
State-of-the-Art Review on Immersive Virtual Reality Interventions for Colonoscopy-Induced Anxiety and Pain

 ,
, 
 , ,
, ,
Abstract
:
1. Introduction
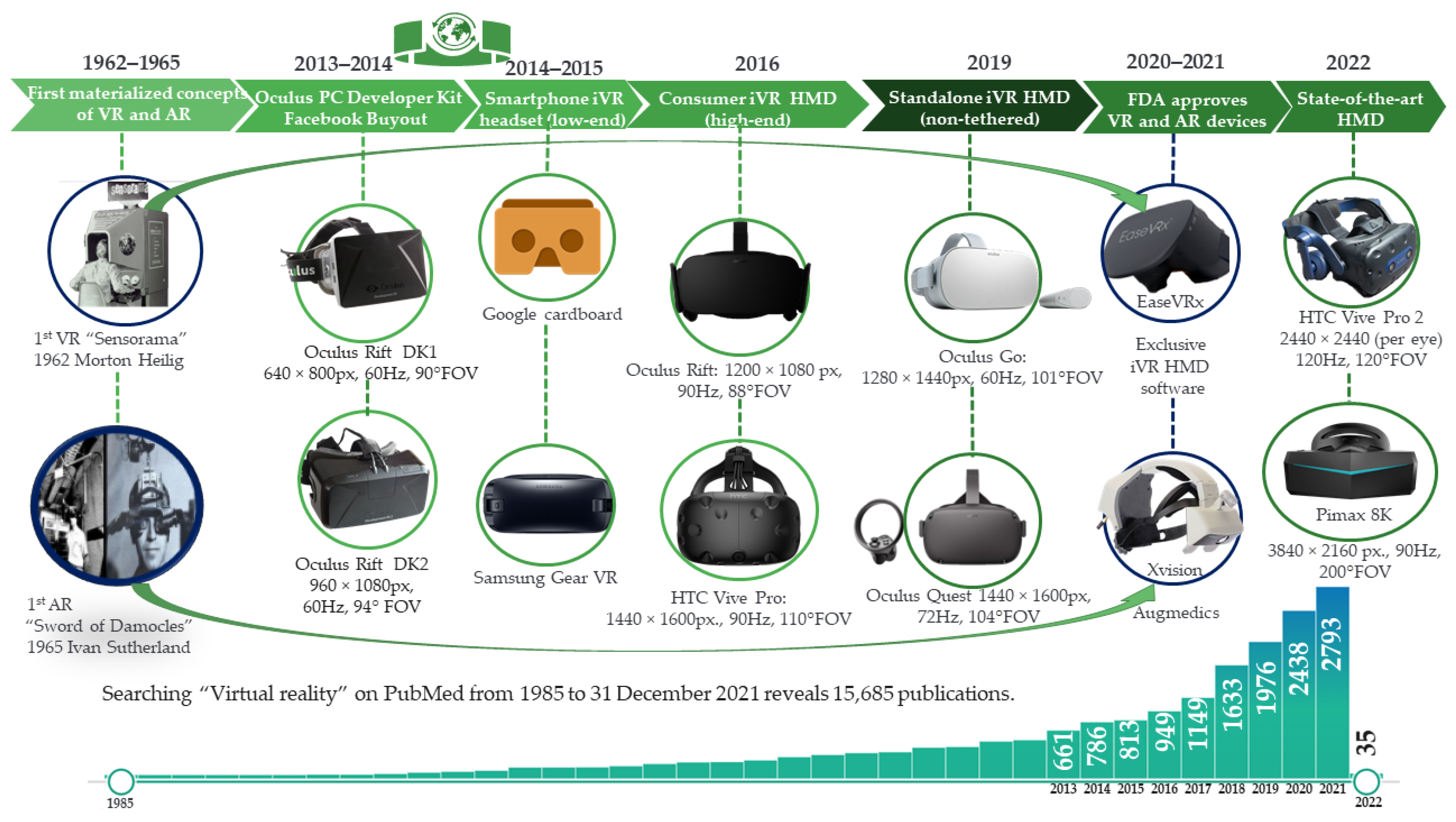
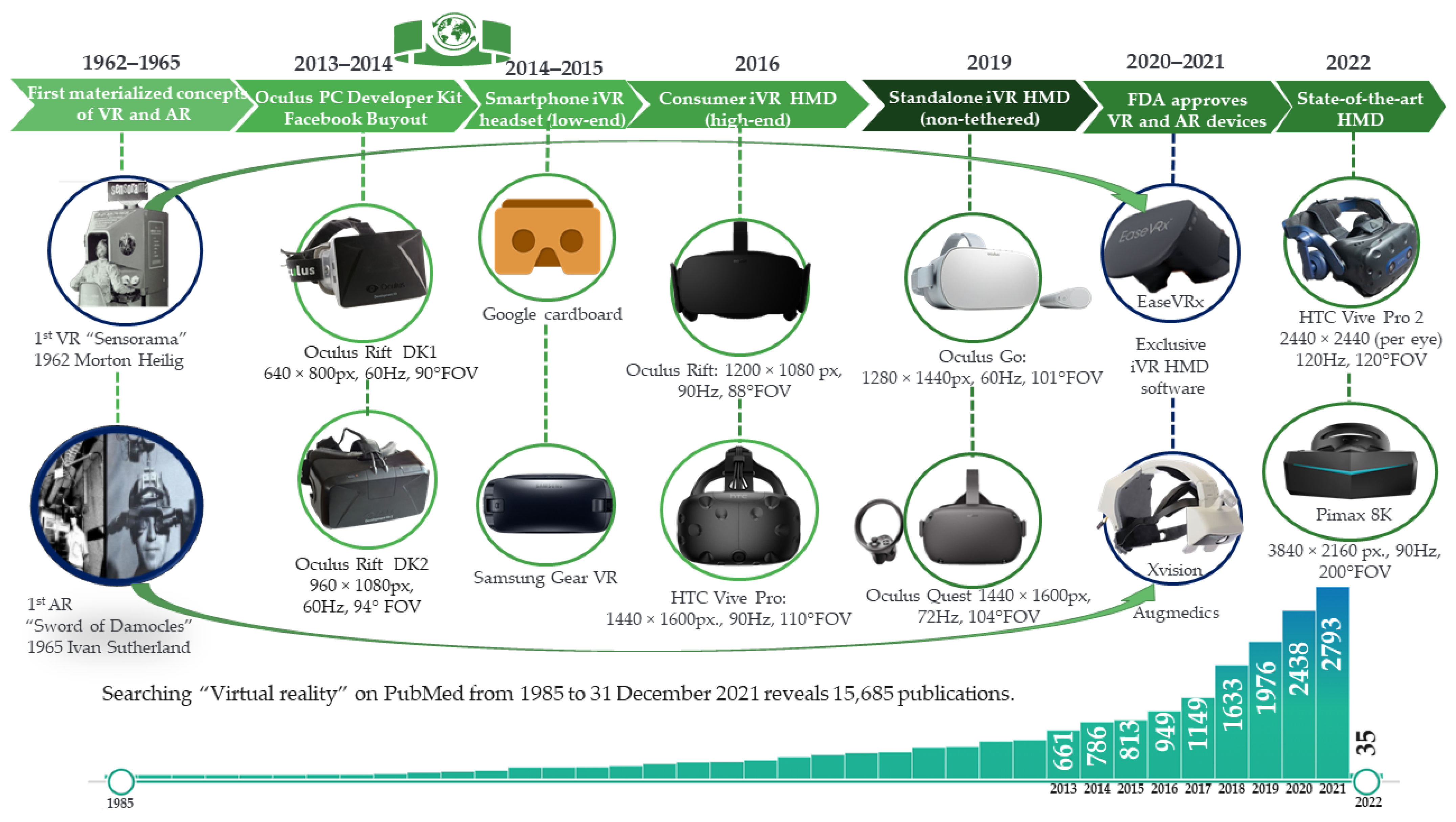
- AR: In 1966, Ivan Sutherland imagined an “ultimate display”, but the lack of graphical processing power determined a resemblance of a primitive form of AR through the first Head Mounted Display (HMD) [17]. Sutherland’s device was backed by a large and heavy computer and mechanism that provided its invention with the name “Sword of Damocles” [18]. Then, 54 years later, on 11 June 2020, Xvision Augmedics AR HMD was approved by the United States Food and Drug Administration (U.S. FDA) for intra-operative use, offering real-time visualisation of individual anatomy of the patient reconstructed from previous scans and therefore facilitating precision in screw insertion [19].
- VR: Through “Sensorama”, Morton Heilig created in 1962 the first interactive, immersive VR (iVR) all-in-one system, meant to capture all senses of the user, from dynamic visuals, auditory, olfactive, and even vibratory sensation [20]. In November 2021, U.S. FDA authorised EaseVRx, a remote cognitive-behavioural approach targeting chronic back pain delivered through an iVR HMD [21].
2. Materials and Methods
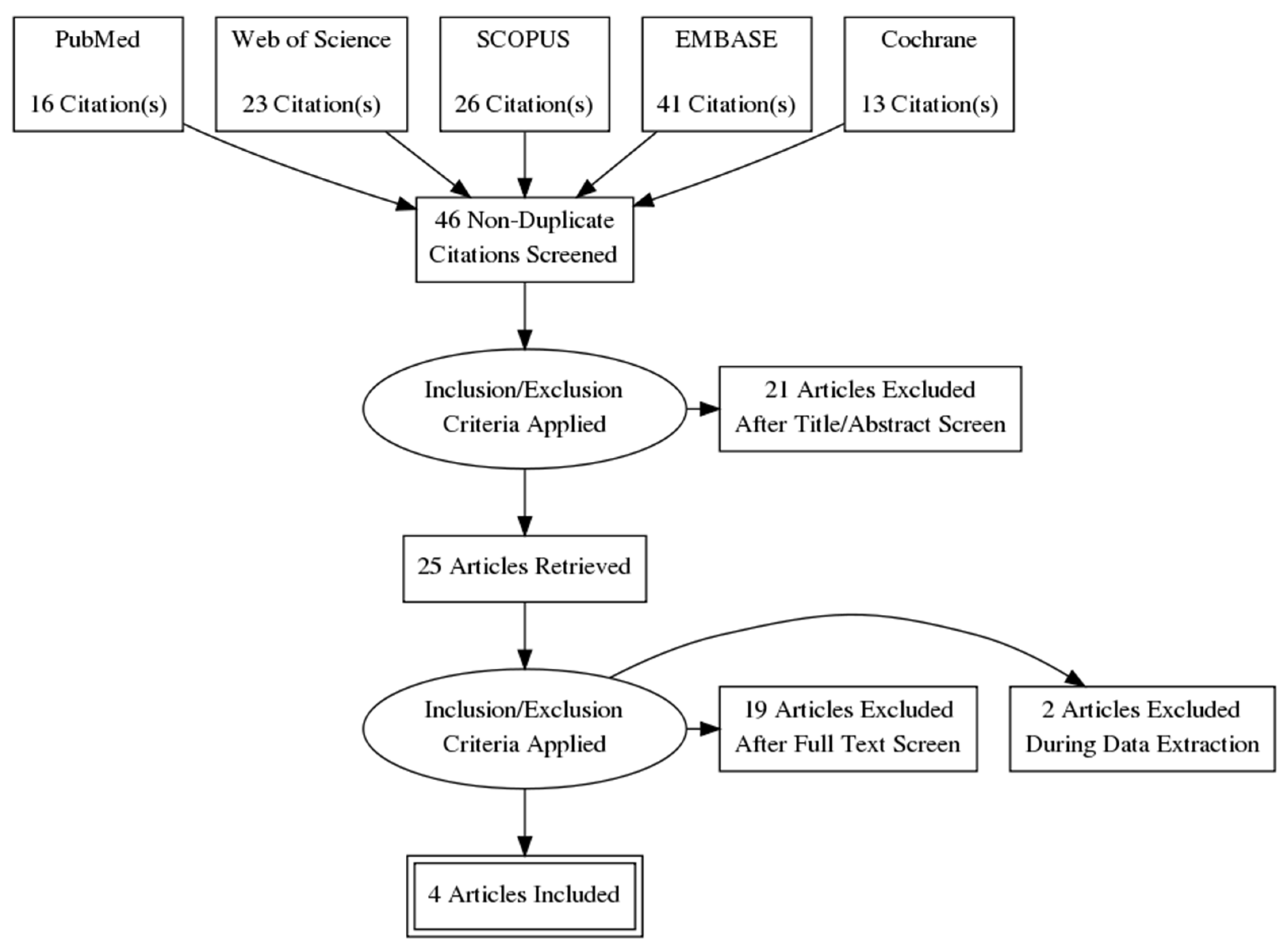
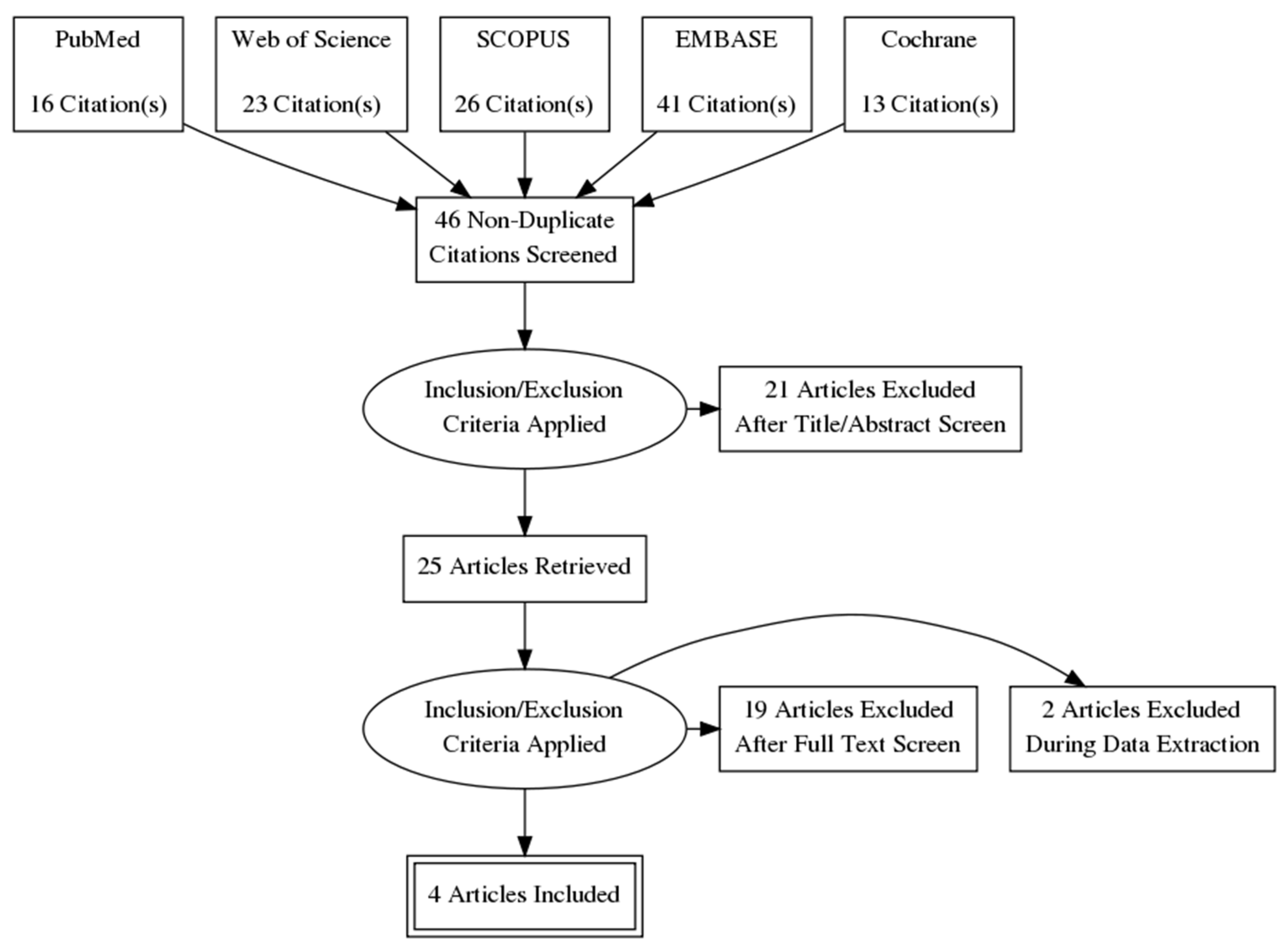
2.1. Electronic Searches
2.2. Study Selection
3. Results
3.1. Virtual Reality as a Therapy for Reducing the Anxiety of Patients during a Colonoscopy Procedure
3.2. iVR Education Reduces Anxiety of Patients before Colonoscopy
4. Discussion
4.1. iVR as an Alternative to Sedation during Colonoscopy
4.2. iVR Education for Bowel Preparation in Reducing Anxiety before Colonoscopy
4.3. How Colonoscopy Can Progress through the Implementation of iVR
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bhise, V.; Modi, V.; Kalavar, A.; Espadas, D.; Hanser, L.; Gould, M.; El-Serag, H.B.; Singh, H. Patient-Reported Attributions for Missed Colonoscopy Appointments in Two Large Healthcare Systems. Dig. Dis. Sci. 2016, 61, 1853–1861. [Google Scholar] [CrossRef] [PubMed]
- Braithwaite, E.; Carbonell, J.; Kane, J.S.; Gracie, D.; Selinger, C.P. Patients’ Perception of Colonoscopy and Acceptance of Colonoscopy Based IBD Related Colorectal Cancer Surveillance. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Shafer, L.A.; Walker, J.R.; Waldman, C.; Yang, C.; Michaud, V.; Bernstein, C.N.; Hathout, L.; Park, J.; Sisler, J.; Restall, G.; et al. Factors Associated with Anxiety About Colonoscopy: The Preparation, the Procedure, and the Anticipated Findings. Dig. Dis. Sci. 2018, 63, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Aljebreen, A.M.; Almadi, M.A.; Leung, F.W. Sedated vs Unsedated Colonoscopy: A Prospective Study. World J. Gastroenterol. WJG 2014, 20, 5113–5118. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.N.; Ferrari, A.; Hoeck, S.; Peeters, M.; Van Hal, G. Colorectal Cancer Screening: Have We Addressed Concerns and Needs of the Target Population? Gastrointest. Disord. 2021, 3, 173–203. [Google Scholar] [CrossRef]
- Levin, T.R. Beyond Colonoscopy: The Role of Alternative Screening Tests for Colorectal Cancer in Your Practice. Am. J. Gastroenterol. 2017, 112, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Ferlizza, E.; Solmi, R.; Sgarzi, M.; Ricciardiello, L.; Lauriola, M. The Roadmap of Colorectal Cancer Screening. Cancers 2021, 13, 1101. [Google Scholar] [CrossRef] [PubMed]
