

Enhancing Cognition in Older Adults with Mild Cognitive Impairment through High-Intensity Functional Training: A Single-Blind Randomized Controlled Trial

 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
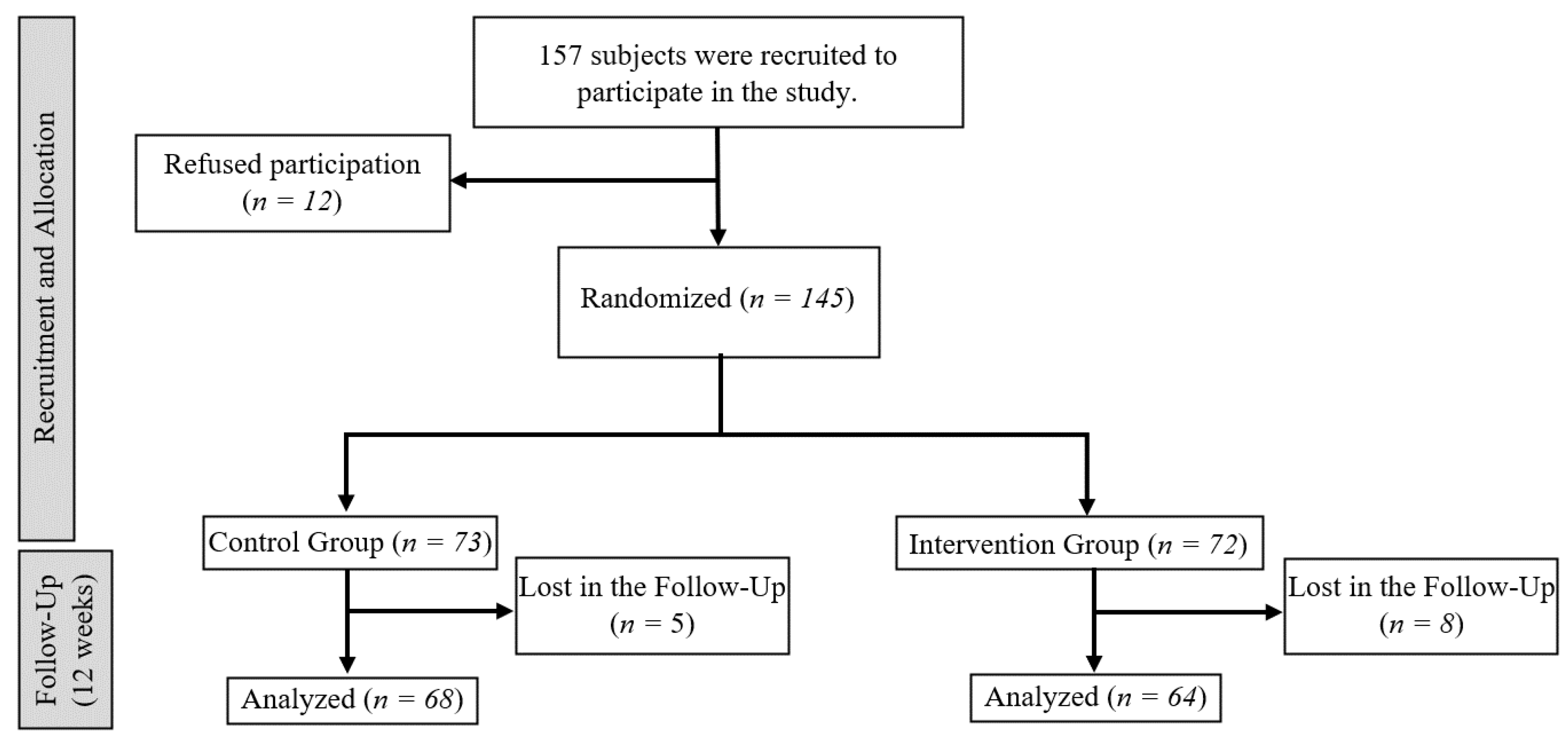
2.2. Participants
2.3. Procedures
2.4. Outcomes
2.5. Intervention
2.6. Statistical Analysis
3. Results
3.1. General Cognition
3.2. Attention
3.3. Executive Functions
3.4. Verbal Fluency
3.5. Selective Attention and Concentration
3.6. Processing Speed
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morley, J.E.; Morris, J.C.; Berg-Weger, M.; Borson, S.; Carpenter, B.D.; del Campo, N.; Dubois, B.; Fargo, K.; Fitten, L.J.; Flaherty, J.H.; et al. Brain Health: The Importance of Recognizing Cognitive Impairment: An IAGG Consensus Conference. J. Am. Med. Dir. Assoc. 2015, 16, 731–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jäncke, L.; Martin, M.; Röcke, C.; Mérillat, S. Editorial: Longitudinal aging research: Cognition, behavior and neuroscience. Front. Hum. Neurosci. 2022, 16, 1002560. [Google Scholar] [CrossRef] [PubMed]
- Anderson, N.D. State of the science on mild cognitive impairment (MCI). CNS Spectr. 2019, 24, 78–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez Palmer, N.; Trejo Ortega, B.; Joshi, P. Cognitive Impairment in Older Adults: Epidemiology, Diagnosis, and Treatment. Psychiatr. Clin. N. Am. 2022, 45, 639–661. [Google Scholar] [CrossRef] [PubMed]
- Sanford, A.M. Mild Cognitive Impairment. Clin. Geriatr. Med. 2017, 33, 325–337. [Google Scholar] [CrossRef]
- Middleton, L.E.; Barnes, D.E.; Lui, L.Y.; Yaffe, K. Physical activity over the life course and its association with cognitive performance and impairment in old age. J. Am. Geriatr. Soc. 2010, 58, 1322–1326. [Google Scholar] [CrossRef]
- Scarmeas, N.; Luchsinger, J.A.; Schupf, N.; Brickman, A.M.; Cosentino, S.; Tang, M.X.; Stern, Y. Physical activity, diet, and risk of Alzheimer disease. JAMA 2009, 302, 627–637. [Google Scholar] [CrossRef] [Green Version]
- Rodulfo, J.I.A. Sedentary lifestyle a disease from XXI century. Clin. Investig. Arterioscler. Publ. Off. Soc. Esp. Arterioscler. 2019, 31, 233–240. [Google Scholar] [CrossRef]
- GBD US Health Disparities Collaborators. Life expectancy by county, race, and ethnicity in the USA, 2000–2019: A systematic analysis of health disparities. Lancet 2022, 400, 25–38. [Google Scholar] [CrossRef]
- De la Rosa, A.; Olaso-Gonzalez, G.; Arc-Chagnaud, C.; Millan, F.; Salvador-Pascual, A.; García-Lucerga, C.; Blasco-Lafarga, C.; Garcia-Dominguez, E.; Carretero, A.; Correas, A.G.; et al. Physical exercise in the prevention and treatment of Alzheimer’s disease. J. Sport Health Sci. 2020, 9, 394–404. [Google Scholar] [CrossRef]
- Gomes, M.J.; Martinez, P.F.; Pagan, L.U.; Damatto, R.L.; Cezar, M.D.M.; Lima, A.R.R.; Okoshi, K.; Okoshi, M.P. Skeletal muscle aging: Influence of oxidative stress and physical exercise. Oncotarget 2017, 8, 20428–20440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López, M.D.; Zamarrón, M.D.; Fernández-Ballesteros, R. Relationship between exercising and physical and cognitive function indicators. Comparison of results with age. Rev. Esp. Geriatr. Gerontol. 2011, 46, 15–20. [Google Scholar] [CrossRef]
- Welford, P.; Östh, J.; Hoy, S.; Rossell, S.L.; Pascoe, M.; Diwan, V.; Hallgren, M. Effects of Yoga and Aerobic Exercise on Verbal Fluency in Physically Inactive Older Adults: Randomized Controlled Trial (FitForAge). Clin. Interv. Aging 2023, 18, 533–545. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Davis, J.C.; Falck, R.S.; Best, J.R.; Dao, E.; Vesely, K.; Ghag, C.; Rosano, C.; Hsu, C.L.; Dian, L.; et al. Exercise, Processing Speed, and Subsequent Falls: A Secondary Analysis of a 12-Month Randomized Controlled Trial. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 76, 675–682. [Google Scholar] [CrossRef]
- Ayers, M.R.; Bushnell, J.; Gao, S.; Unverzagt, F.; Gaizo, J.D.; Wadley, V.G.; Kennedy, R.; Clark, D.G. Verbal fluency response times predict incident cognitive impairment. Alzheimer’s Dement. 2022, 14, e12277. [Google Scholar] [CrossRef] [PubMed]
- Feito, Y.; Heinrich, K.M.; Butcher, S.J.; Poston, W.S.C. High-Intensity Functional Training (HIFT): Definition and Research Implications for Improved Fitness. Sports 2018, 6, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, S.; Knapp, K.; Lackie, A.; Lewry, C.; Horvey, K.; Benko, C.; Trinh, J.; Butcher, S. Multimodal high-intensity interval training increases muscle function and metabolic performance in females. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2015, 40, 1157–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiménez-García, J.D.; Martínez-Amat, A.; De la Torre-Cruz, M.J.; Fábrega-Cuadros, R.; Cruz-Díaz, D.; Aibar-Almazán, A.; Achalandabaso-Ochoa, A.; Hita-Contreras, F. Suspension Training HIIT Improves Gait Speed, Strength and Quality of Life in Older Adults. Int. J. Sport. Med. 2019, 40, 116–124. [Google Scholar] [CrossRef]
- Peixoto, R.P.; Trombert, V.; Poncet, A.; Kizlik, J.; Gold, G.; Ehret, G.; Trombetti, A.; Reny, J.L. Feasibility and safety of high-intensity interval training for the rehabilitation of geriatric inpatients (HIITERGY) a pilot randomized study. BMC Geriatr. 2020, 20, 197. [Google Scholar] [CrossRef]
- Rivas-Campo, Y.; García-Garro, P.A.; Aibar-Almazán, A.; Martínez-Amat, A.; Vega-Ávila, G.C.; Afanador-Restrepo, D.F.; León-Morillas, F.; Hita-Contreras, F. The Effects of High-Intensity Functional Training on Cognition in Older Adults with Cognitive Impairment: A Systematic Review. Healthcare 2022, 10, 670. [Google Scholar] [CrossRef]
- Pedraza, O.L.; Salazar, A.M.; Sierra, F.A.; Soler, D.; Castro, J.; Castillo, P.C.; Hernandez, M.A.; Piñeros, C. Confiabilidad, validez de criterio y discriminante del Montreal Cognitive Assessment (MoCA) test, en un grupo de Adultos de Bogotá. Acta Médica Colomb. 2017, 41, 221–228. [Google Scholar] [CrossRef]
- Reitan, R.M. Validity of the Trail Making Test as an Indicator of Organic Brain Damage. Percept. Mot. Ski. 1958, 8, 271–276. [Google Scholar] [CrossRef]
- Ryan, J.; Carrière, I.; Amieva, H.; Rouaud, O.; Berr, C.; Ritchie, K.; Scarabin, P.Y.; Ancelin, M.L. Prospective analysis of the association between estrogen receptor gene variants and the risk of cognitive decline in elderly women. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2013, 23, 1763–1768. [Google Scholar] [CrossRef] [Green Version]
- Isaacs, B.; Kennie, A.T. The Set test as an aid to the detection of dementia in old people. Br. J. Psychiatry J. Ment. Sci. 1973, 123, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Brickenkamp, R.; Cubero, N.S. D2: Test de Atención; Tea: Madrid, Spain, 2002. [Google Scholar]
- Jaeger, J. Digit Symbol Substitution Test: The Case for Sensitivity Over Specificity in Neuropsychological Testing. J. Clin. Psychopharmacol. 2018, 38, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Baskı: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Sugano, K.; Yokogawa, M.; Yuki, S.; Dohmoto, C.; Yoshita, M.; Hamaguchi, T.; Yanase, D.; Iwasa, K.; Komai, K.; Yamada, M. Effect of cognitive and aerobic training intervention on older adults with mild or no cognitive impairment: A derivative study of the nakajima project. Dement. Geriatr. Cogn. Disord. Extra 2012, 2, 69–80. [Google Scholar] [CrossRef]
- Mattap, S.M.; Mohan, D.; McGrattan, A.M.; Allotey, P.; Stephan, B.C.; Reidpath, D.D.; Siervo, M.; Robinson, L.; Chaiyakunapruk, N. The economic burden of dementia in low- and middle-income countries (LMICs): A systematic review. BMJ Glob. Health 2022, 7, e007409. [Google Scholar] [CrossRef]
- Tari, A.R.; Norevik, C.S.; Scrimgeour, N.R.; Kobro-Flatmoen, A.; Storm-Mathisen, J.; Bergersen, L.H.; Wrann, C.D.; Selbæk, G.; Kivipelto, M.; Moreira, J.B.N.; et al. Are the neuroprotective effects of exercise training systemically mediated? Prog. Cardiovasc. Dis. 2019, 62, 94–101. [Google Scholar] [CrossRef]
- Domingos, C.; Pêgo, J.M.; Santos, N.C. Effects of physical activity on brain function and structure in older adults: A systematic review. Behav. Brain Res. 2021, 402, 113061. [Google Scholar] [CrossRef]
- Falck, R.S.; Hsu, C.L.; Best, J.R.; Li, L.C.; Egbert, A.R.; Liu-Ambrose, T. Not Just for Joints: The Associations of Moderate-to-Vigorous Physical Activity and Sedentary Behavior with Brain Cortical Thickness. Med. Sci. Sport. Exerc. 2020, 52, 2217–2223. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Gbiri, C.A.O.; Amusa, B.F. Progressive task-oriented circuit training for cognition, physical functioning and societal participation in individuals with dementia. Physiother. Res. Int. J. Res. Clin. Phys. Ther. 2020, 25, e1866. [Google Scholar] [CrossRef]
