
Pregnancies and Gynecological Follow-Up after Solid Organ Transplantation: Experience of a Decade

 ,
,  ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
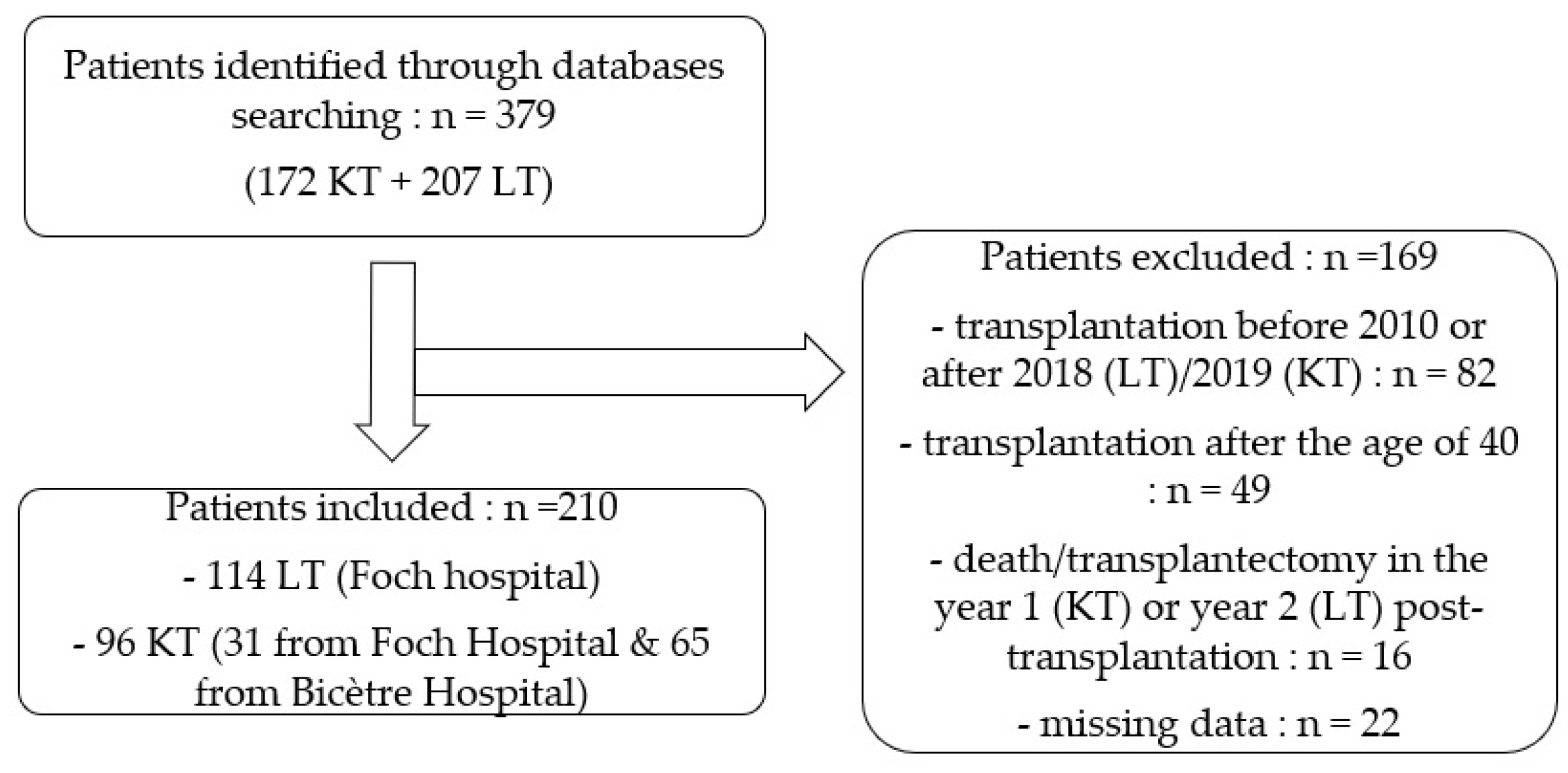
2.1. Study Design
2.2. Data Collection
- Women aged 15 to 40 years at organ transplantation.
- At least one year after kidney transplantations and two years after lung transplantations, in line with recommendations to reduce possible complications.
