
Anterior Pedicled Nasal Flap in Frontal Sinus Drill-Out Patients: A Randomised Controlled Pilot Study

 , , and
, , and 
Abstract
:1. Introduction and Objectives
1.1. Scientific Background
1.2. Study Objectives
2. Materials and Methods
2.1. Trial Design and Allocation Ratio
2.2. Participant Eligibility
2.3. Setting of Participant Recruitment
2.4. Randomisation and Intervention
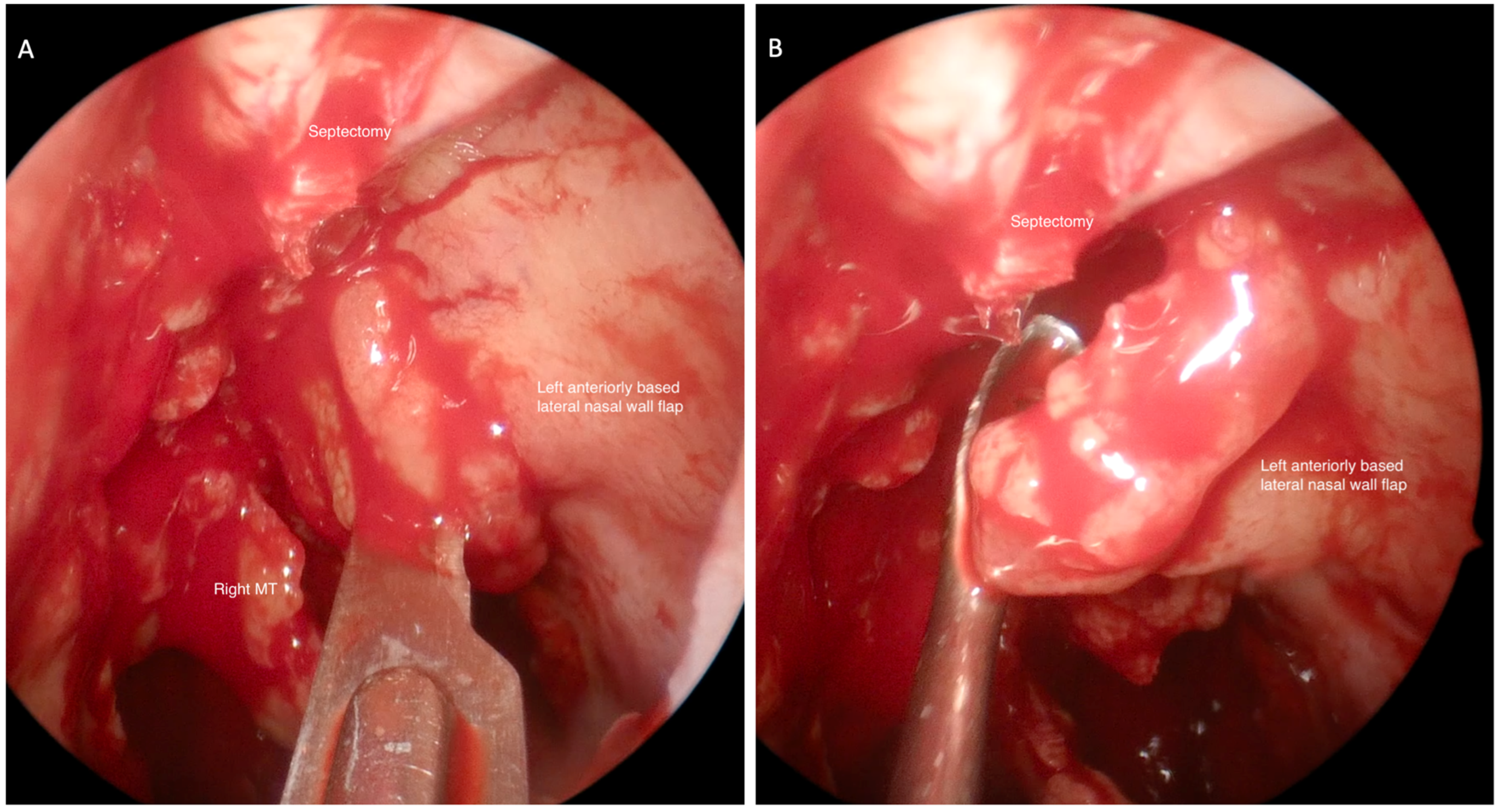
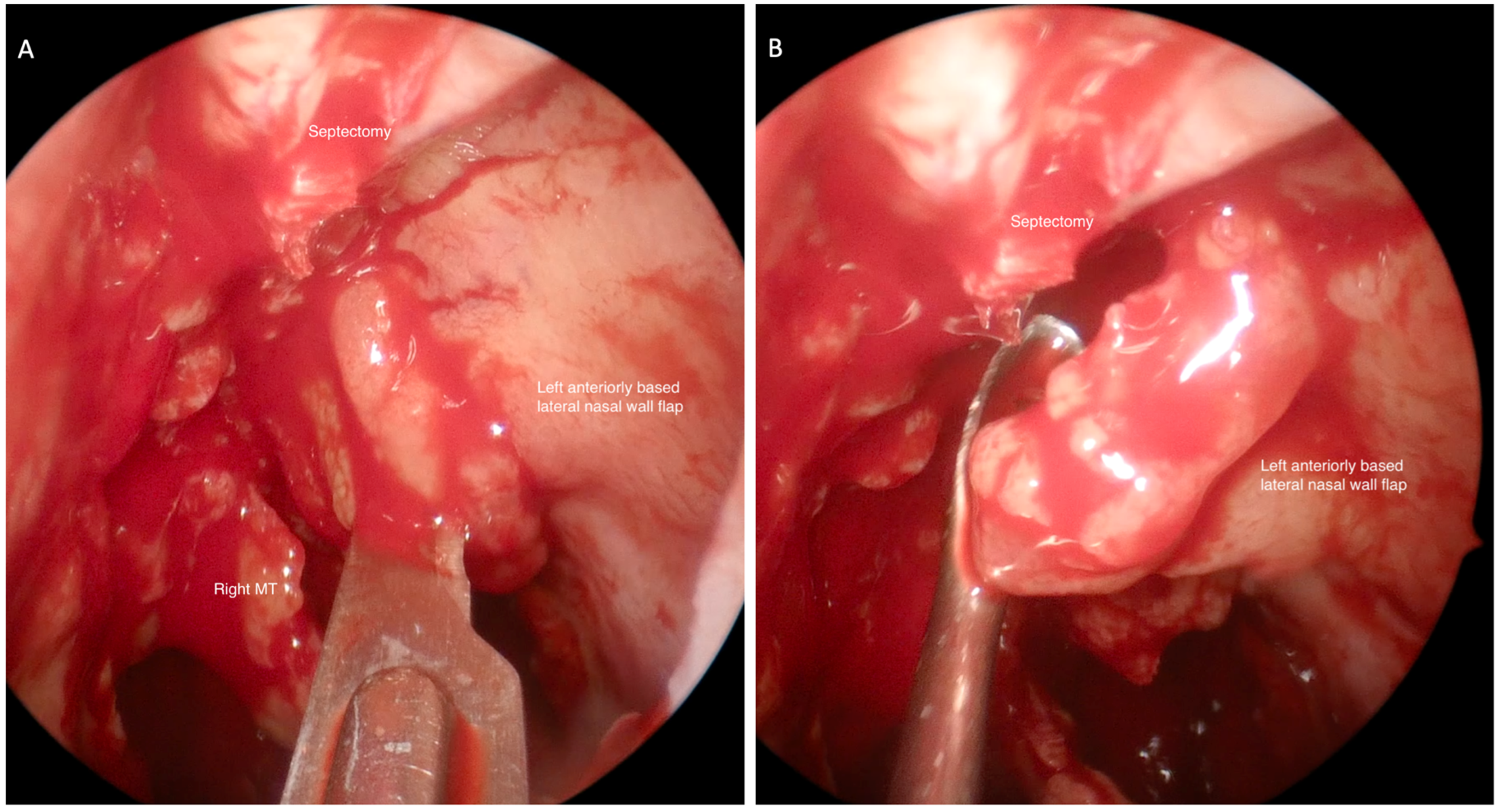
2.5. Surgical Technique
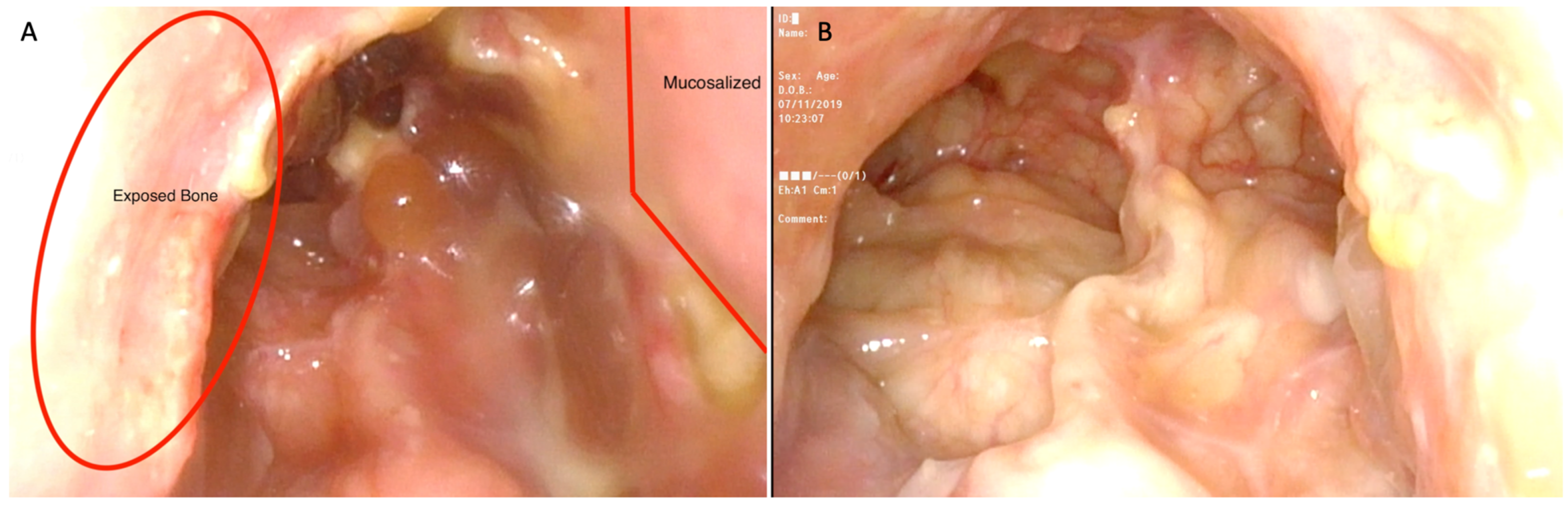
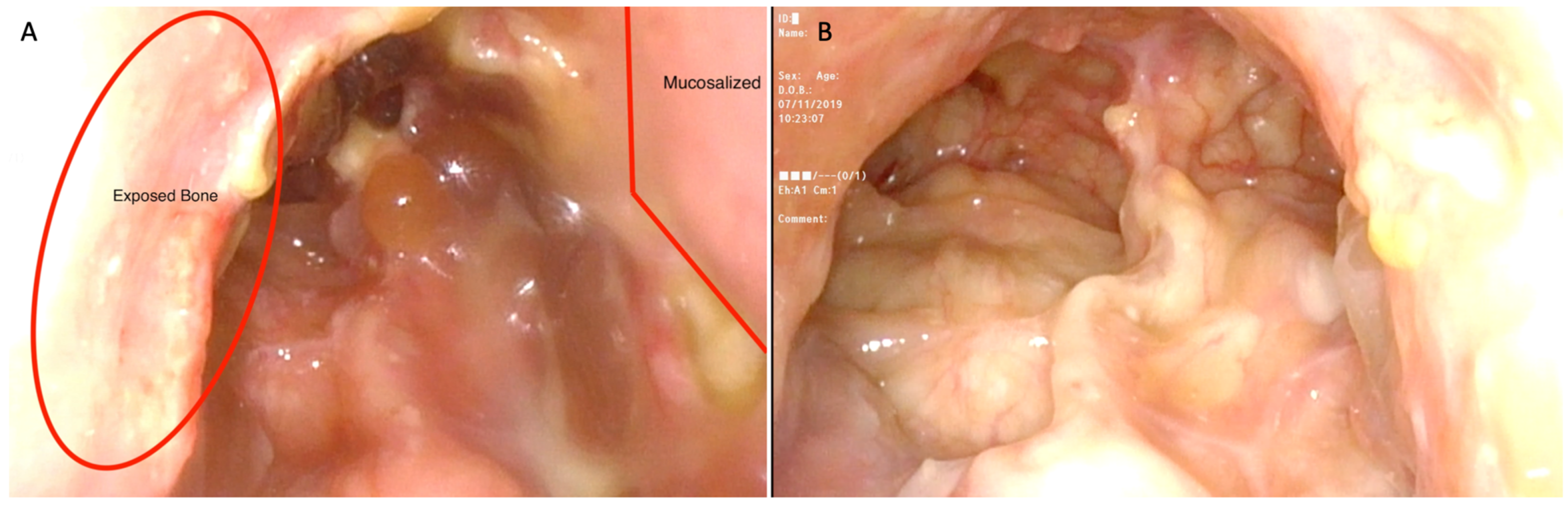
2.6. Study Outcomes
2.7. Sample Size
2.8. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Recruitment
3.3. Result Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Illing, E.A.; Cho, D.Y.; Riley, K.O.; Woodworth, B.A. Draf III mucosal graft technique: Long-term results. Int. Forum Allergy Rhinol. 2016, 6, 514–517. [Google Scholar] [CrossRef] [PubMed]
- Samaha, M.; Cosenza, M.J.; Metson, R. Endoscopic frontal sinus drillout in 100 patients. Arch. Otolaryngol.-Head Neck Surg. 2003, 129, 854–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Draf, W. Endonasal micro-endoscopic frontal sinus surgery: The fulda concept. Oper. Tech. Otolaryngol.-Head Neck Surg. 1991, 2, 234–240. [Google Scholar] [CrossRef]