- Singh, M.A.F.; Gates, N.; Saigal, N.; Wilson, G.C.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. The Study of Mental and Resistance Training (SMART) study—Resistance training and/or cognitive training in mild cognitive impairment: A randomized, double-blind, double-sham controlled trial. J. Am. Med. Dir. Assoc. 2014, 15, 873–880. [Google Scholar] [CrossRef]
- Zhu, Y.; Gao, Y.; Guo, C.; Qi, M.; Xiao, M.; Wu, H.; Ma, J.; Zhong, Q.; Ding, H.; Zhou, Q.; et al. Effect of 3-Month Aerobic Dance on Hippocampal Volume and Cognition in Elderly People With Amnestic Mild Cognitive Impairment: A Randomized Controlled Trial. Front. Aging Neurosci. 2022, 14, 771413. [Google Scholar] [CrossRef]
- Vega-Ávila, G.C.; Afanador-Restrepo, D.F.; Rivas-Campo, Y.; García-Garro, P.A.; Hita-Contreras, F.; Carcelén-Fraile, M.D.C.; Castellote-Caballero, Y.; Aibar-Almazán, A. Rhythmic Physical Activity and Global Cognition in Older Adults with and without Mild Cognitive Impairment: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 12230. [Google Scholar] [CrossRef]
- Masika, G.M.; Yu, D.S.F.; Li, P.W.C. Visual art therapy as a treatment option for cognitive decline among older adults. A systematic review and meta-analysis. J. Adv. Nurs. 2020, 76, 1892–1910. [Google Scholar] [CrossRef] [PubMed]
- Broadhouse, K.M.; Singh, M.F.; Suo, C.; Gates, N.; Wen, W.; Brodaty, H.; Jain, N.; Wilson, G.C.; Meiklejohn, J.; Singh, N.; et al. Hippocampal plasticity underpins long-term cognitive gains from resistance exercise in MCI. NeuroImage Clin. 2020, 25, 102182. [Google Scholar] [CrossRef] [PubMed]
- Varma, V.R.; Tang, X.; Carlson, M.C. Hippocampal sub-regional shape and physical activity in older adults. Hippocampus 2016, 26, 1051–1060. [Google Scholar] [CrossRef] [PubMed]
- Barha, C.K.; Best, J.R.; Rosano, C.; Yaffe, K.; Catov, J.M.; Liu-Ambrose, T. Sex-Specific Relationship Between Long-Term Maintenance of Physical Activity and Cognition in the Health ABC Study: Potential Role of Hippocampal and Dorsolateral Prefrontal Cortex Volume. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020, 75, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Regier, N.G.; Hodgson, N.A.; Gitlin, L.N. Characteristics of Activities for Persons With Dementia at the Mild, Moderate, and Severe Stages. Gerontologist 2017, 57, 987–997. [Google Scholar] [CrossRef] [PubMed]
- García-Garro, P.A.; Hita-Contreras, F.; Martínez-Amat, A.; Achalandabaso-Ochoa, A.; Jiménez-García, J.D.; Cruz-Díaz, D.; Aibar-Almazán, A. Effectiveness of A Pilates Training Program on Cognitive and Functional Abilities in Postmenopausal Women. Int. J. Environ. Res. Public Health 2020, 17, 3580. [Google Scholar] [CrossRef] [PubMed]
