Best Pract. Res. Clin. Endocrinol. Metab. 2016, 5, 591–601. [Google Scholar] [CrossRef]
- Seeliger, C.; Krauss, T.; Honecker, J.; Mengel, L.A.; Buekens, L.; Mesas-Fernández, A.; Skurk, T.; Claussnitzer, M.; Hauner, H. miR-375 is cold exposure sensitive and drives thermogenesis in visceral adipose tissue derived stem cells. Sci. Rep. 2022, 12, 9557. [Google Scholar] [CrossRef] [PubMed]
- Saliminejad, K.; Khorram Khorshid, H.R.; Soleymani Fard, S.; Ghaffari, S.H. An overview of microRNAs: Biology, functions, therapeutics, and analysis methods. J. Cell Physiol. 2019, 234, 5451–5465. [Google Scholar] [CrossRef]
- He, Y.; Ding, Y.; Liang, B.; Lin, J.; Kim, T.K.; Yu, H.; Wang, K. A Systematic Study of Dysregulated MicroRNA in Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2017, 18, 456. [Google Scholar] [CrossRef]
- Villard, A.; Marchand, L.; Thivolet, C.; Rome, S. Diagnostic Value of Cell-free Circulating MicroRNAs for Obesity and Type 2 Diabetes: A Meta-analysis. J. Mol. Biomark. Diagn. 2015, 6, 251. [Google Scholar] [CrossRef]
- Deiuliis, J. MicroRNAs as regulators of metabolic disease: Pathophysiologic significance and emerging role as biomarkers and therapeutics. Int. J. Obes. 2016, 40, 88–101. [Google Scholar] [CrossRef]
- Ramzan, F.; D’Souza, R.F.; Durainayagam, B.R.; Milan, A.M.; Markworth, J.F.; Miranda-Soberanis, V.; Cameron-Smith, D. Circulatory miRNA biomarkers of metabolic syndrome. Acta Diabetol. 2019, 57, 203–214. [Google Scholar] [CrossRef]
- Karolina, D.S.; Tavintharan, S.; Armugam, A.; Sepramaniam, S.; Pek, S.L.; Wong, M.T.; Lim, S.C.; Sum, C.F.; Jeyaseelan, K. Circulating miRNA Profiles in Patients with Metabolic Syndrome. J. Clin. Endocrinol. Metab. 2012, 97, E2271–E2276. [Google Scholar] [CrossRef]
- Darabi, F.; Aghaei, M.; Movahedian, A.; Elahifar, A.; Pourmoghadas, A.; Sarrafzadegan, N. Association of serum microRNA-21 levels with visfatin, inflammation, and acute coronary syndromes. Heart Vessel. 2017, 32, 549–557. [Google Scholar] [CrossRef]
- Roos, J.; Enlund, E.; Funcke, J.B.; Tews, D.; Holzmann, K.; Debatin, K.M.; Fischer-Posovszky, P. miR-146a-mediated suppression of the inflammatory response in human adipocytes. Sci. Rep. 2016, 6, 38339. [Google Scholar] [CrossRef]
- Wen, D.; Qiao, P.; Wang, L. Circulating microRNA-223 as a potential biomarker for obesity. Obes. Res. Clin. Pract. 2015, 9, 398–404. [Google Scholar] [CrossRef]
- DIANA-miRPath v4.0. Available online: https://diana-lab.e-ce.uth.gr/app/miRPathv4 (accessed on 3 August 2023).