- Gross, W.E.; Gross, C.W.; Becker, D.; Phillips, D.; Moore, D. Modified Transnasal Endoscopic Lothrop Procedure as an Alternative to Frontal Sinus Obliteration. Otolaryngol.-Head Neck Surg. 1995, 113, 427–434. [Google Scholar] [CrossRef]
- Wang, Y.P.; Shen, P.H.; Hsieh, L.C.; Wormald, P.J. Free mucosal grafts and anterior pedicled flaps to prevent ostium restenosis after endoscopic modified Lothrop (frontal drillout) procedure: A randomized, controlled study. Int. Forum Allergy Rhinol. 2019, 9, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Rajapaksa, S.P.; Ananda, A.; Cain, T.M.; Oates, L.; Wormald, P.J. Frontal ostium neo-osteogenesis and restenosis after modified endoscopic Lothrop procedure in an animal model. Clin. Otolaryngol. Allied Sci. 2004, 29, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.; Sindwani, R. Safety and efficacy of the endoscopic modified lothrop procedure: A systematic review and meta-analysis. Laryngoscope 2009, 119, 1828–1833. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Ye, T.; Huang, Z.; Huang, Q.; Xian, J.; Li, J.; Zhou, B. Clinical Predictors of Frontal Ostium Restenosis After Draf 3 Procedure for Refractory Chronic Rhinosinusitis. Am. J. Rhinol. Allergy 2018, 32, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.M.; on behalf of the PAFS Consensus Group; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. Pilot Feasibility Stud. 2016, 355, i5239. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, J.L.; Hubbard, M.A.; Huyett, P.; Patrie, J.T.; Borish, L.; Payne, S.C. Sino-nasal outcome test (SNOT-22): A predictor of postsurgical improvement in patients with chronic sinusitis. Ann. Allergy Asthma Immunol. 2013, 111, 246–251.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doty, R.L. Office procedures for quantitative assessment of olfactory function. Am. J. Rhinol. 2007, 21, 460–473. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.M.; Piccirillo, J.F.; Chandrasekhar, S.S.; Brook, I.; Kumar, K.A.; Kramper, M.; Orlandi, R.R.; Palmer, J.N.; Patel, Z.M.; Peters, A.; et al. Clinical practice guideline (update): Adult sinusitis. Otolaryngol.-Head Neck Surg. 2015, 152 (Suppl. 2), S1–S39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grayson, J.W.; Cavada, M.; Harvey, R.J. Clinically relevant phenotypes in chronic rhinosinusitis. J. Otolaryngol.-Head Neck Surg. 2019, 48, 23. [Google Scholar] [CrossRef] [PubMed]
- Tran, K.N.; Beule, A.G.; Singal, D.; Wormald, P.J. Frontal ostium restenosis after the endoscopic modified lothrop procedure. Laryngoscope 2007, 117, 1457–1462. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.C.; Sama, A. What is the evidence for the use of mucosal flaps in Draf III procedures. Curr. Opin. Otolaryngol. Head Neck Surg. 2014, 22, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Ting, J.Y.; Wu, A.; Metson, R. Frontal sinus drillout (modified Lothrop procedure): Long-term results in 204 patients. Laryngoscope 2014, 124, 1066–1070. [Google Scholar] [CrossRef] [PubMed]
- Wormald, P.J. Salvage frontal sinus surgery: The endoscopic modified Lothrop procedure. Laryngoscope 2003, 113, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Tzelnick, S.; Alkan, U.; Leshno, M.; Hwang, P.; Soudry, E. Sinonasal debridement versus no debridement for the postoperative care of patients undergoing endoscopic sinus surgery. Cochrane Database Syst. Rev. 2018, 2018, CD011988. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Participant Number | Flap Side | Time to Healing (Weeks) | |
|---|---|---|---|
| Non-Flap Side | Flap Side | ||
| 1 | right | 6 | 4 |
| 2 | left | 2 | 2 |
| 3 | left | 2 | 2 |
| 4 | Right | 6 | 2 |
| 5 | right | 2 | 2 |
| 6 | left | 4 | 6 |
| 7 | right | 6 | 4 |
| 8 | left | 4 | 4 |
