
Effects of Surgical Treatment for Obstructive Sleep Apnea on Renal and Survival Outcomes in Patients with Chronic Kidney Disease: A Taiwanese Nationwide Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
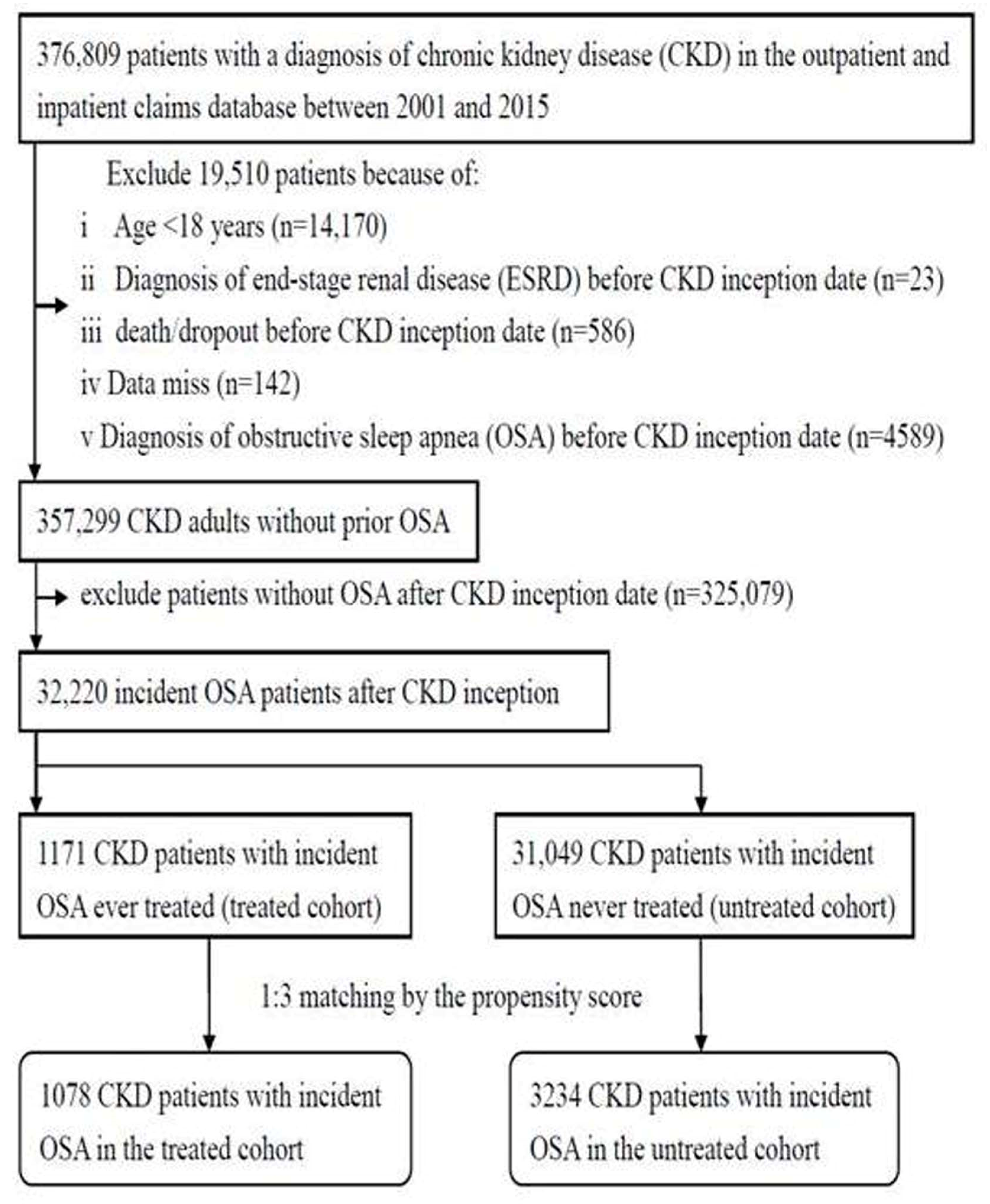
2.2. Study Population
2.3. Covariate
2.4. Study Outcomes
2.5. Statistical Analyses
3. Results
3.1. Demographic Characteristics of the CKD with Incident OSA Cohort
3.2. Fifteen-Year Cumulative Incidences and Risks of Study Outcomes
3.3. Subgroup Analysis of Mortality Outcome Stratified by Follow-Up Interval
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Chen, J.C.; Tsai, T.Y.; Li, C.Y.; Hwang, J.H. Obstructive Sleep Apnea and Risk of Parkinson’s Disease: A Population-Based Cohort Study. J. Sleep Res. 2015, 24, 432–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.C.; Koo, M.; Hwang, J.H. Risks of peripheral arterial occlusive disease in patients with obstructive sleep apnea: A population-based case-control study. Clin. Otolaryngol. 2015, 40, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.C.; Hwang, J.H. Sleep Apnea Increased Incidence of Primary Central Nervous System Cancers: A nationwide cohort study. Sleep Med. 2014, 15, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.W.; Duffy, J.F. Sleep, sleep disorders, and sexual dysfunction. World J. Mens Health 2019, 37, 261–275. [Google Scholar] [CrossRef]
- Hwang, J.H.; Ong, H.L.; Chen, J.C. Surgical treatments for obstructive sleep apnea decrease the risk of erectile dysfunction: A nationwide cohort study. Andrology 2022, 10, 477–485. [Google Scholar] [CrossRef]
- Koo, M.; Hwang, J.H. Risk of tinnitus in patients with sleep apnea: A nationwide, population-based case-control study. Laryngoscope 2017, 127, 2171–2175. [Google Scholar] [CrossRef]
- Mashaqi, S.; Gozal, D. The impact of obstructive sleep apnea and PAP therapy on all-cause and cardiovascular mortality based on age and gender—A literature review. Respir. Investig. 2020, 58, 7–20. [Google Scholar] [CrossRef]
- Pollicina, I.; Maniaci, A.; Lechien, J.R.; Iannella, G.; Vicini, C.; Cammaroto, G.; Cannavicci, A.; Magliulo, G.; Pace, A.; Cocuzza, S.; et al. Neurocognitive Performance Improvement after Obstructive Sleep Apnea Treatment: State of the Art. Behav. Sci. 2021, 11, 180. [Google Scholar] [CrossRef]
- Umbro, I.; Fabiani, V.; Fabiani, M.; Angelico, F.; Del Ben, M. A systematic review on the association between obstructive sleep apnea and chronic kidney disease. Sleep Med. Rev. 2020, 53, 101337. [Google Scholar] [CrossRef]