- Anghel, S.A.; Ioniță-Mîndrican, C.-B.; Luca, I.; Pop, A.L. Promising Epigenetic Biomarkers for the Early Detection of Colorectal Cancer: A Systematic Review. Cancers 2021, 13, 4965. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Neefs, I.; Hoeck, S.; Peeters, M.; Van Hal, G. Towards Novel Non-Invasive Colorectal Cancer Screening Methods: A Comprehensive Review. Cancers 2021, 13, 1820. [Google Scholar] [CrossRef] [PubMed]
- Spada, C.; Hassan, C.; Bellini, D.; Burling, D.; Cappello, G.; Carretero, C.; Dekker, E.; Eliakim, R.; de Haan, M.; Kaminski, M.F.; et al. Imaging Alternatives to Colonoscopy: CT Colonography and Colon Capsule. European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Gastrointestinal and Abdominal Radiology (ESGAR) Guideline—Update 2020. Endoscopy 2020, 52, 1127–1141. [Google Scholar] [CrossRef]
- Suffeda, A.; Meissner, W.; Rosendahl, J.; Guntinas-Lichius, O. Influence of Depression, Catastrophizing, Anxiety, and Resilience on Postoperative Pain at the First Day after Otolaryngological Surgery. Medicine 2016, 95, e4256. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Sriranjan, V.; Abou-Setta, A.M.; Poluha, W.; Walker, J.R.; Singh, H. Anxiety Associated with Colonoscopy and Flexible Sigmoidoscopy: A Systematic Review. Am. J. Gastroenterol. 2018, 113, 1810–1818. [Google Scholar] [CrossRef] [PubMed]
- Hassan, C.; Antonelli, G. I Want to Have Virtual Reality Distraction during My Colonoscopy! Endosc. Int. Open 2020, 8, E1389–E1391. [Google Scholar] [CrossRef] [PubMed]
- Gams, M.; Kolenik, T. Relations between Electronics, Artificial Intelligence and Information Society through Information Society Rules. Electronics 2021, 10, 514. [Google Scholar] [CrossRef]
- Xiong, J.; Hsiang, E.-L.; He, Z.; Zhan, T.; Wu, S.-T. Augmented Reality and Virtual Reality Displays: Emerging Technologies and Future Perspectives. Light Sci. Appl. 2021, 10, 216. [Google Scholar] [CrossRef]
- Sutherland, J.; Belec, J.; Sheikh, A.; Chepelev, L.; Althobaity, W.; Chow, B.J.W.; Mitsouras, D.; Christensen, A.; Rybicki, F.J.; La Russa, D.J. Applying Modern Virtual and Augmented Reality Technologies to Medical Images and Models. J. Digit. Imaging 2019, 32, 38–53. [Google Scholar] [CrossRef]
- Botella, C.; Baños, R.M.; García-Palacios, A.; Quero, S. Virtual Reality and Other Realities. In The Science of Cognitive Behavioral Therapy; Elsevier Academic Press: San Diego, CA, USA, 2017; pp. 551–590. ISBN 978-0-12-803457-6. [Google Scholar]
- Hersh, A.; Mahapatra, S.; Weber-Levine, C.; Awosika, T.; Theodore, J.N.; Zakaria, H.M.; Liu, A.; Witham, T.F.; Theodore, N. Augmented Reality in Spine Surgery: A Narrative Review. HSS J. Musculoskelet. J. Hosp. Spec. Surg. 2021, 17, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Basso, A. Advantages, Critics and Paradoxes of Virtual Reality Applied to Digital Systems of Architectural Prefiguration, the Phenomenon of Virtual Migration. Proceedings 2017, 1, 915. [Google Scholar] [CrossRef] [Green Version]
- Garcia, L.M.; Birckhead, B.J.; Krishnamurthy, P.; Sackman, J.; Mackey, I.G.; Louis, R.G.; Salmasi, V.; Maddox, T.; Darnall, B.D. An 8-Week Self-Administered At-Home Behavioral Skills-Based Virtual Reality Program for Chronic Low Back Pain: Double-Blind, Randomized, Placebo-Controlled Trial Conducted During COVID-19. J. Med. Internet Res. 2021, 23, e26292. [Google Scholar] [CrossRef]
