
Evaluation of the Progression of Periodontitis with the Use of Neural Networks


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Population
2.2. Clinical Periodontal Measurements
- Teeth with gingival recession of traumatic origin;
- Dental caries near cervical area of the tooth;
- The presence of CAL at the distal surface of second molar due to the malposition
- Extraction of third molar;
- An endodontic lesion in the marginal periodontium;
- Vertical root fracture [11].
2.3. Artificial Neural Network
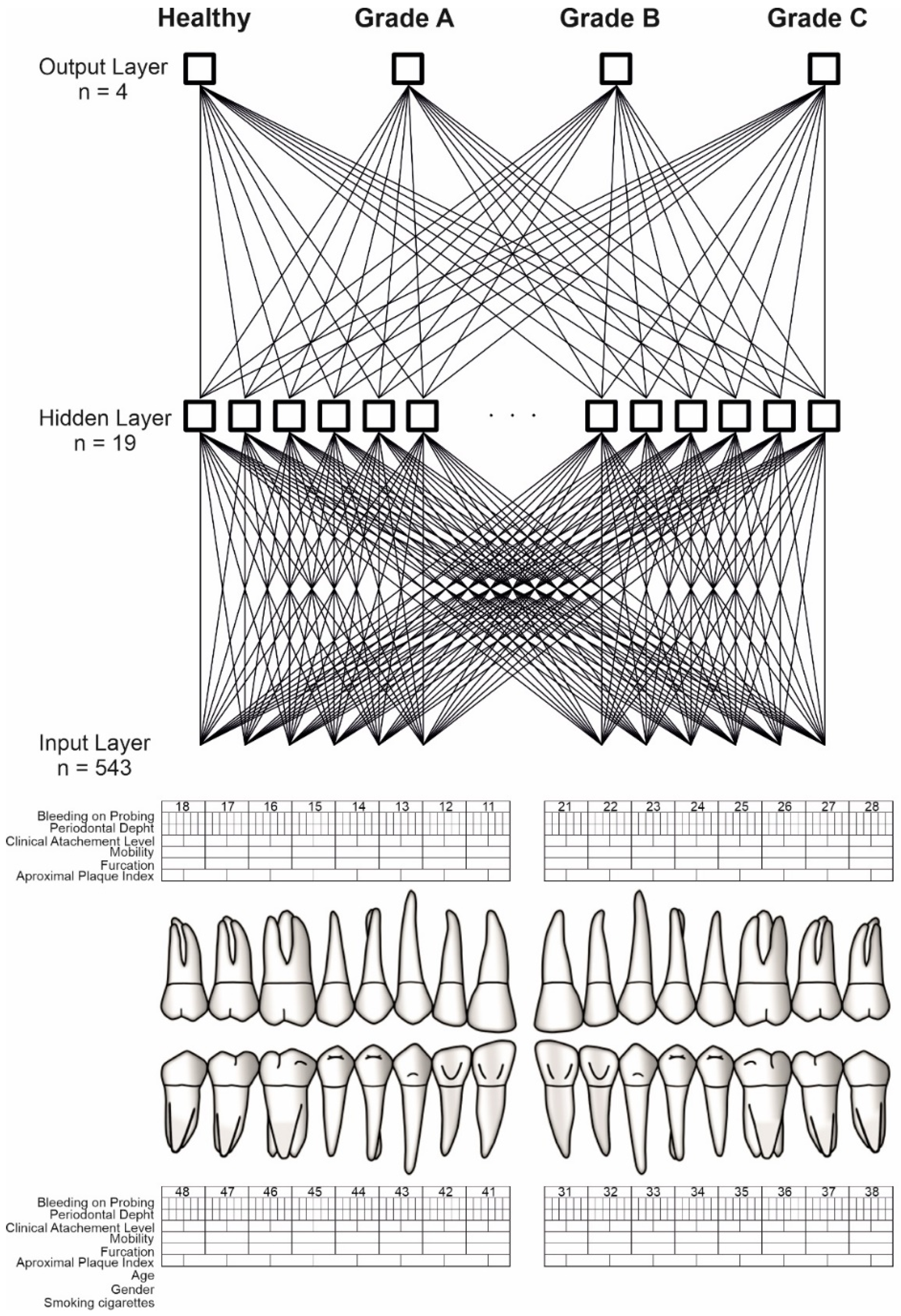
2.3.1. ANN Construction
2.3.2. Input Signals for Artificial Neural Network
2.4. Software Simulation of ANN and the Statistical Analysis
3. Results
3.1. Basic Characteristics
3.2. Classification Assessment of the ANN
3.3. Sensitivity Analysis
3.4. Implementation of the Model into Clinical Practice
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lang, N.P.; Bartold, P.M. Periodontal health. J. Periodontol. 2018, 89 (Suppl. S1), S9–S16. [Google Scholar] [CrossRef] [Green Version]
- Kinane, D.F. Periodontitis modified by systemic factors. Ann. Periodontol. 1999, 4, 54–64. [Google Scholar] [CrossRef]
- Zmora, N.; Bashiardes, S.; Levy, M.; Elinav, E. The Role of the Immune System in Metabolic Health and Disease. Cell Metab. 2017, 25, 506–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quirynen, M.; Dadamio, J.; van den Velde, S.; de Smit, M.; Dekeyser, C.; van Tornout, M.; Vandekerckhove, B. Characteristics of 2000 patients who visited a halitosis clinic. J. Clin. Periodontol. 2009, 36, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Chapple, I.L.; Jepsen, S.; Sanz, M. Primary and secondary prevention of periodontal and peri-implant diseases: Introduction to, and objectives of the 11th European Workshop on Periodontology consensus conference. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S1–S4. [Google Scholar] [CrossRef]
- Murakami, S.; Mealey, B.L.; Mariotti, A.; Chapple, I.L.C. Dental plaque-induced gingival conditions. J. Periodontol. 2018, 89 (Suppl. S1), S17–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinane, D.F.; Attström, R.; European Workshop in Periodontology Group B. Advances in the pathogenesis of periodontitis. Group B consensus report of the fifth European Workshop in Periodontology. J. Clin. Periodontol. 2005, 32 (Suppl. S6), 130–131. [Google Scholar] [CrossRef]
- Mariotti, A. Sex steroid hormones and cell dynamics in the periodontium. Crit. Rev. Oral Biol. Med. 1994, 5, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Mariotti, A.; Mawhinney, M. Endocrinology of sex steroid hormones and cell dynamics in the periodontium. Periodontology 2013, 61, 69–88. [Google Scholar] [CrossRef] [PubMed]
- Meyle, J.; Chapple, I. Molecular aspects of the pathogenesis of periodontitis. Periodontol. 2000 2015, 69, 7–17. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. S1), S159–S172, Erratum in J. Periodontol. 2018, 89, 1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapple, I.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S74–S84. [Google Scholar] [CrossRef] [PubMed]
- Ossowska, A.; Kusiak, A.; Świetlik, D. Artificial Intelligence in Dentistry—Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 3449. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Wennström, J.L.; Gröndahl, K. A 10-year retrospective study of periodontal disease progression. J. Clin. Periodontol. 1989, 16, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N. Patterns of alveolar bone loss in the assessment of periodontal treatment priorities. Swed. Dent. J. Suppl. 1989, 66, 1–45. [Google Scholar]
- Morelli, T.; Moss, K.L.; Preisser, J.S.; Beck, J.D.; Divaris, K.; Wu, D.; Offenbacher, S. Periodontal profile classes predict periodontal disease progression and tooth loss. J. Periodontol. 2018, 89, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Mombelli, A. Early-onset periodontitis. Ann. Periodontol. 1999, 4, 39–53. [Google Scholar] [CrossRef]
- Lang, N.P.; Tonetti, M.S. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev. Dent. 2003, 1, 7–16. [Google Scholar]
- Kakileti, S.T.; Madhu, H.J.; Krishnan, L.; Manjunath, G.; Sampangi, S.; Ramprakash, H. Observational Study to Evaluate the Clinical Efficacy of Thermalytix for Detecting Breast Cancer in Symptomatic and Asymptomatic Women. JCO Glob. Oncol. 2020, 6, 1472–1480. [Google Scholar] [CrossRef]
- Fakhoury, M. Artificial Intelligence in Psychiatry. Adv. Exp. Med. Biol. 2019, 1192, 119–125. [Google Scholar]
- Feeny, A.K.; Chung, M.K.; Madabhushi, A.; Attia, Z.I.; Cikes, M.; Firouznia, M.; Friedman, P.A.; Kalscheur, M.M.; Kapa, S.; Narayan, S.M.; et al. Artificial Intelligence and Machine Learning in Arrhythmias and Cardiac Electrophysiology. Circ. Arrhythm. Electrophysiol. 2020, 13, e007952. [Google Scholar] [CrossRef] [PubMed]
- Swietlik, D.; Bandurski, T.; Lass, P. Artificial neural networks in nuclear medicine. Nucl. Med. Rev. 2004, 7, 15318313. [Google Scholar]
- Swietlik, D.; Białowas, J. Application of Artificial Neural Networks to Identify Alzheimer’s Disease Using Cerebral Perfusion SPECT Data. Int. J. Environ. Res. Public Health 2019, 16, 1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Świetlik, D.; Białowąs, J.; Kusiak, A.; Cichońska, D. Memory and forgetting processes with the firing neuron model. Folia Morphol. 2018, 77, 221–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Świetlik, D. Simulations of Learning, Memory, and Forgetting Processes with Model of CA1 Region of the Hippocampus. Complexity 2018, 2018, 1297150. [Google Scholar] [CrossRef] [Green Version]
- Świetlik, D.; Białowąs, J.; Kusiak, A.; Cichońska, D. A computational simulation of long-term synaptic potentiation inducing protocol processes with model of CA3 hippocampal microcircuit. Folia Morphol. 2018, 77, 210–220. [Google Scholar] [CrossRef]
- Świetlik, D.; Białowąs, J.; Moryś, J.; Kusiak, A. Computer Model of Synapse Loss During an Alzheimer’s Disease-like Pathology in Hippocampal Subregions DG, CA3 and CA1—The Way to Chaos and Information Transfer. Entropy 2019, 21, 408. [Google Scholar] [CrossRef] [Green Version]
- Świetlik, D.; Białowąs, J.; Moryś, J.; Klejbor, I.; Kusiak, A. Effects of Inducing Gamma Oscillations in Hippocampal Subregions DG, CA3, and CA1 on the Potential Alleviation of Alzheimer’s Disease-Related Pathology: Computer Modeling and Simulations. Entropy 2019, 21, 587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Świetlik, D.; Białowąs, J.; Kusiak, A.; Krasny, M. Virtual Therapy with the NMDA Antagonist Memantine in Hippocampal. Models of Moderate to Severe Alzheimer’s Disease, in Silico Trials. Pharmaceuticals 2022, 15, 546. [Google Scholar] [CrossRef]
- Świetlik, D.; Kusiak, A.; Ossowska, A. Computational Modeling of Therapy with the NMDA Antagonist in Neurodegenerative Disease: Information Theory in the Mechanism of Action of Memantine. Int. J. Environ. Res. Public Health 2022, 19, 4727. [Google Scholar] [CrossRef]
- Świetlik, D.; Kusiak, A.; Krasny, M.; Białowąs, J. The Computer Simulation of Therapy with the NMDA Antagonist in Excitotoxic Neurodegeneration in an Alzheimer’s Disease—like Pathology. J. Clin. Med. 2022, 11, 1858. [Google Scholar] [CrossRef] [PubMed]
- Bishop, C. Neural Networks for Pattern Recognition; University Press: Oxford, UK, 1995. [Google Scholar]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions–Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Loe, H.; Theilade, E.; Jensen, S.B. Experimental gingivitis in man. J. Periodontol. 1965, 36, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Löe, H.; Anerud, A.; Boysen, H.; Morrison, E. Natural history of periodontal disease in man. Rapid, moderate and no loss of attachment in Sri Lankan laborers 14 to 46 years of age. J. Clin. Periodontol. 1986, 13, 431–445. [Google Scholar] [CrossRef]
- Kornman, K.S.; Crane, A.; Wang, H.Y.; di Giovine, F.S.; Newman, M.G.; Pirk, F.W.; Wilson, T.G.; Higginbottom, F.L., Jr.; Duff, G.W. The interleukin-1 genotype as a severity factor in adult periodontal disease. J. Clin. Periodontol. 1997, 24, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Page, R.C.; Kornman, K.S. The pathogenesis of human periodontitis: An introduction. Periodontology 2000, 1997, 9–11, 14. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S162–S170. [Google Scholar] [CrossRef]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontol. 2000 2013, 62, 59–94. [Google Scholar] [CrossRef]
- López, R.; Smith, P.C.; Göstemeyer, G.; Schwendicke, F. Ageing, dental caries and periodontal diseases. J. Clin. Periodontol. 2017, 44 (Suppl. S18), S145–S152. [Google Scholar] [CrossRef] [Green Version]
- Shiau, H.J.; Reynolds, M.A. Sex differences in destructive periodontal disease: Exploring the biologic basis. J. Periodontol. 2010, 81, 1505–1517. [Google Scholar] [CrossRef]
- Leite, F.; Nascimento, G.G.; Scheutz, F.; López, R. Effect of Smoking on Periodontitis: A Systematic Review and Meta-regression. Am. J. Prev. Med. 2018, 54, 831–841. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, T.; Walter, C.; Oluwagbemigun, K.; Bergmann, M.; Pischon, T.; Pischon, N.; Boeing, H. Smoking, Smoking Cessation, and Risk of Tooth Loss: The EPIC-Potsdam Study. J. Dent. Res. 2015, 94, 1369–1375. [Google Scholar] [CrossRef]
- Cairo, F.; Rotundo, R.; Frazzingaro, G.; Muzzi, L.; Pini Prato, G.P. Il diabete mellito come fattore di rischio per la parodontite [Diabetes mellitus as a risk factor for periodontitis]. Minerva Stomatol. 2001, 50, 321–330. [Google Scholar]
- Thanathornwong, B.; Suebnukarn, S. Automatic detection of periodontal compromised teeth in digital panoramic radiographs using faster regional convolutional neural networks. Imaging Sci. Dent. 2020, 50, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.T.; Kabir, T.; Nelson, J.; Sheng, S.; Meng, H.W.; Van Dyke, T.E.; Walji, M.F.; Jiang, X.; Shams, S. Use of the deep learning approach to measure alveolar bone level. J. Clin. Periodontol. 2022, 49, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.J.; Lee, S.J.; Yong, T.H.; Shin, N.Y.; Jang, B.G.; Kim, J.E.; Huh, K.H.; Lee, S.S.; Heo, M.S.; Choi, S.C.; et al. Deep Learning Hybrid Method to Automatically Diagnose Periodontal Bone Loss and Stage Periodontitis. Sci. Rep. 2020, 10, 7531. [Google Scholar] [CrossRef]
- Krois, J.; Ekert, T.; Meinhold, L.; Golla, T.; Kharbot, B.; Wittemeier, A.; Dörfer, C.; Schwendicke, F. Deep Learning for the Radiographic Detection of Periodontal Bone Loss. Sci. Rep. 2019, 9, 8495. [Google Scholar] [CrossRef]
- Ozden, F.O.; Özgönenel, O.; Özden, B.; Aydogdu, A. Diagnosis of periodontal diseases using different classification algorithms: A preliminary study. Niger. J. Clin. Pract. 2015, 18, 416–421. [Google Scholar] [CrossRef] [Green Version]
- Cha, J.Y.; Yoon, H.I.; Yeo, I.S.; Huh, K.H.; Han, J.S. Peri-Implant Bone Loss Measurement Using a Region-Based Convolutional Neural Network on Dental Periapical Radiographs. J. Clin. Med. 2021, 10, 1009. [Google Scholar] [CrossRef]
- Vadzyuk, S.; Boliuk, Y.; Luchynskyi, M.; Papinko, I.; Vadzyuk, N. Prediction of the Development of Periodontal Disease. Proc. Shevchenko Sci. Soc. Med. Sci. 2021, 65, 108–117. Available online: https://mspsss.org.ua/index.php/journal/article/view/363 (accessed on 22 January 2022). [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S313–S318. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Periodontitis Stage | Stage I | Stage II | Stage III | Stage IV | |
|---|---|---|---|---|---|
| Severity | Interdental CAL 1 at site of greatest loss | 1–2 mm | 3–4 mm | ≥5 mm | ≥5 mm |
| Radiographic bone loss | <15% | 15–33% | Extending to mid-third of the root or beyond | Extending to mid-third of the root or beyond | |
| Tooth loss | No tooths loss due to the periodontitis | No tooths loss due to the periodontitis | Tooth loss due to the periodontitis ≤ 4 | Tooth loss due to the periodontitis ≥ 5 | |
| Complexity | Local | Probing depth ≤ 4 mm | Probing depth ≤ 5 mm | Probing depth ≥ 6 mm | Criteria as in III stage plus: |
| Horizontal bone loss | Horizontal bone loss | Vertical bone loss ≥ 3 mm | Need for complex rehabilitation due to: | ||
| Furcation II or III class | -masticatory dysfunction -secondary occlusal trauma | ||||
| Moderate ridge defect | -severe occlusal defect -less than 10 opposing pairs of teeth | ||||
| Extent and distribution | Localized (<30% teeth involved), generalized, molar/incisor pattern | ||||
| Periodontitis Grade | Grade A: Slow Progression | Grade B: Moderate Progression | Grade C: Rapid Progression | ||
|---|---|---|---|---|---|
| Primary criteria | Direct evidence of progression | Longitudinal data | Evidence of no loss over 5 years | <2 mm over 5 years | ≥2 mm over 5 years |
| Indirect evidence of progression | % Bone loss/age | <0.25 | 0.25 to 1.0 | >1.0 | |
| Phenotype | Heavy biofilm deposits and slow progression | Progression corresponding with biofilm deposits | Rapid progression which exceeds amount of biofilm, early onset of disease | ||
| Grade modifiers | Risk factors | Smoking | Non-smoker | <10 cigarettes/day | ≥10 cigarettes/day |
| Diabetes | Normoglycemic | Diabetes HbA1c < 7.0% | Diabetes HbA1c ≥ 7.0% | ||
| Healthy (n = 10) | A (n = 15) | B (n = 43) | C (n = 42) | |
|---|---|---|---|---|
| Gender | ||||
| Female | 6 (60.0%) | 12 (80.0%) | 30 (69.8%) | 24 (57.1%) |
| Male | 4 (40.0%) | 3 (20.0%) | 13 (30.2%) | 18 (42.9%) |
| Grade | ||||
| gingivitis | 10 (100.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| 1 | 0 (0.0%) | 12 (80.0%) | 0 (0.0%) | 0 (0.0%) |
| 2 | 0 (0.0%) | 3 (20.0%) | 12 (27.9%) | 4 (9.5%) |
| 3 | 0 (0.0%) | 0 (0.0%) | 28 (65.1%) | 14 (33.3%) |
| Nicotinism | 1 (10.0%) | 1 (6.7%) | 2 (4.7%) | 21 (50.0%) |
| Age | 33.1 (4.7) | 43.1 (5.4) | 48.1 (6.8) | 45.8 (6.5) |
| API 1 (%) | 55.1 (27.1) | 64.7 (27.1) | 78.5 (21.3) | 87.3 (18.4) |
| BoP 2 (%) | 40.3 (34.9) | 47.2 (25.2) | 62.5 (33.1) | 66.7 (36.2) |
| PPD 3 (mm) | 2.1 (0.1) | 2.3 (0.1) | 2.8 (0.5) | 3.4 (0.9) |
| CAL 4 (mm) | - | 1.7 (1.3) | 3.4 (1.8) | 4.6 (2.4) |
| Training Group (n = 90) | Test Group (n = 20) | p-Value | |
|---|---|---|---|
| Gender | 0.5706 | ||
| Female | 60 (66.7%) | 12 (60.0%) | |
| Male | 30 (33.3%) | 8 (40.0%) | |
| Age mean (SD) | 45.5 (7.2) | 43.9 (8.9) | 0.3849 |
| Training Group (n = 90) | Test Group (n = 20) | p-Value | |
|---|---|---|---|
| API 1 | 79.8 (23.0) | 69.2 (25.7) | 0.0713 |
| BoP 2 | 60.2 (35.0) | 59.2 (31.6) | 0.9051 |
| PPD 3 | 2.9 (0.8) | 2.7 (0.7) | 0.1313 |
| CAL 4 | 3.6 (2.2) | 4.1 (2.2) | 0.3952 |
| Correctly% | |
|---|---|
| All | 84.2% |
| healthy | 80.0% |
| A | 100.0% |
| B | 80.0% |
| C | 80.0% |
| Gender | |
| Female | 90.9% |
| Male | 75.0% |
| Age (years) | |
| 20–30 | 100.0% |
| 30–40 | 80.0% |
| 40–50 | 83.3% |
| 50–60 | 85.7% |
| Cigarettes | |
| smoking | 100.0% |
| no smoking | 83.3% |
| Parameter | Correctly% |
|---|---|
| Cigarettes | 1.417 |
| API 1 | 1.052 |
| PPD 2 | 1.048 |
| Age | 1.038 |
| CAL 3 | 1.015 |
| Gender | 1.0 |
| BoP 4 | 0.994 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ossowska, A.; Kusiak, A.; Świetlik, D. Evaluation of the Progression of Periodontitis with the Use of Neural Networks. J. Clin. Med. 2022, 11, 4667. https://doi.org/10.3390/jcm11164667
Ossowska A, Kusiak A, Świetlik D. Evaluation of the Progression of Periodontitis with the Use of Neural Networks. Journal of Clinical Medicine. 2022; 11(16):4667. https://doi.org/10.3390/jcm11164667
Chicago/Turabian StyleOssowska, Agata, Aida Kusiak, and Dariusz Świetlik. 2022. "Evaluation of the Progression of Periodontitis with the Use of Neural Networks" Journal of Clinical Medicine 11, no. 16: 4667. https://doi.org/10.3390/jcm11164667
APA StyleOssowska, A., Kusiak, A., & Świetlik, D. (2022). Evaluation of the Progression of Periodontitis with the Use of Neural Networks. Journal of Clinical Medicine, 11(16), 4667. https://doi.org/10.3390/jcm11164667