External Validation of Surrogate Indices of Fatty Liver in the General Population: The Bagnacavallo Study


 ,
,  , , and
, , and
Abstract
1. Introduction
2. Subjects and Methods
2.1. Source of Data
2.2. Participants
2.3. Outcomes
2.4. Predictors
2.5. Sample Size
2.6. Missing Data
2.7. Statistical Analysis
3. Results
3.1. Study Population
3.2. Diagnosis of FL
3.3. Diagnosis of NAFLD
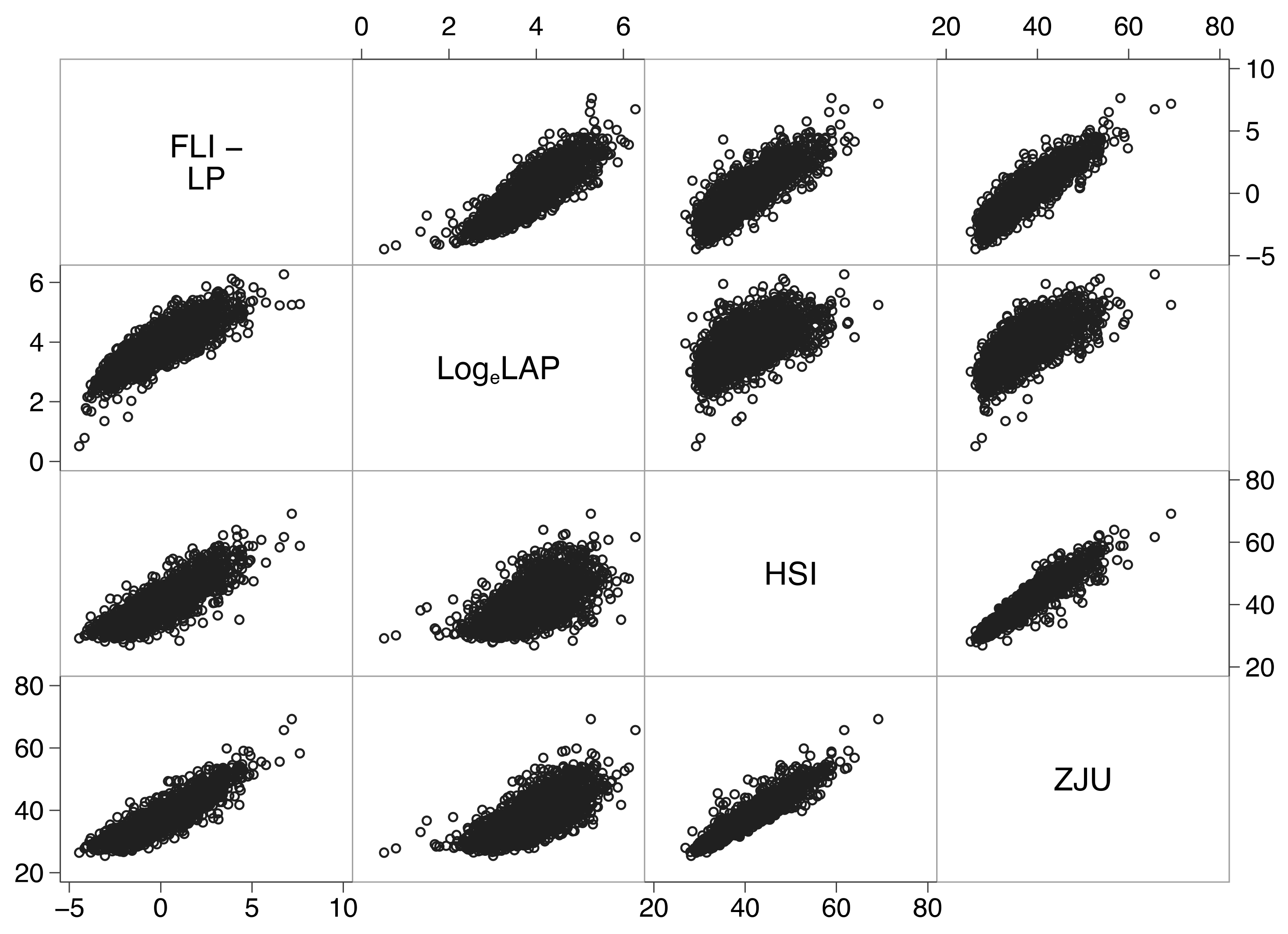
3.4. Association between Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Section/Topic | Item | Checklist Item | Page |
|---|---|---|---|
| Title and abstract | |||
| Title | 1 | Identify the study as developing and/or validating a multivariable prediction model, the target population, and the outcome to be predicted. | 1 |
| Abstract | 2 | Provide a summary of objectives, study design, setting, participants, sample size, predictors, outcome, statistical analysis, results, and conclusions. | 1 |
| Introduction | |||
| Background and objectives | 3a | Explain the medical context (including whether diagnostic or prognostic) and rationale for developing or validating the multivariable prediction model, including references to existing models. | 2 |
| 3b | Specify the objectives, including whether the study describes the development or validation of the model or both. | 2 | |
| Methods | |||
| Source of data | 4a | Describe the study design or source of data (e.g., randomized trial, cohort, or registry data), separately for the development and validation data sets, if applicable. | 2 |
| 4b | Specify the key study dates, including start of accrual; end of accrual; and, if applicable, end of follow-up. | 2 | |
| Participants | 5a | Specify key elements of the study setting (e.g., primary care, secondary care, general population) including number and location of centres. | 2 |
| 5b | Describe eligibility criteria for participants. | 2 | |
| 5c | Give details of treatments received, if relevant. Comment: no treatment was administered outside good clinical practice. | NAP | |
| Outcome | 6a | Clearly define the outcome that is predicted by the prediction model, including how and when assessed. | 3 |
| 6b | Report any actions to blind assessment of the outcome to be predicted. Comment: biomarkers were calculated after the end of the study. | NAP | |
| Predictors | 7a | Clearly define all predictors used in developing or validating the multivariable prediction model, including how and when they were measured. | 13 |
| 7b | Report any actions to blind assessment of predictors for the outcome and other predictors. Comment: biomarkers were calculated after the end of the study. | NAP | |
| Sample size | 8 | Explain how the study size was arrived at. | 3 |
| Missing data | 9 | Describe how missing data were handled (e.g., complete-case analysis, single imputation, multiple imputation) with details of any imputation method. | 3 |
| Statistical analysis methods | 10c | For validation, describe how the predictions were calculated. | 13 |
| 10d | Specify all measures used to assess model performance and, if relevant, to compare multiple models. | 4 | |
| 10e | Describe any model updating (e.g., recalibration) arising from the validation, if done. Comment: there was no need to recalibrate any biomarker. | NAP | |
| Risk groups | 11 | Provide details on how risk groups were created, if done. | 4 |
| Development vs. validation | 12 | For validation, identify any differences from the development data in setting, eligibility criteria, outcome, and predictors. | 3, 12 |
| Results | |||
| Participants | 13a | Describe the flow of participants through the study, including the number of participants with and without the outcome and, if applicable, a summary of the follow-up time. A diagram may be helpful. | 2 |
| 13b | Describe the characteristics of the participants (basic demographics, clinical features, available predictors), including the number of participants with missing data for predictors and outcome. | 2 | |
| 13c | For validation, show a comparison with the development data of the distribution of important variables (demographics, predictors and outcome). | 2 | |
| Model performance | 16 | Report performance measures (with CIs) for the prediction model. | 5 |
| Model-updating | 17 | If done, report the results from any model updating (i.e., model specification, model performance). No attempt was made to update any biomarker. | NAP |
| Discussion | |||
| Limitations | 18 | Discuss any limitations of the study (such as nonrepresentative sample, few events per predictor, missing data). | 9 |
| Interpretation | 19a | For validation, discuss the results with reference to performance in the development data, and any other validation data. | 9 |
| 19b | Give an overall interpretation of the results, considering objectives, limitations, results from similar studies, and other relevant evidence. | 9 | |
| Implications | 20 | Discuss the potential clinical use of the model and implications for future research. | 9 |
| Other information | |||
| Supplementary information | 21 | Provide information about the availability of supplementary resources, such as study protocol, Web calculator, and data sets. Comment: The data presented in this study are available on reasonable request from the corresponding author. | NAP |
| Funding | 22 | Give the source of funding and the role of the funders for the present study. | 9 |
Appendix B
| Biomarkers | ||||
|---|---|---|---|---|
| FLI | LAP | HSI | ZJU | |
| Triglycerides | ✓ | ✓ | ✓ | |
| BMI | ✓ | ✓ | ✓ | |
| GGT | ✓ | |||
| Waist | ✓ | ✓ | ||
| ALT:AST | ✓ | ✓ | ||
| T2DM | ✓ | |||
| Sex | ✓ | |||
| Glucose | ✓ | |||
| Abbreviations and Units of Measurements | |
|---|---|
| altsalt | alanine transaminase (U/L)/aspartate transaminase (U/L) |
| bmi | body mass index (kg/m2) |
| exp | exponential operator |
| female | female gender (1 = female; 0 = male) |
| ggt | gamma-glutamyltransferase (U/L) |
| gmmol | glucose (mmol/L) |
| loge | natural logarithm |
| fli_lp | fatty liver index-linear predictor |
| t2dm | type 2 diabetes mellitus (1 = yes; 0 = no) |
| tg | triglycerides (mg/dL) |
| tgmmol | triglycerides (mmol/L) |
| wc | waist circumference (cm) |
| Fatty liver index (FLI) | |
| fli_lp | 0.953*loge(tg) + 0.139*bmi + 0.718* loge(ggt) + 0.053*wc−15.745 |
| FLI | [(exp(fli_lp)/(1 + exp(fli_lp)]*100 |
| Lipid accumulation product (LAP) | |
| LAP | (wc−k)*tgmmol with k=65 if sex=male or k=58 if sex=female |
| Hepatic steatosis index (HIS) | |
| HSI | 8*altast + bmi + 2*t2dm + 2*female |
| Zhejiang University index (ZJU) | |
| ZJU | bmi + gmmol + tgmmol + 3*altast +2*female |
