
Potential Application of Cardiac Computed Tomography for Early Detection of Coronary Atherosclerosis: From Calcium Score to Advanced Atherosclerosis Analysis



 ,
,  and
and
Abstract
1. Introduction
2. Noninvasive Coronary Atherosclerosis Assessment by CT
2.1. Cardiac CT: Technological Background
2.2. Coronary Artery Calcium Score (CACS): Noncontrast CT
2.3. Coronary Artery Evaluation by CCTA
2.4. Advanced Atherosclerosis Analysis by CCTA
3. Current Evidence on CCTA Use among Asymptomatic Patients
4. Future Perspectives for Potential Use of CCTA in Primary Prevention
5. Limitation to CCTA in Asymptomatic Patients
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation
| CCTA | Coronary computed tomography angiography |
| CACS | Coronary artery calcium score |
| MACE | Major adverse cardiovascular events |
| SIS | Segment-involvement score |
| SSS | Segment-stenosis score |
| CT-LeSC | CT-adapted Leaman score |
| IVUS | Intravascular ultrasound |
| CAD | Coronary artery disease |
References
- Timmis, A.; Townsend, N.; Gale, C.; Grobbee, R.; Maniadakis, N.; Flather, M.; Wilkins, E.; Wright, L.; Vos, R.; Bax, J.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2017. Eur. Heart J. 2018, 39, 508–577. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar]
- Paech, D.C.; Weston, A.R. A systematic review of the clinical effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of suspected coronary artery disease. BMC Cardiovasc. Disord. 2011, 16, 11–32. [Google Scholar] [CrossRef] [PubMed]
- Andreini, D.; Mushtaq, S.; Pontone, G.; Conte, E.; Guglielmo, M.; Annoni, A.; Baggiano, A.; Formenti, A.; Ditali, V.; Mancini, M.E.; et al. Diagnostic performance of coronary CT angiography carried out with a novel whole-heart coverage high-definition CT scanner in patients with high heart rate. Int. J. Cardiol. 2018, 257, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Min, J.K.; Dunning, A.; Lin, F.Y.; Achenbach, S.; Al-Mallah, M.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; Chang, H.J.; Cheng, V.; et al. CONFIRM Investigators. Age- and Sex-Related Differences in All-Cause Mortality Risk Based on Coronary Computed Tomography Angiography Findings. J. Am. Coll. Cardiol. 2011, 58, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.J.; Bindeman, J.; Feuerstein, I.; Cao, F.; Brazaitis, M.; O’Malley, P.G. Coronary calcium independently predicts incident premature coronary heart disease over measured cardiovascular risk factors: Mean three-year outcomes in the Prospective Army Coronary Calcium (PACC) project. J. Am. Coll. Cardiol. 2005, 46, 807–814. [Google Scholar] [CrossRef]
- Andreini, D.; Pontone, G.; Mushtaq, S.; Bartorelli, A.L.; Bertella, E.; Antonioli, L.; Formenti, A.; Cortinovis, S.; Veglia, F.; Annoni, A.; et al. A long-term prognostic value of coronary CT angiography in suspected coronary artery disease. JACC Cardiovasc. Imaging 2012, 5, 690–701. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Chest pain. In NICE Pathway; NICE: Manchester, UK, 2017; Available online: https://pathways.nice.org.uk/pathways/chest-pain (accessed on 5 January 2021).