- Sapp, R.M.; Shill, D.D.; Dash, C.; Hicks, J.C.; Adams-Campbell, L.L.; Hagberg, J.M. Circulating microRNAs and endothelial cell migration rate are associated with metabolic syndrome and fitness level in postmenopausal African American women. Physiol. Rep. 2019, 7, e14173. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Bartolini, D.; Mensà, E.; Torquato, P.; Albertini, M.C.; Olivieri, F.; Testa, R.; Rossi, S.; Piroddi, M.; Cruciani, G.; et al. Physical Activity Modulates the Overexpression of the Inflammatory miR-146a-5p in Obese Patients. IUBMB Life 2018, 70, 1012–1022. [Google Scholar] [CrossRef]
- Biernat, E. International Physical Activity Questionnaire—Polish long version. Polish J. Sport. Med. 2013, 1, 1–15. [Google Scholar]
- Dugué, B.; Bernard, J.P.; Bouzigon, R.; De Nardi, M.; Douzi, W.; Feirreira, J.J.; GUILPART, J.; Lombardi, G.; Miller, E.; Tiemessen, I. Whole body cryotherapy/cryostimulation, 39th Informatory Note on Refrigeration Technologies. Int. Inst. Refrig. 2020, 1–9. [Google Scholar] [CrossRef]
- Lubkowska, A.; Szygula, Z. Changes in blood pressure with compensatory heart rate decrease and in the level in aerobic capacity in response to repeated whole-body cryostimulation in normotensive, young and physically active men. Int. J. Occup. Med. Environ. Health 2010, 23, 367–375. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Bawelski, M.; Więcek, M.; Szygula, Z.; Michailov, M.L.; Vadašová, B.; Kačúr, P.; Pałka, T. Acute Effects of Whole-Body Vibration on Resting Metabolic Rate and Substrate Utilisation in Healthy Women. Biology 2022, 11, 655. [Google Scholar] [CrossRef]
- Piotrowska, A.M.; Bigosińska, M.; Potok, H.; Cisoń-Apanasewicz, U.; Czerwińska-Ledwig, O.; Tota, Ł.M.; Zuziak, R.; Pałka, T.; Pilch, W. Impact of oscillatory-cycloid vibration interventions on body composition, waist and hip circumference, and blood lipid profile in women aged over 65 years with hypercholesterolaemia. Menopause Rev. 2018, 17, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, J.A.; Laukkanen, T.; Kunutsor, S.K. Cardiovascular and Other Health Benefits of Sauna Bathing: A Review of the Evidence. Mayo Clin. Proc. 2018, 93, 1111–1121. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Huan, M.T.; Sang, J.J.; Luo, S.S.; Kong, X.T.; Xie, Z.Y.; Zheng, S.H.; Wei, Q.B.; Wu, Y.C. Clinical Effect of Abdominal Massage Therapy on Blood Glucose and Intestinal Microbiota in Patients with Type 2 Diabetes. Oxid. Med. Cell. Longev. 2022, 2022, 2286598. [Google Scholar] [CrossRef]
- Szponar, L.; Wolnicka, K.; Rychli, E. Album of Photographs of Food Products and Dishes; National Food and Nutrition Institute: Warsaw, Poland, 2000. [Google Scholar]
- Jarosz, M.; Rychlik, E.; Stoś, K.; Charzewska, J. Nutrition Standards for the Polish Population and Their Application, 1st ed.; National Institute of Public Health—National Institute of Hygiene: Warsaw, Poland, 2020. [Google Scholar]
- National Health Fund. Available online: https://www.nfz.gov.pl/zarzadzenia-prezesa/zarzadzenia-prezesa-nfz/zarzadzenie-nr-132019dsoz,6878.html (accessed on 29 May 2023).
