
Factors Associated with Failed Trial of Labor after Cesarean, among Women with Twin Gestation—A Multicenter Retrospective Cohort Study


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Study Outcomes
2.4. Statistical Analysis
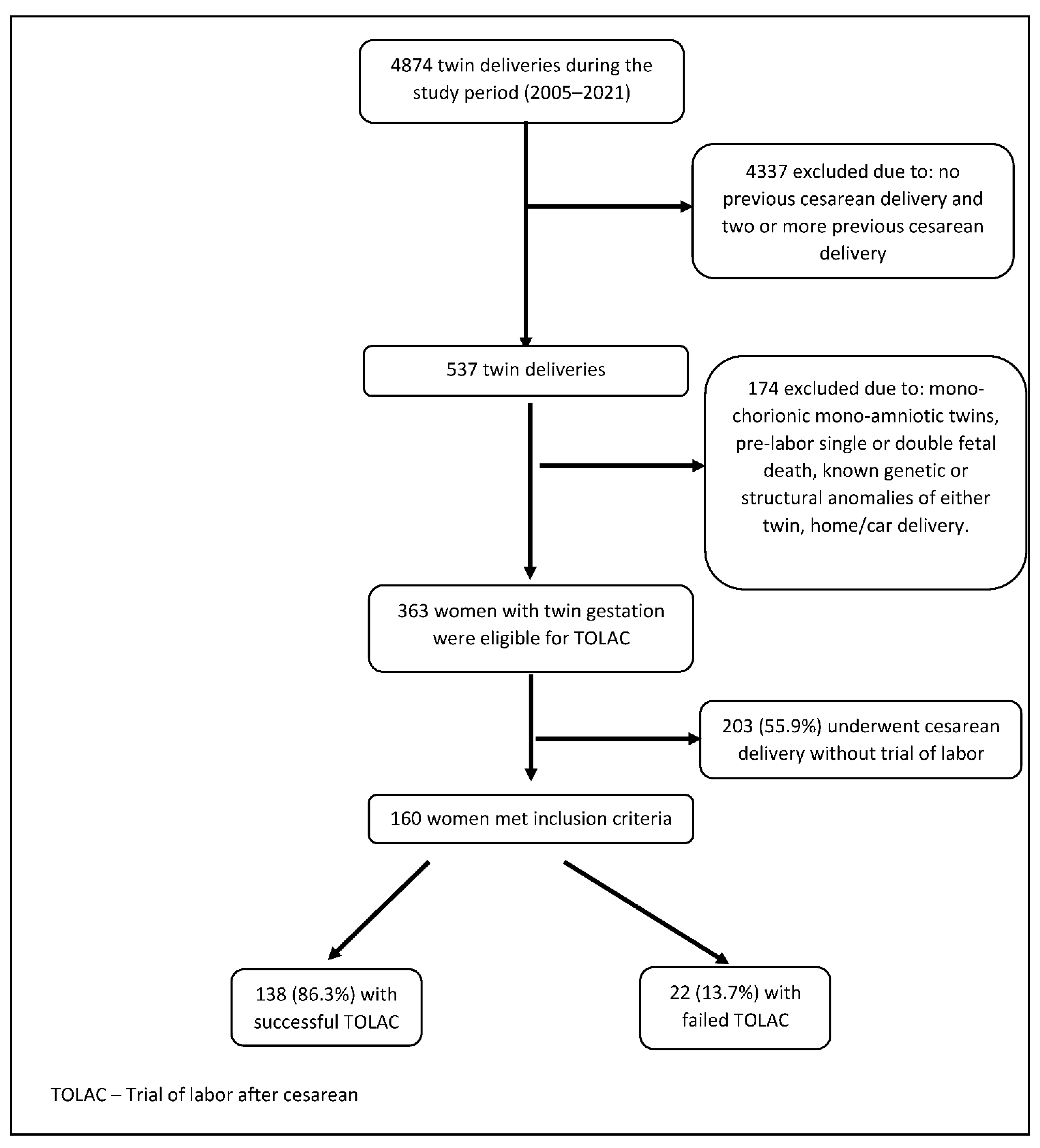
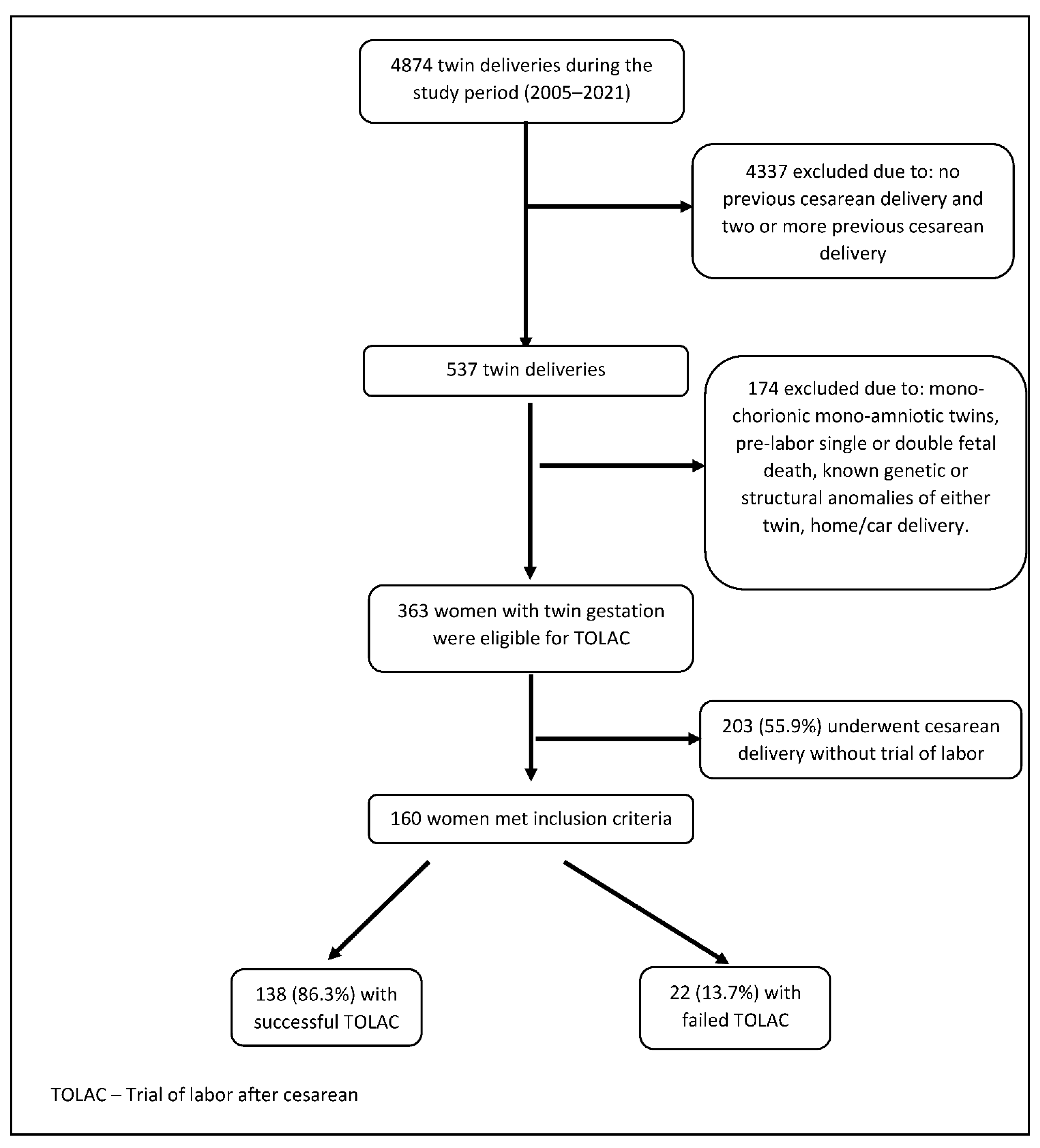
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sandall, J.; Tribe, R.M.; Avery, L.; Mola, G.; Visser, G.H.; Homer, C.S.; Gibbons, D.; Kelly, N.M.; Kennedy, H.P.; Kidanto, H.; et al. Short-term and long-term effects of caesarean section on the health of women and children. Lancet Lond. Engl. 2018, 392, 1349–1357. [Google Scholar] [CrossRef]
- Junior, L.C.M.; Famá, E.A.B.; Zamboni, J.W.; Awada, P.F.; Araújo, T.A.; Nascimento-Ferreira, M.V.; De Carvalho, H.B. Risk score for failed trial of vaginal birth after a previous cesarean section including data of labor course. J. Obstet. Gynaecol. Res. 2020, 46, 93–103. [Google Scholar] [CrossRef] [PubMed]
- El-Sayed, Y.Y.; Watkins, M.M.; Fix, M.; Druzin, M.L.; Pullen, K.M.; Caughey, A.B. Perinatal outcomes after successful and failed trials of labor after cesarean delivery. Am. J. Obstet. Gynecol. 2007, 196, 583.e1–583.e5. [Google Scholar] [CrossRef] [PubMed]
- Levin, G.; Yagel, S.; Schwartz, A.; Many, A.; Rosenbloom, J.I.; Yinon, Y.; Meyer, R. Trial of labor after cesarean in twin gestation with no prior vaginal delivery–evidence from largest cohort reported. Int. J. Gynecol. Obstet. 2022, 2022, 14090. [Google Scholar] [CrossRef] [PubMed]
- Lopian, M.; Kashani-Ligumski, L.; Cohen, R.; Assaraf, S.; Herzlich, J.; Lessing, J.B.; Perlman, S. Twin TOLAC is an independent risk factor for adverse maternal and neonatal outcome. Arch. Gynecol. Obstet. 2021, 304, 1433–1441. [Google Scholar] [CrossRef] [PubMed]
