
Cardiovascular Risk Perception and Knowledge among Italian Women: Lessons from IGENDA Protocol

 ,
,  , , , ,
, , , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Structure of the Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Respondents
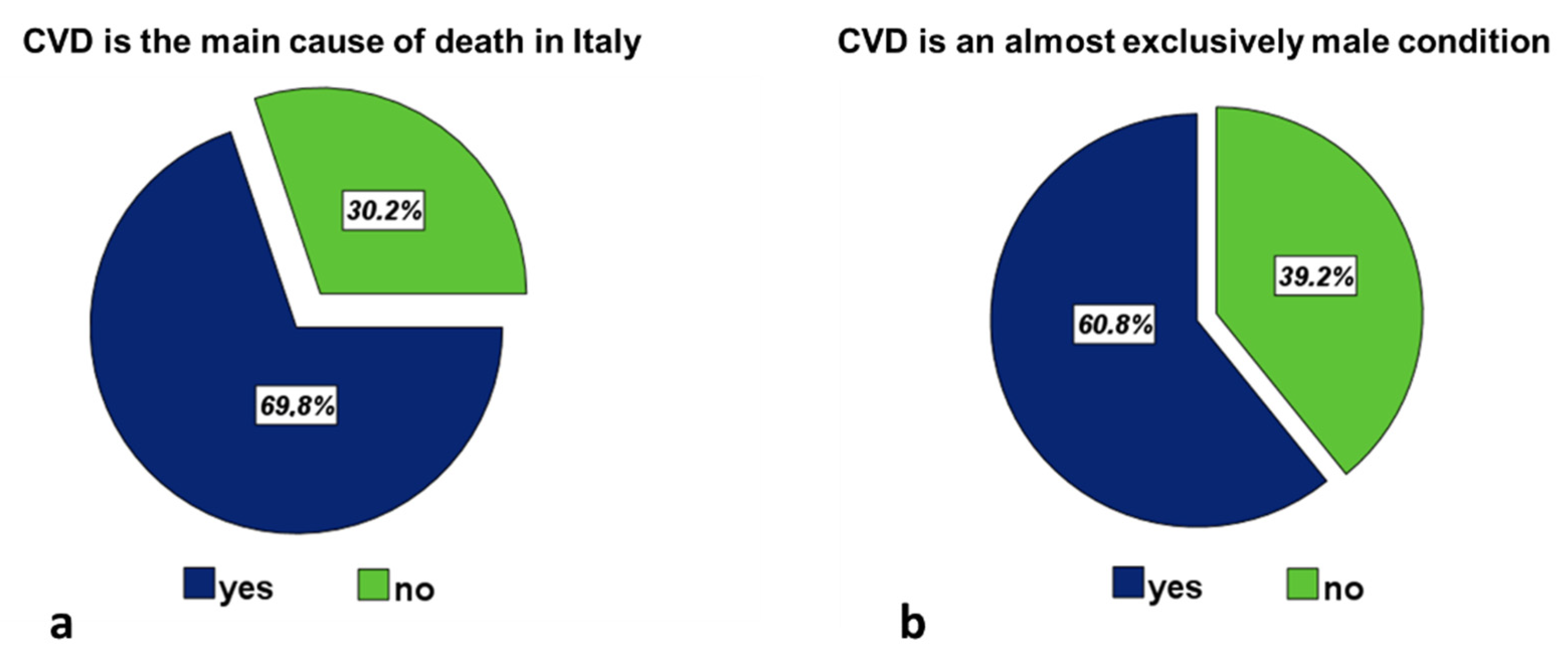
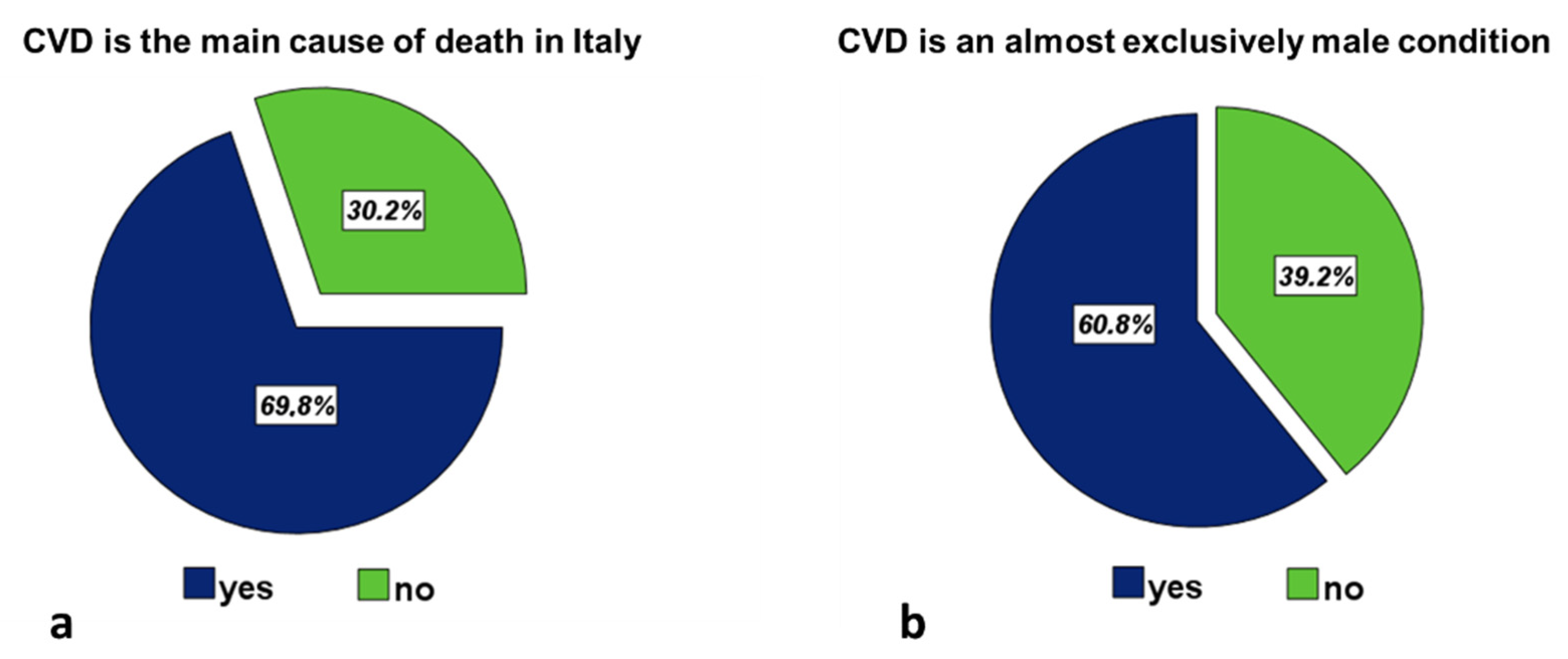
3.2. Knowledge of CVD
3.3. Knowledge of the Main CVRF
3.4. Self-Rating of Health
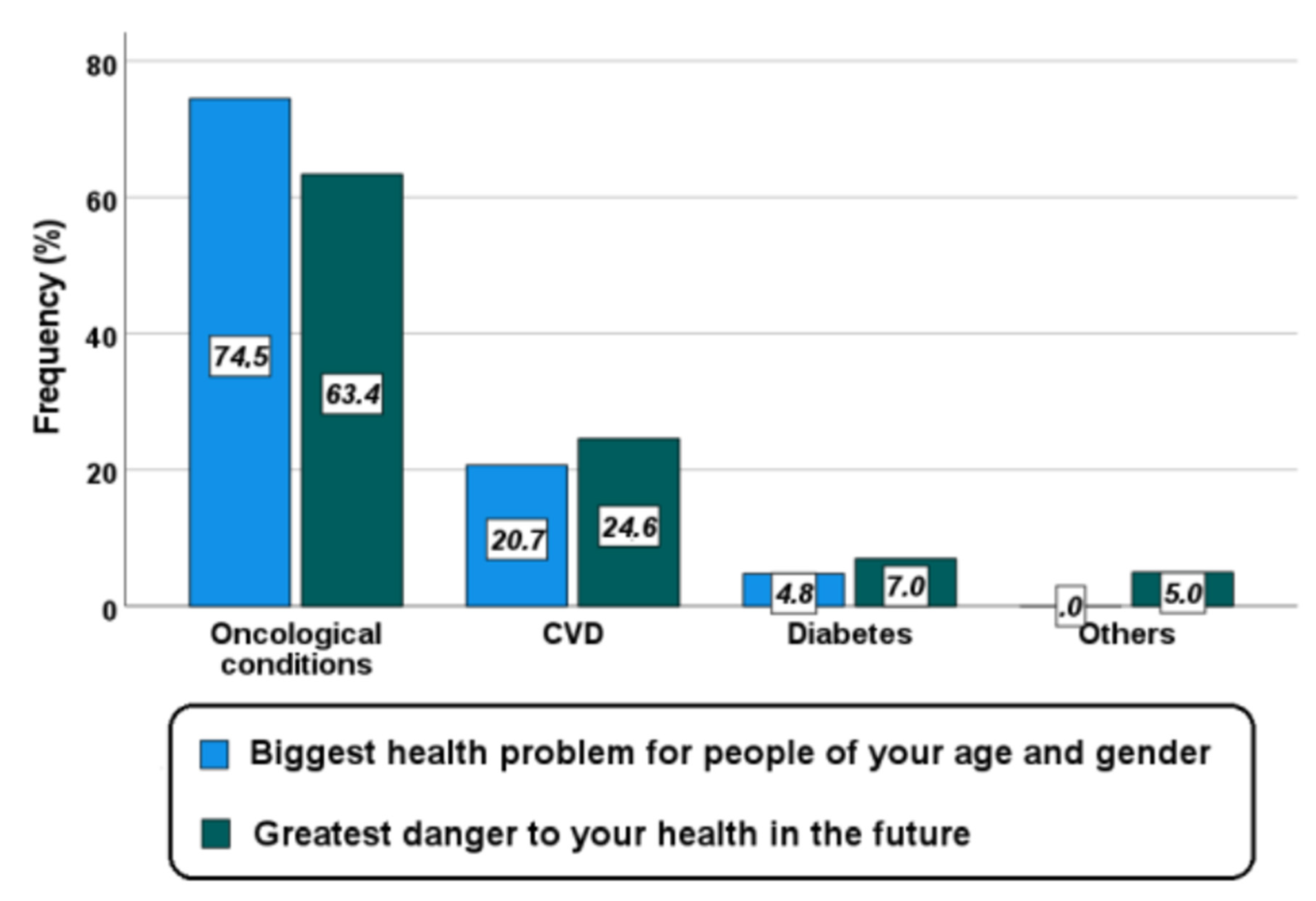
3.5. Perception of CVD Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cannon, C.P. Cardiovascular disease and modifiable cardiometabolic risk factors. Clin. Cornerstone 2007, 8, 11–28. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Sciomer, S.; Moscucci, F.; Maiello, M.; Cugusi, L.; Gallina, S.; Dei Cas, A.; Lombardi, C.; Pengo, M.; Parati, G.; et al. Cardiovascular prevention in women: A narrative review from the Italian Society of Cardiology working groups on ‘Cardiovascular Prevention, Hypertension and peripheral circulation’ and on ‘Women Disease’. J. Cardiovasc. Med. (Hagerstown) 2019, 20, 575–583. [Google Scholar] [CrossRef]
- Song, P.S.; Kim, M.J.; Seong, S.-W.; Choi, S.W.; Gwon, H.-C.; Hur, S.-H.; Rha, S.-W.; Yoon, C.-H.; Jeong, M.H.; Jeong, J.-O.; et al. Gender Differences in All-Cause Mortality after Acute Myocardial Infarction: Evidence for a Gender–Age Interaction. J. Clin. Med. 2022, 11, 541. [Google Scholar] [CrossRef]
- Conroy, R.M.; Pyorala, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetiere, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Wilson, P.W.; Castelli, W.P.; Kannel, W.B. Coronary risk prediction in adults (the Framingham Heart Study). Am. J. Cardiol. 1987, 59, G91–G94. [Google Scholar] [CrossRef]
- Alm-Roijer, C.; Fridlund, B.; Stagmo, M.; Erhardt, L. Knowing your risk factors for coronary heart disease improves adherence to advice on lifestyle changes and medication. J. Cardiovasc. Nurs. 2006, 21, E24–E31. [Google Scholar] [CrossRef]
