
The Risk of BPPV, Meniere’s Disease, and Vestibular Neuronitis in Patients with Gout: A Longitudinal Follow-Up Study Using a National Health Screening Cohort

Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics
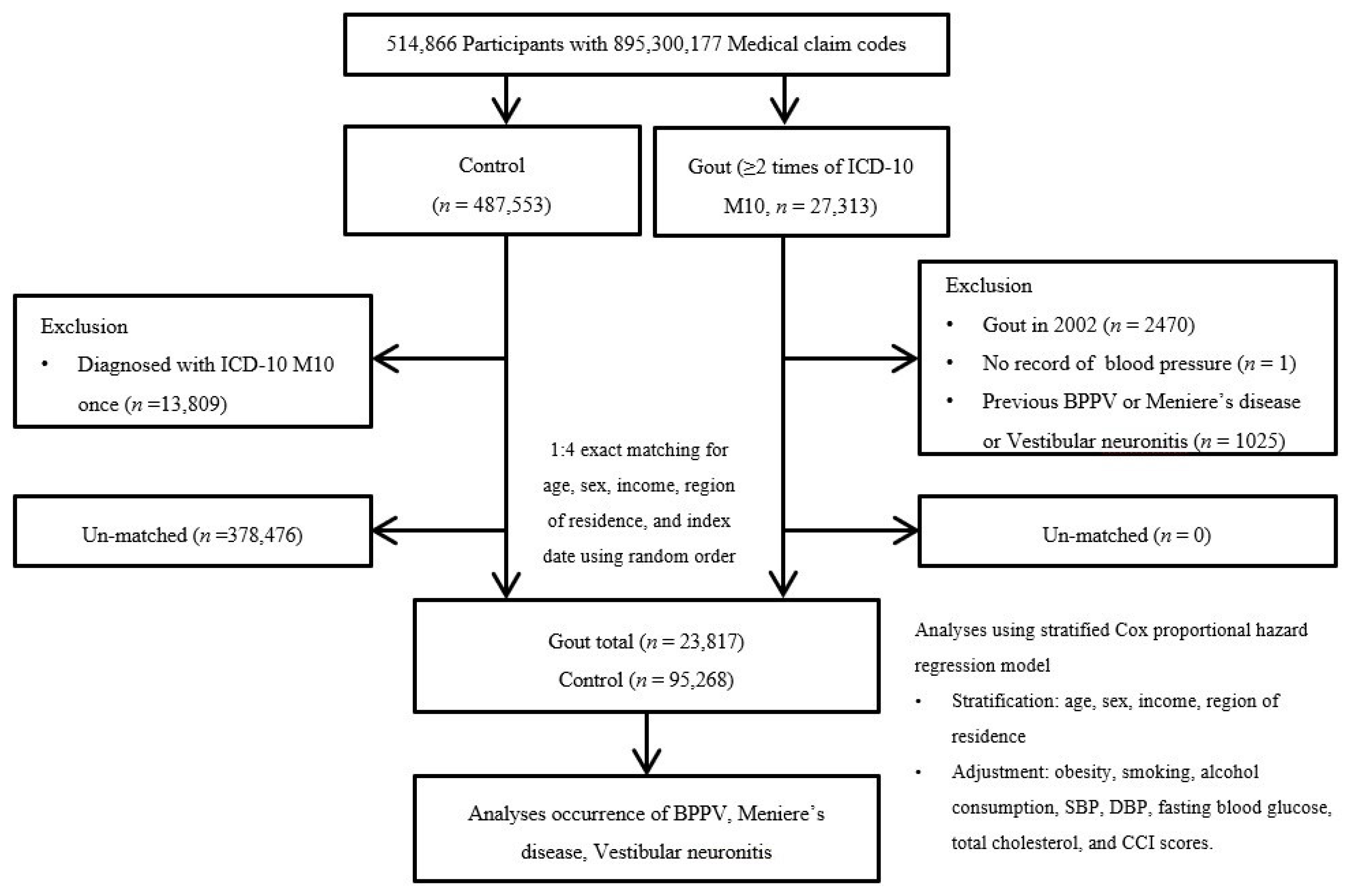
2.2. Study Population and Participant Selection
2.3. Definition of Gout
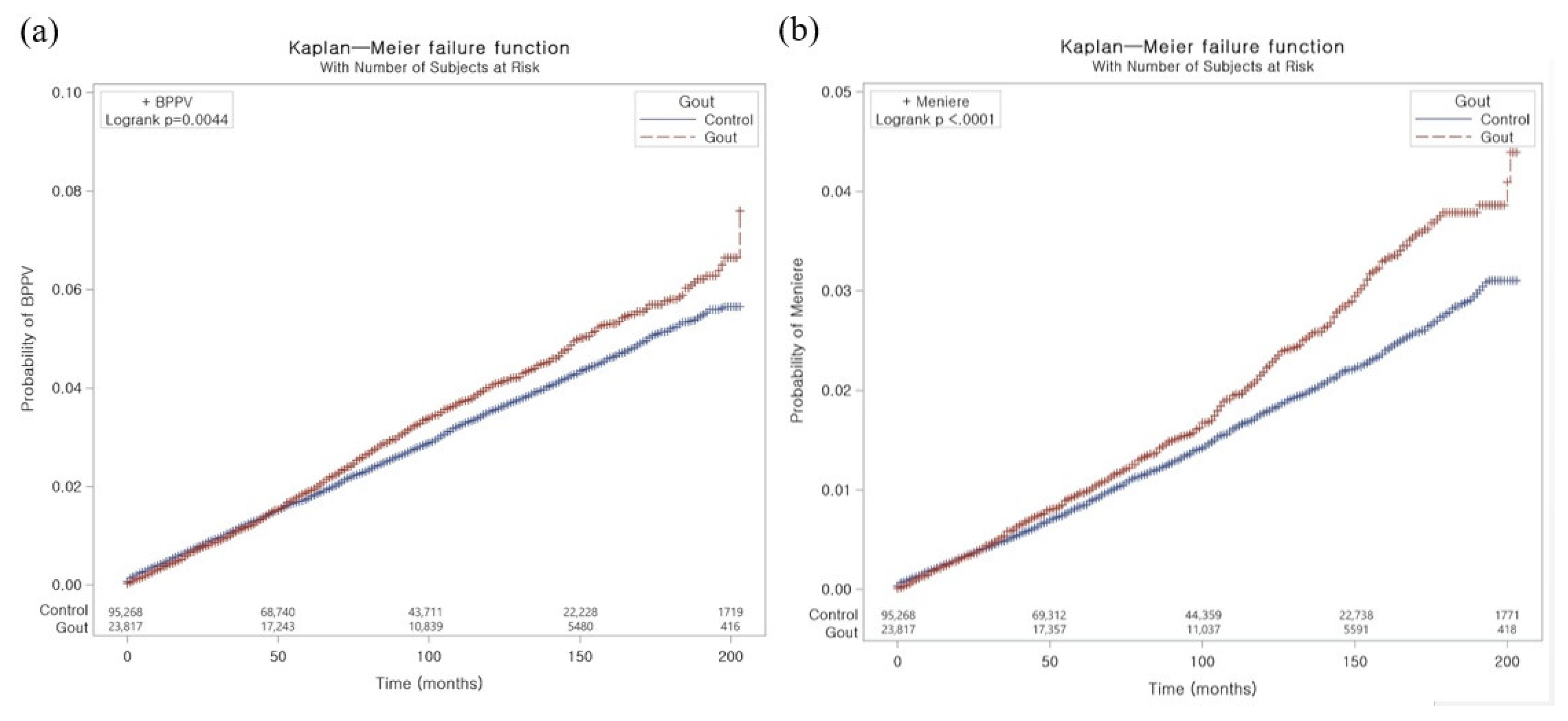
2.4. Definition of Benign Paroxysmal Positional Vertigo
2.5. Definition of Meniere’s Disease
2.6. Definition of Vestibular Neuronitis
2.7. Covariates
2.8. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Prevalence of gout and hyperuricemia in the US general population: The National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 2011, 63, 3136–3141. [Google Scholar] [CrossRef]
- Dehlin, M.; Jacobsson, L.; Roddy, E. Global epidemiology of gout: Prevalence, incidence, treatment patterns and risk factors. Nat. Rev. Rheumatol. 2020, 16, 380–390. [Google Scholar] [CrossRef]
- Kim, J.-W.; Kwak, S.G.; Lee, H.; Kim, S.-K.; Choe, J.-Y.; Park, S.-H. Prevalence and incidence of gout in Korea: Data from the national health claims database 2007–2015. Rheumatol. Int. 2017, 37, 1499–1506. [Google Scholar] [CrossRef]
- Kuo, C.-F.; Grainge, M.J.; Mallen, C.; Zhang, W.; Doherty, M. Comorbidities in patients with gout prior to and following diagnosis: Case-control study. Ann. Rheum. Dis. 2016, 75, 210–217. [Google Scholar] [CrossRef]
- Jung, J.H.; Song, G.G.; Ji, J.D.; Lee, Y.H.; Kim, J.-H.; Seo, Y.H.; Choi, S.J. Metabolic syndrome: Prevalence and risk factors in Korean gout patients. Korean J. Intern. Med. 2018, 33, 815. [Google Scholar] [CrossRef]
- Choi, H.K.; Ford, E.S.; Li, C.; Curhan, G. Prevalence of the metabolic syndrome in patients with gout: The Third National Health and Nutrition Examination Survey. Arthritis Rheum. 2007, 57, 109–115. [Google Scholar] [CrossRef]
- Abdul Sultan, A.; Mallen, C.; Hayward, R.; Muller, S.; Whittle, R.; Hotston, M.; Roddy, E. Gout and subsequent erectile dysfunction: A population-based cohort study from England. Arthritis Res. Ther. 2017, 19, 123. [Google Scholar] [CrossRef]
- Chen, Y.-F.; Lin, H.-H.; Lu, C.-C.; Hung, C.-T.; Lee, M.-H.; Hsu, C.-Y.; Chung, W.-S. Gout and a subsequent increased risk of erectile dysfunction in men aged 64 and under: A nationwide cohort study in Taiwan. J. Rheumatol. 2015, 42, 1898–1905. [Google Scholar] [CrossRef]
- Hsu, C.-Y.; Lin, C.-L.; Kao, C.-H. Gout is associated with organic and psychogenic erectile dysfunction. Eur. J. Intern. Med. 2015, 26, 691–695. [Google Scholar] [CrossRef]
- Singh, J.A.; Cleveland, J.D. Gout and the risk of incident atrial fibrillation in older adults: A study of US Medicare data. RMD Open 2018, 4, e000712. [Google Scholar] [CrossRef]