- No objection recorded for inclusion in medical research.
2.3. Statistical Analyses
3. Results
3.1. Patient Medical Histories and Demographic Characteristics
3.2. Patient Clinical Profiles at and after Transplantations
3.3. Pregnancies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Axelrod, D.A.; Schnitzler, M.A.; Xiao, H.; Irish, W.; Tuttle-Newhall, E.; Chang, S.H.; Kasiske, B.L.; Alhamad, T.; Lentine, K.L. An economic assessment of contemporary kidney transplant practice. Am. J. Transplant. 2018, 18, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Roux, A.; Sage, E.; Cerf, C.; Le Guen, M.; Picard, C.; Hamid, A.M.; Parquin, F.; Stern, M.; Bonnette, P. Evolution and progress of lung transplantation: An analysis of a cohort of 600 lung transplant patients at the Hospital Foch. Rev. Mal. Respir. 2019, 36, 142–154. [Google Scholar] [CrossRef] [PubMed]
- The French Agency of Biomedicine. Press Release. 11 February 2021. Available online: https://www.agence-biomedecine.fr/IMG/pdf/cp_abm___bilan_activite-greffes_2020.pdf (accessed on 27 February 2022).
- Leroy, C.; Rigot, J.M.; Leroy, M.; Decanter, C.; Le Mapihan, K.; Parent, A.S.; Le Guillou, A.C.; Yakoub-Agha, I.; Dharancy, S.; Noel, C.; et al. Immunosuppressive drugs and fertility. Orphanet J. Rare Dis. 2015, 10, 136. [Google Scholar] [CrossRef] [PubMed]
- Bos, S.; Vos, R.; Van Raemdonck, D.E.; Verleden, G.M. Survival in adult lung transplantation: Where are we in 2020? Curr. Opin. Organ Transplant. 2020, 25, 268–273. [Google Scholar] [CrossRef]
- Poggio, E.D.; Augustine, J.J.; Arrigain, S.; Brennan, D.C.; Schold, J.D. Long-term kidney transplant graft survival—Making progress when most needed. Am. J. Transplant. 2021, 21, 2824–2832. [Google Scholar] [CrossRef]
- Rupley, D.M.; Janda, A.M.; Kapeles, S.R.; Wilson, T.M.; Berman, D.; Mathur, A.K. Preconception counseling, fertility, and pregnancy complications after abdominal organ transplantation: A survey and cohort study of 532 recipients. Clin. Transplant. 2014, 28, 937–945. [Google Scholar] [CrossRef]
- Krajewski, C.; Sucato, G. Reproductive health care after transplantation. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 1222–1234. [Google Scholar] [CrossRef]
- McKay, D.B. Pregnancy in Recipients of Solid Organs—Effects on Mother and Child. N. Engl. J. Med. 2006, 354, 1281–1293. [Google Scholar] [CrossRef]
- Källén, B.; Westgren, M.; Åberg, A.; Olausson, P.O. Pregnancy outcome after maternal organ transplantation in Sweden. BJOG Int. J. Obstet. Gynaecol. 2005, 112, 904–909. [Google Scholar] [CrossRef]
- Mak, R.H.; Hoffman, H.M. Outcomes of prenatal immunosuppression. Nat. Rev. Nephrol. 2015, 11, 390–391. [Google Scholar] [CrossRef]
- Richman, K.; Gohh, R. Pregnancy after renal transplantation: A review of registry and single-center practices and outcomes. Nephrol. Dial. Transplant. 2012, 27, 3428–3434. [Google Scholar] [CrossRef]
- Josephson, M.A.; McKay, D.B. Pregnancy and Kidney Transplantation. Semin. Nephrol. 2011, 31, 100–110. [Google Scholar] [CrossRef]