- Mosca, L.; Jones, W.K.; King, K.B.; Ouyang, P.; Redberg, R.F.; Hill, M.N. Awareness, perception, and knowledge of heart disease risk and prevention among women in the United States. American Heart Association Women’s Heart Disease and Stroke Campaign Task Force. Arch. Fam. Med. 2000, 9, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Alm-Roijer, C.; Stagmo, M.; Udén, G.; Erhardt, L. Better knowledge improves adherence to lifestyle changes and medication in patients with coronary heart disease. Eur. J. Cardiovasc. Nurs. 2004, 3, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Ciambrone, G.; Kaski, J.C. The importance of gender differences in the diagnosis and management of cardiovascular disease. Curr. Pharm. Des. 2011, 17, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Maffei, S.; Guiducci, L.; Cugusi, L.; Cadeddu, C.; Deidda, M.; Gallina, S.; Sciomer, S.; Gastaldelli, A.; Kaski, J.C. Working Group on “Gender difference in cardiovascular disease” of the Italian Society of, C. Women-specific predictors of cardiovascular disease risk-New paradigms. Int. J. Cardiol. 2019, 286, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Arnott, C.; Patel, S.; Hyett, J.; Jennings, G.; Woodward, M.; Celermajer, D.S. Women and Cardiovascular Disease: Pregnancy, the Forgotten Risk Factor. Heart Lung Circ. 2020, 29, 662–667. [Google Scholar] [CrossRef]
- Arnott, C.; Nelson, M.; Alfaro Ramirez, M.; Hyett, J.; Gale, M.; Henry, A.; Celermajer, D.S.; Taylor, L.; Woodward, M. Maternal cardiovascular risk after hypertensive disorder of pregnancy. Heart 2020, 106, 1927–1933. [Google Scholar] [CrossRef]
- Mosca, L.; Ferris, A.; Fabunmi, R.; Robertson, R.M.; American Heart, A. Tracking women’s awareness of heart disease: An American Heart Association national study. Circulation 2004, 109, 573–579. [Google Scholar] [CrossRef] [Green Version]
- Mosca, L.; Mochari, H.; Christian, A.; Berra, K.; Taubert, K.; Mills, T.; Burdick, K.A.; Simpson, S.L. National study of women’s awareness, preventive action, and barriers to cardiovascular health. Circulation 2006, 113, 525–534. [Google Scholar] [CrossRef]
- Lynch, E.B.; Liu, K.; Kiefe, C.I.; Greenland, P. Cardiovascular disease risk factor knowledge in young adults and 10-year change in risk factors: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am. J. Epidemiol. 2006, 164, 1171–1179. [Google Scholar] [CrossRef]