- Voulgaris, A.; Marrone, O.; Bonsignore, M.R.; Steiropoulos, P. Chronic kidney disease in patients with obstructive sleep apnea. A narrative review. Sleep Med. Rev. 2019, 47, 74–89. [Google Scholar] [CrossRef]
- Lin, C.H.; Lurie, R.C.; Lyons, O.D. Sleep apnea and chronic kidney disease: A state-of-the-art review. Chest 2020, 157, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Nigam, G.; Camacho, M.; Chang, E.T.; Riaz, M. Exploring sleep disorders in patients with chronic kidney disease. Nat. Sci. Sleep 2018, 10, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, H.S.; Kim, H.Y.; Han, K.D.; Jung, J.H.; Kim, C.S.; Bae, E.H.; Ma, S.K.; Kim, S.W. Obstructive sleep apnea as a risk factor for incident end stage renal disease: A nationwide population-based cohort study from Korea. Clin. Exp. Nephrol. 2019, 23, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Chen, H.T.; Yeh, C.C.; Hung, S.K.; Yu, B.H. Four prescribed Chinese herbal medicines provide renoprotection and survival benefit without hyperkalemia risk in patients with advanced chronic kidney disease: A nationwide cohort study. Phytomedicine 2022, 95, 153873. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Lin, H.Y.; Li, C.Y.; Lee, M.S.; Su, Y.C. A nationwide cohort study suggests that hepatitis C virus infection is associated with increased risk of chronic kidney disease. Kidney Int. 2014, 85, 1200–12078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, M.Y.; Chiu, Y.W.; Chang, J.S.; Lin, H.L.; Lee, T.C.; Chiu, G.F.; Kuo, M.C.; Wu, M.T.; Chen, H.C.; Hwang, S.J. Association of prescribed Chinese herbal medicine use with risk of end-stage renal disease in patients with chronic kidney disease. Kidney Int. 2015, 88, 1365–1373. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.C.; Wu, C.J.; Lin, C.J.; Pan, C.F.; Chen, C.Y.; Huang, T.M.; Wu, C.H.; Lin, S.L.; Chen, Y.M.; Chen, L.; et al. Pentoxifylline decreases dialysis risk in patients with advanced chronic kidney disease. Clin. Pharmacol. Ther. 2015, 98, 442–449. [Google Scholar] [CrossRef]
- Wu, C.Y.; Chen, Y.J.; Ho, H.J.; Hsu, Y.C.; Kuo, K.N.; Wu, M.S.; Lin, J.T. Association between nucleoside analogues and risk of hepatitis B virus–related hepatocellular carcinoma recurrence following liver resection. JAMA 2012, 308, 1906–1914. [Google Scholar] [CrossRef] [Green Version]