- Kuo, Y.-J.; Tsai, T.-H.; Chang, H.-P.; Chua, S.; Chung, S.-Y.; Yang, C.-H.; Lin, C.-J.; Wu, C.-J.; Hang, C.-L. The risk of atrial fibrillation in patients with gout: A nationwide population-based study. Sci. Rep. 2016, 6, 32220. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kuo, C.-F.; Grainge, M.J.; Mallen, C.; Zhang, W.; Doherty, M. Impact of gout on the risk of atrial fibrillation. Rheumatology 2016, 55, 721–728. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kim, S.C.; Liu, J.; Solomon, D.H. Risk of incident atrial fibrillation in gout: A cohort study. Ann. Rheum. Dis. 2016, 75, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Peloquin, C.E.; Dubreuil, M.; Roddy, E.; Lu, N.; Neogi, T.; Choi, H.K. Sleep apnea and the risk of incident gout: A population-based, body mass index–matched cohort study. Arthritis Rheumatol. 2015, 67, 3298–3302. [Google Scholar] [CrossRef] [PubMed]
- Blagojevic-Bucknall, M.; Mallen, C.; Muller, S.; Hayward, R.; West, S.; Choi, H.; Roddy, E. The risk of gout among patients with sleep apnea: A matched cohort study. Arthritis Rheumatol. 2019, 71, 154–160. [Google Scholar] [CrossRef]
- Kok, V.; Horng, J.-T.; Wang, M.; Chen, Z.-Y.; Kuo, J.-T.; Hung, G.-D. Gout as a risk factor for osteoporosis: Epidemiologic evidence from a population-based longitudinal study involving 108,060 individuals. Osteoporos. Int. 2018, 29, 973–985. [Google Scholar] [CrossRef]
- Chiu, C.; Chen, Y.; Hsu, C.; Chang, C.; Huang, C.; Leu, H.; Li, S.; Kuo, S.; Huang, P.; Chen, J. Association between previous history of gout attack and risk of deep vein thrombosis—A nationwide population-based cohort study. Sci. Rep. 2016, 6, 26541. [Google Scholar] [CrossRef]
- Li, L.; McCormick, N.; Sayre, E.C.; Esdaile, J.M.; Lacaille, D.; Xie, H.; Choi, H.K.; Aviña-Zubieta, J.A. Trends of venous thromboembolism risk before and after diagnosis of gout: A general population-based study. Rheumatology 2020, 59, 1099–1107. [Google Scholar] [CrossRef]
- Sultan, A.A.; Muller, S.; Whittle, R.; Roddy, E.; Mallen, C.; Clarson, L. Venous thromboembolism in patients with gout and the impact of hospital admission, disease duration and urate-lowering therapy. CMAJ 2019, 191, E597–E603. [Google Scholar] [CrossRef]
- Kubota, Y.; McAdams-DeMarco, M.; Folsom, A.R. Serum uric acid, gout, and venous thromboembolism: The atherosclerosis risk in communities study. Thromb. Res. 2016, 144, 144–148. [Google Scholar] [CrossRef]
- Neuhauser, H.; Von Brevern, M.; Radtke, A.; Lezius, F.; Feldmann, M.; Ziese, T.; Lempert, T. Epidemiology of vestibular vertigo: A neurotologic survey of the general population. Neurology 2005, 65, 898–904. [Google Scholar] [CrossRef]
- Lempert, T.; Neuhauser, H. Epidemiology of vertigo, migraine and vestibular migraine. J. Neurol. 2009, 256, 333–338. [Google Scholar] [CrossRef]
- Neuhauser, H.K. Epidemiology of vertigo. Hand. Clin. Neurol. 2007, 20, 40–46. [Google Scholar] [CrossRef]
- Bhattacharyya, N.; Gubbels, S.P.; Schwartz, S.R.; Edlow, J.A.; El-Kashlan, H.; Fife, T.; Holmberg, J.M.; Mahoney, K.; Hollingsworth, D.B.; Roberts, R. Clinical practice guideline: Benign paroxysmal positional vertigo (update). Otolaryngol. Head Neck Surg. 2017, 156 (Suppl. S3), S1–S47. [Google Scholar] [CrossRef]