- Cahill, A.; Stamilio, D.M.; Paré, E.; Peipert, J.P.; Stevens, E.J.; Nelson, D.B.; Macones, G.A. Vaginal birth after cesarean (VBAC) attempt in twin pregnancies: Is it safe? Am. J. Obstet. Gynecol. 2005, 193, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Shinar, S.; Agrawal, S.; Hasan, H.; Berger, H. Trial of labor versus elective repeat cesarean delivery in twin pregnancies after a previous cesarean delivery—A systematic review and meta-analysis. Birth 2019, 46, 550–559. [Google Scholar] [CrossRef]
- Myles, T. Vaginal birth of twins after a previous Cesarean section. J. Matern. Neonatal Med. 2001, 10, 171–174. [Google Scholar] [CrossRef]
- Aaronson, D.; Harlev, A.; Sheiner, E.; Levy, A. Trial of labor after cesarean section in twin pregnancies: Maternal and neonatal safety. J. Matern. Neonatal Med. 2010, 23, 550–554. [Google Scholar] [CrossRef]
- Committee on Practice Bulletins-Obstetrics. ACOG Practice Bulletin No. 205: Vaginal Birth After Cesarean Delivery. Obstet. Gynecol. 2019, 133, e110–e127. [Google Scholar] [CrossRef]
- Schmitz, T.; Carnavalet, C.D.C.; Azria, E.; Lopez, E.; Cabrol, D.; Goffinet, F. Neonatal Outcomes of Twin Pregnancy According to the Planned Mode of Delivery. Obstet. Gynecol. 2008, 111, 695–703. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Practice Bulletin No. 169 Summary: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal Pregnancies. Obstet. Gynecol. 2016, 128, 926–928. [Google Scholar] [CrossRef]
- Barrett, J.F.; Hannah, M.E.; Hutton, E.K.; Willan, A.R.; Allen, A.C.; Armson, B.A.; Gafni, A.; Joseph, K.; Mason, D.; Ohlsson, A.; et al. A Randomized Trial of Planned Cesarean or Vaginal Delivery for Twin Pregnancy. N. Engl. J. Med. 2013, 369, 1295–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hochler, H.; Tevet, A.; Barg, M.; Suissa-Cohen, Y.; Lipschuetz, M.; Yagel, S.; Aviram, A.; Mei-Dan, E.; Melamed, N.; Barrett, J.F.; et al. Trial of labor of vertex-nonvertex twins following a previous cesarean delivery. Am. J. Obstet. Gynecol. MFM 2022, 4, 100640. [Google Scholar] [CrossRef]
- Kabiri, D.; Masarwy, R.; Schachter-Safrai, N.; Masarwa, R.; Raccah, B.H.; Ezra, Y.; Matok, I. Trial of labor after cesarean delivery in twin gestations: Systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2019, 220, 336–347. [Google Scholar] [CrossRef]