- Tamang, L.D.; Kim, B.W. Deep Learning Approaches to Colorectal Cancer Diagnosis: A Review. Appl. Sci. 2021, 11, 10982. [Google Scholar] [CrossRef]
- Rauschnabel, P.A. Augmented Reality Is Eating the Real-World! The Substitution of Physical Products by Holograms. Int. J. Inf. Manag. 2021, 57, 102279. [Google Scholar] [CrossRef]
- Kılıç, A.; Brown, A.; Aras, I.; Hui, R.; Hare, J.; Hughes, L.D.; McCracken, L.M. Using Virtual Technology for Fear of Medical Procedures: A Systematic Review of the Effectiveness of Virtual Reality-Based Interventions. Ann. Behav. Med. Publ. Soc. Behav. Med. 2021, 55, 1062–1079. [Google Scholar] [CrossRef] [PubMed]
- Georgescu, R.; Fodor, L.A.; Dobrean, A.; Cristea, I.A. Psychological Interventions Using Virtual Reality for Pain Associated with Medical Procedures: A Systematic Review and Meta-Analysis. Psychol. Med. 2020, 50, 1795–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eijlers, R.; Dierckx, B.; Staals, L.M.; Berghmans, J.M.; van der Schroeff, M.P.; Strabbing, E.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Legerstee, J.S.; Utens, E.M.W.J. Virtual Reality Exposure before Elective Day Care Surgery to Reduce Anxiety and Pain in Children: A Randomized Controlled Trial. Eur. J. Anaesthesiol. 2019, 36, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Nordgård, R.; Låg, T. The Effects of Virtual Reality on Procedural Pain and Anxiety in Pediatrics: A Systematic Review and Meta-Analysis. Front. Virtual Real. 2021, 2, 95. [Google Scholar] [CrossRef]
- Koo, C.-H.; Park, J.-W.; Ryu, J.-H.; Han, S.-H. The Effect of Virtual Reality on Preoperative Anxiety: A Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 3151. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veldhuijzen, G.; Klaassen, N.J.M.; Van Wezel, R.J.A.; Drenth, J.P.H.; Van Esch, A.A. Virtual Reality Distraction for Patients to Relieve Pain and Discomfort during Colonoscopy. Endosc. Int. Open 2020, 8, E959–E966. [Google Scholar] [CrossRef]
- Cakir, S.K.; Evirgen, S. The Effect of Virtual Reality on Pain and Anxiety During Colonoscopy: A Randomized Controlled Trial. Turk. J. Gastroenterol. 2021, 32, 451–457. [Google Scholar] [CrossRef]
- Friedman, M.; Rand, K.; Patel, T.; Colizzo, F.; Carolan, P.; Kelsey, P.; Chung, D.C. A Pilot Study of Virtual Reality as an Alternative to Pharmacological Sedation during Colonoscopy. Endosc. Int. Open 2021, 9, E343–E347. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Zhao, Y.; Xie, F.; Shi, W.; Yang, Y.; Yang, A.; Wu, D. Educating Outpatients for Bowel Preparation Before Colonoscopy Using Conventional Methods vs Virtual Reality Videos Plus Conventional Methods: A Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2135576. [Google Scholar] [CrossRef] [PubMed]
- Le May, S.; Tsimicalis, A.; Noel, M.; Rainville, P.; Khadra, C.; Ballard, A.; Guingo, E.; Cotes-Turpin, C.; Addab, S.; Chougui, K.; et al. Immersive Virtual Reality vs. Non-immersive Distraction for Pain Management of Children during Bone Pins and Sutures Removal: A Randomized Clinical Trial Protocol. J. Adv. Nurs. 2021, 77, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Dualé, C.; Mourgues, C. The Price of Pain Relief, or Should Non-Invasive Medical Devices Be Treated Differently in Analgesic Clinical Trials? Eur. J. Pain 2022, 26, 553–554. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.; Chun, J.; Han, K.; Park, S.; Soh, H.; Kim, J.; Lee, J.; Lee, H.J.; Im, J.P.; Kim, J.S. Risk of Anxiety and Depression in Patients with Inflammatory Bowel Disease: A Nationwide, Population-Based Study. J. Clin. Med. 2019, 8, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blokzijl, S.J.; Lamberts, K.F.; van der Waaij, L.A.; Spikman, J.M. Willingness to Undergo Colonoscopy with Virtual Reality Instead of Procedural Sedation and Analgesia. Eur. J. Gastroenterol. Hepatol. 2019, 31, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Xiaolian, J.; Xiaolin, L.; Lan, Z.H. Effects of Visual and Audiovisual Distraction on Pain and Anxiety Among Patients Undergoing Colonoscopy. Gastroenterol. Nurs. 2015, 38, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.H.; Chan, A.C.W.; Wong, S.K.H.; Fung, T.M.K.; Li, A.C.N.; Chan, S.K.C.; Mui, L.M.; Ng, E.K.W.; Chung, S.C.S. Can Visual Distraction Decrease the Dose of Patient-Controlled Sedation Required During Colonoscopy? A Prospective Randomized Controlled Trial. Endoscopy 2004, 36, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Antioch, I.; Furuta, T.; Uchikawa, R.; Okumura, M.; Otogoto, J.; Kondo, E.; Sogawa, N.; Ciobica, A.; Tomida, M. Favorite Music Mediates Pain-Related Responses in the Anterior Cingulate Cortex and Skin Pain Thresholds. J. Pain Res. 2020, 13, 2729–2737. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.P.D.; Niriella, M.A.; Nandamuni, Y.; Nanayakkara, S.D.; Perera, K.R.P.; Kodisinghe, S.K.; Subasinghe, K.C.E.; Pathmeswaran, A.; Silva, H.J. de Effect of Audio and Visual Distraction on Patients Undergoing Colonoscopy: A Randomized Controlled Study. Endosc. Int. Open 2016, 4, E1211–E1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, P.; Ivanov, D.; Bhatt, S.; Mastorakos, G.; Birckhead, B.; Khera, N.; Vittone, J. Low-Cost Virtual Reality Headsets Reduce Perceived Pain in Healthy Adults: A Multicenter Randomized Crossover Trial. Games Health J. 2020, 9, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Slater, M. Immersion and the Illusion of Presence in Virtual Reality. Br. J. Psychol. 2018, 109, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Triberti, S.; Repetto, C.; Riva, G. Psychological Factors Influencing the Effectiveness of Virtual Reality-Based Analgesia: A Systematic Review. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Găină, M.-A.; Boloș, A.; Alexinschi, O.; Cristofor, A.-C.; Găină, A.-M.; Chiriță, R.; Ștefănescu, C. Perspective on the Double Edges of Virtual Reality in Medicine—Both Addiction & Treatment. BRAIN Broad Res. Artif. Intell. Neurosci. 2021, 12, 364–373. [Google Scholar] [CrossRef]
- Luo, H.; Cao, C.; Zhong, J.; Chen, J.; Cen, Y. Adjunctive Virtual Reality for Procedural Pain Management of Burn Patients during Dressing Change or Physical Therapy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials: Virtual Reality for Burn Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Wound Repair Regen. 2019, 27, 90–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauwens, Y.; Rafaatpoor, F.; Corbeel, K.; Broekmans, S.; Toelen, J.; Allegaert, K. Immersive Virtual Reality as Analgesia during Dressing Changes of Hospitalized Children and Adolescents with Burns: A Systematic Review with Meta-Analysis. Children 2020, 7, 194. [Google Scholar] [CrossRef] [PubMed]
- Mallari, B.; Spaeth, E.K.; Goh, H.; Boyd, B.S. Virtual Reality as an Analgesic for Acute and Chronic Pain in Adults: A Systematic Review and Meta-Analysis. J. Pain Res. 2019, 12, 2053–2085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aardema, F.; O’Connor, K.; Côté, S.; Taillon, A. Virtual Reality Induces Dissociation and Lowers Sense of Presence in Objective Reality. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Schauer, M.; Elbert, T. Dissociation Following Traumatic Stress: Etiology and Treatment. Z. Psychol. Psychol. 2010, 218, 109–127. [Google Scholar] [CrossRef]