- McDonnell, L.A.; Pipe, A.L.; Westcott, C.; Perron, S.; Younger-Lewis, D.; Elias, N.; Nooyen, J.; Reid, R.D. Perceived vs. actual knowledge and risk of heart disease in women: Findings from a Canadian survey on heart health awareness, attitudes, and lifestyle. Can. J. Cardiol. 2014, 30, 827–834. [Google Scholar] [CrossRef]
- McKenzie, C.; Skelly, A.H. Perceptions of coronary heart disease risk in African American women with type 2 diabetes: A qualitative study. Diabetes Educ. 2010, 36, 766–773. [Google Scholar] [CrossRef]
- Haidinger, T.; Zweimüller, M.; Stütz, L.; Demir, D.; Kaider, A.; Strametz-Juranek, J. Effect of gender on awareness of cardiovascular risk factors, preventive action taken, and barriers to cardiovascular health in a group of Austrian subjects. Gend. Med. 2012, 9, 94–102. [Google Scholar] [CrossRef]
- Hoare, E.; Stavreski, B.; Kingwell, B.A.; Jennings, G.L. Australian adults’ behaviours, knowledge and perceptions of risk factors for heart disease: A cross-sectional study. Prev. Med. Rep. 2017, 8, 204–209. [Google Scholar] [CrossRef]
- Lange, J.; Evans-Benard, S.; Cooper, J.; Fahey, E.; Kalapos, M.; Tice, D.; Wang-D’Amato, N.; Watsky, N. Puerto Rican Women’s Perceptions of Heart Disease Risk. Clin. Nurs. Res. 2009, 18, 291–306. [Google Scholar] [CrossRef]
- Mochari, H.; Ferris, A.; Adigopula, S.; Henry, G.; Mosca, L. Cardiovascular disease knowledge, medication adherence, and barriers to preventive action in a minority population. Prev. Cardiol. 2007, 10, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Mosca, L.; Mochari-Greenberger, H.; Dolor, R.J.; Newby, L.K.; Robb, K.J. Twelve-year follow-up of American women’s awareness of cardiovascular disease risk and barriers to heart health. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 120–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bairey Merz, C.N.; Andersen, H.; Sprague, E.; Burns, A.; Keida, M.; Walsh, M.N.; Greenberger, P.; Campbell, S.; Pollin, I.; McCullough, C.; et al. Knowledge, Attitudes, and Beliefs Regarding Cardiovascular Disease in Women: The Women’s Heart Alliance. J. Am. Coll. Cardiol. 