- Bachmann, F.; Budde, K.; Gerland, M.; Wiechers, C.; Heyne, N.; Nadalin, S.; Brucker, S.; Bachmann, C. Pregnancy following kidney transplantation-impact on mother and graft function and focus on childrens’ longitudinal development. BMC Pregnancy Childbirth 2019, 19, 376. [Google Scholar] [CrossRef]
- Stoumpos, S.; McNeill, S.H.; Gorrie, M.; Mark, P.B.; Brennand, J.E.; Geddes, C.C.; Deighan, C.J. Obstetric and long-term kidney outcomes in renal transplant recipients: A 40-yr single-center study. Clin. Transplant. 2016, 30, 673–681. [Google Scholar] [CrossRef]
- Shaner, J.; Coscia, L.A.; Constantinescu, S.; McGrory, C.H.; Doria, C.; Moritz, M.J.; Armenti, V.T.; Cowan, S.W. Pregnancy after Lung Transplant. Prog. Transplant. 2012, 22, 134–140. [Google Scholar] [CrossRef]
- Al Khalaf, S.; Bodunde, E.; Maher, G.M.; O’Reilly, É.J.; McCarthy, F.P.; O’Shaughnessy, M.M.; O’Neill, S.M.; Khashan, A.S. Chronic kidney disease and adverse pregnancy outcomes: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021, 226, 656–670.e32. [Google Scholar] [CrossRef]
- Wyld, M.L.; Clayton, P.A.; Kennedy, S.E.; Alexander, S.I.; Chadban, S.J. Pregnancy Outcomes for Kidney Transplant Recipients with Transplantation as a Child. JAMA Pediatr. 2015, 169, e143626. [Google Scholar] [CrossRef]
- Mastrobattista, J.M.; Gomez-Lobo, V. Pregnancy After Solid Organ Transplantation. Obstet. Gynecol. 2008, 112, 919–932. [Google Scholar] [CrossRef]
- Kilpatrick, S.K.; Ecker, J.L. Severe maternal morbidity: Screening and review. Am. J. Obstet. Gynecol. 2016, 215, B17–B22. [Google Scholar] [CrossRef]
- Friedman, R.L. Ethical Considerations Related to Pregnancy in Transplant Recipients. N. Engl. J. Med. 2006, 354, 1313. [Google Scholar]
- Wainwright, C.E.; Elborn, J.S.; Ramsey, B.W.; Marigowda, G.; Huang, X.; Cipolli, M.; Colombo, C.; Davies, J.C.; De Boeck, K.; Flume, P.A.; et al. Lumacaftor-Ivacaftor in Patients with Cystic Fibrosis Homozygous for Phe508del CFTR. N. Engl. J. Med. 2015, 373, 220–231. [Google Scholar] [CrossRef]
- Taylor-Cousar, J.L.; Jain, R. Maternal and fetal outcomes following elexacaftor-tezacaftor-ivacaftor use during pregnancy and lactation. J. Cyst. Fibros. 2021, 20, 402–406. [Google Scholar] [CrossRef]
- Boyd, J.M.; Mehta, A.; Murphy, D.J. Fertility and pregnancy outcomes in men and women with cystic fibrosis in the United Kingdom. Hum. Reprod. 2004, 19, 2238–2243. [Google Scholar] [CrossRef]
- Paulen, M.E.; Folger, S.G.; Curtis, K.M.; Jamieson, D.J. Contraceptive use among solid organ transplant patients: A systematic review. Contraception 2010, 82, 102–112. [Google Scholar] [CrossRef]
- Krajewski, C.M.; Geetha, D.; Gomez-Lobo, V. Contraceptive Options for Women with a History of Solid-Organ Transplantation. Transplantation 2013, 95, 1183–1186. [Google Scholar] [CrossRef]
- Kallapur, A.; Jang, C.; Yin, O.; Mei, J.Y.; Afshar, Y. Pregnancy care in solid organ transplant recipients. Int. J. Gynecol. Obstet. 2022, 157, 502–513. Available online: http://onlinelibrary.wiley.com/doi/abs/10.1002/ijgo.13819 (accessed on 27 February 2022). [CrossRef]