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 4, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Bovolini, A.; Garcia, J.; Andrade, M.A.; Duarte, J.A. Metabolic Syndrome Pathophysiology and Predisposing Factors. Int. J. Sports Med. 2021, 42, 199–214. [Google Scholar] [CrossRef]
- Kim, J.E.; Kim, J.S.; Jo, M.J.; Cho, E.; Ahn, S.Y.; Kwon, Y.J.; Ko, G.J. The Roles and Associated Mechanisms of Adipokines in Development of Metabolic Syndrome. Molecules 2022, 27, 334. [Google Scholar] [CrossRef] [PubMed]
- Arhire, L.I.; Mihalache, L.; Covasa, M. Irisin: A Hope in Understanding and Managing Obesity and Metabolic Syndrome. Front. Endocrinol. 2019, 10, 524. [Google Scholar] [CrossRef]
- Goguet-Rubio, P.; Klug, R.L.; Sharma, D.L.; Srikanthan, K.; Puri, N.; Lakhani, V.H.; Nichols, A.; O’Hanlon, K.M.; Abraham, N.G.; Shapiro, J.I.; et al. Existence of a Strong Correlation of Biomarkers and miRNA in Females with Metabolic Syndrome and Obesity in a Population of West Virginia. Int. J. Med. Sci. 2017, 14, 543–553. [Google Scholar] [CrossRef]
- Flowers, E.; Gadgil, M.; Aouizerat, B.E.; Kanaya, A.M. Circulating micrornas associated with glycemic impairment and progression in Asian Indians. Biomark. Res. 2015, 3, 22. [Google Scholar] [CrossRef][Green Version]
- Heyn, G.S.; Corrêa, L.H.; Magalhães, K.G. The Impact of Adipose Tissue-Derived miRNAs in Metabolic Syndrome, Obesity, and Cancer. Front. Endocrinol. 2020, 11, 563816. [Google Scholar] [CrossRef]
- Al-Rawaf, H.A. Circulating microRNAs and adipokines as markers of metabolic syndrome in adolescents with obesity. Clin. Nutr. 2019, 38, 2231–2238. [Google Scholar] [CrossRef]
- Kamalden, T.A.; Macgregor-Das, A.M.; Kannan, S.M.; Dunkerly-Eyring, B.; Khaliddin, N.; Xu, Z.; Fusco, A.P.; Abu Yazib, S.; Chow, R.C.; Duh, E.J.; et al. Exosomal MicroRNA-15a Transfer from the Pancreas Augments Diabetic Complications by Inducing Oxidative Stress. Antioxid. Redox Signal. 2017, 27, 913–930. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Sanchez, A.; Rutter, G.A.; Latreille, M. miRNAs in β-cell development, identity, and disease. Front. Genet. 2017, 7, 226. [Google Scholar] [CrossRef]
- Sun, L.L.; Jiang, B.G.; Li, W.T.; Zou, J.J.; Shi, Y.Q.; Liu, Z.M. MicroRNA-15a positively regulates insulin synthesis by inhibiting uncoupli1ng protein-2 expression. Diabetes Res. Clin. Pract. 2011, 91, 94–100. [Google Scholar] [CrossRef]
- Rawal, S.; Munasinghe, P.E.; Nagesh, P.T.; Lew, J.K.S.; Jones, G.T.; Williams, M.J.A.; Davis, P.; Bunton, D.; Galvin, I.F.; Manning, P.; et al. Down-regulation of miR-15a/b accelerates fibrotic remodelling in the Type 2 diabetic human and mouse heart. Clin. Sci. 2017, 131, 847–863. [Google Scholar] [CrossRef]
- Corrêa, M.M.; Thumé, E.; De Oliveira, E.R.; Tomasi, E. Performance of the waist-to-height ratio in identifying obesity and predicting non-communicable diseases in the elderly population: A systematic literature review. Arch. Gerontol. Geriatr. 2016, 65, 174–182. [Google Scholar] [CrossRef]