- Nowicki, M.; Zawiasa-Bryszewska, A.; Taczykowska, M.; Białasiewicz, P.; Nowak, D. The pattern of overnight changes in novel markers of acute kidney injury in patients with obstructive sleep apnea. Adv. Clin. Exp. Med. 2020, 29, 1065–1072. [Google Scholar] [CrossRef]
- Hui, L.; Benca, R. The Bidirectional Relationship Between Obstructive Sleep Apnea and Chronic Kidney Disease. J. Stroke Cerebrovasc. Dis. 2021, 30, 105652. [Google Scholar] [CrossRef]
- Lin, C.H.; Perger, E.; Lyons, O.D. Obstructive sleep apnea and chronic kidney disease. Curr. Opin. Pulm. Med. 2018, 24, 549–554. [Google Scholar] [CrossRef]
- Choi, J.H.; Kim, E.J.; Choi, J.; Kwon, S.Y.; Lee, H.M.; Kim, T.H.; Lee, S.H.; Shin, C.; Lee, S.H. Effect of successful surgical treatment on changes of position during sleep in adults with obstructive sleep apnea syndrome. Ann. Otol. Rhinol. Laryngol. 2011, 120, 104–109. [Google Scholar] [CrossRef]
- Woods, C.M.; Gunawardena, I.; Chia, M.; Vowles, N.J.; Ullah, S.; Robinson, S.; Carney, A.S. Long-term quality-of-life outcomes following treatment for adult obstructive sleep apnea: Comparison of upper airway surgery, continuous positive airway pressure and mandibular advancement splints. Clin. Otolaryngol. 2016, 41, 762–770. [Google Scholar] [CrossRef]
- Khafagy, A.H. Treatment of obstructive sleep apnoea as a therapeutic modality for associated erectile dysfunction. Int. J. Clin. Pract. 2012, 66, 1204–1208. [Google Scholar] [CrossRef]
- Shin, H.W.; Park, J.H.; Park, J.W.; Rhee, C.S.; Lee, C.H.; Min, Y.G.; Kim, D.Y. Effects of surgical vs. nonsurgical therapy on erectile dysfunction and quality of life in obstructive sleep apnea syndrome: A pilot study. J. Sex. Med. 2013, 10, 2053–2059. [Google Scholar] [CrossRef]
- Konstantinopoulou, S.; Tapia, I.E. Neurocognitive and behaviouraloutcomes following intervention for obstructive sleep apnoeasyndrome in children. Paediatr. Respir. Rev. 2016, 20, 51–54. [Google Scholar] [CrossRef]
- Kataoka, T.; Enomoto, F.; Kim, R.; Yokoi, H.; Fujimori, M.; Sakai, Y.; Ando, I.; Ichikawa, G.; Ikeda, K. The effect of surgical treatment of obstructive sleep apnea syndrome on the plasma TNF-alpha levels. Tohoku J. Exp. Med. 2004, 204, 267–272. [Google Scholar] [CrossRef] [Green Version]
- Halle, T.R.; Oh, M.S.; Collop, N.A.; Quyyumi, A.A.; Bliwise, D.L.; Dedhia, R.C. Surgical Treatment of OSA on Cardiovascular Outcomes: A Systematic Review. Chest 2017, 152, 1214–1229. [Google Scholar] [CrossRef]
- Brietzke, S.E.; Ishman, S.L.; Cohen, S.; Cyr, D.D.; Shin, J.J.; Kezirian, E.J. National database analysis of single-level versus multilevel sleep surgery. Otolaryngol. Head Neck Surg. 2017, 156, 955–961. [Google Scholar] [CrossRef]
- Friedman, J.J.; Salapatas, A.M.; Bonzelaar, L.B.; Hwang, M.S.; Friedman, M. Changing rates of morbidity and mortality in obstructive sleep apnea surgery. Otolaryngol. Head Neck Surg. 2017, 157, 123–127. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Propensity Score-Matched CKD Patients with Incident OSA (n = 4312) | p-Value | |
|---|---|---|---|
| Treated Cohort | Untreated Cohort | ||
| (n = 1078) | (n = 3234) | ||
| Sex, n (%) | 0.97 | ||
| Men | 719 (66.7) | 2155 (66.6) | |
| Women | 359 (33.3) | 10797 (33.4) | |
| Age (year), n (%) | 0.99 | ||
| 18–34 | 235 (21.8) | 710 (22.0) | |
| 35–44 | 272 (25.2) | 806 (24.9) | |
| 45–54 | 291 (27.0) | 877 (27.1) | |
| ≧55 | 280 (26.0) | 841 (26.0) | |
| Mean (±SD) | 46.1 ± 13.5 | 46.9 ± 14.6 | 0.10 |
| Comorbidities, n (%) | |||
| Diabetes | 122 (11.3) | 326 (10.1) | 0.25 |
| Hypertension | 303 (28.1) | 893 (27.6) | 0.75 |
| Coronary heart disease | 106 (9.8) | 2969 (9.22) | 0.51 |
| Hyperlipidemia | 188 (17.4) | 544 (16.8) | 0.64 |
| Chronic liver disease | 111 (10.3) | 394 (9.2) | 0.24 |
| Charlson comorbidity index, n (%) | 0.89 | ||
| 0 | 5311 (49.3) | 1592 (49.2) | |
| 1 | 2324 (21.5) | 728 (22.5) | |
| 2 | 1779 (16.4) | 516 (16.0) | |
| ≧3 | 198 (12.8) | 398 (12.3) | |
| Mean (±SD) | 0.99 ± 1.25 | 0.98 ± 1.24 | 0.78 |
| Number of medical visits, n (%) | 0.99 | ||
| 1–12 | 345 (32.0) | 1041 (32.2) | |
| 13–24 | 338 (31.4) | 1009 (31.2) | |
| ≧25 | 395 (36.6) | 1184 (36.6) | |
| Mean (±SD) | 23.6 ± 19.3 | 23.0 ± 18.3 | 0.37 |
| Confounding drug use, n (%) | |||
| ACEI/ARB | 200 (18.6) | 565 (17.5) | 0.42 |
| Outcomes | Treated Cohort (n = 1.078) | Untreated Cohort (n = 3.234) | p-Value | Adjusted HR (95% CI) | p-Value |
|---|---|---|---|---|---|
| ESRD | 0.38 * (0.15–0.97) | 0.043 | |||
| Mean follow-up (±SD) | 4.5 ± 3.6 | 4.7 ± 3.6 | |||
| Event (n, %) | 5 (0.5) | 41 (1.3) | |||
| Cumulative incidence (%, 95% CI) | 0.76% (0.26–1.85%) | 1.19% (0.79–1.74%) | 0.037 | ||
| Overall mortality | 2.54 # (1.79–3.59) | <0.0001 | |||
| Mean follow-up (±SD) | 4.5 ± 3.6 | 4.7 ± 3.6 | |||
| Event (n, %) | 53 (4.9) | 85 (2.6) | |||