- French, V.A.; Davis, J.S.; Sayles, H.S.; Wu, S.S. Contraception and Fertility Awareness among Women With Solid Organ Transplants. Obstet. Gynecol. 2013, 122, 809–814. [Google Scholar] [CrossRef]
- Rafie, S.; Lai, S.; Garcia, J.E.; Mody, S.K. Contraceptive use in female recipients of a solid-organ transplant. Prog. Transpl. 2014, 24, 344–348. [Google Scholar] [CrossRef]
- Klitzke, S.; Wender, I.O.; Salcedo, M.P.; Pessini, S.A. Cervical cancer screening abnormalities in immunosuppressed renal transplant women: Case–control study in Southern Brazil. Arch. Gynecol. Obstet. 2020, 302, 649–655. [Google Scholar] [CrossRef]
- Park, S.T.; Song, M.J.; Park, J.S.; Hur, S.Y.; Lee, C.W. Incidence and clinicopathologic behavior of uterine cervical carcinoma in renal transplant recipients. World J. Surg. Oncol. 2011, 9, 72. [Google Scholar] [CrossRef]
- Rousset Jablonski, C.; Reynaud, Q.; Perceval, M.; Nove-Josserand, R.; Durupt, S.; Lega, J.C.; Durieu, I. Contraceptive practices and cervical screening in women with cystic fibrosis. Hum. Reprod. 2015, 30, 2547–2551. [Google Scholar] [CrossRef] [PubMed]
- Danziger-Isakov, L.; Kumar, D.; AST ID Community of Practice. Vaccination of solid organ transplant candidates and recipients: Guidelines from the American society of transplantation infectious diseases community of practice. Clin. Transplant. 2019, 33, e13563. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.W.; Wilt, J.; Restaino, S. Pregnancy After Thoracic Organ Transplantation. Semin. Perinatol. 2007, 31, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Coscia, L.A.; Constantinescu, S.; Davison, J.M.; Moritz, M.J.; Armenti, V.T. Immunosuppressive drugs and fetal outcome. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 1174–1187. [Google Scholar] [CrossRef]
- Thakrar, M.V.; Morley, K.; Lordan, J.L.; Meachery, G.; Fisher, A.J.; Parry, G.; Corris, P.A. Pregnancy after lung and heart-lung transplantation. J. Heart Lung Transplant. 2014, 33, 593–598. [Google Scholar] [CrossRef]
- Edenborough, F.P. Women with cystic fibrosis and their potential for reproduction. Thorax 2001, 56, 649–655. [Google Scholar] [CrossRef]
- Lockwood, G.M.; Ledger, W.L.; Barlow, D.H. Successful pregnancy outcome in a renal transplant patient following in-vitro fertilization. Hum. Reprod. 1995, 10, 1528–1530. [Google Scholar] [CrossRef]
- Davison, J.M. Dialysis, Transplantation, and Pregnancy. Am. J. Kidney Dis. 1991, 17, 127–132. [Google Scholar] [CrossRef]
- Bry, C.; Hubert, D.; Reynaud-Gaubert, M.; Dromer, C.; Mal, H.; Roux, A.; Boussaud, V.; Claustre, J.; le Pavec, J.; Murris-Espin, M.; et al. Pregnancy after lung and heart-lung transplantation: A French multicentre retrospective study of 39 pregnancies. ERJ Open Res. 2019, 5, 00254-2018. [Google Scholar] [CrossRef]
- Kovač, D.; Kovač, L.; Mertelj, T.; Steblovnik, L. Pregnancy after Kidney Transplantation. Transplant. Proc. 2021, 53, 1080–1084. [Google Scholar] [CrossRef]
- Methods for Managing Miscarriage: A Network Meta-Analysis-Ghosh, J-2021|Cochrane Library. Available online: https://www-cochranelibrary-com.ezproxy.u-paris.fr/cdsr/doi/10.1002/14651858.CD012602.pub2/full (accessed on 2 June 2022).