- Biazus-Sehn, L.F.; Schuch, F.B.; Firth, J.; Stigger, F.S. Effects of physical exercise on cognitive function of older adults with mild cognitive impairment: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2020, 89, 104048. [Google Scholar] [CrossRef] [PubMed]
- Boyne, P.; Meyrose, C.; Westover, J.; Whitesel, D.; Hatter, K.; Reisman, D.S.; Cunningham, D.; Carl, D.; Jansen, C.; Khoury, J.C.; et al. Exercise intensity affects acute neurotrophic and neurophysiological responses poststroke. J. Appl. Physiol. 2019, 126, 431–443. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, A.; Harvey, M.; Houghton, D.; Gray, W.K.; Weston, K.L.; Oates, L.L.; Romano, B.; Walker, R.W. Comparing the influence of exercise intensity on brain-derived neurotrophic factor serum levels in people with Parkinson’s disease: A pilot study. Aging Clin. Exp. Res. 2020, 32, 1731–1738. [Google Scholar] [CrossRef]
- Dos Santos, J.R.; Bortolanza, M.; Ferrari, G.D.; Lanfredi, G.P.; do Nascimento, G.C.; Azzolini, A.; Del Bel, E.; de Campos, A.C.; Faça, V.M.; Vulczak, A.; et al. One-Week High-Intensity Interval Training Increases Hippocampal Plasticity and Mitochondrial Content without Changes in Redox State. Antioxidants 2020, 9, 445. [Google Scholar] [CrossRef]
- De Lima, N.S.; De Sousa, R.A.L.; Amorim, F.T.; Gripp, F.; Diniz, E.M.C.O.; Henrique Pinto, S.; Peixoto, M.F.D.; Monteiro-Junior, R.S.; Bourbeau, K.; Cassilhas, R.C. Moderate-intensity continuous training and high-intensity interval training improve cognition, and BDNF levels of middle-aged overweight men. Metab. Brain Dis. 2022, 37, 463–471. [Google Scholar] [CrossRef]
- Kao, S.C.; Westfall, D.R.; Soneson, J.; Gurd, B.; Hillman, C.H. Comparison of the acute effects of high-intensity interval training and continuous aerobic walking on inhibitory control. Psychophysiology 2017, 54, 1335–1345. [Google Scholar] [CrossRef]
- Kao, S.C.; Wang, C.H.; Kamijo, K.; Khan, N.; Hillman, C. Acute effects of highly intense interval and moderate continuous exercise on the modulation of neural oscillation during working memory. Int. J. Psychophysiol. Off. J. Int. Organ. Psychophysiol. 2021, 160, 10–17. [Google Scholar] [CrossRef]
- Koyuncuoğlu, T.; Sevim, H.; Çetrez, N.; Meral, Z.; Gönenç, B.; Dertsiz, E.K.; Akakın, D.; Yüksel, M.; Çakır, Ö.K. High intensity interval training protects from Post Traumatic Stress Disorder induced cognitive impairment. Behav. Brain Res. 2021, 397, 112923. [Google Scholar] [CrossRef]
- Nicolò, A.; Girardi, M. The physiology of interval training: A new target to HIIT. J. Physiol. 2016, 594, 7169–7170. [Google Scholar] [CrossRef]