- Hassan, C.; Benamouzig, R.; Spada, C.; Ponchon, T.; Zullo, A.; Saurin, J.C.; Costamagna, G. Cost Effectiveness and Projected National Impact of Colorectal Cancer Screening in France. Endoscopy 2011, 43, 780–793. [Google Scholar] [CrossRef] [Green Version]
- Delshad, S.D.; Almario, C.V.; Fuller, G.; Luong, D.; Spiegel, B.M.R. Economic Analysis of Implementing Virtual Reality Therapy for Pain among Hospitalized Patients. npj Digit. Med. 2018, 1, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papanicolas, I.; Woskie, L.R.; Jha, A.K. Health Care Spending in the United States and Other High-Income Countries. JAMA 2018, 319, 1024–1039. [Google Scholar] [CrossRef] [PubMed]
- Amornyotin, S. Sedation-Related Complications in Gastrointestinal Endoscopy. World J. Gastrointest. Endosc. 2013, 5, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Tychsen, L.; Thio, L.L. Concern of Photosensitive Seizures Evoked by 3D Video Displays or Virtual Reality Headsets in Children: Current Perspective. Eye Brain 2020, 12, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, G. Full-Immersion Virtual Reality: Adverse Effects Related to Static Balance. Neurosci. Lett. 2020, 733, 134974. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, J.S. The Ethics of Virtual Reality Technology: Social Hazards and Public Policy Recommendations. Sci. Eng. Ethics 2018, 24, 1537–1550. [Google Scholar] [CrossRef] [PubMed]
- Weech, S.; Kenny, S.; Barnett-Cowan, M. Presence and Cybersickness in Virtual Reality Are Negatively Related: A Review. Front. Psychol. 2019, 10, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanney, K.; Fidopiastis, C.; Foster, L. Virtual Reality Is Sexist: But It Does Not Have to Be. Front. Robot. AI 2020, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caserman, P.; Garcia-Agundez, A.; Gámez Zerban, A.; Göbel, S. Cybersickness in Current-Generation Virtual Reality Head-Mounted Displays: Systematic Review and Outlook. Virtual Real. 2021, 25, 1153–1170. [Google Scholar] [CrossRef]
- Breivik, H.; Borchgrevink, P.C.; Allen, S.M.; Rosseland, L.A.; Romundstad, L.; Hals, E.K.B.; Kvarstein, G.; Stubhaug, A. Assessment of Pain. Br. J. Anaesth. 2008, 101, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Găină, M.-A.; Ștefănescu, C. The Urge for an Ethical Framework Regarding Virtual Reality Interventional Studies in Psychiatry. In Proceedings of the Book International Congress of Bioethics, Ankara, Turkey, 10–12 October 2021; pp. 146–150. [Google Scholar]
- Bouchard, S.; Berthiaume, M.; Robillard, G.; Forget, H.; Daudelin-Peltier, C.; Renaud, P.; Blais, C.; Fiset, D. Arguing in Favor of Revising the Simulator Sickness Questionnaire Factor Structure When Assessing Side Effects Induced by Immersions in Virtual Reality. Front. Psychiatry 2021, 12, 1926. [Google Scholar] [CrossRef] [PubMed]