- Sciarra, J.J.; Toledo-Pereyra, L.H.; Bendel, R.P.; Simmons, R.L. Pregnancy following renal transplantation. Am. J. Obstet. Gynecol. 1975, 123, 411–425. [Google Scholar] [CrossRef]
- Merkatz, I.R.; Schwartz, G.H.; David, D.S.; Stenzel, K.H.; Riggio, R.R.; Whitsell, J.C. Resumption of Female Reproductive Function Following Renal Transplantation. JAMA 1971, 216, 1749–1754. [Google Scholar] [CrossRef]
- Starzl, T.E.; Fung, J.; Jordan, M.; Shapiro, R.; Tzakis, A.; McCauley, J.; Johnston, J.; Iwaki, Y.; Jain, A.; Alessiani, M.; et al. Kidney Transplantation Under FK 506. JAMA J. Am. Med. Assoc. 1990, 264, 63–67. [Google Scholar] [CrossRef]
- Durst, J.K.; Rampersad, R.M. Pregnancy in Women With Solid-Organ Transplants: A Review. Obstet. Gynecol. Surv. 2015, 70, 408–418. [Google Scholar] [CrossRef]
- Kainz, A.; Harabacz, I.; Cowlrick, I.S.; Gadgil, S.; Hagiwara, D. Analysis of 100 pregnancy outcomes in women treated systemically with tacrolimus. Transpl. Int. 2000, 13, S299–S300. [Google Scholar] [CrossRef]
- Roman, A.S. Pregnancy After Transplant—Addressing Mode of Obstetrical Delivery among Solid Organ Transplant Recipients. JAMA Netw. Open 2021, 4, e2127414. [Google Scholar] [CrossRef]
- Yin, O.; Kallapur, A.; Coscia, L.; Kwan, L.; Tandel, M.; Constantinescu, S.; Moritz, M.J.; Afshar, Y. Mode of Obstetric Delivery in Kidney and Liver Transplant Recipients and Associated Maternal, Neonatal, and Graft Morbidity During 5 Decades of Clinical Practice. JAMA Netw. Open 2021, 4, e2127378. [Google Scholar] [CrossRef]
- Brännström, M. Introduction. Fertil Steril. 2019, 112, 1–2. [Google Scholar] [CrossRef]
- The French Agency of Biomedicine. Available online: https://rams.agence-biomedecine.fr/greffe-renale-0 (accessed on 27 February 2022).



{kind=link}
{kind=link}
{kind=link}