- Furman, J.M.; Cass, S.P. Benign paroxysmal positional vertigo. N. Engl. J. Med. 1999, 341, 1590–1596. [Google Scholar] [CrossRef]
- Chen, C.-C.; Cho, H.-S.; Lee, H.-H.; Hu, C.-J. Efficacy of repositioning therapy in patients with benign paroxysmal positional vertigo and preexisting central neurologic disorders. Front. Neurol. 2018, 9, 486. [Google Scholar] [CrossRef]
- Sajjadi, H.; Paparella, M.M. Meniere’s disease. Lancet 2008, 372, 406–414. [Google Scholar] [CrossRef]
- Watanabe, Y.; Mizukoshi, K.; Shojaku, H.; Watanabe, I.; Hinoki, M.; Kitahara, M. Epidemiological and clinical characteristics of Meniere’s disease in Japan. Acta Otolaryngol. 1995, 115, 206–210. [Google Scholar] [CrossRef]
- Le, T.N.; Westerberg, B.D.; Lea, J. Vestibular neuritis: Recent advances in etiology, diagnostic evaluation, and treatment. Adv. Otorhinolaryngol. 2019, 82, 87–92. [Google Scholar]
- Adam, A. Benign positional vertigo as a clinical manifestation of hyperuricemia–a recent discovery. J. Neurol. Sci. 2001, 187 (Suppl. S1), 222. [Google Scholar]
- Celikbilek, A.; Gencer, Z.; Saydam, L.; Zararsiz, G.; Tanik, N.; Ozkiris, M. Serum uric acid levels correlate with benign paroxysmal positional vertigo. Eur. J. Neurol. 2014, 21, 79–85. [Google Scholar] [CrossRef]
- Yang, X.; Yang, B.; Wu, M.; Wang, F.; Huang, X.; Li, K.; Mao, Z.; Xu, Z.; Ren, H. Association between serum uric acid levels and benign paroxysmal positional vertigo: A systematic review and meta-analysis of observational studies. Front. Neurol. 2019, 10, 91. [Google Scholar] [CrossRef]
- Lin, Y.-T.; Lin, H.-W.; Huang, Y.-C.; Ho, W.-T.; Li, Y.-C.; Chen, T.-J. Association between gout and vertigo in a Taiwanese population. J. Clin. Neurosci. 2013, 20, 857–861. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.G. Tobacco smoking and alcohol consumption are related to benign parotid tumor: A nested case-control study using a national health screening cohort. Clin. Exp. Otorhinolaryngol. 2019, 12, 412–419. [Google Scholar] [CrossRef]
- World Health Organization Western Pacific Region; IASO, International Association for the Study of Obesity. The Asia-Pacific perspective: Redefining obesity and its treatment. Int. Obes. Taskforce 2000, 2, 15–21. [Google Scholar]
- Quan, H.; Li, B.; Couris, C.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.; Sundararajan, V. Practice of epidemiology: Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef]
- Yuan, J.; Chen, Y.; Niu, S.; Li, S.; Dong, Q.; Hu, W. Relationship between serum level of uric acid and benign paroxysmal positional vertigo. Zhonghua Yi Xue Za Zhi 2015, 95, 344–348. [Google Scholar]
- Dong, L.; Wang, Z.; Zhang, W.; Bao, L.; Cui, G.; Ye, X. The correlation between serum uric acid level and benign paroxysmal position vertigo. Chin. J. Pract Nervous Dis. 2017, 20, 21–23. [Google Scholar]
- Xu, M.; Chen, W.; Liu, L.; Wang, F.; Ling, Y.; Huang, Z. Study on the correlation between uric acid level and benign paroxysmal positional vertigo. J. Xiangnan Univ. 2015, 17, 11–13. [Google Scholar]