- Task Force Members; Montalescot, G.; Sechtem, U.; Achenbach, S.; Andreotti, F.; Arden, C.; Budaj, A.; Bugiardini, R.; Crea, F.; Cuisset, T.; et al. Task Force Members. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Heart J. 2013, 34, 2949–3003. [Google Scholar]
- Andreini, D.; Martuscelli, E.; Guaricci, A.I.; Carrabba, N.; Magnoni, M.; Tedeschi, C.; Pelliccia, A.; Pontone, G. Clinical recommendations on Cardiac-CT in 2015: A position paper of the Working Group on Cardiac-CT and Nuclear Cardiology of the Italian Society of Cardiology. J. Cardiovasc. Med. 2016, 17, 73–84. [Google Scholar] [CrossRef]
- Taylor, A.J.; Cerqueira, M.; Hodgson, J.M.; Mark, D.; Min, J.; O’Gara, P.; Rubin, G.D. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 Appropriate Use Criteria for Cardiac Computed Tomography: A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J. Cardiovasc. Comput. Tomogr. 2010, 4, 1864–1894. [Google Scholar] [CrossRef]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef]
- Voros, S.; Rivera, J.J.; Berman, D.S.; Blankstein, R.; Budoff, M.J.; Cury, R.C.; Desai, M.Y.; Dey, D.; Halliburton, S.S.; Hecht, H.S.; et al. Guideline for minimizing radiation exposure during acquisition of coronary artery calcium scans with the use of multidetector computed tomography: A report by the Society for Atherosclerosis Imaging and Prevention Tomographic Imaging and Prevention Councils in collaboration with the Society of Cardiovascular Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2011, 5, 75–83. [Google Scholar] [PubMed]
- Kondos, G.T.; Hoff, J.A.; Sevrukov, A.; Daviglus, M.L.; Garside, D.B.; Devries, S.S.; Chomka, E.V.; Liu, K. Electron-beam tomography coronary artery calcium and cardiac events: A 37-month follow-up of 5635 initially asymptomatic low- to intermediate-risk adults. Circulation 2003, 107, 2571–2576. [Google Scholar] [CrossRef] [PubMed]
- Budoff, M.J.; Shaw, L.J.; Liu, S.T.; Weinstein, S.R.; Mosler, T.P.; Tseng, P.H.; Flores, F.R.; Callister, T.Q.; Raggi, P.; Berman, D.S. Long-term prognosis associated with coronary calcification: Observations from a registry of 25,253 patients. J. Am. Coll. Cardiol. 2007, 49, 1860–1870. [Google Scholar] [CrossRef] [PubMed]
- Alashi, A.; Lang, R.; Seballos, R.; Feinleib, S.; Sukol, R.; Cho, L.; Schoenhagen, P.; Griffin, B.P.; Flamm, S.D. Desai MYReclassification of coronary heart disease risk in a primary prevention setting: Traditional risk factor assessment vs. coronary artery calcium scoring. Cardiovasc. Diagn. Ther. 2019, 9, 214–220. [Google Scholar] [CrossRef]
- Cho, I.; Al’Aref, S.J.; Berger, A.; Ó Hartaigh, B.; Gransar, H.; Valenti, V.; Lin, F.Y.; Achenbach, S.; Berman, D.S.; Budoff, M.J. Prognostic value of coronary computed tomographic angiography findings in asymptomatic individuals: A 6-year follow-up from the prospective multicentre international CONFIRM study. Eur. Heart J. 2018, 39, 934–941. [Google Scholar] [CrossRef]
- Silverman, M.G.; Blaha, M.J.; Krumholz, H.M.; Budoff, M.J.; Blankstein, R.; Sibley, C.T.; Agatston, A.; Blumenthal, R.S.; Nasir, K. Impact of coronary artery calcium on coronary heart disease events in individuals at the extremes of traditional risk factor burden: The Multi-Ethnic Study of Atherosclerosis. Eur. Heart J. 2014, 35, 2232–2241. [Google Scholar] [CrossRef]
- Hecht, H.S.; Cronin, P.; Blaha, M.J.; Budoff, M.J.; Kazerooni, E.A.; Narula, J.; Yankelevitz, D.; Abbara, S. 2016 SCCT/STR guidelines for coronary artery calcium scoring of noncontrast noncardiac chest CT scans: A report of the Society of Cardiovascular Computed Tomography and Society of Thoracic Radiology. J. Cardiovasc. Comput. Tomogr. 2017, 11, 74–84. [Google Scholar] [CrossRef]