| Lung Transplantation n = 114 | Kidney Transplantation n = 96 | p-Value | |||
|---|---|---|---|---|---|
| Age at SOT, years | 27.6 ± 5.59 1 | 31.1 ± 5.93 | <0.001 | ||
| BMI at SOT, kg/m2 | 18.0 ± 2.15 | 23.6 ± 5.39 (n = 79) | <0.001 | ||
| History of | |||||
| Hypertension | 3 (2.6%) 2 | 68 (70.8%) | <0.001 | ||
| Diabetes mellitus | 55 (48.2%) | 19 (19.8%) | <0.001 | ||
| Gyn. cancer | 1 (0.9%) | 0 | 1.000 | ||
| Gravidity (G) | <0.001 | ||||
| G0 | 86 (75.4%) | 47 (49.0%) | |||
| ≥G1 | 28 (24.6%) | 49 (51.0%) | |||
| Parity (P) | <0.001 | ||||
| P0 | 94 (82.5%) | 53 (55.2%) | |||
| ≥P1 | 20 (17.5%) | 43 (44.8%) | |||
| History of pre-eclampsia | n = 9 | n = 20 | |||
| (of n: ≥P1) | 0 | 12 (60.0%) | 0.003 | ||
| Etiology | CF Bronch. Fibrosis Other 3 PCD | 104 (91.2%) 4 (3.5%) 3 (2.6%) 2 (1.8%) 1 (0.9%) | Glom. Unknown Diabetes Interst. Vasc. PKD Other 4 | 25 (26.0%) 19 (19.8%) 13 (13.5%) 6 (6.3%) 5 (5.2%) 5 (5.2%) 23 (24%) | |
| Duration on dialysis before SOT, years | NA | n = 93 2.34 ± 2.23 | |||
| Lung Transplantation n = 114 | Kidney Transplantation n = 96 | p Value | |
|---|---|---|---|
| Multi-SOT | 3 (2.6%) 1 | 15 (15.6%) | <0.001 |
| IS therapy (year 1) by | |||
| MMF | 98 (86%) | 84 (87.5%) | 0.744 |
| Tacrolimus | 113 (99.1%) | 92 (95.8%) | 0.181 |
| CTS | 114 (100%) | 93 (96.9%) | 0.094 |
| Other | 17 (14.9%) | 16 (16.7%) | 0.728 |
| ≥1 T rejection | 75 (65.8%) | 16 (16.7%) | <0.001 |
| 1st rejection type: | n = 75 | n = 16 | |
| Antibody-mediated | 6 (8.0%) | 8 (50.0%) | <0.001 |
| Cellular | 64 (85.3%) | 5 (31.3%) | <0.001 |
| Combined | 5 (6.7%) | 3 (18.8%) | 0.143 |
| GFR 2 (mL/min/1.73 m2) 1 year after SOT 2 years after SOT | NA | 59 3 ± 23 (n = 83) 57 ± 24 (n = 72) | |
| FEV1 4 (%) 1 year after SOT 2 years after SOT | 81.1 ± 17.6 82.3 ± 18.2 (n = 112) | NA | |