- Wei, S.; Liu, J.; Liu, Z. Plasma homocysteine and uric acid levels in young patients with benign paroxysmal positional vertigo and their correlations. Chin. J. Ophthalmol. Otorhinolaryngol. 2017, 17, 126–751. [Google Scholar]
- Si, J. Analysis of serum uric acid level in patients with benign paroxysmal positional vertigo. Qinghai Med. J. 2016, 46, 54–55. [Google Scholar]
- Zhu, X.; Sima, G.; Dai, L.; Ji, W. Relationship between benign paroxysmal positional vertigo and serum uric acid level in elderly patients. Chin. Arch. Otolaryngol. Head Neck Surg. 2016, 23, 696–699. [Google Scholar]
- Ziavra, N.V.; Bronstein, A.M. Is uric acid implicated in benign paroxysmal positional vertigo? J. Neurol. 2004, 251, 115. [Google Scholar] [CrossRef]
- Lu, L.; Wang, W.; Fan, C.; Li, J. Risk factors associated with benign paroxysmal positional vertigo—A case-control study. J. Nantong Univ. 2017, 37, 442–444. [Google Scholar]
- Yuan, J.; Dai, J.; Li, W.A.; Hu, W. Factors associated with benign paroxysmal positional vertigo: A Chinese case-control study. Med. Sci. Monit. 2017, 23, 3885. [Google Scholar] [CrossRef]
- Jeong, S.H.; Kim, J.S. The effect of serum uric acid in generating idiopathic benign paroxysmal positional vertigo. Res. Vestib. Sci. 2010, 9, 27–31. [Google Scholar]
- Lins, U.; Farina, M.; Kurc, M.C.; Riordan, G.; Thalmann, R.; Thalmann, I.; Kachar, B. The otoconia of the guinea pig utricle: Internal structure, surface exposure, and interactions with the filament matrix. J. Struct. Biol. 2000, 131, 67–78. [Google Scholar] [CrossRef]
- Chen, D.P.; Wong, C.K.; Tam, L.S.; Li, E.K.; Lam, C.W. Activation of human fibroblast-like synoviocytes by uric acid crystals in rheumatoid arthritis. Cell. Mol. Immunol. 2011, 8, 469–478. [Google Scholar] [CrossRef]
- Chao, H.H.; Liu, J.C.; Lin, J.W.; Chen, C.H.; Wu, C.H.; Cheng, T.H. Uric acid stimulates endothelin-1 gene expression associated with NADPH oxidase in human aortic smooth muscle cells. Acta pharmacol. Sin. 2008, 29, 1301–1312. [Google Scholar] [CrossRef]
- Khosla, U.M.; Zharikov, S.; Finch, J.L.; Nakagawa, T.; Roncal, C.; Mu, W.; Krotova, K.; Block, E.R.; Prabhakar, S.; Johnson, R.J. Hyperuricemia induces endothelial dysfunction. Kidney Int. 2005, 67, 1739–1742. [Google Scholar] [CrossRef]
- Kariya, S.; Cureoglu, S.; Fukushima, H.; Nomiya, S.; Nomiya, R.; Schachern, P.A.; Nishizaki, K.; Paparella, M.M. Vascular findings in the stria vascularis of patients with unilateral or bilateral Ménière’s disease: A histopathologic temporal bone study. Otol. Neurotol. 2009, 30, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.J.; Brown, D. Experimental animal models for meniere’s disease: A mini-review. J. Audiol. Otol. 2020, 24, 53. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.; Breeze, R. The Meniere attack: An ischemia/reperfusion disorder of inner ear sensory tissues. Med. Hypotheses 2013, 81, 1108–1115. [Google Scholar] [CrossRef] [PubMed]