References
- Fouad, Y.; Waked, I.; Bollipo, S.; Gomaa, A.; Ajlouni, Y.; Attia, D. What’s in a name? Renaming ‘NAFLD’ to ‘MAFLD’. Liver Int. 2020, 40, 1254–1261. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Anstee, Q.M.; Targher, G.; Gomez, M.R.; Zelber-Sagi, S.; Wong, V.W.-S.; Dufour, J.-F.; Schattenberg, J.; Arrese, M. A new definition for metabolic associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Sanyal, A.J.; George, J.; Sanyal, A.; Neuschwander-Tetri, B.; Tiribelli, C.; Kleiner, D.E.; Brunt, E.; Bugianesi, E.; Yki-Järvinen, H.; et al. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Rinella, M.; Beuers, U.; Loomba, R.; Anstee, Q.M.; Harrison, S.; Francque, S.; Sanyal, A.; Newsome, P.N.; Younossi, Z. The times they are a-changin’ (for NAFLD as well). J. Hepatol. 2020, 73, 1307–1309. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W. Clinical Prediction Models; Springer International: Cham, Switzerland, 2019. [Google Scholar]
- Van Calster, B.; Nieboer, D.; Vergouwe, Y.; De Cock, B.; Pencina, M.J.; Steyerberg, E.W. A calibration hierarchy for risk models was defined: From utopia to empirical data. J. Clin. Epidemiol. 2016, 74, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.N.; Yu, M.X.; Gao, Q.; Li, Y.Y.; Huang, J.J.; Sun, C.M.; Qiao, N.; Zhang, H.X.; Wang, H.; Lu, Q.; et al. External validation of non-invasive prediction models for identifying ultrasonography-diagnosed fatty liver disease in a Chinese population. Medicine 2017, 96, e7610. [Google Scholar] [CrossRef] [PubMed]
- Meffert, P.J.; Baumeister, S.E.; Lerch, M.M.; Mayerle, J.; Kratzer, W.; Volzke, H. Development, external validation, and comparative assessment of a new diagnostic score for hepatic steatosis. Am. J. Gastroenterol. 2014, 109, 1404–1414. [Google Scholar] [CrossRef]
- Wan, F.; Pan, F.; Ayonrinde, O.T.; Adams, L.A.; Mori, T.A.; Beilin, L.J.; O’Sullivan, T.A.; Olynyk, J.K.; Oddy, W.H. Validation of fatty liver disease scoring systems for ultrasound diagnosed non-alcoholic fatty liver disease in adolescents. Dig. Liver Dis. 2020. [Google Scholar] [CrossRef]
- Foschi, F.G.; Domenicali, M.; Giacomoni, P.; Dall’Aglio, A.C.; Conti, F.; Borghi, A.; Bevilacqua, V.; Napoli, L.; Mirici, F.; Cucchetti, A.; et al. Is there an association between commonly employed biomarkers of liver fibrosis and liver stiffness in the general population. Ann. Hepatol. 2020, 19, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Foschi, F.G.; Bedogni, G.; Domenicali, M.; Giacomoni, P.; Dall’Aglio, A.C.; Dazzani, F.; Lanzi, A.; Conti, F.; Savini, S.; Saini, G.; et al. Prevalence of and risk factors for fatty liver in the general population of Northern Italy: The Bagnacavallo Study. BMC Gastroenterol. 2018, 18, 177. [Google Scholar] [CrossRef] [PubMed]
- Rimini, M.; Casadei-Gardini, A.; Ravaioli, A.; Rovesti, G.; Conti, F.; Borghi, A.; Dall’Aglio, A.C.; Bedogni, G.; Domenicali, M.; Giacomoni, P.; et al. Could Inflammatory Indices and Metabolic Syndrome Predict the Risk of Cancer Development? Analysis from the Bagnacavallo Population Study. J. Clin. Med. 2020, 9, 1177. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, G.; Miglioli, L.; Masutti, F.; Tiribelli, C.; Marchesini, G.; Bellentani, S. Prevalence of and risk factors for nonalcoholic fatty liver disease: The Dionysos nutrition and liver study. Hepatology 2005, 42, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1991. [Google Scholar]
- Bedogni, G.; Kahn, H.S.; Bellentani, S.; Tiribelli, C. A simple index of lipid overaccumulation is a good marker of liver steatosis. BMC Gastroenterol. 2010, 10, 98. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. The Evidence Report. National Institutes of Health. Obes. Res. 1998, 6 (Suppl. 2), 51S–209S. [Google Scholar]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the Metabolic Syndrome A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention National Heart, Lung, and Blood Institute American. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Wang, J.; Xu, C.; Xun, Y.; Lu, Z.; Shi, J.; Yu, C.; Li, Y. ZJU index: A novel model for predicting nonalcoholic fatty liver disease in a Chinese population. Sci. Rep. 2015, 5, 16494. [Google Scholar] [CrossRef]
- Otgonsuren, M.; Estep, M.J.; Hossain, N.; Younossi, E.; Frost, S.; Henry, L.; Hunt, S.; Fang, Y.; Goodman, Z.; Younossi, Z.M. A single non-invasive model to diagnose non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH). J. Gastroenterol. Hepatol. 2014, 29, 2006–2013. [Google Scholar] [CrossRef] [PubMed]
- Poynard, T.; Ratziu, V.; Naveau, S.; Thabut, D.; Charlotte, F.; Messous, D.; Capron, D.; Abella, A.; Massard, J.; Ngo, Y.; et al. The diagnostic value of biomarkers (SteatoTest) for the prediction of liver steatosis. Comp Hepatol. 2005, 4, 10. [Google Scholar] [CrossRef] [PubMed]
- Kotronen, A.; Peltonen, M.; Hakkarainen, A.; Sevastianova, K.; Bergholm, R.; Johansson, L.M.; Lundbom, N.; Rissanen, A.; Ridderstråle, M.; Groop, L.; et al. Prediction of non-alcoholic fatty liver disease and liver fat using metabolic and genetic factors. Gastroenterology 2009, 137, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Stevens, R.J.; Poppe, K.K. Validation of clinical prediction models: What does the “calibration slope” really measure. J. Clin. Epidemiol 2019. [Google Scholar] [CrossRef]
- Harrell, F. Regression Modeling Strategies; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Ensor, J.; Snell, K.I.; Martin, E.C. PMCALPLOT: Stata Module to Produce Calibration Plot of Prediction Model Performance. Statistical Software Components. 2018. Available online: https://ideas.repec.org/c/boc/bocode/s458486.html (accessed on 28 January 2021).
- Haghish, E.F. Seamless interactive language interfacing between R and Stata. Stata J. 2019, 19, 61–82. [Google Scholar] [CrossRef]
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: A meta-analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef]
- Xu, Z.; Li, H.; Tian, S.; Wu, J.; Li, X.; Liu, Z.L.; Li, S.; Chen, Y.L.; Xiao, J.; Wei, J.Y.; et al. Blood biomarkers for the diagnosis of hepatic steatosis in metabolic dysfunction-associated fatty liver disease. J. Hepatol. 2020, 73, 1264–1265. [Google Scholar] [CrossRef]



| n = 2159 | |
|---|---|
| Altered liver enzymes | 349 (16.2%) |
| Male sex | 1079 (50.0%) |
| Age (years) | 49 (41; 56) |
| Body mass index (kg/m2) | 25.5 (23.0; 29.0) |
| Normal liver | 1263 (58.5%) |
| Fatty liver | 896 (41.5%) |
| Non-alcoholic fatty liver disease | 567 (26.3%) |
| Alcoholic fatty liver disease | 329 (15.2%) |
| Waist circumference (cm) | 101.0 (94.0; 108.0) |
| Glucose (mg/dL) | 89 (83; 97) |
| Triglycerides (mg/dL) | 102 (71; 153) |
| Total cholesterol (mg/dL) | 209 (185; 235) |
| HDL-cholesterol (mg/dL) | 59 (49; 71) |
| LDL-cholesterol (mg/dL) | 128 (105; 152) |
| Systolic blood pressure (mm Hg) | 130 (120; 140) |
| Diastolic blood pressure (mm Hg) | 80 (80; 90) |
| Metabolic syndrome | 615 (28.5%) |
| Alanine transaminase (U/L) | 22 (16; 32) |
| Aspartate transaminase (U/L) | 22 (18; 26) |
| Gamma-glutamyltransferase (U/L) | 19 (13; 32) |
| Alcohol intake (units/day) | 2 (0; 4) |
| Fatty liver index (FLI) | 46 (21; 76) |
| Lipid accumulation product (LAP) | 44 (28; 75) |
| Hepatic steatosis index (HSI) | 39 (35; 44) |
| Zhejiang University index (ZJU) | 36 (33; 41) |
| Fatty Liver | ||||
| FLI | LAP | HSI | ZJU | |
| Expected event rate † | 0.42 (0.40 to 0.43) | 0.42 (0.40 to 0.43) | 0.42 (0.40 to 0.43) | 0.42 (0.40 to 0.43) |
| Calibration intercept | 0.00 (−0.11 to 0.11) | 0.00 (−0.10 to 0.10) | 0.00 (−0.10 to 0.10) | 0.00 (−0.10 to 0.10) |
| Calibration slope | 1.00 (0.92 to 1.08) | 1.00 (0.89 to 1.11) | 1.00 (0.91 to 1.09) | 1.00 (0.91 to 1.09) |
| C-statistic | 0.85 (0.84 to 0.87) | 0.80 (0.78 to 0.82) | 0.82 (0.80 to 0.83) | 0.83 (0.81 to 0.85) |
| Non-Alcoholic Fatty Liver Disease | ||||
| FLI | LAP | HSI | ZJU | |
| Expected event rate †† | 0.26 (0.25 to 0.28) | 0.26 (0.24 to 0.28) | 0.26 (0.25 to 0.28) | 0.26 (0.25 to 0.28) |
| Calibration intercept | 0.00 (−0.11 to 0.11) | 0.00 (−0.10 to 0.10) | 0.00 (−0.10 to 0.10) | 0.00 (−0.10 to 0.10) |
| Calibration slope | 1.00 (0.89 to 1.11) | 1.00 (0.84 to 1.16) | 1.00 (0.88 to 1.12) | 1.00 (0.88 to 1.12) |
| C-statistic | 0.77 (0.75 to 0.79) | 0.74 (0.71 to 0.76) | 0.75 (0.72 to 0.77) | 0.76 (0.74 to 0.78) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foschi, F.G.; Conti, F.; Domenicali, M.; Giacomoni, P.; Borghi, A.; Bevilacqua, V.; Napoli, L.; Berardinelli, D.; Altini, M.; Cucchetti, A.; et al. External Validation of Surrogate Indices of Fatty Liver in the General Population: The Bagnacavallo Study. J. Clin. Med. 2021, 10, 520. https://doi.org/10.3390/jcm10030520
Foschi FG, Conti F, Domenicali M, Giacomoni P, Borghi A, Bevilacqua V, Napoli L, Berardinelli D, Altini M, Cucchetti A, et al. External Validation of Surrogate Indices of Fatty Liver in the General Population: The Bagnacavallo Study. Journal of Clinical Medicine. 2021; 10(3):520. https://doi.org/10.3390/jcm10030520
Chicago/Turabian StyleFoschi, Francesco Giuseppe, Fabio Conti, Marco Domenicali, Pierluigi Giacomoni, Alberto Borghi, Vittoria Bevilacqua, Lucia Napoli, Dante Berardinelli, Mattia Altini, Alessandro Cucchetti, and et al. 2021. "External Validation of Surrogate Indices of Fatty Liver in the General Population: The Bagnacavallo Study" Journal of Clinical Medicine 10, no. 3: 520. https://doi.org/10.3390/jcm10030520
APA StyleFoschi, F. G., Conti, F., Domenicali, M., Giacomoni, P., Borghi, A., Bevilacqua, V., Napoli, L., Berardinelli, D., Altini, M., Cucchetti, A., Ercolani, G., Casadei-Gardini, A., Bellentani, S., Gastaldelli, A., Tiribelli, C., Bedogni, G., & Bagnacavallo Study Group. (2021). External Validation of Surrogate Indices of Fatty Liver in the General Population: The Bagnacavallo Study. Journal of Clinical Medicine, 10(3), 520. https://doi.org/10.3390/jcm10030520