| Gyn. cancer after SOT | 1 (0.88%) | 1 (1.04%) | 1.000 |
| Contraception after SOT | n = 81 | n = 41 | |
| Progestin | 52 (64.2%) | 24 (58.5%) | 0.542 |
| Copper IUD/condom | 13 (16.1%) | 9 (22.0%) | 0.423 |
| Estrogen + progestin | 15 (18.5%) | 7 (17.1%) | 0.844 |
| Other | 1 (1.2%) | 1 (2.4%) | 0.621 |
| Cervical conization after SOT | n = 25 3 (12.0%) | n = 12 3 (25.0%) | 0.366 |
| Total Pregnancies n = 33 | Pregnancies in LT Group: n = 11 (114 Patients) | Pregnancies in KT Group: n = 22 (96 Patients) | p Value | |
|---|---|---|---|---|
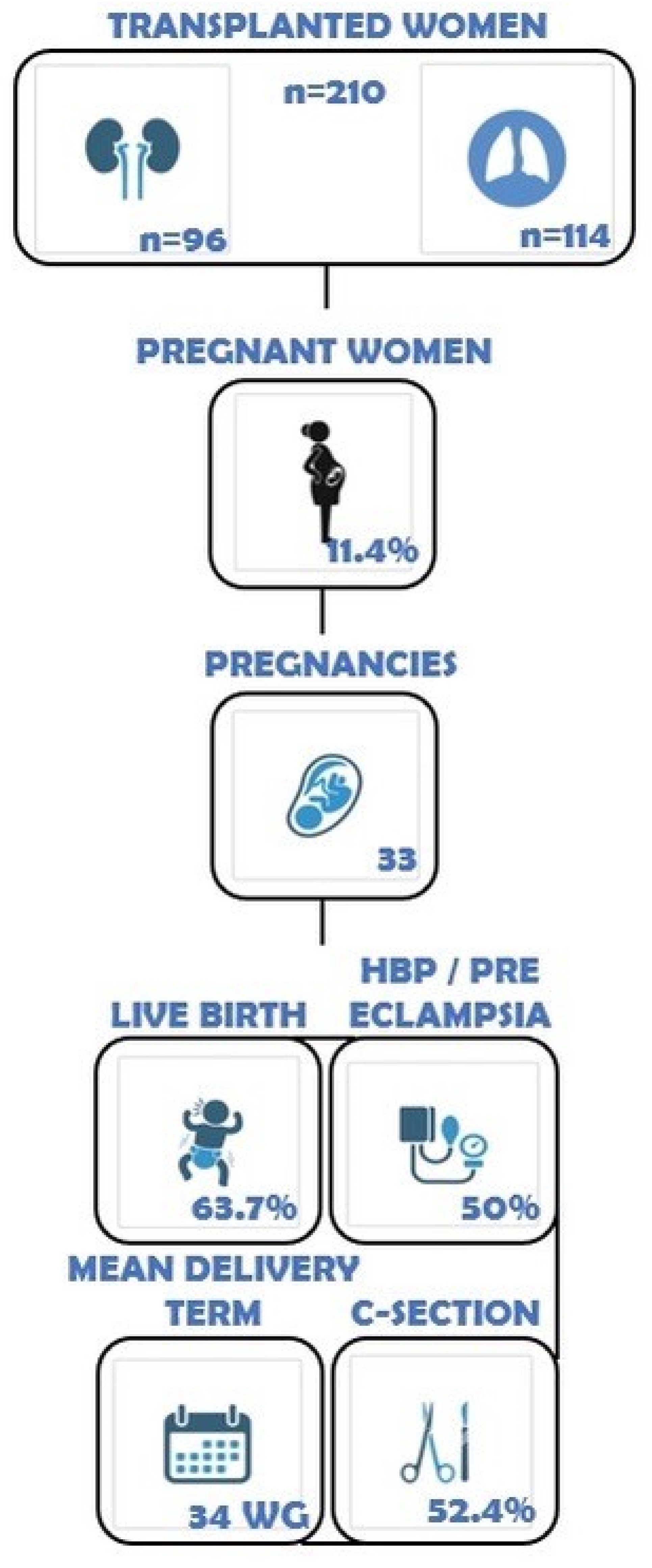
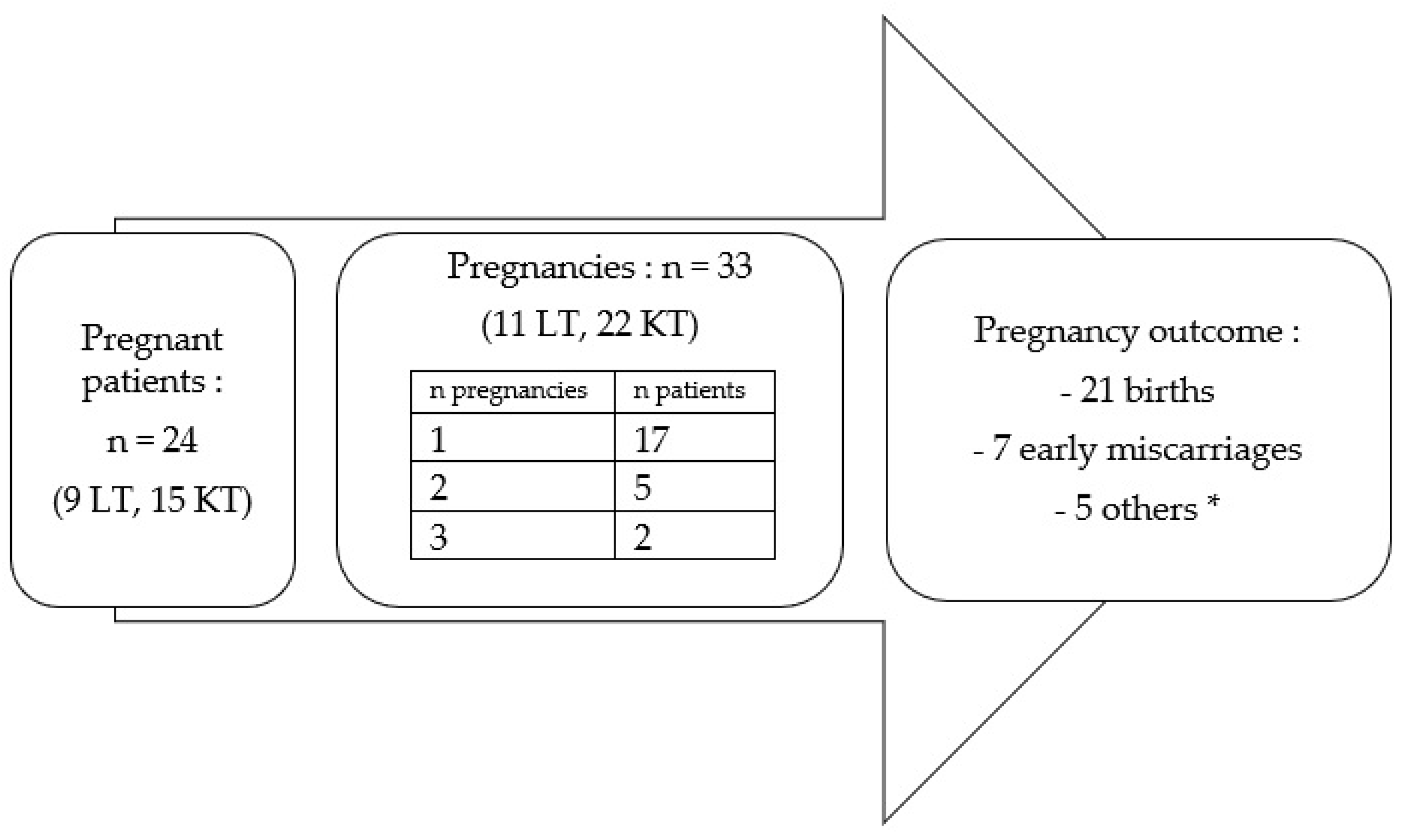
| Patients with ≥1 Pregnancy | 24 1 (11.4%) | 9 (7.9%) | 15 (15.6%) | 0.079 |
| Interval from SOT to authorization for 1st pregnancy (years) | n = 18 | n = 8 | n = 10 | |
| 3.7 ± 2.16 2 | 3.2 ± 0.76 | 4.2 ± 2.91 | 0.361 | |
| Mode of pregnancy | ||||
| Planned | 25 (75.8%) | 8 (72.7%) | 17 (77.3%) | 1.000 |
| Unplanned | 8 (24.2%) | 3 (27.3%) | 5 (22.7%) | |
| Mode of conception | <0.001 | |||
| Natural pregnancy: n (%) | 27 (81.8%) | 5 (45.5%) | 22 (100%) | |
| ART pregnancy: n (%) | 6 (18.2%) | 6 (54.5%) | 0 | |
| IS switch before | ||||
| pregnancy | 27 (81.8%) | 10 (90.9%) | 17 (77.3%) | 0.637 |
| Outcomes | ||||
| Early miscarriages | 7 (21.2%) | 2 (18.2%) | 5 (22.7%) | 1.000 |
| Medical termination | 1 (3.0%) | 1 (9.1%) | 0 | 0.333 |
| Other 3 | 4 (12.1%) | 1 (9.1%) | 3 (13.6%) | 0.706 |
| Births | 21 (63.7%) | 7 (63.6%) | 14 (63.7%) | 1.000 |
| Complications | n = 22 | n = 7 | n = 15 | |
| PE/HTA | 11 (50.0%) | 3 (42.9%) | 8 (53.3%) | 1.000 |
| Infection | 4 (18.1%) | 2 (28.6%) | 2 (13.3%) | 0.565 |
| Graft failure | 3 (13.6%) | 1 (14.3%) | 2 (13.3%) | 1.000 |
| Rejection | 0 | 0 | 0 | |
| Fetal malformation | 1 (4.5%) | 1 (14.3%) | 0 | 0.318 |
| Other 4 | 7 (31.8%) | 2 (28.6%) | 5 (33.3%) | 0.823 |