- Evans, P.L.; Prior, J.A.; Belcher, J.; Mallen, C.D.; Hay, C.A.; Roddy, E. Obesity, hypertension and diuretic use as risk factors for incident gout: A systematic review and meta-analysis of cohort studies. Arthritis Res. Ther. 2018, 20, 136. [Google Scholar] [CrossRef]
- Li, X.; Tong, Q.; Xie, D.; Chen, Z.; Pan, S.; Zhang, X.; Dong, W. Low serum uric acid levels in patients with acute central nervous system viral infections. Neuroreport 2017, 28, 1250–1254. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rho, Y.H.; Zhu, Y.; Choi, H.K. The epidemiology of uric acid and fructose. Semin. Nephrol. 2011, 31, 410–419. [Google Scholar] [CrossRef]
- Hak, A.E.; Curhan, G.C.; Grodstein, F.; Choi, H.K. Menopause, postmenopausal hormone use and risk of incident gout. Ann. Rheum. Dis. 2010, 69, 1305–1309. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Before Overlap Weighting Adjustment | After Overlap Weighting Adjustment | ||||
|---|---|---|---|---|---|---|
| Gout | Control | Standardized Difference | Gout | Control | Standardized Difference | |
| Age (n, %) | 0.00 | 0.00 | ||||
| 40–44 | 591 (2.48) | 2364 (2.48) | 444 (2.44) | 444 (2.44) | ||
| 45–49 | 2072 (8.70) | 8288 (8.70) | 1547 (8.51) | 1547 (8.51) | ||
| 50–54 | 3602 (15.12) | 14,408 (15.12) | 2719 (14.97) | 2719 (14.97) | ||
| 55–59 | 4688 (19.68) | 18,752 (19.68) | 3582 (19.72) | 3582 (19.72) | ||
| 60–64 | 4080 (17.13) | 16,320 (17.13) | 3131 (17.23) | 3131 (17.23) | ||
| 65–69 | 3382 (14.20) | 13,528 (14.20) | 2589 (14.25) | 2589 (14.25) | ||
| 70–74 | 2645 (11.11) | 10,580 (11.11) | 2027 (11.16) | 2027 (11.16) | ||
| 75–79 | 1687 (7.08) | 6748 (7.08) | 1300 (7.15) | 1300 (7.15) | ||
| 80–84 | 815 (3.42) | 3260 (3.42) | 632 (3.48) | 632 (3.48) | ||
| 85+ | 255 (1.07) | 1020 (1.07) | 198 (1.09) | 198 (1.09) | ||
| Sex (n, %) | 0.00 | 0.00 | ||||
| Male | 18,948 (79.56) | 75,792 (79.56) | 14,372 (79.11) | 14,372 (79.11) | ||
| Female | 4869 (20.44) | 19,476 (20.44) | 3796 (20.89) | 3796 (20.89) | ||
| Income (n, %) | 0.00 | 0.00 | ||||
| 1 (lowest) | 3456 (14.51) | 13,824 (14.51) | 2637 (14.51) | 2637 (14.51) | ||
| 2 | 2944 (12.36) | 11,776 (12.36) | 2252 (12.40) | 2252 (12.40) | ||
| 3 | 3609 (15.15) | 14,436 (15.15) | 2756 (15.17) | 2756 (15.17) | ||
| 4 | 5038 (21.15) | 20,152 (21.15) | 3841 (21.14) | 3841 (21.14) | ||
| 5 (highest) | 8770 (36.82) | 35,080 (36.82) | 6681 (36.78) | 6681 (36.78) | ||
| Region of residence (n, %) | 0.00 | 0.00 | ||||
| Urban | 10,062 (42.25) | 40,248 (42.25) | 7668 (42.21) | 7668 (42.21) | ||
| Rural | 13,755 (57.75) | 55,020 (57.75) | 10,499 (57.79) | 10,499 (57.79) | ||
| Obesity † (n, %) | 0.28 | 0.00 | ||||
| Underweight | 317 (1.33) | 2415 (2.53) | 269 (1.48) | 269 (1.48) | ||
| Normal | 5969 (25.06) | 33,032 (34.67) | 4901 (26.98) | 4901 (26.98) | ||
| Overweight | 6511 (27.34) | 26,813 (28.14) | 5057 (27.84) | 5057 (27.84) | ||
| Obese I | 9960 (41.82) | 30,612 (32.13) | 7231 (39.80) | 7231 (39.80) | ||
| Obese II | 1060 (4.45) | 2396 (2.52) | 709 (3.90) | 709 (3.90) | ||
| Smoking status (n, %) | 0.08 | 0.00 | ||||
| Nonsmoker | 12,449 (53.79) | 49,257 (53.23) | 9771 (53.78) | 9771 (53.78) | ||