- Pot-Kolder, R.; Veling, W.; Counotte, J.; van der Gaag, M. Anxiety Partially Mediates Cybersickness Symptoms in Immersive Virtual Reality Environments. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Kastrinos, F.; Glick, M.; Rosenbaum, A.J.; Wang, T.; Neugut, A.I. The Impact of Suboptimal Bowel Preparation on Adenoma Miss Rates and the Factors Associated with Early Repeat Colonoscopy. Gastrointest. Endosc. 2011, 73, 1207–1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Luo, H.; Zhang, L.; Leung, F.W.; Liu, Z.; Wang, X.; Huang, R.; Hui, N.; Wu, K.; Fan, D.; et al. Telephone-Based Re-Education on the Day before Colonoscopy Improves the Quality of Bowel Preparation and the Polyp Detection Rate: A Prospective, Colonoscopist-Blinded, Randomized, Controlled Study. Gut 2014, 63, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Perin, A.; Galbiati, T.F.; Ayadi, R.; Gambatesa, E.; Orena, E.F.; Riker, N.I.; Silberberg, H.; Sgubin, D.; Meling, T.R.; DiMeco, F. Informed Consent through 3D Virtual Reality: A Randomized Clinical Trial. Acta Neurochir. 2021, 163, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhang, M.M.; Li, Y.Y.; Li, L.X.; Li, Y.Q. Enhanced Education for Bowel Preparation before Colonoscopy: A State-of-the-Art Review. J. Dig. Dis. 2017, 18, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Vijan, S.; Inadomi, J.; Hayward, R.A.; Hofer, T.P.; Fendrick, A.M. Projections of Demand and Capacity for Colonoscopy Related to Increasing Rates of Colorectal Cancer Screening in the United States. Aliment. Pharmacol. Ther. 2004, 20, 507–515. [Google Scholar] [CrossRef]
- Joseph, D.A.; Meester, R.G.S.; Zauber, A.G.; Manninen, D.L.; Winges, L.; Dong, F.B.; Peaker, B.; van Ballegooijen, M. Colorectal Cancer Screening: Estimated Future Colonoscopy Need and Current Volume and Capacity. Cancer 2016, 122, 2479–2486. [Google Scholar] [CrossRef]
- Harber, I.; Zeidan, D.; Aslam, M.N. Colorectal Cancer Screening: Impact of COVID-19 Pandemic and Possible Consequences. Life 2021, 11, 1297. [Google Scholar] [CrossRef]
- Mazidimoradi, A.; Tiznobaik, A.; Salehiniya, H. Impact of the COVID-19 Pandemic on Colorectal Cancer Screening: A Systematic Review. J. Gastrointest. Cancer 2021, 1–15. [Google Scholar] [CrossRef]
- Hoffman, H.G.; Chambers, G.T.; Meyer, W.J.; Arceneaux, L.L.; Russell, W.J.; Seibel, E.J.; Richards, T.L.; Sharar, S.R.; Patterson, D.R. Virtual Reality as an Adjunctive Non-Pharmacologic Analgesic for Acute Burn Pain during Medical Procedures. Ann. Behav. Med. Publ. Soc. Behav. Med. 2011, 41, 183–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, H.G.; Seibel, E.J.; Richards, T.L.; Furness, T.A.; Patterson, D.R.; Sharar, S.R. Virtual Reality Helmet Display Quality Influences the Magnitude of Virtual Reality Analgesia. J. Pain 2006, 7, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Saavedra, L.; Miró-Amarante, L.; Domínguez-Morales, M. Augmented and Virtual Reality Evolution and Future Tendency. Appl. Sci. 2020, 10, 322. [Google Scholar] [CrossRef] [Green Version]
- Walker, M.R.; Kallingal, G.J.S.; Musser, J.E.; Folen, R.; Stetz, M.C.; Clark, J.Y. Treatment Efficacy of Virtual Reality Distraction in the Reduction of Pain and Anxiety during Cystoscopy. Mil. Med. 2014, 179, 891–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curran-Everett, D. Evolution in Statistics: P Values, Statistical Significance, Kayaks, and Walking Trees. Adv. Physiol. Educ. 2020, 44, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.-H.; Ryu, J.J.; Nam, E.; Lee, H.-S.; Lee, J.K. Effects of Preoperative Virtual Reality Magnetic Resonance Imaging on Preoperative Anxiety in Patients Undergoing Arthroscopic Knee Surgery: A Randomized Controlled Study. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 2394–2399. [Google Scholar] [CrossRef] [PubMed]
- Martirosov, S.; Hořejší, P.; Kopeček, P.; Bureš, M.; Šimon, M. The Effect of Training in Virtual Reality on the Precision of Hand Movements. Appl. Sci. 2021, 11, 8064. [Google Scholar] [CrossRef]
- Pulijala, Y.; Ma, M.; Pears, M.; Peebles, D.; Ayoub, A. Effectiveness of Immersive Virtual Reality in Surgical Training—A Randomized Control Trial. J. Oral Maxillofac. Surg. 2018, 76, 1065–1072. [Google Scholar] [CrossRef] [Green Version]
- Lohre, R.; Bois, A.J.; Athwal, G.S.; Goel, D.P.; Canadian Shoulder and Elbow Society (CSES). Improved Complex Skill Acquisition by Immersive Virtual Reality Training: A Randomized Controlled Trial. J. Bone Jt. Surg. Am. 2020, 102, e26. [Google Scholar] [CrossRef]
- Coiffet, P.; Burdea, G.C. Virtual Reality Technology; John Wiley & Sons: Hoboken, NJ, USA, 2017; ISBN 978-1-119-48572-8. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Theme | MeSH Descriptor and Boolean Descriptors | Keywords and Boolean Descriptors |
|---|---|---|
| Virtual reality | [Virtual Reality Exposure Therapy] OR [Smart Glasses] OR [Virtual Reality] | VR OR “virtual therapy” OR “virtual environment” OR “virtual treatment” OR “immersive” OR “non-immersive” OR hmd OR “head-mounted display” OR HTC OR oculus |
| Colonoscopy | [Colonoscopy] OR [Sigmoidoscopy] OR [Endoscopy] | colonoscopy OR sigmoidoscopy OR rectoscope OR endoscopy OR “gastrointestinal endoscopy” OR “secondary prevention” OR prevention |
| Anxiety/pain/sedative/anxiolytic therapy | [Pain] OR [Fear] OR [Anxiety] OR [Heart Rate] OR [Blood Pressure] OR [Anti-Anxiety Agents] OR [Antidepressive Agents] OR [Barbiturates] OR [Benzodiazepines] OR [Hypnotics and Sedatives] | “pain score” OR “pain level” OR fears OR “fear score” OR “fear level” OR “anxiety level” OR “anxiety score” OR pulse OR “pulse rate” |
| Authors | RCT Design; Participants (n) | iVR Intervention: Hardware, Software, Duration | Psychometric Evaluation of Anxiety | Pain Evaluation | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Veldhuijzen et al., 2020 [30] | RCT VRG: (10), CG: (9) Sedated | Samsung Gear VR (Consumer Edition–SM-R322), powered by a Samsung Galaxy S7 smartphone running: A mute 19 min and 59 s long 360° video of tropical islands and forests in the Caribbean. | STAI-S and STAI-T | NRS | ||||||
| VRG | CG | p | VRG | CG | p | |||||
| STAI-S Pre: | 48.5 | 49 | 0.497 | Pre: | 0 (0, 3) | 0 (0, 1.75) | 0.968 | |||
| STAI-S Post: | 50 | 50 | 0.156 | During: | 3 (1.5, 5.5) | 3 (1, 4) | 0.661 | |||
| STAI-T: | 29 | 35 | 0.549 | |||||||
| Çakır and Evirgen, 2021 [31] | RCT VRG: (30), CG: (30) Non-sedated | VR Cardboard Super Flex Googles Android smartphone-powered headset running: “A walk on the beach” software (2016) for the entire procedure duration. | STAI-T and STAI-S | VAS (1–10) | ||||||
| VRG | CG | p | VRG | CG | p | |||||
| STAI-T: | 39.73 ± 3.14 | 46.70 ± 5.97 | 0.000 | During: | 2.76 ± 1.25 | 3.76 ± 2.11 | 0.03 | |||
| STAI-S Pre: | 47.70 ± 3.55 | 48.28 ± 5.26 | 0.647 | Post: | 0.83 ± 1.44 | 1.36 ± 1.51 | 0.168 | |||
| STAI-S Post: | 46.83 ± 10.94 | 49.66 ± 2.83 | 0.175 | |||||||
| Friedman et al., 2021 [32] | Pilot study Comparing iVR experience of previously consciously sedated patients VRG (27) | Samsung Gear VR Headset powered by Samsung Galaxy S7 smartphone running: 1 to 7-min video of nature and animal content, starting synchronously with colonoscopy procedure. | 1–10 patient-reported questionnaires | VAS (1–10) | ||||||
| Pre-procedure anxiety mean ± SD: 3.8 ± 2.2 | Procedural pain mean: 3.6 ± 1.6 | |||||||||