- Brończyk-Puzoń, A.; Koszowska, A.; Bieniek, J. Basic anthropometric measurements and derived ratios in dietary counseling: Part one. Nurs. Public. Health 2018, 8, 217–222. [Google Scholar] [CrossRef][Green Version]
- Balasubramanyam, M.; Aravind, S.; Gokulakrishnan, K.; Prabu, P.; Sathishkumar, C.; Ranjani, H.; Mohan, V. Impaired miR-146a expression links subclinical inflammation and insulin resistance in Type 2 diabetes. Mol. Cell. Biochem. 2011, 351, 197–205. [Google Scholar] [CrossRef]
- Ghaffari, M.; Razi, S.; Zalpoor, H.; Nabi-Afjadi, M.; Mohebichamkhorami, F.; Zali, H. Association of MicroRNA-146a with Type 1 and 2 Diabetes and their Related Complications. J. Diabetes Res. 2023, 2023, 2587104. [Google Scholar] [CrossRef]
- Opoku, A.A.; Abushama, M.; Konje, J.C. Obesity and menopause. Best Pract. Res. Clin. Obstet. Gynaecol. 2023, 88, 102348. [Google Scholar] [CrossRef] [PubMed]
- Ho, P.T.B.; Clark, I.M.; Le, L.T.T. MicroRNA-Based Diagnosis and Therapy. Int. J. Mol. Sci. 2022, 23, 7167. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Signaling Pathway | miRNA Names (Number of Target Genes) |
|---|---|
| FoxO signaling pathway | miR-15a-5p (31), miR-21-5p (25), miR-23a-3p (24), miR-223-3p (7) |
| EGFR tyrosine kinase inhibitor resistance | miR-21-5p (14), miR-23a-3p (17), miR-223-3p (6) |
| MAPK signaling pathway | miR-15a-5p (59), miR-21-5p (39), miR-146a-5p (64) |
| AMPK signaling pathway | miR-15a-5p (26), miR-23a-3p (22), miR-223-3p (6) |
| Rap1 signaling pathway | miR-15a-5p (41), miR-23a-3p (33), miR-146a-5p (44) |
| PI3K-Akt signaling pathway | miR-15a-5p (60), miR-23a-3p (50), miR-223-3p (8) |
| HIF-1 signaling pathway | miR-23a-3p (22), miR-223-3p (5) |
| Fluid shear stress and atherosclerosis | miR-15a-5p (28), miR-23a-3p (25), miR-223-3p (4) |
| mTOR signaling pathway | miR-23a-3p (26), miR-223-3p (6) |
| cGMP-PKG signaling pathway | miR-197-3p (18) |
| IL-17 signaling pathway | miR-146a-5p (28) |
| Insulin signaling pathway | miR-15a-5p (29), miR-23a-3p (24) |
| Insulin resistance | miR-23a-3p (20), miR-223-3p 95) |
| AGE-RAGE signaling pathway in diabetic complications | miR-21-5p (18), miR-223-3p (4) |
| Glucagon signaling pathway | miR-15a-5p (23) |
| Fatty acid metabolism | miR-15a-5p (16) |
| TGF-beta signaling pathway | miR-15a-5p (24) |
| Th17 cell differentiation | miR-223-3p (5) |
| Thermogenesis | miR-146a-5p (49) |
| T cell receptor signaling pathway | miR-223-3p (4) |
| Aldosterone-regulated sodium reabsorption | miR-23a-3p (9) |
| NF-kappa B signaling pathway | miR-146a-5p (6) |
| Variable | H-20 | H-60 | M-60 | Statistical Analysis p | ||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (1–2) | (1–3) | (2–3) | |
| BM (kg) | 65.00 ± 9.20 | 66.32 ± 6.23 | 77.73 ± 12.18 | 0.61 | <0.01 | <0.01 |
| BH (cm) | 168.57 ± 5.93 | 161.39 ± 6.02 | 160.61 ± 7.37 | <0.01 | <0.01 | 0.73 |
| WHtR | 0.46 ± 0.05 | 0.52 ± 0.04 | 0.59 ± 0.06 | <0.01 | <0.01 | <0.01 |
| BF (%) | 27.21 ± 5.32 | 34.14 ± 3.59 | 38.71 ± 4.34 | <0.01 | <0.01 | <0.01 |
| LBM (kg) | 46.92 ± 3.99 | 43.57 ± 3.51 | 47.29 ± 5.47 | 0.01 | 0.82 | 0.02 |