| 9 | right | 6 | 6 |
| 10 | left | 6 | 6 |
| 11 | right | 4 | 4 |
| 12 | left | 4 | 4 |
| Average | 4.7 | 4.2 | |
| Median | 4 | 4 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bastianelli, M.; Huang, L.; Moore, P.; Iqbal, I.Z.; Woods, C.M.; Ooi, E.H. Anterior Pedicled Nasal Flap in Frontal Sinus Drill-Out Patients: A Randomised Controlled Pilot Study. J. Clin. Med. 2022, 11, 4329. https://doi.org/10.3390/jcm11154329
Bastianelli M, Huang L, Moore P, Iqbal IZ, Woods CM, Ooi EH. Anterior Pedicled Nasal Flap in Frontal Sinus Drill-Out Patients: A Randomised Controlled Pilot Study. Journal of Clinical Medicine. 2022; 11(15):4329. https://doi.org/10.3390/jcm11154329
Chicago/Turabian StyleBastianelli, Mark, Lucy Huang, Paige Moore, Isma Zafar Iqbal, Charmaine M. Woods, and Eng H. Ooi. 2022. "Anterior Pedicled Nasal Flap in Frontal Sinus Drill-Out Patients: A Randomised Controlled Pilot Study" Journal of Clinical Medicine 11, no. 15: 4329. https://doi.org/10.3390/jcm11154329
APA StyleBastianelli, M., Huang, L., Moore, P., Iqbal, I. Z., Woods, C. M., & Ooi, E. H. (2022). Anterior Pedicled Nasal Flap in Frontal Sinus Drill-Out Patients: A Randomised Controlled Pilot Study. Journal of Clinical Medicine, 11(15), 4329. https://doi.org/10.3390/jcm11154329