- Calverley, T.A.; Ogoh, S.; Marley, C.J.; Steggall, M.; Marchi, N.; Brassard, P.; Lucas, S.J.E.; Cotter, J.D.; Roig, M.; Ainslie, P.N.; et al. HIITing the brain with exercise: Mechanisms, consequences and practical recommendations. J. Physiol. 2020, 598, 2513–2530. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 132) | CG (n = 68) | IG (n = 64) | p Value | ||
|---|---|---|---|---|---|
| Age. Mean (SD) | 77.2 (7.6) | 77.19 (7.7) | 77.11 (7.3) | 0.951 | |
| MMSE. Mean (SD) | 21.5 (1.37) | 21.56 (1.25) | 21.62 (1.59) | 0.862 | |
| Sex. n (%) | Female | 79 (59.8) | 41 (60.3) | 38 (59.4) | 0.914 |
| Male | 53 (40.2) | 27 (39.7) | 26 (40.6) | ||
| Socioeconomic strata. n (%) | 1 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.731 |
| 2 | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| 3 | 45 (34.1) | 26 (38.2) | 19 (29.7) | ||
| 4 | 48 (36.4) | 23 (33.8) | 25 (39.1) | ||
| 5 | 22 (16.7) | 10 (14.7) | 12 (18.8) | ||
| 6 | 17 (12.9) | 9 (13.2) | 8 (12.5) | ||
| Education level. n (%) | Elementary school | 21 (15.9) | 12 (17.6) | 9 (14.1) | 0.862 |
| High school | 70 (53.0) | 35 (51.5) | 35 (54.7) | ||
| College | 38 (28.8) | 20 (29.4) | 18 (28.1) | ||
| Postgraduate | 3 (2.3) | 1 (1.5) | 2 (3.1) | ||
| Occupation. n (%) | Housewife | 55 (41.7) | 35 (51.5) | 20 (31.3) | 0.821 |
| Businessman | 5 (3.8) | 3 (4.4) | 2 (3.1) | ||
| Self-employed | 30 (22.7) | 14 (20.6) | 16 (25.0) | ||
| Employed | 42 (31.8) | 16 (23.5) | 26 (40.6) | ||
| Tobacco consumption. n (%) | No | 126 (95.5) | 63 (92.6) | 63 (98.4) | 0.115 |
| Yes | 6 (4.5) | 5 (7.4) | 1 (1.6) | ||
| Alcohol consumption. n (%) | No | 93 (70.5) | 46 (67.6) | 47 (73.4) | 0.466 |
| Yes | 39 (29.5) | 22 (32.4) | 17 (26.6) |
| Test Mean (SD) | Pre | Post | Group | Time | Group × Time | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CG | IG | p Value | CG | IG | p Value | F | p Value | η2 | F | p Value | η2 | F | p Value | η2 | |
| MoCA TEST. | 21.53 (1.18) | 21.63 (1.53) | 0.687 | 21.68 (1.27) | 22.58 (1.41) | <0.001 ** | 8.98 | 0.003 * | 0.031 | 10.93 | 0.001 * | 0.038 | 5.87 | 0.016 * | 0.021 |
| TMTA | 95.44 (10.47) | 97.25 (12.71) | 0.373 | 93.99 (10.37) | 85.86 (10.72) | <0.001 ** | 5.35 | 0.021 * | 0.018 | 22.13 | <0.001 ** | 0.074 | 13.24 | <0.001 ** | 0.044 |
| TMTB | 204.25 (38.60) | 199.33 (29.09) | 0.412 | 199.49 (41.91) | 186.83 (24.12) | 0.037 * | 3.067 | 0.039 * | 0.016 | 4155 | 0.043 | 0.015 | 0.834 | 0.362 | 0.003 |
| VFT | 20.19 (3.08) | 19.92 (3.18) | 0.622 | 22.2 (3.08) | 25.8 (2.43) | <0.001 ** | 20.5 | <0.001 ** | 0.048 | 115.6 | <0.001 ** | 0.273 | 27.8 | <0.001 ** | 0.065 |
| D2 | 48.90 (9.88) | 48.13 (10.45) | 0.663 | 53.97 (14.29) | 51.64 (12.12) | 0.316 | 1.135 | 0.288 | 0.004 | 8.699 | 0.003 * | 0.032 | 0.286 | 0.593 | 0.001 |
| D2-TA | 130.71 (17.78) | 128.53 (16.02) | 0.463 | 111.99 (19.34) | 210.58 (41.56) | <0.001 ** | 20.8 | <0.001 ** | 0.275 | 100 | <0.001 ** | 0.118 | 254 | <0.001 ** | 0.300 |