| BMI (kg/m2) | 22.90 ± 3.19 | 25.57 ± 2.46 | 30.56 ± 5.38 | 0.01 | <0.01 | <0.01 |
| Obesity classification (BMI) | n (%) | n (%) | n (%) | |||
| underweight (<18.5) | 1 (5.3) | 0 (0) | 0 (0) | |||
| normal weight (18.5–24.9) | 13 (68.4) | 7 (38.9) | 1 (5.6) | |||
| overweight (25.0–29.9) | 5 (26.3) | 11 (61.1) | 9 (50.0) | |||
| obesity class I (30.0–34.9) | 0 (0) | 0 (0) | 5 (27.8) | |||
| obesity class II (35.00–39.9) | 0 (0) | 0 (0) | 1 (5.6) | |||
| obesity class III (>40.0) | 0 (0) | 0 (0) | 2 (11.0) | |||
| Variable | H-20 | H-60 | M-60 | Statistical Analysis p | ||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (1–2) | (1–3) | (2–3) | |
| MetS Criteria (NCEP—ATP III) | ||||||
| WC (cm) | 69.88 ± 24.25 | 83.37 ± 4.92 | 93.77 ± 8.36 | 0.01 | <0.01 | <0.01 |
| TG (mmol/L) | 0.94 ± 0.33 | 1.23 ± 0.43 | 1.61 ± 0.71 | 0.01 | 0.01 | 0.02 |
| HDL-C (mmol/L) | 1.71 ± 0.37 | 1.66 ± 0.41 | 1.47 ± 0.34 | 0.69 | 0.04 | 0.13 |
| FBG (mmol/L) | 4.94 ± 0.43 | 5.27 ± 0.39 | 5.83 ± 0.45 | 0.02 | <0.01 | <0.01 |
| SBP (mmHg) | 113.68 ± 12.68 | 120.17 ± 16.78 | 125.83 ± 15.83 | 0.20 | 0.02 | 0.30 |
| DBP (mmHg) | 70.53 ± 8.48 | 77.83 ± 7.69 | 81.67 ± 6.86 | 0.02 | <0.01 | 0.12 |
| H-20 | H-60 | M-60 | ||
|---|---|---|---|---|
| MetS Diagnostics acc. NCEP—ATP III | MetS Criterion | n (%) | n (%) | n (%) |
| WC (cm) | >88 | 2 (10.5) | 3 (16.7) | 16 (88.9) |
| TG (mmol/L) | >1.7 | 1 (5.3) | 3 (16.7) | 5 (27.8) |
| HDL-C (mmol/L) | <1.3 | 4 (21.1) | 2 (11.1) | 8 (44.4) |
| FBG (mmol/L) | >5.6 | 1 (5.3) | 3 (16.7) | 15 (83.3) |
| SBP (mmHg) | ≥130 | 2 (10.5) | 6 (33.3) | 9 (50.0) |
| DBP (mmHg) | ≥85 | no one | 4 (22.2) | 7 (38.9) |
| Number of fulfilled MetS criteria | 0 | 12 (63.2) | 4 (22.2) | no one |
| 1 | 4 (21.1) | 10 (55.6) | no one | |
| 2 | 3 (15.8) | 4 (22.2) | no one | |
| 3 | no one | no one | 12 (66.7) | |
| 4 | no one | no one | 6 (33.3) | |
| 5 | no one | no one | no one |
| Variable | H-20 | H-60 | M-60 | Statistical Analysis p | ||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (1–2) | (1–3) | (2–3) | |
| Blood Count | ||||||
| RBC (106/µL) | 4.46 ± 0.24 | 4.59 ± 0.24 | 4.62 ± 0.22 | 0.22 | 0.04 | 0.78 |
| HGB (g/dL) | 13.23 ± 0.76 | 13.94 ± 0.55 | 13.93 ± 0.54 | <0.01 | <0.01 | 0.98 |
| HCT (%) | 38.29 ± 1.80 | 41.14 ± 1.62 | 40.92 ± 1.74 | <0.01 | <0.01 | 0.69 |
| PLT (103/µL) | 253.0 ± 43.3 | 254.9 ± 56.6 | 247.3 ± 79.9 | 0.91 | 0.79 | 0.75 |
| LEUC (103/µL) | 5.96 ± 1.10 | 5.29 ± 1.06 | 6.16 ± 1.29 | 0.07 | 0.61 | 0.03 |
| NEUT (%) | 49.10 ± 7.63 | 48.36 ± 7.10 | 50.03 ± 7.67 | 0.76 | 0.71 | 0.50 |
| LYMPH (%) | 38.16 ± 6.84 | 37.56 ± 6.60 | 37.89 ± 7.59 | 0.79 | 0.91 | 0.89 |
| MONO (%) | 10.03 ± 2.24 | 9.66 ± 2.07 | 8.13 ± 1.61 | 0.58 | 0.01 | 0.06 |
| EOS (%) | 2.05 ± 1.27 | 3.59 ± 1.77 | 3.17 ± 1.58 | <0.01 | <0.01 | 0.41 |
| BASO (%) | 0.66 ± 0.37 | 0.84 ± 0.59 | 0.69 ± 0.40 | 0.24 | 0.35 | 0.67 |
| Variable | H-20 | H-60 | M-60 | Statistical Analysis p | ||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (1–2) | (1–3) | (2–3) | |
| Other Metabolic Markers | ||||||
| HbA1c (%) | 5.15 ± 0.32 | 5.65 ± 0.29 | 5.83 ± 0.28 | <0.01 | <0.01 | 0.04 |