- Miedema, M.D.; Duprez, D.A.; Misialek, J.R.; Blaha, M.J.; Nasir, K.; Silverman, M.G.; Blankstein, R.; Budoff, M.J.; Greenland, P.; Folsom, A.R. Use of coronary artery calcium testing to guide aspirin utilization for primary prevention: Estimates from the multi-ethnic study of atherosclerosis. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 453–460. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2019. [Google Scholar] [CrossRef]
- Dedic, A.; Ten Kate, G.J.; Roos, C.J.; Neefjes, L.A.; de Graaf, M.A.; Spronk, A.; Delgado, V.; van Lennep, J.E.; Moelker, A.; Ouhlous, M.; et al. Prognostic Value of Coronary Computed Tomography Imaging in Patients at High Risk without Symptoms of Coronary Artery Disease. Am. J. Cardiol. 2016, 117, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Motoyama, S.; Sarai, M.; Harigaya, H.; Anno, H.; Inoue, K.; Hara, T.; Naruse, H.; Ishii, J.; Hishida, H.; Wong, N.D.; et al. Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J. Am. Coll. Cardiol. 2009, 54, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Andreini, D.; Magnoni, M.; Conte, E.; Masson, S.; Mushtaq, S.; Berti, S.; Canestrari, M.; Casolo, G.; Gabrielli, D.; Latini, R.; et al. CAPIRE Investigators. Coronary Plaque Features on CTA Can Identify Patients at Increased Risk of Cardiovascular Events. JACC Cardiovasc. Imaging 2020, 13, 1704–1717. [Google Scholar] [CrossRef]
- Min, J.K.; Dunning, A.; Lin, F.Y.; Achenbach, S.; Al-Mallah, M.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; Chang, H.J.; Cheng, V.; et al. Age- and sex-related differences in all-cause mortality risk based on coronary computed tomography angiography findings results from the International Multicenter CONFIRM of 23,854 patients without known coronary artery disease. J. Am. Coll. Cardiol. 2011, 58, 849–860. [Google Scholar] [CrossRef]
- Conte, E.; Annoni, A.; Pontone, G.; Mushtaq, S.; Guglielmo, M.; Baggiano, A.; Volpato, V.; Agalbato, C.; Bonomi, A.; Veglia, F.; et al. Evaluation of coronary plaque characteristics with coronary computed tomography angiography in patients with non-obstructive coronary artery disease: A long-term follow-up study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1170–1178. [Google Scholar] [CrossRef]
- Mushtaq, S.; De Araujo Gonçalves, P.; Garcia-Garcia, H.M.; Pontone, G.; Bartorelli, A.L.; Bertella, E.; Campos, C.M.; Pepi, M.; Serruys, P.W.; Andreini, D. Long-term prognostic effect of coronary atherosclerotic burden: Validation of the computed tomography-Leaman score. Circ. Cardiovasc. Imaging 2015, 8, e002332. [Google Scholar] [CrossRef]
- Andreini, D.; Pontone, G.; Mushtaq, S.; Gransar, H.; Conte, E.; Bartorelli, A.L.; Pepi, M.; Opolski, M.P.; Ó Hartaigh, B.; Berman, D.S.; et al. Long-term prognostic impact of CT-Leaman score in patients with non-obstructive CAD: Results from the COronary CT Angiography EvaluatioN for Clinical Outcomes InteRnational Multicenter (CONFIRM) study. Int. J. Cardiol. 2017, 231, 18–25. [Google Scholar] [CrossRef]
- Boogers, M.J.; Broersen, A.; van Velzen, J.E.; de Graaf, F.R.; El-Naggar, H.M.; Kitslaar, P.H.; Dijkstra, J.; Delgado, V.; Boersma, E.; de Roos, A.; et al. Automated quantification of coronary plaque with computed tomography: Comparison with intravascular ultrasound using a dedicated registration algorithm for fusion-based quantification. Eur. Heart J. 2012, 33, 1007–1016. [Google Scholar] [CrossRef]
- Fischer, C.; Hulten, E.; Belur, P.; Smith, R.; Voros, S.; Villines, T.C. Coronary CT angiography versus intravascular ultrasound for estimation of coronary stenosis and atherosclerotic plaque burden: A meta-analysis. J. Cardiovasc. Comput. Tomogr. 2013, 7, 256–266. [Google Scholar] [CrossRef]
