
Predicting Renal Denervation Response in Resistant High Blood Pressure by Arterial Stiffness Assessment: A Systematic Review

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
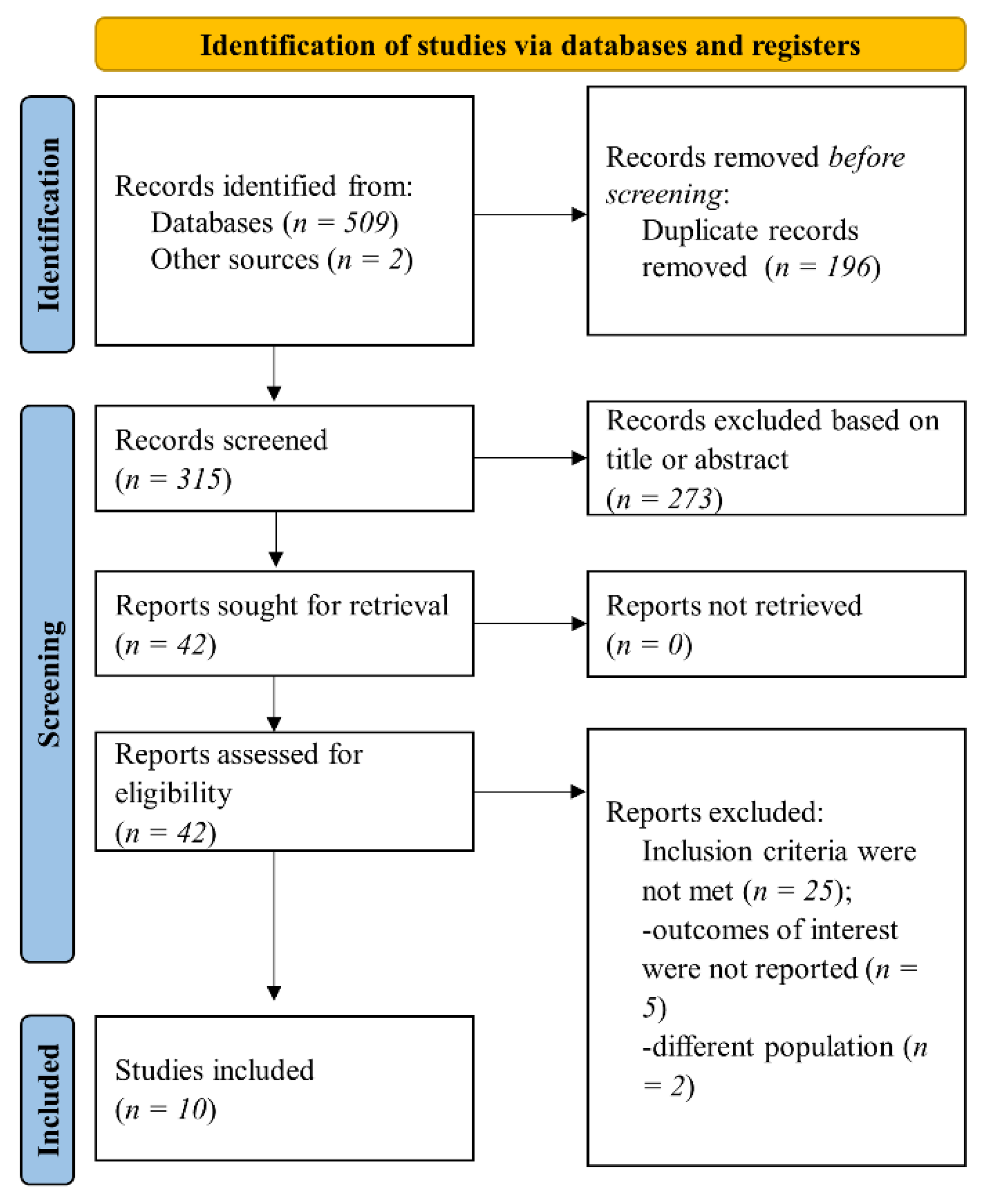
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria and Outcomes
2.3. Data Collection and Synthesis
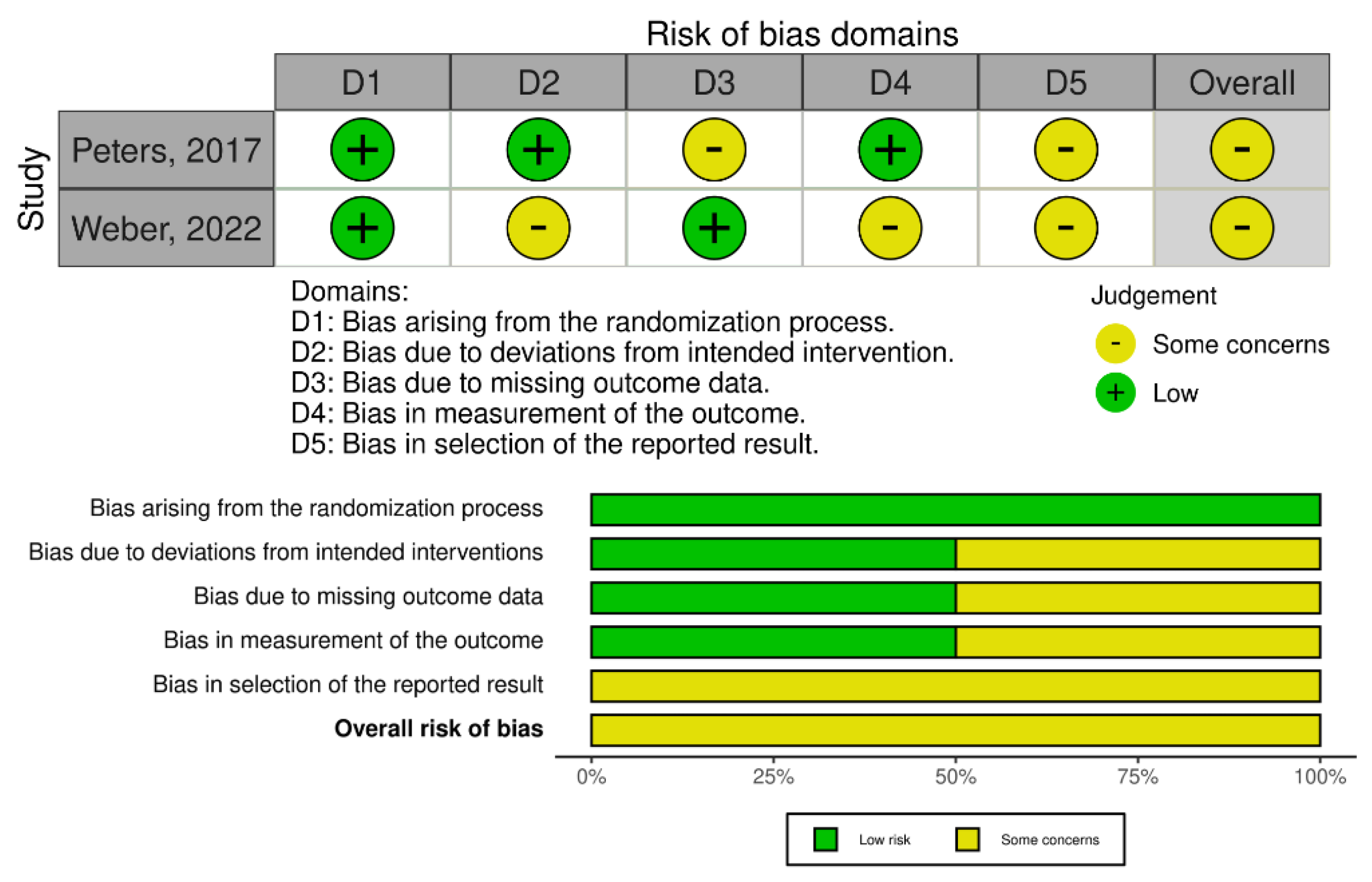
2.4. Quality Assessment
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-I.; Ji, E.; Choi, J.-Y.; Kim, S.-W.; Ahn, S.; Kim, C.-H. Ten-year trends of hypertension treatment and control rate in Korea. Sci. Rep. 2021, 11, 6966. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef] [PubMed]
- Pimenta, E.; Calhoun, D.A. Resistant hypertension: Incidence, prevalence, and prognosis. Circulation 2012, 125, 1594–1596. [Google Scholar] [CrossRef]
- Noubiap, J.J.; Nansseu, J.R.; Nyaga, U.F.; Sime, P.S.; Francis, I.; Bigna, J.J. Global prevalence of resistant hypertension: A meta-analysis of data from 3.2 million patients. Heart 2019, 105, 98–105. [Google Scholar] [CrossRef]
- Daugherty, S.L.; Powers, J.D.; Magid, D.J.; Tavel, H.M.; Masoudi, F.A.; Margolis, K.L.; O’Connor, P.J.; Selby, J.V.; Ho, P.M. Incidence and Prognosis of Resistant Hypertension in Hypertensive Patients. Circulation 2012, 125, 1635–1642. [Google Scholar] [CrossRef]
- Kaczmarski, K.R.; Sozio, S.M.; Chen, J.; Sang, Y.; Shafi, T. Resistant hypertension and cardiovascular disease mortality in the US: Results from the National Health and Nutrition Examination Survey (NHANES). BMC Nephrol. 2019, 20, 138. [Google Scholar] [CrossRef]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redón, J.; Zanchetti, A.; Böhm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2013, 31, 1281–1357. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Kandzari, D.E.; O’Neill, W.W.; D’Agostino, R.; Flack, J.M.; Katzen, B.T.; Leon, M.B.; Liu, M.; Mauri, L.; Negoita, M.; et al. A Controlled Trial of Renal Denervation for Resistant Hypertension. N. Engl. J. Med. 2014, 370, 1393–1401. [Google Scholar] [CrossRef]
- Santos-Gallego, C.; Badimón, J. Catheter-based Renal Denervation as a Treatment for Pulmonary Hypertension: Hope or Hype? Rev. Española Cardiol. 2015, 68, 551–553. [Google Scholar] [CrossRef]
- Versaci, F.; Sciarretta, S.; Scappaticci, M.; Calcagno, S.; di Pietro, R.; Sbandi, F.; Dei Giudici, A.; Del Prete, A.; de Angelis, S.; Biondi-Zoccai, G. Renal arteries denervation with second generation systems: A remedy for resistant hypertension? Eur. Heart J. Suppl. 2020, 22, L160–L165. [Google Scholar] [CrossRef] [PubMed]
- Ogoyama, Y.; Tada, K.; Abe, M.; Nanto, S.; Shibata, H.; Mukoyama, M.; Kai, H.; Arima, H.; Kario, K. Effects of renal denervation on blood pressures in patients with hypertension: A systematic review and meta-analysis of randomized sham-controlled trials. Hypertens. Res. 2022, 45, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Rosa, J.; Kvasnicka, J.; Lambert, L.; Waldauf, P.; Zelinka, T.; Petrak, O.; Strauch, B.; Holaj, R.; Indra, T.; Kratka, Z.; et al. PREDICTION OF LONG-TERM RENAL DENERVATION EFFICACY. J. Hypertens. 2018, 36, e48. [Google Scholar] [CrossRef]
- Böhm, M.; Tsioufis, K.; Kandzari, D.E.; Kario, K.; Weber, M.A.; Schmieder, R.E.; Townsend, R.R.; Kulenthiran, S.; Ukena, C.; Pocock, S.; et al. Effect of Heart Rate on the Outcome of Renal Denervation in Patients with Uncontrolled Hypertension. J. Am. Coll. Cardiol. 2021, 78, 1028–1038. [Google Scholar] [CrossRef]
- Fengler, K.; Rommel, K.P.; Kriese, W.; Kresoja, K.P.; Blazek, S.; Obradovic, D.; Feistritzer, H.J.; Lücke, C.; Gutberlet, M.; Desch, S.; et al. Assessment of arterial stiffness to predict blood pressure response to renal sympathetic denervation. EuroIntervention: J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Laurent, S.; Boutouyrie, P. Arterial Stiffness and Hypertension in the Elderly. Front. Cardiovasc. Med. 2020, 7, 544302. [Google Scholar] [CrossRef]
- Salvi, P.; Valbusa, F.; Kearney-Schwartz, A.; Labat, C.; Grillo, A.; Parati, G.; Benetos, A. Non-Invasive Assessment of Arterial Stiffness: Pulse Wave Velocity, Pulse Wave Analysis and Carotid Cross-Sectional Distensibility: Comparison between Methods. J. Clin. Med. 2022, 11, 2225. [Google Scholar] [CrossRef]
- Townsend, R.R.; Wilkinson, I.B.; Schiffrin, E.L.; Avolio, A.P.; Chirinos, J.A.; Cockcroft, J.R.; Heffernan, K.S.; Lakatta, E.G.; McEniery, C.M.; Mitchell, G.F.; et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement From the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Ott, C.; Schmid, A.; Toennes, S.W.; Ditting, T.; Veelken, R.; Uder, M.; Schmieder, R.E. Central pulse pressure predicts BP reduction after renal denervation in patients with treatment-resistant hypertension. EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2015, 11, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Okon, T.; Röhnert, K.; Stiermaier, T.; Rommel, K.P.; Müller, U.; Fengler, K.; Schuler, G.; Desch, S.; Lurz, P. Invasive aortic pulse wave velocity as a marker for arterial stiffness predicts outcome of renal sympathetic denervation. EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2016, 12, e684–e692. [Google Scholar] [CrossRef] [PubMed]
- Fengler, K.; Rommel, K.P.; Hoellriegel, R.; Blazek, S.; Besler, C.; Desch, S.; Schuler, G.; Linke, A.; Lurz, P. Pulse Wave Velocity Predicts Response to Renal Denervation in Isolated Systolic Hypertension. J. Am. Heart Assoc. 2017, 6, e005879. [Google Scholar] [CrossRef]
- Fengler, K.; Rommel, K.P.; Blazek, S.; Von Roeder, M.; Besler, C.; Lücke, C.; Gutberlet, M.; Steeden, J.; Quail, M.; Desch, S.; et al. Cardiac magnetic resonance assessment of central and peripheral vascular function in patients undergoing renal sympathetic denervation as predictor for blood pressure response. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2018, 107, 945–955. [Google Scholar] [CrossRef]
- Fengler, K.; Rommel, K.P.; Blazek, S.; von Roeder, M.; Besler, C.; Hartung, P.; Desch, S.; Thiele, H.; Lurz, P. Predictors for profound blood pressure response in patients undergoing renal sympathetic denervation. J. Hypertens. 2018, 36, 1578–1584. [Google Scholar] [CrossRef]
- Peters, C.D.; Mathiassen, O.N.; Vase, H.; Bech Nørgaard, J.; Christensen, K.L.; Schroeder, A.P.; Rickers, H.; Opstrup, U.K.; Poulsen, P.L.; Langfeldt, S.; et al. The effect of renal denervation on arterial stiffness, central blood pressure and heart rate variability in treatment resistant essential hypertension: A substudy of a randomized sham-controlled double-blinded trial (the ReSET trial). Blood Press. 2017, 26, 366–380. [Google Scholar] [CrossRef]
- Sata, Y.; Hering, D.; Head, G.A.; Walton, A.S.; Peter, K.; Marusic, P.; Duval, J.; Lee, R.; Hammond, L.J.; Lambert, E.A.; et al. Ambulatory arterial stiffness index as a predictor of blood pressure response to renal denervation. J. Hypertens. 2018, 36, 1414–1422. [Google Scholar] [CrossRef]
- Stoiber, L.; Mahfoud, F.; Zamani, S.M.; Lapinskas, T.; Böhm, M.; Ewen, S.; Kulenthiran, S.; Schlaich, M.P.; Esler, M.D.; Hammer, T.; et al. Renal sympathetic denervation restores aortic distensibility in patients with resistant hypertension: Data from a multi-center trial. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2018, 107, 642–652. [Google Scholar] [CrossRef]
- Weber, T.; Wassertheurer, S.; Mayer, C.C.; Hametner, B.; Danninger, K.; Townsend, R.R.; Mahfoud, F.; Kario, K.; Fahy, M.; DeBruin, V.; et al. Twenty-Four-Hour Pulsatile Hemodynamics Predict Brachial Blood Pressure Response to Renal Denervation in the SPYRAL HTN-OFF MED Trial. Hypertension 2022, 79, 1506–1514. [Google Scholar] [CrossRef] [PubMed]
- Bonarjee, V.V.S. Arterial Stiffness: A Prognostic Marker in Coronary Heart Disease. Available Methods and Clinical Application. Front. Cardiovasc. Med. 2018, 5, 64. [Google Scholar] [CrossRef] [PubMed]
- Berukstis, A.; Navickas, R.; Neverauskaite-Piliponiene, G.; Ryliskyte, L.; Misiura, J.; Vajauskas, D.; Misonis, N.; Laucevicius, A. Arterial Destiffening Starts Early after Renal Artery Denervation. Int. J. Hypertens. 2019, 2019, 3845690. [Google Scholar] [CrossRef]
- Grotenhuis, H.B.; Westenberg, J.J.M.; Steendijk, P.; van der Geest, R.J.; Ottenkamp, J.; Bax, J.J.; Jukema, J.W.; de Roos, A. Validation and reproducibility of aortic pulse wave velocity as assessed with velocity-encoded MRI. J. Magn. Reson. Imaging 2009, 30, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Azizi, M.; Schmieder, R.E.; Mahfoud, F.; Weber, M.A.; Daemen, J.; Davies, J.; Basile, J.; Kirtane, A.J.; Wang, Y.; Lobo, M.D.; et al. Endovascular ultrasound renal denervation to treat hypertension (RADIANCE-HTN SOLO): A multicentre, international, single-blind, randomised, sham-controlled trial. Lancet 2018, 391, 2335–2345. [Google Scholar] [CrossRef]
- Saxena, M.; Schmieder, R.E.; Kirtane, A.J.; Mahfoud, F.; Daemen, J.; Basile, J.; Lurz, P.; Gosse, P.; Sanghvi, K.; Fisher, N.D.L.; et al. Predictors of blood pressure response to ultrasound renal denervation in the RADIANCE-HTN SOLO study. J. Hum. Hypertens. 2022, 36, 629–639. [Google Scholar] [CrossRef]
- Chowdhury, E.K.; Reid, C.M.; Zomer, E.; Kelly, D.J.; Liew, D. Cost-Effectiveness of Renal Denervation Therapy for Treatment-Resistant Hypertension: A Best Case Scenario. Am. J. Hypertens. 2018, 31, 1156–1163. [Google Scholar] [CrossRef]
- Schlaich, M.P.; Lambert, E.; Kaye, D.M.; Krozowski, Z.; Campbell, D.J.; Lambert, G.; Hastings, J.; Aggarwal, A.; Esler, M.D. Sympathetic augmentation in hypertension: Role of nerve firing, norepinephrine reuptake, and Angiotensin neuromodulation. Hypertension 2004, 43, 169–175. [Google Scholar] [CrossRef]
- Boutouyrie, P.; Chowienczyk, P.; Humphrey, J.D.; Mitchell, G.F. Arterial Stiffness and Cardiovascular Risk in Hypertension. Circ. Res. 2021, 128, 864–886. [Google Scholar] [CrossRef]
- Sethi, S.; Rivera, O.; Oliveros, R.; Chilton, R. Aortic stiffness: Pathophysiology, clinical implications, and approach to treatment. Integr. Blood Press. Control 2014, 7, 29–34. [Google Scholar] [CrossRef]
- Requena-Ibáñez, J.A.; Santos-Gallego, C.G.; Rodriguez-Cordero, A.; Vargas-Delgado, A.P.; Mancini, D.; Sartori, S.; Atallah-Lajam, F.; Giannarelli, C.; Macaluso, F.; Lala, A.; et al. Mechanistic Insights of Empagliflozin in Nondiabetic Patients with HFrEF: From the EMPA-TROPISM Study. JACC Heart Fail. 2021, 9, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Bosch, A.; Ott, C.; Jung, S.; Striepe, K.; Karg, M.V.; Kannenkeril, D.; Dienemann, T.; Schmieder, R.E. How does empagliflozin improve arterial stiffness in patients with type 2 diabetes mellitus? Sub analysis of a clinical trial. Cardiovasc. Diabetol. 2019, 18, 44. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author, Year | Design | Patients, No | Age, Median/Mean ± SD | Setting | Methods | Outcomes | Follow-Up |
|---|---|---|---|---|---|---|---|
| Ott et al., 2015 [23] | Observational, prospective, single-center | 63 | 56.5 ± 11 (low cPP) | Patients with TRH (office BP ≥ 140/90 mmHg and 24 h ABP ≥ 130/80 mmHg despite treatment with at least 3 AHT drugs, including a diuretic) and eGFR ≥ 15 mL/min/1.73 m2. | Baseline cPP was measured using SphygmoCor. Patients were stratified according to median cPP: low cPP (below 55 mmHg) and high cPP (above 55 mmHg). RDN—radiofrequency technique. | (a) Office and 24 h systolic and diastolic BP reduction after RDN. (b) Renal function. | 6 months |
| 66.1 ± 8.0 (high cPP) | |||||||
| Okon et al., 2016 [24] | Observational, single-center | 58 | 60.41 ± 10.3 (responders) | Patients with resistant hypertension (24 h ABP: mean daytime systolic BP ≥ 135 mmHg or diastolic BP ≥ 90 mmHg, despite treatment with at least 3 AHT drugs, including a diuretic. Patients with eGFR < 45 mL/min/1.73 m2 were excluded. | PWV was measured invasively. RDN response was defined as reduction with ≥5 mmHg in systolic daytime BP (24 h ABPM). RDN—radiofrequency technique. | Daytime, night-time, and 24 h BP reduction after RDN. | 6 months |
| 63.1 ± 9.0 (non-responders) | |||||||
| Fengler et al., 2017 [25] | Observational, prospective, single-center | 109 | 60.4 ± 9.0 (combined hypertension) | Patients with resistant hypertension, defined as mean daytime systolic BP > 135 mmHg or diastolic BP > 90 mmHg in ABPM despite treatment with at least 3 AHT drugs, including 1 diuretic unless intolerant. | PWV was measured invasively immediately before renal denervation. Response to RDN was defined as a drop ≥ 5 mmHg in ABPM daytime systolic BP after 3 months. RDN—radiofrequency and ultrasound techniques. | (a) BP reduction after RDN at 3 months. (b) BP response in relation to PWV tertiles. | 3 months |
| 66.5 ± 9.8 (isolated systolic hypertension) | |||||||
| Fengler et al., 2018 [26] | Observational, single-center, study sub-analysis | 32 | 64.5 ± 9.9 | Patients treated for resistant hypertension, defined as mean daytime systolic ≥135 mmHg or diastolic BP ≥ 90 mmHg in ABPM, despite intake of at least 3 AHT drugs, including a diuretic. Patients with eGFR < 45 mL/min/1.73 m2 were excluded. | Arterial stiffness measured using MRI (ascending aortic distensibility, total arterial compliance, systemic vascular resistance) versus invasive PWV. Response to RDN was defined as a drop ≥5 mmHg in ABPM daytime systolic BP after 3 months. RDN—radiofrequency technique. | (a) BP reduction after RDN using ABPM. (b) Invasive and non-invasive parameters of arterial stiffness as predictors for the response after RDN. | 3 months |
| Fengler et al., 2022 [16] | Observational, prospective, single-center | 79 | 62.6 ± 8.8 | Patients with resistant hypertension defined as systolic daytime BP > 135 mmHg, despite treatment with 3 or more different classes of AHT drugs, including one diuretic, unless intolerant to diuretics. | Arterial stiffness was measured invasively (PWV) or non-invasively (CMR-derived ascending aortic distensibility, PWV, and total arterial compliance). Response to RDN was defined as a drop ≥ 5 mmHg in ABPM daytime systolic BP after 3 months. RDN—ultrasound and radiofrequency (in validation cohort) techniques. | (a) Change in systolic daytime BP on ABPM at 3 months in different arterial stiffness subgroups. (b) RDN response predicting power of non-invasive arterial stiffness parameters compared to invasive PWV measurement. | 3 months |
| Fengler et al., 2018 [27] | Observational, retrospective, single-center | 190 | 62.2 ± 9.9 | Patients with TRH defined as office systolic BP > 160 mmHg and 24 h BP > 135/90 mmHg, despite treatment with 3 or more classes of AHT drugs, including one diuretic, unless intolerant to diuretics. | PWV measured invasively and non-invasive pulse pressure. Response to RDN was defined as a drop ≥ 5 mmHg in ABPM daytime average BP after 3 months. The profound response was defined as a drop ≥ 20 mmHg in ABPM daytime average BP. RDN—radiofrequency and ultrasound techniques. | Change in BP on ABPM, including a profound response, in relation to arterial stiffness. | 3 months |
| Peters et al., 2017 [28] | Substudy of a randomized, sham-controlled, double-blind trial | 53 | 59 ± 9 (sham) | Patients with therapy-resistant hypertension, with daytime ABPM systolic >145 mmHg and 1 month of stable treatment with at least 3 AHT drugs, including a diuretic. Patients with eGFR < 30 mL/min/1.73 m2 were excluded. | Carotid-femoral PWV was measured non-invasively at baseline and after 6 months (SphygmoCor). RDN—radiofrequency technique. | Changes in 24 h AMBP and PWV after RDN. | 6 months |
| 54 ± 8 (RDN) | |||||||
| Sata et al., 2018 [29] | Observational, retrospective | 111 | 63.2 ± 10.3 | Patients with resistant hypertension are defined as having office BP > 140/90 mmHg, despite prescribed treatment with three or more AHT drugs. | The ambulatory arterial stiffness index was derived from 24 h ABPM monitoring. Response to RDN was defined as a reduction of 5% in systolic BP on ABPM. RDN—radiofrequency technique. | (a) Reduction in systolic BP on ABPM after 6 months from RDN. (b) The predictive value of RDN response attributed to ambulatory arterial stiffness index. | 12 months |
| Stoiber et al., 2018 [30] | Observational, prospective, multicenter | 58 | 64.4 ± 9.6 | Resistant hypertension was defined as office systolic BP ≥ 140 mmHg or mean ambulatory 24 h systolic BP > 135 mmHg despite using≥ 3 AHT drugs, including a diuretic. | Aortic distensibility was derived from MRI. Response to RDN was defined as reduction with at least 10 mmHg in systolic BP. RDN—radiofrequency technique. | (a) Office systolic and diastolic BP at 6 months after RDN in relation to aortic distensibility. (b) Aortic distensibility response to RDN. | 6 months |
| Weber et al., 2022 [31] | A post hoc analysis of a randomized, sham-controlled clinical trial | 222 | 53.0 ± 11.0 (RDN) | Patients with average systolic BP ≥ 140 mmHg and <170 mmHg on 24 h ABPM, office systolic BP ≥ 150 mmHg and <180 mmHg, and office diastolic BP ≥ 90 mmHg. | Augmentation index, augmentation pressure, backward and forward wave amplitude, estimated aortic PWV, measured non-invasively. RDN—radiofrequency technique. | Predictive value of RDN response in relation to non-invasive arterial stiffness parameters. | 3 months |
| 51.6 ± 11.0 (sham) |
| Study, Year | Parameters | Outcomes | Results | ||
|---|---|---|---|---|---|
| Ott, 2015 [23] | Pre-RDN | Post-RDN | |||
| Low cPP | Office SBP, mmHg | 160 ± 16 | 137 ± 16 | p < 0.001 | |
| Office DBP, mmHg | 95 ± 13 | 82 ± 11 | p < 0.001 | ||
| 24 h SBP, mmHg | 155 ± 15 | 144 ± 15 | p < 0.001 | ||
| 24 h DBP, mmHg | 93 ± 12 | 86 ± 10 | p < 0.001 | ||
| eGFR, mL/min/1.73 m2 | 76.4 ± 21 | 76.0 ± 22 | p = 0.846 | ||
| High cPP | Office SBP, mmHg | 166 ± 20 | 154 ± 26 | p = 0.003 | |
| Office DBP, mmHg | 85 ± 16 | 80 ± 14 | p = 0.049 | ||
| 24 h SBP, mmHg | 157 ± 16 | 154 ± 23 | p = 0.326 | ||
| 24 h DBP, mmHg | 84 ± 11 | 81 ± 12 | p = 0.059 | ||
| eGFR, mL/min/1.73 m2 | 72.1 ± 28 | 70.1 ± 30 | p = 0.243 | ||
| cPP | Office SBP reduction, mmHg | −22 ± 19 in low cPP vs.−12 ± 20 in high cPP | p = 0.038 | ||
| Office DBP reduction, mmHg | −13 ± 11 in low cPP vs.−5 ± 13 in high cPP | p = 0.014 | |||
| 24 h SBP reduction, mmHg | −11 ± 13 in low cPP vs.−3 ± 18 in high cPP | p = 0.07 | |||
| 24 h DBP reduction, mmHg | −8 ± 10 in low cPP vs.−4 ± 10 in high cPP | p = 0.112 | |||
| Okon, 2016 [24] | iPWV | RDN response | OR 1.15 (95% CI, 1.014–1.327) | p = 0.03 | |
| AUC 0.79 (95% CI, 0.658–0.882) | p < 0.0001 | ||||
| 13.7 m/s cut-off: sensitivity 71%, specificity 83%, positive predictive value 85.7% | |||||
| Fengler, 2017 [25] | iPWV | Daytime BP response | Patients with iPWV < 14.4 m/s had a better BP response vs. those with iPWV > 14.4 m/s (11.7 ± 12.7 mmHg vs. 7.2 ± 10.4 mmHg) | p = 0.047 | |
| Patients with isolated systolic hypertension in the lowest iPWV tertile had the best BP response vs. those in the middle iPWV tertile | p = 0.012 | ||||
| Patients with isolated systolic hypertension in the lowest iPWV tertile had the best BP response vs. those in high iPWV tertile | p = 0.013 | ||||
| Responder rate | 77% in low iPWV tertile, 50% in middle iPWV tertile and 23% in high iPWV tertile | p = 0.001 | |||
| BP response | Per 1 m/s of iPWV: OR 0.91, 95% CI, 0.83–0.99) | p = 0.037 | |||
| Fengler, 2018 [30] | iPWV | BP response | Patients with iPWV < 13.6 m/s had better BP response than those with iPWV > 13.6 m/s (−13.0 ± 8.7 mmHg vs. −4.1 ± 5.5 mmHg) | p = 0.002 | |
| AUC 0.849, 95% CI, 0.713–0.985 | p = 0.004 | ||||
| AAD | BP response | Patients with AAD above the median (2.0 × 10−3 mmHg−1) had a better BP response than those with AAD below the median (−11.9 ± 6.9 mmHg vs. −5.6 ± 8.8 mmHg) | p = 0.034 | ||
| AUC 0.828, 95% CI, 0.677–0.979 | p = 0.006 | ||||
| Multivariate analysis: OR 6.8, 95% CI, 1.4–34.2—AAD the only predictor for BP response | p = 0.019 | ||||
| cTAC, TAC | BP response | Patients with cTAC or TAC above the median had a better BP response than those with parameters below the median (−11.6 ± 6.8 mmHg vs. −5.5 ± 9.1 mmHg) | p = 0.041 | ||
| cTAC | BP response | AUC 0.776, 95% CI, 0.563–0.989 | p = 0.021 | ||
| TAC | BP response | AUC 0.753, 95% CI, 0.576–0.929 | p = 0.035 | ||
| Fengler, 2022 [16] | iPWV | Daytime BP reduction | β 0.242, 95% CI, 0.054–0.430 | p = 0.012 | |
| 24 h BP reduction | β = 0.232, 95% CI, 0.046–0.419, AUC 0.695 | p = 0.015 | |||
| AAD | 24 h BP reduction | β = −0.243, 95% CI, −0.428 to −0.058, AUC 0.714 | p = 0.011 | ||
| AAD (logarithmic) | 24 h BP reduction | Β = −0.306, 95% CI, −0.484 to −0.128 | p = 0.001 | ||
| TAC | 24 h BP reduction | β = −0.058 | p = 0.61 | ||
| PWV (MRI) | 24 h BP reduction | β = 0.207 | p = 0.07 | ||
| Carotid-femoral PWV | 24 h BP reduction | β = 0.109 | p = 0.34 | ||
| Fengler, 2018 [27] | iPWV | BP reduction | Lower iPWV was associated with a higher rate of profound BP response (per m/s: OR 0.834, 95% CI, 0.724–0.961) | p = 0.012 | |
| Non-invasive pulse pressure | BP reduction | No differences were observed between no or regular BP response as compared to those with profound BP response | p = 0.16 | ||
| Peters, 2017 [28] | PWV | SBP 24 h response | r2 = 0.002 | p = NS | |
| MAP reduction | r2 = 0.001 | p = NS | |||
| Sata, 2018 [29] | AASI | BP response | Responders had lower AASI compared to non-responders (0.47 ± 0.12 vs. 0.54 ± 0.15) | p = 0.031 | |
| 84% of patients from the highest AASI tertile were non-respondent, compared to 42% in the lowest AASI tertile | |||||
| AASI < 0.51 | BP response | OR 2.62, 95% CI, 1.05–6.79 (univariate analysis) | p = 0.038 | ||
| OR 3.46, 95% CI, 1.0–13.3 (multivariate adjustment) | p = 0.04 | ||||
| AASI < 0.64 | BP response | OR 14.0, 95% CI, 2.57–261.37 | p = 0.001 | ||
| Stoiber, 2018 [30] | Aortic distensibility | SBP reduction | −24.0 ± 26.5 mmHg (low distensibility group) vs. −18.5 ± 16.1 mmHg (high distensibility group) | p = 0.770 | |
| DBP reduction | −8.4 ± 14.7 mmHg (low distensibility group) vs. −6.9 ± 9.6 mmHg (high distensibility group) | p = 0.570 | |||
| Weber, 2022 [31] | Augmentation index | 24 h SBP reduction | −8.4 mmHg in the low augmentation index group vs. −0.6 mmHg in the high augmentation index group | p < 0.001 | |
| AUC 0.70, 95% CI, 0.61–0.79 | p < 0.0001 | ||||
| Augmentation pressure | 24 h SBP reduction | −8.5 mmHg in the low augmentation pressure group vs. −0.5 mmHg in the high augmentation pressure group | p < 0.001 | ||
| AUC 0.74, 95% CI, 0.64–0.82 | p < 0.0001 | ||||
| BWA | 24 h SBP reduction | −7.9 mmHg in low BWA group vs. −1.1 mmHg in high BWA group | p < 0.001 | ||
| AUC 0.70, 95% CI, 0.61–0.79 | p < 0.0001 | ||||
| FWA | 24 h SBP reduction | −7.4 mmHg in low FWA group vs. −1.7 mmHg in high FWA group | p = 0.004 | ||
| AUC 0.65, 95% CI, 0.55–0.74 | p = 0.004 | ||||
| ePWV | 24 h SBP reduction | −8.4 mmHg in low ePWV group vs. −0.6 mmHg in high ePWV group | p < 0.001 | ||
| AUC 0.62, 95% CI, 0.53–0.71 | p = 0.03 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burlacu, A.; Brinza, C.; Floria, M.; Stefan, A.E.; Covic, A.; Covic, A. Predicting Renal Denervation Response in Resistant High Blood Pressure by Arterial Stiffness Assessment: A Systematic Review. J. Clin. Med. 2022, 11, 4837. https://doi.org/10.3390/jcm11164837
Burlacu A, Brinza C, Floria M, Stefan AE, Covic A, Covic A. Predicting Renal Denervation Response in Resistant High Blood Pressure by Arterial Stiffness Assessment: A Systematic Review. Journal of Clinical Medicine. 2022; 11(16):4837. https://doi.org/10.3390/jcm11164837
Chicago/Turabian StyleBurlacu, Alexandru, Crischentian Brinza, Mariana Floria, Anca Elena Stefan, Andreea Covic, and Adrian Covic. 2022. "Predicting Renal Denervation Response in Resistant High Blood Pressure by Arterial Stiffness Assessment: A Systematic Review" Journal of Clinical Medicine 11, no. 16: 4837. https://doi.org/10.3390/jcm11164837
APA StyleBurlacu, A., Brinza, C., Floria, M., Stefan, A. E., Covic, A., & Covic, A. (2022). Predicting Renal Denervation Response in Resistant High Blood Pressure by Arterial Stiffness Assessment: A Systematic Review. Journal of Clinical Medicine, 11(16), 4837. https://doi.org/10.3390/jcm11164837