| T-CHOL (mmol/L) | 4.14 ± 0.81 | 5.78 ± 0.92 | 5.52 ± 1.00 | <0.01 | <0.01 | 0.42 |
| LDL-C (mmol/L) | 2.00 ± 0.65 | 3.56 ± 0.90 | 3.32 ± 0.98 | <0.01 | <0.01 | 0.45 |
| AIP (log10TG/HDL-C) | −0.27 ± 0.20 | −0.14 ± 0.20 | 0.02 ± 0.23 | 0.04 | <0.01 | 0.04 |
| CRI-I (T-CHOL/HDL-C) | 2.48 ± 0.51 | 3.65 ± 0.92 | 3.92 ± 0.97 | <0.01 | <0.01 | 0.40 |
| CRI-II (LDL-C/HDL-C) | 0.60 ± 0.33 | 0.80 ± 0.37 | 1.20 ± 0.75 | 0.03 | <0.01 | 0.04 |
| TyG (lnTG × FBG/2) | 8.16 ± 0.31 | 8.50 ± 0.30 | 8.85 ± 0.41 | <0.01 | <0.01 | 0.01 |
| LAP (WC-58) × TG | 18.36 ± 8.16 | 31.04 ± 11.14 | 57.24 ± 26.43 | <0.01 | <0.01 | <0.01 |
| VAI | 1.09 ± 0.61 | 1.47 ± 0.66 | 2.24 ± 1.29 | 0.08 | <0.01 | 0.03 |
| Mean ± SD | ANOVA | Mean (95% CI) | Post hoc | Mean (95% CI) | Post hoc | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable (Relative Fold Change) | Group | (1) Pre 1 WBC | (2) After 10 WBCs | (3) After 20 WBCs | Group | WBC | Group × WBC | (2-1) Δ10 WBCs | p | (3-1) Δ20 WBCs | p | |
| H-20 (a) | 1.00 ± 0.74 | 1.05 ± 0.79 | 1.13 ± 0.73 | p | <0.01 | 0.01 | 0.32 | 0.05 (−0.47; 0.57) | 0.77 | 0.13 (−0.40; 0.67) * | <0.01 | |
| miR-15a-5p | H-60 (b) | 0.69 ± 0.50 | 1.19 ± 0.40 | 1.15 ± 0.43 | F | 19.47 | 4.88 | 1.18 | 0.50 (0.17; 0.83) * | 0.01 | 0.46 (0.09; 0.83) * | 0.02 |
| M-60 (c) | 0.35 ± 0.16 a | 0.44 ± 0.16 ab | 0.78 ± 0.61 ab | η2 | 0.43 | 0.09 | 0.04 | 0.10 (0.00; 0.19) | 0.62 | 0.43 (0.14; 0.72) * | 0.03 | |
| H-20 (a) | 1.00 ± 0.62 | 1.19 ± 0.85 | 1.28 ± 0.78 | p | <0.01 | 0.04 | 0.58 | 0.18 (−0.33; 0.69) | 0.39 | 0.27 (−0.30; 0.85) | 0.20 | |
| miR-21-5p | H-60 (b) | 0.93 ± 0.64 | 1.49 ± 0.48 | 1.29 ± 0.61 | F | 23.54 | 3.23 | 0.72 | 0.56 (0.09; 1.03) * | 0.01 | 0.36 (−0.11; 0.83) | 0.10 |
| M-60 (c) | 0.55 ± 0.25 a | 0.62 ± 0.27 ab | 0.75 ± 0.66 ab | η2 | 0.48 | 0.06 | 0.03 | 0.08 (−0.07; 0.22) | 0.73 | 0.21 (−0.15; 0.57) | 0.35 | |
| H-20 (a) | 1.00 ± 0.63 | 1.01 ± 0.70 | 1.10 ± 1.03 | p | <0.01 | 0.56 | 0.87 | 0.01 (−0.49; 0.51) | 0.99 | 0.11 (−0.40; 0.61) | 0.91 | |
| miR-23a-3p | H-60 (b) | 5.51 ± 5.27 a | 5.31 ± 4.78 a | 4.27 ± 4.11 a | F | 29.91 | 0.58 | 0.30 | −0.21 (−4.11; 3.69) | 0.83 | −1.28 (−4.72; 2.16) | 0.20 |
| M-60 (c) | 6.32 ± 2.85 a | 5.93 ± 3.01 a | 5.70 ± 2.12 a | η2 | 0.53 | 0.01 | 0.01 | −0.40 (−1.75; 0.94) | 0.69 | −0.64 (−2.50; 1.22) | 0.52 | |
| H-20 (a) | 1.00 ± 1.45 | 0.84 ± 0.77 | 0.92 ± 1.00 | p | <0.01 | 0.24 | 0.31 | −0.13 (−0.62; 0.36) | 0.89 | −0.06 (−0.82; 0.70) | 0.95 | |
| miR-146a-5p | H-60 (b) | 0.91 ± 1.21 | 1.28 ± 0.99 | 1.14 ± 2.62 | F | 20.80 | 1.46 | 1.21 | 0.30 (−0.35; 0.94) | 0.74 | 0.18 (−0.95; 1.32) | 0.84 |
| M-60 (c) | 2.88 ± 2.37 | 5.96 ± 8.42 ab | 4.68 ± 3.67 ab | η2 | 0.44 | 0.03 | 0.04 | 2.47 (−0.81; 5.75) * | 0.01 | 1.45 (−0.25; 3.14) | 0.11 | |
| H-20 (a) | 1.00 ± 0.47 | 0.87 ± 0.35 | 1.02 ± 0.58 | p | <0.01 | 0.04 | 0.14 | −0.15 (−0.50; 0.19) | 0.89 | 0.02 (−0.42; 0.46) | 0.99 | |
| miR-197-3p | H-60 (b) | 10.61 ± 5.72 a | 7.10 ± 3.66 a | 8.07 ± 4.89 a | F | 74.47 | 3.42 | 1.78 | −4.00 (−7.53; −0.48) * | 0.01 | −2.90 (−7.16;1.37) * | 0.02 |