| Cumulative incidence (%, 95% CI) | 5.57% (4.06–7.40%) | 2.54% (1.91–3.30%) | <0.0001 | ||
| Cardiovascular mortality | 1.46 # (0.29–7.22) | 0.64 | |||
| Mean follow-up (±SD) | 4.5 ± 3.6 | 4.7 ± 3.6 | |||
| Event (n, %) | 2 (0.2) | 7 (0.2) | |||
| Cumulative incidence (%, 95% CI) | 0.29% (0.06–1.05%) | 0.28% (0.11–0.64%) | 0.89 | ||
| Non-cardiovascular mortality | 2.62 # (1.83–3.75) | <0.0001 | |||
| Mean follow-up (±SD) | 4.5 ± 3.6 | 4.7 ± 3.6 | |||
| Event (n, %) | 51 (4.7) | 78 (2.4) | |||
| Cumulative incidence (%, 95% CI) | 5.29% (3.83–7.08%) | 2.26% (1.68–2.98%) | <0.0001 |
| Follow-Up Interval | Overall Mortality | Cardiovascular Mortality | Non-Cardiovascular Mortality | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Event | Adjusted HR | p-Value | Event | Adjusted HR | p-Value | Event | Adjusted HR | p-Value | |
| 0–3 months | |||||||||
| Untreated (n = 3.234) | 4 | 1 (Reference) | 0 | 1 (Reference) | 4 | 1 (Reference) | |||
| Treated (n = 1.078) | 10 | 8.81 | 0.0003 | 1 | Not converged | 9 | 7.84 | 0.0007 | |
| >3 months | |||||||||
| Untreated (n = 3.234) | 81 | 1 (Reference) | 7 | 1 (Reference) | 74 | 1 (Reference) | |||
| Treated (n = 1.078) | 43 | 2.18 | <0.0001 | 1 | 0.90 | 0.93 | 42 | 2.30 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, J.-H.; Yu, B.-H.; Chen, Y.-C. Effects of Surgical Treatment for Obstructive Sleep Apnea on Renal and Survival Outcomes in Patients with Chronic Kidney Disease: A Taiwanese Nationwide Cohort Study. J. Clin. Med. 2022, 11, 4411. https://doi.org/10.3390/jcm11154411
Hwang J-H, Yu B-H, Chen Y-C. Effects of Surgical Treatment for Obstructive Sleep Apnea on Renal and Survival Outcomes in Patients with Chronic Kidney Disease: A Taiwanese Nationwide Cohort Study. Journal of Clinical Medicine. 2022; 11(15):4411. https://doi.org/10.3390/jcm11154411
Chicago/Turabian StyleHwang, Juen-Haur, Ben-Hui Yu, and Yi-Chun Chen. 2022. "Effects of Surgical Treatment for Obstructive Sleep Apnea on Renal and Survival Outcomes in Patients with Chronic Kidney Disease: A Taiwanese Nationwide Cohort Study" Journal of Clinical Medicine 11, no. 15: 4411. https://doi.org/10.3390/jcm11154411
APA StyleHwang, J.-H., Yu, B.-H., & Chen, Y.-C. (2022). Effects of Surgical Treatment for Obstructive Sleep Apnea on Renal and Survival Outcomes in Patients with Chronic Kidney Disease: A Taiwanese Nationwide Cohort Study. Journal of Clinical Medicine, 11(15), 4411. https://doi.org/10.3390/jcm11154411