- Ford, A.A.; Bateman, B.T.; Simpson, L.L. Vaginal birth after cesarean delivery in twin gestations: A large, nationwide sample of deliveries. Am. J. Obstet. Gynecol. 2006, 195, 1138–1142. [Google Scholar] [CrossRef]
- Baradaran, K. Risk of Uterine Rupture with Vaginal Birth after Cesarean in Twin Gestations. Obstet. Gynecol. Int. 2021, 2021, 6693142. [Google Scholar] [CrossRef]
- Trojano, G.; Damiani, G.R.; Olivieri, C.; Villa, M.; Malvasi, A.; Alfonso, R.; Loverro, M.; Cicinelli, E. VBAC: Antenatal predictors of success. Acta Bio Med. Atenei Parm. 2019, 90, 300–309. [Google Scholar] [CrossRef]
- Grisaru-Granovsky, S.; Bas-Lando, M.; Drukker, L.; Haouzi, F.; Farkash, R.; Samueloff, A.; Ioscovich, A. Epidural analgesia at trial of labor after cesarean (TOLAC): A significant adjunct to successful vaginal birth after cesarean (VBAC). J. Périnat. Med. 2018, 46, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Domingues, A.P.; Dinis, S.R.; Belo, A.; Couto, D.; Fonseca, E.; Moura, P. Impact of induced pregnancies in the obstetrical outcome of twin pregnancies. Fertil Steril. 2014, 101, 172–177. [Google Scholar] [CrossRef]
- Okby, R.; Druyan, Y.; Sonenklar, M.; Aricha-Tamir, B.; Sacks, K.N.; Sheiner, E. Fertility treatment as a risk factor for maternal request of cesarean delivery in twin pregnancies. Arch Gynecol Obstet. 2016, 294, 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, E.A.; Chapman, M.G.; Wang, Y.A.; Adamson, G.D. Population-based study of cesarean section after in vitro fertilization in Australia. Birth 2010, 37, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Diamant, H.; Okby, R.; Imterat, M.; Sergienko, R.; Sheiner, E. Trial of labor after cesarean in twin gestations: Does it increase maternal or neonatal complications? Harefuah 2016, 155, 547–550. [Google Scholar] [PubMed]

{kind=link}
| Successful TOLAC N = 138 | Failed TOLAC N = 22 | p Value | |
|---|---|---|---|
| Maternal age, years | 32.5 ± 5.1 | 32.3 ± 5.2 | 0.82 |