| M-60 (c) | 6.41 ± 3.53 ab | 5.82 ± 2.77 a | 5.03 ± 1.95 ab | η2 | 0.74 | 0.06 | 0.06 | −0.67 (−2.81; 1.47) | 0.58 | −1.58 (−3.97; 0.82) | 0.19 | |
| H-20 (a) | 1.00 ± 1.58 | 1.57 ± 2.19 | 1.22 ± 1.18 | p | <0.01 | 0.67 | 0.68 | 0.29 (−0.41; 1.00) | 0.08 | 0.11 (−0.35; 0.57) | 0.50 | |
| miR-223-3p | H-60 (b) | 0.02 ± 0.03 a | 0.03 ± 0.04 a | 0.01 ± 0.01 a | F | 25.29 | 0.39 | 0.58 | 0.01 (−0.01; 0.02) | 0.97 | 0.00 (−0.01; 0.01) | 0.98 |
| M-60 (c) | 0.20 ± 0.25 a | 0.12 ± 0.12 a | 0.20 ± 0.24 a | η2 | 0.49 | 0.01 | 0.02 | −0.04 (−0.10; 0.03) | 0.83 | 0.00 (−0.08; 0.09) | 0.99 | |
| Mean ± SD | ANOVA | Mean (95% CI) | Post hoc | Mean (95% CI) | Post hoc | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Group | (1) Pre 1 WBC | (2) After 10 WBCs | (3) After 20 WBCs | Group | WBC | Group × WBC | (2-1) Δ10 WBCs | p | (3-1) Δ20 WBCs | p | |
| H-20 (a) | 4.94 ± 0.43 | 4.68 ± 0.38 | 4.77 ± 0.40 | p | <0.01 | <0.01 | 0.27 | −0.23 (−0.40; −0.06) * | 0.03 | −0.17 (−0.43; 0.08) | 0.16 | |
| FBG | H-60 (b) | 5.27 ± 0.39 a | 5.00 ± 0.30 a | 5.14 ± 0.39 a | F | 24.40 | 13.06 | 1.31 | −0.28 (−0.46; −0.09) * | 0.01 | −0.13 (−0.24; −0.03) | 0.19 |
| (mmol/L) | M-60 (c) | 5.83 ± 0.45 ab | 5.50 ± 0.59 ab | 5.42 ± 0.45 ab | η2 | 0.49 | 0.20 | 0.05 | −0.34 (−0.62; −0.06) * | 0.01 | −0.41 (−0.70; −0.13) * | <0.01 |
| H-20 (a) | 4.14 ± 0.81 | 4.01 ± 0.85 | 4.02 ± 0.62 | p | <0.01 | 0.27 | 0.85 | −0.12 (−0.27; 0.04) | 0.38 | −0.15 (−0.36; 0.05) | 0.30 | |
| T-CHOL | H-60 (b) | 5.78 ± 0.92 a | 5.69 ± 0.90 a | 5.65 ± 1.16 a | F | 16.60 | 1.34 | 0.34 | −0.09 (−0.28; 0.11) | 0.44 | −0.13 (−0.40; 0.14) | 0.25 |
| (mmol/L) | M-60 (c) | 5.52 ± 1.00 a | 5.58 ± 0.99 a | 5.45 ± 1.08 a | η2 | 0.40 | 0.03 | 0.01 | 0.06 (−0.15; 0.27) | 0.58 | −0.07 (−0.41; 0.28) | 0.54 |
| H-20 (a) | 2.00 ± 0.65 | 1.95 ± 0.73 | 1.98 ± 0.53 | p | <0.01 | 0.64 | 0.64 | −0.03 (−0.18; 0.12) | 0.75 | −0.06 (−0.18; 0.07) | 0.73 | |
| LDL-C | H-60 (b) | 3.56 ± 0.90 a | 3.45 ± 0.89 a | 3.41 ± 1.09 a | F | 16.06 | 0.44 | 0.64 | −0.11 (−0.32; 0.10) | 0.30 | −0.14 (−0.40; 0.12) | 0.17 |
| (mmol/L) | M-60 (c) | 3.32 ± 0.98 a | 3.43 ± 0.99 a | 3.34 ± 1.03 a | η2 | 0.39 | 0.01 | 0.02 | 0.11 (−0.09; 0.31) | 0.30 | 0.02 (−0.30; 0.34) | 0.86 |
| H-20 (a) | 1.71 ± 0.37 | 1.69 ± 0.42 | 1.66 ± 0.36 | p | 0.13 | 0.60 | 0.78 | −0.03 (−0.11; 0.06) | 0.79 | −0.04 (−0.14; 0.06) | 0.42 | |
| HDL-C | H-60 (b) | 1.66 ± 0.41 | 1.70 ± 0.43 | 1.69 ± 0.45 | F | 2.14 | 0.52 | 0.44 | 0.04 (−0.04; 0.11) | 0.36 | 0.03 (−0.09; 0.15) | 0.45 |
| (mmol/L) | M-60 (c) | 1.47 ± 0.34 a | 1.48 ± 0.31 | 1.44 ± 0.33 | η2 | 0.08 | 0.01 | 0.02 | 0.02 (−0.05; 0.08) | 0.70 | −0.03 (−0.10; 0.04) | 0.50 |
| H-20 (a) | 0.94 ± 0.33 | 0.82 ± 0.18 | 0.84 ± 0.19 | p | <0.01 | 0.24 | 0.96 | −0.12 (−0.29; 0.05) | 0.27 | −0.11 (−0.25; 0.03) | 0.34 | |
| TG | H-60 (b) | 1.23 ± 0.43 a | 1.20 ± 0.59 a | 1.19 ± 0.51 a | F | 12.32 | 1.46 | 0.16 | −0.03 (−0.26; 0.20) | 0.77 | −0.04 (−0.35; 0.27) | 0.74 |
| (mmol/L) | M-60 (c) | 1.61 ± 0.71 ab | 1.48 ± 0.51 a | 1.48 ± 0.45 a | η2 | 0.33 | 0.03 | 0.01 | −0.13 (−0.43; 0.16) | 0.22 | −0.13 (−0.40; 0.14) | 0.24 |