| Anxiety vs. past sedation colonoscopy | Pain vs. past colonoscopy | |||||||||
| Less: 11 (42.3%) | Less: 1 (3.8-requested sedation), | |||||||||
| Similar: 8 (30.8%) | Similar: 11 (42.3) | |||||||||
| More: 3 (11.5%) | More:11 (42.3) | |||||||||
| Not remembering: 1 (3.8%) | No response: 3 (11.5) | |||||||||
| Author | Study Design Enrolled Participants (n) | Outcomes | Anxiety Levels Self-Rated Night before Colonoscopy Sleep Quality | The Boston Bowel Preparation Scale (0–9) |
|---|---|---|---|---|
| Chen et al., 2021 [33] | Single-centre prospective, single-blinded, RCT (346) undergoing the first colonoscopy 173 VRG 173 CG | Primary: evaluate the feasibility of iVR HMD videos for bowel preparation patient education before colonoscopy by comparing them to conventional schooling. Secondary: preprocedural anxiety, adenoma, and polyp detection rates, compliance to bowel cleansing, satisfaction, and willingness to undergo future recommended colonoscopies. | Anxiety score: VRG: 7.60 (2.20) CG: 7.08 (2.64) p: 0.04 | Mean score of ascending, transverse, and descending colon: VRG: 7.61 (1.65) CG: 7.04 (1.70) p: 0.002 |
| Adequate bowel preparation: VRG: 139 (80.3) CG: 125 (72.3) p: 0.08 |
| Sedation and Analgesia Colonoscopy Complications [54] | Immersive Virtual Reality Side Effects [55,56,57,58] | |
|---|---|---|
| Cardiovascular: | Hypotension, hypertension, arrhythmias, myocardial ischemia/infarction | - |
| Respiratory: | Decreased breathing rate, respiratory depression, airway obstruction, hypoxia, pulmonary aspiration | - |
| Allergic reactions: | Minor local response to anaphylactic reactions | - |
| Central nervous system: | Paradoxical reactions (benzodiazepines) | Theoretical epileptic seizures related to intermittent light stimuli in children [55] static imbalance: dizziness, eye strain [56] dissociative symptoms: depersonalization/derealization disorder [57] |
| Other: | Analgesic induced nausea, vomiting | Cybersickness [58]: 3rd cranial nerve (headache, eyestrain, blurred vision) disorientation (imbalance, vertigo) nausea (vomiting, dizziness). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Găină, M.-A.; Szalontay, A.S.; Ștefănescu, G.; Bălan, G.G.; Ghiciuc, C.M.; Boloș, A.; Găină, A.-M.; Ștefănescu, C. State-of-the-Art Review on Immersive Virtual Reality Interventions for Colonoscopy-Induced Anxiety and Pain. J. Clin. Med. 2022, 11, 1670. https://doi.org/10.3390/jcm11061670
Găină M-A, Szalontay AS, Ștefănescu G, Bălan GG, Ghiciuc CM, Boloș A, Găină A-M, Ștefănescu C. State-of-the-Art Review on Immersive Virtual Reality Interventions for Colonoscopy-Induced Anxiety and Pain. Journal of Clinical Medicine. 2022; 11(6):1670. https://doi.org/10.3390/jcm11061670
Chicago/Turabian StyleGăină, Marcel-Alexandru, Andreea Silvana Szalontay, Gabriela Ștefănescu, Gheorghe Gh Bălan, Cristina Mihaela Ghiciuc, Alexandra Boloș, Alexandra-Maria Găină, and Cristinel Ștefănescu. 2022. "State-of-the-Art Review on Immersive Virtual Reality Interventions for Colonoscopy-Induced Anxiety and Pain" Journal of Clinical Medicine 11, no. 6: 1670. https://doi.org/10.3390/jcm11061670
APA StyleGăină, M.-A., Szalontay, A. S., Ștefănescu, G., Bălan, G. G., Ghiciuc, C. M., Boloș, A., Găină, A.-M., & Ștefănescu, C. (2022). State-of-the-Art Review on Immersive Virtual Reality Interventions for Colonoscopy-Induced Anxiety and Pain. Journal of Clinical Medicine, 11(6), 1670. https://doi.org/10.3390/jcm11061670