| Miscarriages, any | 56 (40.6%) | 8 (36.4%) | 0.71 |
| Miscarriages ≥3 | 13 (9.4%) | 2 (9.1%) | 0.96 |
| Gravidity | 5.6 ± 3.2 | 4.5 ± 2 | 0.14 |
| Parity | 4.8 ± 2.6 | 3.9 ± 1.9 | 0.11 |
| Fertility Treatments | 24 (17.4%) | 8 (36.4%) | 0.04 |
| Hypertensive disorders of pregnancy | 7 (5.1%) | 2 (9.1%) | 0.45 |
| Smoking | 3 (2.4%) | 0 (0%) | 0.48 |
| Diabetes (pre-gestational & gestational) | 10 (7.2%) | 1 (4.5%) | 0.64 |
| Obesity (BMI ≥ 30) | 9 (18%) | 2 (22.2%) | 0.77 |
| Monochorionic diamniotic | 17 (12.6%) | 6 (27.3%) | 0.07 |
| Anemia (Hb < 11 mg/dL) on admission | 21 (15.2%) | 4 (18.2%) | 0.72 |
| Cervical dilation on admission | 4 ± 2.1 | 2.8 ± 2.2 | 0.03 |
| Number of vaginal exams | 5.4 ± 3.5 | 4.9 ± 3.7 | 0.55 |
| Induction of labor | 8 (5.8%) | 3 (14.3%) | 0.16 |
| Oxytocin augmentation of labor | 97 (70.3%) | 10 (45.5%) | 0.02 |
| Meconium-stained amniotic fluid | 8 (5.8%) | 0 (0%) | 0.25 |
| Epidural analgesia | 119 (86.2%) | 11 (50%) | <0.01 |
| Gestational age at delivery | 36.8 ± 1.9 | 34.9 ± 5 | <0.01 |
| Gestational age at delivery <37 week | 53 (38.4%) | 12 (54.5%) | 0.15 |
| Duration of first stage of labor | 276.8 ± 273.4 | 193.5 ± 102.5 | 0.67 |
| Duration of second stage of labor | 391.3 ± 987.7 | 562.7 ± 273.9 | 0.57 |
| Placental abruption | 4 (2.9%) | 3 (13.6%) | 0.02 |
| Premature rupture of membranes | 24 (17.4%) | 0 (0%) | 0.03 |
| Inter-twin delivery interval | 9.3 ± 10.2 | 5.8 ± 13 | 0.15 |
| Twins birthweight discordancy, grams | −32.1 ± 360.3 | 19.7 ± 394.4 | 0.54 |
| Birth weight difference, percentage | −2.3 ± 15 | −1.7 ± 18.7 | 0.85 |
| Vertex presentation of second twin | 66 (47.8%) | 12 (54.5%) | 0.56 |
| Successful TOLAC N = 138 | Failed TOLAC N = 22 | p Value | |
|---|---|---|---|
| Hospitalization length, days | 3.2 ± 1.1 | 5.4 ± 1.7 | <0.01 |
| Prolonged hospitalization | 6 (4.3%) | 5 (22.7%) | <0.01 |
| Retained placenta/placental fragments | 13 (9.4%) | 0 (0%) | 0.40 |
| Perineal tear grade 3/4 | 0 (0%) | 0 (0%) | N/A |
| Laceration | 2 (1.4%) | 0 (0%) | 0.57 |