- Symons, R.; Morris, J.Z.; Wu, C.O.; Pourmorteza, A.; Ahlman, M.A.; Lima, J.A.; Chen, M.Y.; Mallek, M.; Sandfort, V.; Bluemke, D.A. Coronary CT Angiography: Variability of CT Scanners and Readers in Measurement of Plaque Volume. Radiology 2016, 281, 737–748. [Google Scholar] [CrossRef] [PubMed]
- Saremi, F.; Achenbach, S. Coronary plaque characterization using CT. AJR Am. J. Roentgenol. 2015, 204, W249–W260. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.J.; Lin, F.Y.; Lee, S.E.; Andreini, D.; Bax, J.; Cademartiri, F.; Chinnaiyan, K.; Chow, B.J.W.; Conte, E.; Cury, R.C.; et al. Coronary Atherosclerotic Precursors of Acute Coronary Syndromes. J. Am. Coll. Cardiol. 2018, 71, 2511–2522. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.C.; Moss, A.J.; Dweck, M.; Adamson, P.D.; Alam, S.; Hunter, A.; Shah, A.S.V.; Pawade, T.; Weir-McCall, J.R.; Roditi, G.; et al. Coronary Artery Plaque Characteristics Associated with Adverse Outcomes in the SCOT-HEART Study. J. Am. Coll. Cardiol. 2019, 73, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Conte, E.; Dwivedi, A.; Mushtaq, S.; Pontone, G.; Lin, F.Y.; Hollenberg, E.J.; Lee, S.E.; Bax, J.; Cademartiri, F.; Chinnaiyan, K.; et al. Age- and sex-related features of atherosclerosis from coronary computed tomography angiography in patients prior to acute coronary syndrome: Results from the ICONIC study. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Hartaigh, B.Ó.; Gransar, H.; Lee, J.H.; Rizvi, A.; Baskaran, L.; Schulman-Marcus, J.; Dunning, A.; Achenbach, S.; Al-Mallah, M.H.; et al. Incremental prognostic value of coronary computed tomography angiography over coronary calcium scoring for major adverse cardiac events in elderly asymptomatic individuals. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Muhlestein, J.B.; Lappé, D.L.; Lima, J.A.; Rosen, B.D.; May, H.T.; Knight, S.; Bluemke, D.A.; Towner, S.R.; Le, V.; Bair, T.L.; et al. Effect of screening for coronary artery disease using CT angiography on mortality and cardiac events in high-risk patients with diabetes: The FACTOR-64 randomized clinical trial. JAMA 2014, 312, 2234–2243. [Google Scholar] [CrossRef]
- Cho, I.; Chang, H.J.; Ó Hartaigh, B.; Shin, S.; Sung, J.M.; Lin, F.Y.; Achenbach, S.; Heo, R.; Berman, D.S.; Budoff, M.J.; et al. Incremental prognostic utility of coronary CT angiography for asymptomatic patients based upon extent and severity of coronary artery calcium: Results from the COronary CT Angiography EvaluatioN for Clinical Outcomes InteRnational Multicenter (CONFIRM) study. Eur. Heart J. 2015, 36, 501–508. [Google Scholar]
- Kim, K.J.; Choi, S.I.; Lee, M.S.; Kim, J.A.; Chun, E.J.; Jeon, C.H. The prevalence and characteristics of coronary atherosclerosis in asymptomatic subjects classified as low risk based on traditional risk stratification algorithm: Assessment with coronary CT angiography. Heart 2013, 99, 1113–1117. [Google Scholar] [CrossRef]
- Detrano, R.; Guerci, A.D.; Carr, J.J.; Bild, D.E.; Burke, G.; Folsom, A.R.; Liu, K.; Shea, S.; Szklo, M.; Bluemke, D.A.; et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N. Engl. J. Med. 2008, 358, 1336–1345. [Google Scholar] [CrossRef]
- Min, J.K.; Labounty, T.M.; Gomez, M.J.; Achenbach, S.; Al-Mallah, M.; Budoff, M.J.; Cademartiri, F.; Callister, T.Q.; Chang, H.J.; Cheng, V.; et al. Incremental prognostic value of coronary computed tomographic angiography over coronary artery calcium score for risk prediction of major adverse cardiac events in asymptomatic diabetic individuals. Atherosclerosis 2014, 232, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Park, G.M.; Lee, S.W.; Yun, S.C.; Kim, Y.H.; Cho, Y.R.; Park, H.W.; Suh, J.; Yang, D.H.; Kang, J.W.; et al. Long-Term Prognostic Value of Coronary CT Angiography in Asymptomatic Type 2 Diabetes Mellitus. JACC Cardiovasc. Imaging 2016, 9, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Halon, D.A.; Lavi, I.; