
Safety and Efficacy of Minimum- or Zero-Contrast IVUS–Guided Percutaneous Coronary Interventions in Chronic Kidney Disease Patients: A Systematic Review

 ,
,  ,
,  ,
,
Abstract
1. Introduction
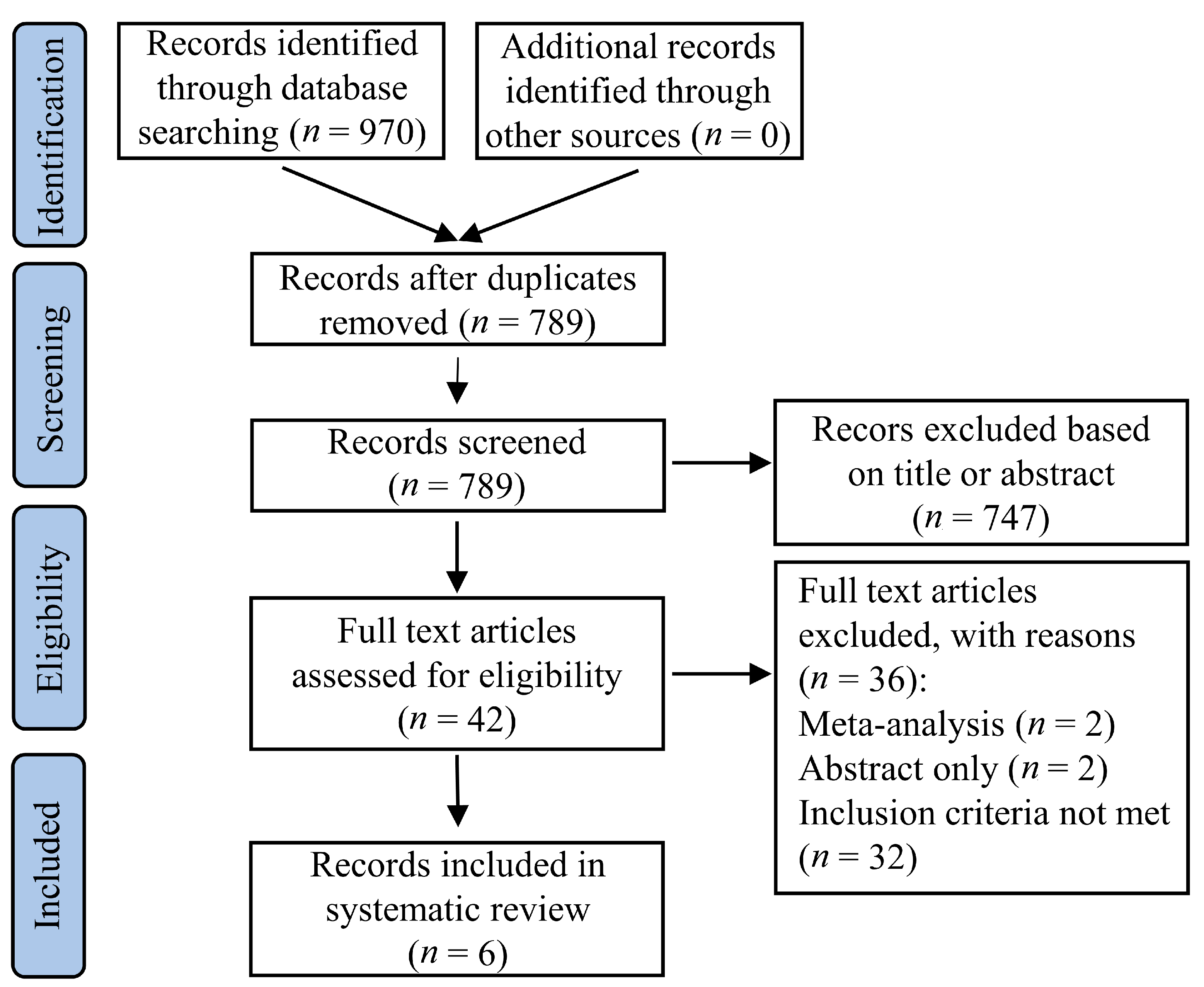
2. Materials and Methods
2.1. Data Sources
2.2. Study Selection
2.3. Data Extraction
2.4. Outcomes
2.5. Quality Assessment
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2020, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2019, 41, 407–477. [Google Scholar] [CrossRef]
- Wickenbrock, I.; Perings, C.; Maagh, P.; Quack, I.; van Bracht, M.; Prull, M.W.; Plehn, G.; Trappe, H.J.; Meissner, A. Contrast medium induced nephropathy in patients undergoing percutaneous coronary intervention for acute coronary syndrome: Differences in STEMI and NSTEMI. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2009, 98, 765–772. [Google Scholar] [CrossRef][Green Version]
- Parfrey, P. The clinical epidemiology of contrast-induced nephropathy. Cardiovasc. Interv. Radiol. 2005, 28 (Suppl. 2), S3–S11. [Google Scholar] [CrossRef]
- Rihal, C.S.; Textor, S.C.; Grill, D.E.; Berger, P.B.; Ting, H.H.; Best, P.J.; Singh, M.; Bell, M.R.; Barsness, G.W.; Mathew, V.; et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation 2002, 105, 2259–2264. [Google Scholar] [CrossRef] [PubMed]
- Gaipov, A.; Molnar, M.Z.; Potukuchi, P.K.; Sumida, K.; Szabo, Z.; Akbilgic, O.; Streja, E.; Rhee, C.M.; Koshy, S.K.G.; Canada, R.B.; et al. Acute kidney injury following coronary revascularization procedures in patients with advanced CKD. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2019, 34, 1894–1901. [Google Scholar] [CrossRef]
- El-Ahmadi, A.; Abassi, M.S.; Andersson, H.B.; Engstrøm, T.; Clemmensen, P.; Helqvist, S.; Jørgensen, E.; Kelbæk, H.; Pedersen, F.; Saunamäki, K.; et al. Acute kidney injury—A frequent and serious complication after primary percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction. PLoS ONE 2019, 14, e0226625. [Google Scholar] [CrossRef] [PubMed]
- Mavromatis, K. The imperative of reducing contrast dose in percutaneous coronary intervention. JACC Cardiovasc. Interv. 2014, 7, 1294–1296. [Google Scholar] [CrossRef]
- Kern, M.J. How Low Can We Go? Use of Ultra-Low Contrast Volume in Patients Undergoing PCI. Available online: https://www.cathlabdigest.com/content/how-low-can-we-go-use-ultra-low-contrast-volume-patients-undergoing-pci (accessed on 11 February 2021).
- Sacha, J.; Gierlotka, M.; Lipski, P.; Feusette, P.; Dudek, D. Zero-contrast percutaneous coronary interventions to preserve kidney function in patients with severe renal impairment and hemodialysis subjects. Postepy Kardiol. Interwencyjnej Adv. Interv. Cardiol. 2019, 15, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Chen, L.; Wu, L.; Huang, J.; Li, H.; Wang, X.; Weng, H. Diagnostic and prognostic predictive values of circulating KL-6 for interstitial lung disease: A PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore) 2020, 99, e19493. [Google Scholar] [CrossRef]
- Ali, Z.A.; Karimi Galougahi, K.; Nazif, T.; Maehara, A.; Hardy, M.A.; Cohen, D.J.; Ratner, L.E.; Collins, M.B.; Moses, J.W.; Kirtane, A.J.; et al. Imaging- and physiology-guided percutaneous coronary intervention without contrast administration in advanced renal failure: A feasibility, safety, and outcome study. Eur. Heart J. 2016, 37, 3090–3095. [Google Scholar] [CrossRef] [PubMed]
- Rahim, H.; Sethi, S.; Karampaliotis, D.; Ali, Z. Imaging and Physiology-Guided PCI without Contrast Administration in Advanced Renal Failure. Available online: https://www.pcronline.com/Cases-resources-images/Cases/Read-share-cases/2019/Imaging-and-physiology-guided-PCI-without-contrast-administration-in-advanced-renal-failure?auth=true (accessed on 11 February 2021).
- Malik, A.H.; Yandrapalli, S.; Aronow, W.S.; Panza, J.A.; Cooper, H.A. Intravascular ultrasound-guided stent implantation reduces cardiovascular mortality—Updated meta-analysis of randomized controlled trials. Int. J. Cardiol. 2020, 299, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Darmoch, F.; Alraies, M.C.; Al-Khadra, Y.; Moussa Pacha, H.; Pinto, D.S.; Osborn, E.A. Intravascular Ultrasound Imaging-Guided Versus Coronary Angiography-Guided Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2020, 9, e013678. [Google Scholar] [CrossRef]
- Sakai, K.; Ikari, Y.; Nanasato, M.; Umetsu, H.; Okutsu, M.; Takikawa, T.; Sumitsuji, S.; Sadamatsu, K.; Takada, M.; Kato, Y.; et al. Impact of intravascular ultrasound-guided minimum-contrast coronary intervention on 1-year clinical outcomes in patients with stage 4 or 5 advanced chronic kidney disease. Cardiovasc. Interv. Ther. 2019, 34, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Jino, B.; Manu, R.; Roy, S.; Villoth, S.G. IVUS guided rota assisted left main zero-contrast PCI in a patient with CKD. IHJ Cardiovasc. Case Rep. (CVCR) 2020, 4, 49–52. [Google Scholar] [CrossRef]
- Patel, N.J.; Jost, C.; Barry, M.D.; Lipskind, S.; Heuser, R.R. Zero Contrast PCI Using SyncVision Precision Guidance. Available online: https://www.cathlabdigest.com/content/zero-contrast-pci-using-syncvision-precision-guidance (accessed on 15 February 2021).
- Escaned, J.; Collet, C.; Ryan, N.; De Maria, G.L.; Walsh, S.; Sabate, M.; Davies, J.; Lesiak, M.; Moreno, R.; Cruz-Gonzalez, I.; et al. Clinical outcomes of state-of-the-art percutaneous coronary revascularization in patients with de novo three vessel disease: 1-year results of the SYNTAX II study. Eur. Heart J. 2017, 38, 3124–3134. [Google Scholar] [CrossRef] [PubMed]
- Serruys, P.W.; Morice, M.C.; Kappetein, A.P.; Colombo, A.; Holmes, D.R.; Mack, M.J.; Ståhle, E.; Feldman, T.E.; van den Brand, M.; Bass, E.J.; et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N. Engl. J. Med. 2009, 360, 961–972. [Google Scholar] [CrossRef]
- Bangalore, S.; Maron, D.J.; O’Brien, S.M.; Fleg, J.L.; Kretov, E.I.; Briguori, C.; Kaul, U.; Reynolds, H.R.; Mazurek, T.; Sidhu, M.S.; et al. Management of Coronary Disease in Patients with Advanced Kidney Disease. N. Engl. J. Med. 2020, 382, 1608–1618. [Google Scholar] [CrossRef]
- Zhang, J.; Gao, X.; Ge, Z.; Han, L.; Lu, S.; Qian, X.; Li, Q.; Lu, Q.; Chen, C.; Chen, S.L. Impact of intravascular ultrasound-guided drug-eluting stent implantation on patients with chronic kidney disease: Results from ULTIMATE trial. Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2019, 93, 1184–1193. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Gao, X.; Kan, J.; Ge, Z.; Han, L.; Lu, S.; Tian, N.; Lin, S.; Lu, Q.; Wu, X.; et al. Intravascular Ultrasound Versus Angiography-Guided Drug-Eluting Stent Implantation: The ULTIMATE Trial. J. Am. Coll. Cardiol. 2018, 72, 3126–3137. [Google Scholar] [CrossRef] [PubMed]
- Fan, P.C.; Chen, T.H.; Lee, C.C.; Tsai, T.Y.; Chen, Y.C.; Chang, C.H. ADVANCIS Score Predicts Acute Kidney Injury After Percutaneous Coronary Intervention for Acute Coronary Syndrome. Int. J. Med. Sci. 2018, 15, 528–535. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Criteria | |
|---|---|
| Population | Patients (aged > 18 years) with chronic kidney disease and acute or chronic coronary syndromes. |
| Intervention | Minimum-contrast or zero-contrast intravascular ultrasound guided percutaneous coronary interventions. |
| Comparators | Angiography guided percutaneous coronary interventions. |
| None. | |
| Outcomes | Efficacy and/or safety |
| Type of Study | Randomized or non-randomized studies, observational studies, case series, and case reports. |
| Language | English. |
| Study, Year | Design | Patients, No | Age (Years), Median/Mean | Setting | Intervention | Comparator | Outcomes | Follow-Up |
|---|---|---|---|---|---|---|---|---|
| Ali et al., 2016 [12] | Retrospective analysis (case series), single center | 31 | 66 ± 11 | Patients with advanced CKD (stages 4–5) and stable CAD | Zero-contrast IVUS guided PCI | N/A | -Requirement of RRT -Stent thrombosis -Revascularization -Myocardial infarction -Death | 79 days (median) |
| Sakai et al., 2018 [16] | Non-randomized, multicenter | 184 | 74 ± 7 (angiography-guided PCI) 76 ± 9 (IVUS-guided PCI) | Patients with CAD, elective PCI, and CKD stages 4–5 (excluding hemodialysis) | IVUS-guided minimum-contrast PCI (98 patients) | Angiography-guided PCI (86 patients) | -All-cause mortality -Cardiac death -Non-cardiac death -Requirement of RRT | 12 months |
| Sacha et al., 2019 [10] | Retrospective analysis, single center | 20 | 73.7 ± 12.8 | Patients with CKD (eGFR < 45 mL/min/1.73 m2) including hemodialysis (preserved urine output) admitted due to acute coronary syndrome or in elective setting | Zero-contrast IVUS guided PCI | N/A | During hospitalization: -Change in creatinine/eGFR -Acute kidney injury -Requirement of RRT (in patients without dialysis) -Periprocedural myocardial infarction -Distal embolization During follow-up: Acute coronary syndrome Stent thrombosis Repeat revascularization StrokeRequirement of RRT (in patients without dialysis) Death | 3.2 months (median) |
| Kumar et al., 2020 [19] | Case report | 1 | 54 | CKD patient with recent history of few cycles of hemodialysis for acute on chronic kidney disease | IVUS-guided rota-assisted left main zero-contrast PCI | N/A | During hospitalization: -Post stenting pericardial effusion -Post intervention symptoms -Hemodynamic instability -Change in creatinine | - |
| Patel et al., 2020 [20] | Case report | 1 | 70 | CKD stage 4 and history of hypertension, type 2 diabetes mellitus | IVUS-guided PCI of RCA with zero-contrast, and PCI of distal LM to LAD using minimum-contrast | N/A | During hospitalization: -Changes in renal function -Post intervention symptoms During follow-up: -Changes in renal function -Post intervention symptoms | 1 week |
| Rahim et al., 2019 [13] | Case report | 1 | 57 | CKD stage 4 and a history of HIV, diabetes mellitus | Zero-contrast PCI of LM (bifurcation),LAD with LV support | N/A | During hospitalization: -Procedural harm -Procedural success | 6 months |
| Author, year | Outcomes | Results | |
|---|---|---|---|
| Sakai et al., 2018 [16] | IVUS-guided PCI versus angiography-guided PCI | ||
| All-cause death | 6 (6.4%) vs. 6 (7.8%) patients | p = 0.85 | |
| Cardiac death | 2 (2.2%) vs. 2 (2.6%) patients | p = 0.98 | |
| Non-cardiac death | 4 (4.4%) vs. 4 (5.3%) patients | p = 0.79 | |
| Requirement of RRT | 3 (3.2%) vs. 11 (13.6%) patients | p = 0.01 | |
| Ali et al., 2016 [12] | Stent thrombosis | 0 (0%) patients | |
| Revascularization | 0 (0%) patients | ||
| Myocardial infarction | 0 (0%) patients | ||
| Death | 0 (0%) patients | ||
| Requirement of RRT | 0 (0%) patients | ||
| Sacha et al., 2019 [10] | During hospitalization | ||
| Change in creatinine (mg/dL) | 0.1 ± 0.31 | p = 0.2 | |
| Change in eGFR (mL/min/1.73 m2) | −0.7 ± 10.9 | p = 0.8 | |
| AKI after zero-contrast PCI | 2 (10%) patients | ||
| Requirement of RRT | 0 (0%) patients | ||
| Periprocedural myocardial infarction | 1 (5%) patient | ||
| Distal embolization | 1 (5%) patient | ||
| During follow-up | |||
| Acute coronary syndrome | 0 (0%) patients | ||
| Stent thrombosis | 0 (0%) patients | ||
| Repeat revascularization | 0 (0%) patients | ||
| Stroke | 0 (0%) patients | ||
| Requirement of RRT | 0 (0%) patients | ||
| Death | 1 (5%) patient | ||
| Kumar et al., 2020 [19] | During hospitalization | ||
| Post stenting pericardial effusion | 0 | ||
| Post intervention symptoms | 0 | ||
| Hemodynamic instability | 0 | ||
| Change in creatinine | 0.2 mg/dL | ||
| Patel et al., 2020 [20] | During hospitalization | ||
| Changes in renal function | 0 | ||
| Post intervention symptoms | 0 | ||
| During follow-up | |||
| Changes in renal function | 0 | ||
| Post intervention symptoms | 0 | ||
| Rahim et al., 2019 [13] | During hospitalization | ||
| Procedural harm | 0 | ||
| Procedural success | 0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burlacu, A.; Tinica, G.; Brinza, C.; Crisan-Dabija, R.; Popa, I.V.; Covic, A. Safety and Efficacy of Minimum- or Zero-Contrast IVUS–Guided Percutaneous Coronary Interventions in Chronic Kidney Disease Patients: A Systematic Review. J. Clin. Med. 2021, 10, 1996. https://doi.org/10.3390/jcm10091996
Burlacu A, Tinica G, Brinza C, Crisan-Dabija R, Popa IV, Covic A. Safety and Efficacy of Minimum- or Zero-Contrast IVUS–Guided Percutaneous Coronary Interventions in Chronic Kidney Disease Patients: A Systematic Review. Journal of Clinical Medicine. 2021; 10(9):1996. https://doi.org/10.3390/jcm10091996
Chicago/Turabian StyleBurlacu, Alexandru, Grigore Tinica, Crischentian Brinza, Radu Crisan-Dabija, Iolanda Valentina Popa, and Adrian Covic. 2021. "Safety and Efficacy of Minimum- or Zero-Contrast IVUS–Guided Percutaneous Coronary Interventions in Chronic Kidney Disease Patients: A Systematic Review" Journal of Clinical Medicine 10, no. 9: 1996. https://doi.org/10.3390/jcm10091996
APA StyleBurlacu, A., Tinica, G., Brinza, C., Crisan-Dabija, R., Popa, I. V., & Covic, A. (2021). Safety and Efficacy of Minimum- or Zero-Contrast IVUS–Guided Percutaneous Coronary Interventions in Chronic Kidney Disease Patients: A Systematic Review. Journal of Clinical Medicine, 10(9), 1996. https://doi.org/10.3390/jcm10091996