| Past smoker | 5483 (23.69) | 19,833 (21.43) | 4218 (23.22) | 4218 (23.22) | ||
| Current smoker | 5212 (22.52) | 23,447 (25.34) | 4178 (23.00) | 4178 (23.00) | ||
| Alcohol consumption (n, %) | 0.09 | 0.00 | ||||
| <1 time a week | 12,085 (50.74) | 52,581 (55.19) | 9380 (51.63) | 9380 (51.63) | ||
| ≥1 time a week | 11,732 (49.26) | 42,687 (44.81) | 8787 (48.37) | 8787 (48.37) | ||
| Systolic blood pressure (Mean, SD) | 129.56 (16.85) | 127.37 (16.29) | 0.13 | 129.04 (14.81) | 129.04 (7.32) | 0.00 |
| Diastolic blood pressure (Mean, SD) | 80.16 (11.03) | 78.83 (10.61) | 0.12 | 79.83 (9.69) | 79.83 (4.77) | 0.00 |
| Fasting blood glucose (Mean, SD) | 102.56 (28.28) | 103.03 (30.88) | 0.02 | 102.68 (25.60) | 102.68 (12.51) | 0.00 |
| Total cholesterol (Mean, SD) | 198.40 (40.52) | 195.26 (37.85) | 0.08 | 197.55 (35.71) | 197.55 (17.06) | 0.00 |
| CCI score (Mean, SD) | 1.20 (1.84) | 0.99 (1.71) | 0.12 | 1.15 (1.58) | 1.15 (0.83) | 0.00 |
| BPPV (n, %) | 762 (3.20) | 2715 (2.85) | 0.02 | 583 (3.21) | 518 (2.85) | 0.02 |
| Meniere’s disease (n, %) | 434 (1.82) | 1382 (1.45) | 0.03 | 329 (1.81) | 264 (1.45) | 0.03 |
| Vestibular neuronitis (n, %) | 195 (0.82) | 714 (0.75) | 0.01 | 148 (0.81) | 139 (0.77) | 0.01 |
| Independent Variables | IR Per 1000 Person-Year | IRD Per 1000 Person-Years (95% Confidence Interval) | Hazard Ratios for BPPV (95% Confidence Interval) | |||
|---|---|---|---|---|---|---|
| Crude † | p-Value | Adjusted †‡ | p-Value | |||
| Total participants (n = 119,085) | ||||||
| Gout | 4.27 | 0.47 (0.15 to 0.80) | 1.12 (1.04–1.22) | 0.004 * | 1.13 (1.06–1.21) | <0.001 * |
| Control | 3.79 | 1 | 1 | |||
| Age < 60 (n = 54,765) | ||||||
| Gout | 3.51 | 0.55 (0.17 to 0.93) | 1.18 (1.05–1.33) | 0.005 * | 1.17 (1.06–1.29) | 0.001 * |
| Control | 2.96 | 1 | 1 | |||
| Age ≥ 60 (n = 64,320) | ||||||
| Gout | 5.29 | 0.37 (−0.19 to 0.93) | 1.07 (0.96–1.20) | 0.208 | 1.09 (0.99–1.19) | 0.070 |
| Control | 4.92 | 1 | 1 | |||
| Men (n = 94,740) | ||||||
| Gout | 3.61 | 0.29 (−0.05 to 0.62) | 1.09 (0.99–1.20) | 0.095 | 1.08 (1–1.17) | 0.049 * |
| Control | 3.32 | 1 | 1 | |||
| Women (n = 24,345) | ||||||
| Gout | 7.07 | 1.32 (0.40 to 2.24) | 1.23 (1.06–1.42) | 0.005 * | 1.23 (1.09–1.38) | <0.001 * |
| Control | 5.76 | 1 | 1 | |||
| Underweight (n = 2732) | ||||||
| Gout | 6.21 | 2.33 (−0.71 to 5.37) | 1.58 (0.85–2.94) | 0.147 | 1.29 (0.82–2.03) | 0.269 |
| Control | 3.88 | 1 | 1 | |||
| Normal weight (n = 29,706) | ||||||
| Gout | 4.84 | 0.43 (−0.55 to 1.42) | 1.32 (1.14–1.54) | <0.001 * | 1.28 (1.14–1.44) | <0.001 * |
| Control | 3.65 | 1 | 1 | |||
| Overweight (n = 39,001) | ||||||
| Gout | 4.32 | 0.46 (−0.16 to 1.08) | 1.12 (0.96–1.30) | 0.149 | 1.13 (1–1.28) | 0.049 * |
| Control | 3.86 | 1 | 1 | |||
| Obese I (n = 40,572) | ||||||
| Gout | 3.95 | 0.08 (−0.43 to 0.59) | 1.02 (0.90–1.16) | 0.740 | 1.04 (0.93–1.16) | 0.521 |
| Control | 3.87 | 1 | 1 | |||
| Obese II (n = 3456) | ||||||
| Gout | 3.34 | −0.60 (−2.27 to 1.06) | 0.84 (0.53–1.33) | 0.466 | 0.86 (0.56–1.32) | 0.489 |