2017, 70, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Christian, A.H.; Rosamond, W.; White, A.R.; Mosca, L. Nine-year trends and racial and ethnic disparities in women’s awareness of heart disease and stroke: An American Heart Association national study. J. Womens Health (Larchmt) 2007, 16, 68–81. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, L.M.; Di Giuseppe, G.; Napolitano, F.; Angelillo, I.F. Cardiovascular diseases and women: Knowledge, attitudes, and behavior in the general population in Italy. BioMed Res. Int. 2015, 2015, 324692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffei, S.; Cugusi, L.; Meloni, A.; Deidda, M.; Colasante, E.; Marchioli, R.; Surico, N.; Mercuro, G. IGENDA protocol: Gender differences in awareness, knowledge and perception of cardiovascular risk: An Italian multicenter study. J. Cardiovasc. Med. (Hagerstown) 2019, 20, 278–283. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed] [Green Version]
- Mosca, L.; Hammond, G.; Mochari-Greenberger, H.; Towfighi, A.; Albert, M.A. Fifteen-year trends in awareness of heart disease in women: Results of a 2012 American Heart Association national survey. Circulation 2013, 127, 1254–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winham, D.M.; Jones, K.M. Knowledge of young African American adults about heart disease: A cross-sectional survey. BMC Public Health 2011, 11, 248. [Google Scholar] [CrossRef] [Green Version]
- Crouch, R.; Wilson, A. An exploration of rural women’s knowledge of heart disease and the association with lifestyle behaviours. Int. J. Nurs. Pract. 2011, 17, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Mazalin Protulipac, J.; Sonicki, Z.; Reiner, Ž. Cardiovascular disease (CVD) risk factors in older adults-Perception and reality. Arch. Gerontol. Geriatr. 2015, 61, 88–92. [Google Scholar] [CrossRef]
- Nicklas, J.M.; Zera, C.A.; Seely, E.W.; Abdul-Rahim, Z.S.; Rudloff, N.D.; Levkoff, S.E. Identifying postpartum intervention approaches to prevent type 2 diabetes in women with a history of gestational diabetes. BMC Pregnancy Childbirth 2011, 11, 23. [Google Scholar] [CrossRef] [Green Version]