| Episiotomy | 11 (8%) | 0 (0%) | 0.17 |
| Vaginal tear | 11 (8%) | 0 (0%) | 0.17 |
| Maternal ICU admissions | 0 (0%) | 0 (0%) | N/A |
| Postpartum hemorrhage | 30 (21.7%) | 7 (31.8%) | 0.30 |
| Hemoglobin drop ≥4 g/dL | 10 (7.4%) | 2 (9.1%) | 0.78 |
| Chorioamnionitis | 1 (0.7%) | 1 (4.5%) | 0.14 |
| Endometritis | 2 (1.4%) | 3 (13.6%) | <0.01 |
| Blood products transfusion | 5 (3.6%) | 1 (4.5%) | 0.83 |
| Dehiscence of Uterine Scar | 0 (0%) | 0 (0%) | N/A |
| Uterine rupture | 0 (0%) | 0 (0%) | N/A |
| Hysterectomy | 0 (0%) | 0 (0%) | N/A |
| Laparotomy | 0 (0%) | 0 (0%) | N/A |
| First Twin | Second Twin | |||||
|---|---|---|---|---|---|---|
| Successful TOLAC N = 138 | Failed TOLAC N = 22 | p Value | Successful TOLAC N = 138 | Failed TOLAC N = 22 | p Value | |
| Birthweight | 2579.9 ± 479 | 2299.9 ± 845.4 | 0.03 | 2547.1 ± 475.6 | 2319.6 ± 895 | 0.07 |
| LGA | 24 (17.4%) | 3 (13.6%) | 0.66 | 19 (13.8%) | 8 (36.4%) | <0.01 |
| SGA | 2 (1.4%) | 0 (0%) | 0.57 | 7 (5.1%) | 1 (4.5%) | 0.92 |
| Male gender | 67 (48.6%) | 11 (50%) | 0.90 | 71 (51.4%) | 8 (36.4%) | 0.19 |
| 1-Minute Apgar score <7 | 4 (2.9%) | 3 (13.6%) | 0.02 | 15 (10.9%) | 6 (27.3%) | 0.03 |
| 5-Minute Apgar score <7 | 1 (0.7%) | 1 (4.5%) | 0.14 | 2 (1.4%) | 2 (9.1%) | 0.03 |
| NICU admission | 33 (23.9%) | 10 (45.5%) | 0.03 | 40 (29%) | 11 (50%) | 0.049 |
| Hospitalization length, days | 6 ± 6.7 | 21 ± 29.7 | <0.01 | 6.7 ± 8.7 | 25.8 ± 42.3 | <0.01 |
| Prolonged hospitalization | 38 (27.5%) | 12 (54.5%) | 0.01 | 41 (29.7%) | 10 (45.5%) | 0.14 |
| Meconium aspiration syndrome | 0 (0%) | 0 (0%) | N/A | 0 (0%) | 0 (0%) | N/A |
| Jaundice | 9 (6.7%) | 3 (13.6%) | 0.26 | 11 (8.4%) | 3 (13.6%) | 0.43 |
| TTN | 7 (5.2%) | 1 (4.5%) | 0.89 | 5 (3.8%) | 4 (18.2%) | <0.01 |
| Mechanical ventilation | 6 (4.5%) | 4 (18.2%) | 0.01 | 4 (3.1%) | 5 (22.7%) | <0.01 |
| Seizures | 1 (0.7%) | 0 (0%) | 0.69 | 1 (0.8%) | 1 (4.5%) | 0.15 |
| Erb’s palsy/fracture of clavicle | 0 (0%) | 0 (0%) | N/A | 0 (0%) | 0 (0%) | N/A |
| Hypoglycemia | 16 (11.9%) | 2 (9.1%) | 0.70 | 12 (9.2%) | 2 (9.1%) | 0.99 |
| Sepsis | 1 (0.7%) | 1 (4.5%) | 0.14 | 0 (0%) | 0 (0%) | N/A |
| Encephalopathy | 0 (0%) | 0 (0%) | N/A | 1 (0.8%) | 1 (4.5%) | 0.15 |
| Intracranial hemorrhage | 1 (0.7%) | 3 (13.6%) | <0.01 | 3 (2.3%) | 2 (9.1%) | 0.10 |
| Birth asphyxia | 1 (0.7%) | 1 (4.5%) | 0.14 | 2 (1.5%) | 0 (0%) | 0.56 |
| p Value | aOR | 95% CI | ||
|---|---|---|---|---|
| Cervical dilation on admission | <0.01 | 0.6 | 0.40 | 0.82 |
| No oxytocin augmentation of labor | 0.02 | 5.2 | 1.36 | 19.73 |
| Gestational age at delivery, weeks | 0.047 | 0.8 | 0.65 | 1.00 |
| Lack of epidural analgesia | 0.049 | 4.5 | 1.01 | 20.16 |
| Fertility Treatments | 0.58 | 1.5 | 0.38 | 5.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peled, T.; Sela, H.Y.; Joseph, J.; Martinotti, T.; Grisaru-Granovsky, S.; Rottenstreich, M. Factors Associated with Failed Trial of Labor after Cesarean, among Women with Twin Gestation—A Multicenter Retrospective Cohort Study. J. Clin. Med. 2022, 11, 4256. https://doi.org/10.3390/jcm11154256
Peled T, Sela HY, Joseph J, Martinotti T, Grisaru-Granovsky S, Rottenstreich M. Factors Associated with Failed Trial of Labor after Cesarean, among Women with Twin Gestation—A Multicenter Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(15):4256. https://doi.org/10.3390/jcm11154256
Chicago/Turabian StylePeled, Tzuria, Hen Y. Sela, Jordanna Joseph, Tal Martinotti, Sorina Grisaru-Granovsky, and Misgav Rottenstreich. 2022. "Factors Associated with Failed Trial of Labor after Cesarean, among Women with Twin Gestation—A Multicenter Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 15: 4256. https://doi.org/10.3390/jcm11154256
APA StylePeled, T., Sela, H. Y., Joseph, J., Martinotti, T., Grisaru-Granovsky, S., & Rottenstreich, M. (2022). Factors Associated with Failed Trial of Labor after Cesarean, among Women with Twin Gestation—A Multicenter Retrospective Cohort Study. Journal of Clinical Medicine, 11(15), 4256. https://doi.org/10.3390/jcm11154256