| D2-%E | 6.69 (2.30) | 6.80 (1.92) | 0.767 | 9.05 (3.38) | 5.37 (2.55) | <0.001 ** | 31.05 | <0.001 ** | 0.095 | 02.07 | 0.151 | 0.006 | 34.98 | <0.001 ** | 0.107 |
| D2-TOT | 338.38 (51.86) | 335.23 (51.74) | 0.728 | 347.47 (67.37) | 354.03 (57.74) | 0.55 | 0.058 | 0.810 | 0.000 | 3.861 | 0.050 | 0.015 | 0.468 | 0.494 | 0.002 |
| D2-CON | 122.29 (18.32) | 120.28 (15.93) | 0.503 | 101.40 (20.53) | 204.33 (43.39) | <0.001 ** | 235.5 | <0.001 ** | 0.280 | 92.2 | <0.001 ** | 0.109 | 254.7 | <0.001 ** | 0.302 |
| DSST | 48.03 (7.63) | 45.50 (8.61) | 0.076 | 48.22 (7.56) | 44.77 (9.69) | 0.24 | 8.3808 | 0.004 * | 0.031 | 0.069 | 0.793 | 0.000 | 0.201 | 0.655 | 0.001 |
| Model | Wilks’ λ | F | p Value |
|---|---|---|---|
| GROUP | 0.133 | 62.922 | <0.001 ** |
| EDUCATION LEVEL | 0.670 | 1.379 | 0.087 |
| SEX | 0.938 | 0.631 | 0.796 |
| GROUP × EDUCATION LEVEL | 0.635 | 1.580 | 0.026 * |
| GROUP × SEX | 0.932 | 0.710 | 0.730 |
| EDUCATION LEVEL × SEX | 0.906 | 0.493 | 0.976 |
| GROUP × EDUCATION LEVEL × SEX | 0.835 | 0.912 | 0.579 |
| AGE | 0.746 | 3.285 | <0.001 ** |
| MMSE | 0.698 | 4.174 | <0.001 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivas-Campo, Y.; Aibar-Almazán, A.; Rodríguez-López, C.; Afanador-Restrepo, D.F.; García-Garro, P.A.; Castellote-Caballero, Y.; Achalandabaso-Ochoa, A.; Hita-Contreras, F. Enhancing Cognition in Older Adults with Mild Cognitive Impairment through High-Intensity Functional Training: A Single-Blind Randomized Controlled Trial. J. Clin. Med. 2023, 12, 4049. https://doi.org/10.3390/jcm12124049
Rivas-Campo Y, Aibar-Almazán A, Rodríguez-López C, Afanador-Restrepo DF, García-Garro PA, Castellote-Caballero Y, Achalandabaso-Ochoa A, Hita-Contreras F. Enhancing Cognition in Older Adults with Mild Cognitive Impairment through High-Intensity Functional Training: A Single-Blind Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(12):4049. https://doi.org/10.3390/jcm12124049
Chicago/Turabian StyleRivas-Campo, Yulieth, Agustín Aibar-Almazán, Carlos Rodríguez-López, Diego Fernando Afanador-Restrepo, Patricia Alexandra García-Garro, Yolanda Castellote-Caballero, Alexander Achalandabaso-Ochoa, and Fidel Hita-Contreras. 2023. "Enhancing Cognition in Older Adults with Mild Cognitive Impairment through High-Intensity Functional Training: A Single-Blind Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 12: 4049. https://doi.org/10.3390/jcm12124049
APA StyleRivas-Campo, Y., Aibar-Almazán, A., Rodríguez-López, C., Afanador-Restrepo, D. F., García-Garro, P. A., Castellote-Caballero, Y., Achalandabaso-Ochoa, A., & Hita-Contreras, F. (2023). Enhancing Cognition in Older Adults with Mild Cognitive Impairment through High-Intensity Functional Training: A Single-Blind Randomized Controlled Trial. Journal of Clinical Medicine, 12(12), 4049. https://doi.org/10.3390/jcm12124049