- Seely, E.W.; Rich-Edwards, J.; Lui, J.; Nicklas, J.M.; Saxena, A.; Tsigas, E.; Levkoff, S.E. Risk of future cardiovascular disease in women with prior preeclampsia: A focus group study. BMC Pregnancy Childbirth 2013, 13, 240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanojevic Jerkovic, O.; Sauliune, S.; Sumskas, L.; Birt, C.A.; Kersnik, J. Determinants of self-rated health in elderly populations in urban areas in Slovenia, Lithuania and UK: Findings of the EURO-URHIS 2 survey. Eur. J. Public Health 2017, 27, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Andersen, F.K.; Christensen, K.; Frederiksen, H. Self-rated health and age: A cross-sectional and longitudinal study of 11,000 Danes aged 45—102. Scand. J. Public Health 2007, 35, 164–171. [Google Scholar] [CrossRef]
- Berdahl, T.A.; McQuillan, J. Self-Rated Health Trajectories among Married Americans: Do Disparities Persist over 20 Years? J. Aging Res. 2018, 2018, 1208598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veromaa, V.; Kautiainen, H.; Juonala, M.; Rantanen, A.; Korhonen, P.E. Self-rated health as an indicator of ideal cardiovascular health among working-aged women. Scand. J. Prim. Health Care 2017, 35, 322–328. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, S.; Slovic, P.; Fischhoff, B.; Layman, M.; Combs, B. Judged frequency of lethal events. J. Exp.Psychol. Hum. Learn. Mem. 1978, 4, 551–578. [Google Scholar] [CrossRef]
- van der Pligt, J. Risk appraisal and health behaviour. In Social Psychology and Health: European Perspectives; Avebury/Ashgate Publishing Co.: Brookfield, VT, USA, 1994; pp. 131–151. [Google Scholar]

{kind=link}
{kind=link}
| Age Group | n (%) |
|---|---|
| <30 years | 820 (18.4) |
| 30–39 years | 851 (19.1) |
| 40–49 years | 1011 (22.7) |
| 50–59 years | 1149 (25.8) |
| ≥60 years | 623 (14.0) |
| Cardiovascular risk factors | n (%) |
| Yes | 2592 (58.2) |
| Cardiovascular disease | n (%) |
| Yes | 125 (2.8) |
| Highest educational level | n (%) |
| Lower secondary school or less | 1114 (25.0) |
| High school | 1897 (42.6) |
| University | 1443 (32.4) |
| CVRF | Correctly Identified n (%) | Age (Years) | Level of Schooling | CVRF c | CVD d | ||||
|---|---|---|---|---|---|---|---|---|---|
| 30–40 a | 40–50 a | 50–60 a | ≥60 a | High School b | University b | ||||
| OR (95%CI) p-Value | OR (95%CI) p-Value | OR (95%CI) p-Value | OR (95%CI) p-Value | OR (95%CI) p-Value | OR (95%CI) p-Value | OR (95%CI) p-Value | OR (95%CI) p-Value | ||
| Family CVD history | 3804 (85.4) | 1.02 (0.78–1.35) p = 0.844 | 1.12 (0.86–1.46) p = 0.416 | 0.95 (0.74–1.22) p = 0.668 | 1.51 (1.09–2.09) p = 0.014 | 1.64 (1.33–2.02) p < 0.0001 | 2.68 (2.09–3.43) p < 0.0001 | 1.31 (1.08–1.60) p = 0.007 | 1.11 (0.63–1.96) p = 0.725 |
| Smoke | 4343 (97.5) | 1.34 (0.76–2.36) p = 0.312 | 1.20 (0.71–2.04) p = 0.491 | 3.09 (1.59–6.01) p = 0.001 | 1.54 (0.80–2.95) p = 0.194 | 1.75 (1.09–2.81) p = 0.021 | 1.72 (1.03–2.86) p = 0.037 | 1.44 (0.93–2.24) p = 0.107 | 2.77 (0.38–20.08) p = 0.313 |
| High blood pressure | 4316 (96.9) | 1.42 (0.89–2.27) p = 0.141 | 1.88 (1.16–3.04) p = 0.010 | 3.72 (2.10–6.57) p < 0.0001 | 2.84 (1.48–5.43) p = 0.002 | 1.94 (1.31–2.88) p = 0.001 | 3.19 (1.94–5.24) p < 0.0001 | 1.32 (0.90–1.93) p = 0.150 | 3.58 (0.49–25.88) p = 0.206 |
| High cholesterol | 4271 (95.9) | 0.97 (0.63–1.49) p = 0.875 | 1.24 (0.80–1.92) p = 0.335 | 2.34 (1.37–3.66) p = 0.001 | 1.72 (0.99–2.99) p = 0.055 | 1.92 (1.35–2.74) p < 0.0001 | 3.32 (2.12–5.19) p < 0.0001 | 1.70 (1.19–2.44) p = 0.004 | 2.16 (0.53–8.86) p = 0.283 |
| Overweight | 4360 (97.9) | 1.62 (0.80–3.29) p = 0.178 | 1.47 (0.76–2.82) p = 0.251 | 1.57 (0.82–2.98) p = 0.172 | 0.88 (0.45–1.70) p = 0.884 | 2.23 (1.37–3.62) p = 0.001 | 3.94 (2.09–7.43) p < 0.0001 | 0.54 (0.52–1.40) p = 0.536 | 0.86 (0.52–1.40) p = 0.536 |
| Physical inactivity | 4258 (95.6) | 1.55 (1.00–2.42) p = 0.050 | 1.86 (1.19–2.88) p = 0.006 | 1.83 (1.19–2.80) p = 0.005 | 1.44 (0.89–2.33) p = 0.133 | 1.44 (1.02–2.03) p = 0.039 | 2.35 (1.55–3.58) p < 0.0001 | 0.97 (0.69–1.37) p = 0.874 | 2.30 (0.56–9.43) p = 0.246 |
| Diabetes | 3910 (87.8) | 1.51 (1.13–2.02) p = 0.005 | 1.12 (0.86–1.45) p = 0.400 | 1.61 (1.23–2.11) p = 0.001 | 2.15 (1.51–3.07) p < 0.0001 | 1.13 (0.89–1.42) p = 0.321 | 1.71 (1.31–2.24) p < 0.0001 | 0.97 (0.78–1.21) p = 0.776 | 1.68 (0.81–3.49) p = 0.162 |
| Menopause | 3692 (82.9) | 0.87 (0.68–1.11) p = 0.266 | 0.91 (0.72–1.15) p = 0.437 | 1.99 (1.53–2.58) p < 0.0001 | 2.09 (1.52–2.87) p < 0.0001 | 1.39 (1.13–1.69) p = 0.002 | 1.96 (1.56–2.47) p < 0.0001 | 1.33 (1.11–1.61) p = 0.003 | 1.23 (0.71–2.14) p = 0.468 |
| SRH Status | p-Value | |||
|---|---|---|---|---|
| Poor | Acceptable | Good | ||
| Age (years) | 49.10 ± 15.16 | 46.54 ± 13.64 | 40.10 ± 12.93 | <0.0001 |
| CVRF % | 64.4 | 65.4 | 47.7 | <0.0001 |
| CVD % | 5.5 | 3.9 | 1.2 | <0.0001 |
| Perceived CVD Risk | p-Value | |||
|---|---|---|---|---|
| Low | Intermediate | High | ||
| Age (years) | 41.27 ± 13.79 | 46.08 ± 13.49 | 50.14 ± 14.56 | <0.0001 |
| CVRF % | 50.2 | 64.6 | 70 | <0.0001 |
| CVD % | 1.7 | 2.9 | 10.2 | <0.0001 |
| SRH status % | <0.0001 | |||
| Poor | 9.9 | 9.8 | 19.5 | |
| Acceptable | 40 | 55.9 | 51.4 | |
| Good | 50.1 | 34.4 | 29.1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maffei, S.; Meloni, A.; Deidda, M.; Sciomer, S.; Cugusi, L.; Cadeddu, C.; Gallina, S.; Franchini, M.; Scambia, G.; Mattioli, A.V.; et al. Cardiovascular Risk Perception and Knowledge among Italian Women: Lessons from IGENDA Protocol. J. Clin. Med. 2022, 11, 1695. https://doi.org/10.3390/jcm11061695
Maffei S, Meloni A, Deidda M, Sciomer S, Cugusi L, Cadeddu C, Gallina S, Franchini M, Scambia G, Mattioli AV, et al. Cardiovascular Risk Perception and Knowledge among Italian Women: Lessons from IGENDA Protocol. Journal of Clinical Medicine. 2022; 11(6):1695. https://doi.org/10.3390/jcm11061695
Chicago/Turabian StyleMaffei, Silvia, Antonella Meloni, Martino Deidda, Susanna Sciomer, Lucia Cugusi, Christian Cadeddu, Sabina Gallina, Michela Franchini, Giovanni Scambia, Anna Vittoria Mattioli, and et al. 2022. "Cardiovascular Risk Perception and Knowledge among Italian Women: Lessons from IGENDA Protocol" Journal of Clinical Medicine 11, no. 6: 1695. https://doi.org/10.3390/jcm11061695
APA StyleMaffei, S., Meloni, A., Deidda, M., Sciomer, S., Cugusi, L., Cadeddu, C., Gallina, S., Franchini, M., Scambia, G., Mattioli, A. V., Surico, N., Mercuro, G., & IGENDA Study Group, on behalf of the Italian Society of Cardiology (SIC) and the Italian Society of Obstetrics and Gynecology (SIGO). (2022). Cardiovascular Risk Perception and Knowledge among Italian Women: Lessons from IGENDA Protocol. Journal of Clinical Medicine, 11(6), 1695. https://doi.org/10.3390/jcm11061695