| H-20 (a) | −0.27 ± 0.20 | −0.31 ± 0.16 | −0.30 ± 0.14 | p | <0.01 | 0.26 | 0.99 | −0.04 (−0.13; 0.05) | 0.31 | −0.03 (−0.10; 0.03) | 0.44 | |
| AIP | H-60 (b) | −0.14 ± 0.20 | −0.17 ± 0.22 | −0.17 ± 0.25 | F | 10.65 | 1.37 | 0.03 | −0.03 (−0.10; 0.04) | 0.43 | −0.03 (−0.16; 0.10) | 0.47 |
| M-60 (c) | 0.02 ± 0.23 ab | −0.02 ± 0.22 ab | 0.00 ± 0.23 ab | η2 | 0.30 | 0.03 | <0.01 | −0.04 (−0.12; 0.04) | 0.34 | −0.02 (−0.09; 0.05) | 0.63 | |
| H-20 (a) | 8.16 ± 0.31 | 8.02 ± 0.23 | 8.04 ± 0.26 | p | <0.01 | 0.01 | 0.98 | −0.16 (−0.35; 0.03) | 0.07 | −0.13 (−0.26; 0.00) | 0.10 | |
| TyG | H-60 (b) | 8.50 ± 0.30 a | 8.40 ± 0.37 a | 8.42 ± 0.37 a | F | 22.11 | 5.18 | 0.09 | −0.11 (−0.24; 0.03) | 0.17 | −0.08 (−0.30; 0.14) | 0.28 |
| M-60 (c) | 8.85 ± 0.41 ab | 8.71 ± 0.41 ab | 8.71 ± 0.36 ab | η2 | 0.47 | 0.10 | <0.01 | −0.14 (−0.28; 0.01) | 0.07 | −0.14 (−0.29; 0.01) | 0.07 | |
| Variable | miR-15a-5p | miR-21-5p | miR-23a-3p | miR-146a-5p | miR-197-3p | miR-223-3p |
|---|---|---|---|---|---|---|
| MetS Criteria (NCEP—ATP III) | ||||||
| WC | −0.59 | −0.37 | 0.59 | 0.29 | 0.36 | NS |
| TG | NS | NS | 0.46 | NS | 0.36 | NS |
| HDL-C | NS | NS | NS | NS | NS | NS |
| FBG | −0.40 | −0.28 | 0.37 | 0.37 | NS | NS |
| SBP | NS | NS | NS | NS | NS | NS |
| DBP | NS | NS | 0.31 | NS | 0.37 | −0.29 |
| Indices of Body Composition | ||||||
| BM | −0.51 | −0.37 | 0.48 | NS | NS | NS |
| LBM | NS | NS | NS | NS | NS | NS |
| BF | −0.52 | −0.35 | 0.64 | NS | 0.48 | NS |
| WHtR | −0.53 | −0.33 | 0.60 | NS | 0.40 | NS |
| BMI | −0.53 | −0.34 | 0.54 | NS | 0.37 | NS |
| Other Metabolic Markers | ||||||
| HbA1c | NS | NS | 0.50 | 0.38 | 0.37 | −0.32 |
| T-CHOL | NS | NS | 0.57 | NS | 0.60 | −0.39 |
| LDL-C | −0.27 | NS | 0.58 | NS | 0.63 | −0.44 |
| AIP | NS | NS | 0.39 | NS | 0.32 | NS |
| CRI-I | −0.29 | NS | 0.54 | NS | 0.53 | −0.35 |
| CRI-II | NS | NS | 0.39 | NS | 0.32 | NS |
| TyG | NS | NS | 0.48 | NS | 0.39 | NS |
| LAP | −0.39 | NS | 0.63 | NS | 0.45 | NS |
| VAI | NS | NS | 0.40 | NS | 0.32 | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiecek, M.; Kusmierczyk, J.; Szymura, J.; Kreiner, G.; Szygula, Z. Whole-Body Cryotherapy Alters Circulating MicroRNA Profile in Postmenopausal Women. J. Clin. Med. 2023, 12, 5265. https://doi.org/10.3390/jcm12165265
Wiecek M, Kusmierczyk J, Szymura J, Kreiner G, Szygula Z. Whole-Body Cryotherapy Alters Circulating MicroRNA Profile in Postmenopausal Women. Journal of Clinical Medicine. 2023; 12(16):5265. https://doi.org/10.3390/jcm12165265
Chicago/Turabian StyleWiecek, Magdalena, Justyna Kusmierczyk, Jadwiga Szymura, Grzegorz Kreiner, and Zbigniew Szygula. 2023. "Whole-Body Cryotherapy Alters Circulating MicroRNA Profile in Postmenopausal Women" Journal of Clinical Medicine 12, no. 16: 5265. https://doi.org/10.3390/jcm12165265
APA StyleWiecek, M., Kusmierczyk, J., Szymura, J., Kreiner, G., & Szygula, Z. (2023). Whole-Body Cryotherapy Alters Circulating MicroRNA Profile in Postmenopausal Women. Journal of Clinical Medicine, 12(16), 5265. https://doi.org/10.3390/jcm12165265