| WG at delivery | n = 21 | n = 7 | n = 14 | |
| All deliveries | 34.0 ± 3.5 | 34.6 ± 2.3 | 33.6 ± 4 | 0.551 |
| <32 WG | 5 (23.8%) | 1 (14.3%) | 4 (28.6%) | 0.624 |
| 32–37 WG | 14 (66.7%) | 5 (71.4%) | 9 (64.3%) | 1.000 |
| Full term | 2 (9.5%) | 1 (14.3%) | 1 (7.1%) | 1.000 |
| Weight at birth (g) | 2049 ± 681 (n = 18) | 1976 ± 121.2 (n = 5) | 2076.9 ± 806 (n = 13) | 0.788 |
| C-section delivery | 11 (52.4%; n = 21) | 3 (42.9%; n = 7) | 8 (57.1%; n = 14) | 0.659 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bedin, A.; Carbonnel, M.; Snanoudj, R.; Roux, A.; Vanlieferinghen, S.; Marchiori, C.; Hertig, A.; Racowsky, C.; Ayoubi, J.-M. Pregnancies and Gynecological Follow-Up after Solid Organ Transplantation: Experience of a Decade. J. Clin. Med. 2022, 11, 4792. https://doi.org/10.3390/jcm11164792
Bedin A, Carbonnel M, Snanoudj R, Roux A, Vanlieferinghen S, Marchiori C, Hertig A, Racowsky C, Ayoubi J-M. Pregnancies and Gynecological Follow-Up after Solid Organ Transplantation: Experience of a Decade. Journal of Clinical Medicine. 2022; 11(16):4792. https://doi.org/10.3390/jcm11164792
Chicago/Turabian StyleBedin, Alice, Marie Carbonnel, Renaud Snanoudj, Antoine Roux, Sarah Vanlieferinghen, Claire Marchiori, Alexandre Hertig, Catherine Racowsky, and Jean-Marc Ayoubi. 2022. "Pregnancies and Gynecological Follow-Up after Solid Organ Transplantation: Experience of a Decade" Journal of Clinical Medicine 11, no. 16: 4792. https://doi.org/10.3390/jcm11164792
APA StyleBedin, A., Carbonnel, M., Snanoudj, R., Roux, A., Vanlieferinghen, S., Marchiori, C., Hertig, A., Racowsky, C., & Ayoubi, J.-M. (2022). Pregnancies and Gynecological Follow-Up after Solid Organ Transplantation: Experience of a Decade. Journal of Clinical Medicine, 11(16), 4792. https://doi.org/10.3390/jcm11164792