| Control | 3.95 | 1 | 1 | |||
| Fasting blood glucose < 100 mg/dL (n = 68,732) | ||||||
| Gout | 4.34 | 0.51 (0.09 to 0.92) | 1.13 (1.02–1.25) | 0.018 * | 1.13 (1.04–1.23) | 0.004 * |
| Control | 3.84 | 1 | 1 | |||
| Fasting blood glucose ≥ 100 mg/dL (n= 50,353) | ||||||
| Gout | 4.16 | 0.43 (−0.08 to 0.94) | 1.11 (0.98–1.27) | 0.099 | 1.12 (1.01–1.25) | 0.033 * |
| Control | 3.73 | 1 | 1 | |||
| Independent Variables | IR Per 1000 Person-Year | IRD Per 1000 Person-Years (95% Confidence Interval) | Hazard ratios for Meniere’s Disease (95% Confidence Interval) | |||
|---|---|---|---|---|---|---|
| Crude † | p-Value | Adjusted †‡ | p-Value | |||
| Total participants (n = 119,085) | ||||||
| Gout | 2.41 | 0.53 (0.27 to 0.80) | 1.26 (1.13–1.40) | <0.001 * | 1.26 (1.15–1.37) | <0.001 * |
| Control | 1.91 | 1 | 1 | |||
| Age < 60 (n = 54,765) | ||||||
| Gout | 1.90 | 0.44 (0.03 to 0.86) | 1.39 (1.18–1.64) | <0.001 * | 1.37 (1.2–1.58) | <0.001 * |
| Control | 1.37 | 1 | 1 | |||
| Age ≥ 60 (n = 64,320) | ||||||
| Gout | 3.08 | 0.37 (−0.19 to 0.93) | 1.17 (1.01–1.35) | 0.035 * | 1.17 (1.03–1.32) | 0.012 * |
| Control | 2.64 | 1 | 1 | |||
| Men (n = 94,740) | ||||||
| Gout | 1.92 | 0.23 (−0.01 to 0.46) | 1.13 (0.99–1.29) | 0.065 | 1.11 (1–1.24) | 0.06 |
| Control | 1.70 | 1 | 1 | |||
| Women (n = 24,345) | ||||||
| Gout | 4.45 | 1.66 (1.00 to 2.32) | 1.59 (1.32–1.92) | <0.001 * | 1.61 (1.37–1.90) | <0.001 * |
| Control | 2.79 | 1 | 1 | |||
| Underweight (n = 2732) | ||||||
| Gout | 4.07 | 2.18 (0.01 to 4.34) | 2.14 (0.98–4.67) | 0.056 | 1.83 (0.98–3.40) | 0.058 |
| Control | 1.89 | 1 | 1 | |||
| Normal weight (n = 29,706) | ||||||
| Gout | 2.75 | 0.80 (0.34 to 1.26) | 1.41 (1.16–1.73) | <0.001 * | 1.32 (1.13–1.54) | <0.001 * |
| Control | 1.95 | 1 | 1 | |||
| Overweight (n = 39,001) | ||||||
| Gout | 2.55 | 0.63 (0.19 to 1.08) | 1.33 (1.09–1.63) | 0.005 * | 1.32 (1.11–1.56) | 0.002 * |
| Control | 1.91 | 1 | 1 | |||
| Obese I (n = 40,572) | ||||||
| Gout | 2.16 | 0.29 (−0.07 to 0.64) | 1.15 (0.97–1.38) | 0.117 | 1.18 (1.01–1.38) | 0.043 * |
| Control | 1.88 | 1 | 1 | |||
| Obese II (n = 3456) | ||||||
| Gout | 1.59 | −0.24 (−1.38 to 0.89) | 0.87 (0.45–1.70) | 0.693 | 0.97 (0.53–1.78) | 0.922 |
| Control | 1.83 | 1 | 1 | |||
| Fasting blood glucose < 100 mg/dL (n = 68,732) | ||||||
| Gout | 2.57 | 0.72 (0.42 to 1.01) | 1.39 (1.21–1.59) | <0.001 * | 1.39 (1.24–1.56) | <0.001 * |
| Control | 1.85 | 1 | 1 | |||
| Fasting blood glucose ≥ 100 mg/dL (n = 50,353) | ||||||
| Gout | 2.16 | 0.15 (−0.22 to 0.52) | 1.08 (0.90–1.29) | 0.418 | 1.06 (0.91–1.23) | 0.467 |
| Control | 2.01 | 1 | 1 | |||
| Independent Variables | IR Per 1000 Person-Year | IRD Per 1000 Person-Years (95% Confidence Interval) | Hazard Ratios for Vestibular Neuronitis (95% Confidence Interval) | |||
|---|---|---|---|---|---|---|
| Crude † | p-Value | Adjusted †‡ | p-Value | |||
| Total participants (n = 119,085) | ||||||
| Gout | 1.07 | 0.09 (−0.07 to 0.25) | 1.09 (0.93–1.28) | 0.274 | 1.06 (0.93–1.21) | 0.391 |
| Control | 0.98 | 1 | 1 | |||
| Age < 60 (n = 54,765) | ||||||
| Gout | 0.94 | 0.13 (−0.06 to 0.33) | 1.16 (0.93–1.46) | 0.187 | 1.11 (0.92–1.34) | 0.277 |
| Control | 0.81 | 1 | 1 | |||
| Age ≥ 60 (n = 64,320) | ||||||
| Gout | 1.25 | 0.04 (−0.24 to 0.31) | 1.03 (0.82–1.29) | 0.805 | 1.01 (0.84–1.20) | 0.952 |
| Control | 1.22 | 1 | 1 | |||
| Men (n = 94,740) | ||||||
| Gout | 0.98 | 0.04 (−0.14 to 0.22) | 1.04 (0.87–1.26) | 0.645 | 1.01 (0.87–1.17) | 0.944 |
| Control | 0.94 | 1 | 1 | |||
| Women (n = 24,345) | ||||||
| Gout | 1.48 | 0.30 (−0.11 to 0.71) | 1.26 (0.92–1.72) | 0.148 | 1.26 (0.97–1.65) | 0.08 |
| Control | 1.17 | 1 | 1 | |||
| Underweight (n = 2732) | ||||||
| Gout | 1.51 | 0.32 (−1.31 to 1.95) | 1.28 (0.38–4.33) | 0.690 | 0.98 (0.41–2.34) | 0.972 |
| Control | 1.19 | 1 | 1 | |||
| Normal weight (n = 29,706) | ||||||
| Gout | 0.95 | 0.03 (−0.28 to 0.34) | 1.03 (0.74–1.43) | 0.866 | 1.06 (0.83–1.34) | 0.656 |
| Control | 0.92 | 1 | 1 | |||
| Overweight (n = 39,001) | ||||||
| Gout | 0.98 | 0.07 (−0.23 to 0.37) | 1.07 (0.78–1.47) | 0.663 | 1.03 (0.79–1.33) | 0.838 |
| Control | 0.91 | 1 | 1 | |||
| Obese I (n = 40,572) | ||||||
| Gout | 1.18 | 0.13 (−0.14 to 0.39) | 1.12 (0.88–1.43) | 0.342 | 1.12 (0.91–1.38) | 0.299 |
| Control | 1.05 | 1 | 1 | |||
| Obese II (n = 3456) | ||||||
| Gout | 1.19 | −0.35 (−1.38 to 0.67) | 0.77 (0.36–1.64) | 0.503 | 0.79 (0.4–1.55) | 0.489 |
| Control | 1.54 | 1 | 1 | |||
| Fasting blood glucose < 100 mg/dL (n = 68,732) | ||||||
| Gout | 1.05 | 0.04 (−0.17 to 0.25) | 1.04 (0.85–1.28) | 0.682 | 1.02 (0.86–1.20) | 0.815 |
| Control | 1.00 | 1 | 1 | |||
| Fasting blood glucose ≥ 100 mg/dL (n = 50,353) | ||||||
| Gout | 1.12 | 0.17 (−0.09 to 0.42) | 1.17 (0.91–1.51) | 0.208 | 1.11 (0.9–1.36) | 0.336 |
| Control | 0.95 | 1 | 1 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.G.; Kim, S.Y.; Chung, J. The Risk of BPPV, Meniere’s Disease, and Vestibular Neuronitis in Patients with Gout: A Longitudinal Follow-Up Study Using a National Health Screening Cohort. J. Clin. Med. 2023, 12, 185. https://doi.org/10.3390/jcm12010185
Choi HG, Kim SY, Chung J. The Risk of BPPV, Meniere’s Disease, and Vestibular Neuronitis in Patients with Gout: A Longitudinal Follow-Up Study Using a National Health Screening Cohort. Journal of Clinical Medicine. 2023; 12(1):185. https://doi.org/10.3390/jcm12010185
Chicago/Turabian StyleChoi, Hyo Geun, So Young Kim, and Juyong Chung. 2023. "The Risk of BPPV, Meniere’s Disease, and Vestibular Neuronitis in Patients with Gout: A Longitudinal Follow-Up Study Using a National Health Screening Cohort" Journal of Clinical Medicine 12, no. 1: 185. https://doi.org/10.3390/jcm12010185
APA StyleChoi, H. G., Kim, S. Y., & Chung, J. (2023). The Risk of BPPV, Meniere’s Disease, and Vestibular Neuronitis in Patients with Gout: A Longitudinal Follow-Up Study Using a National Health Screening Cohort. Journal of Clinical Medicine, 12(1), 185. https://doi.org/10.3390/jcm12010185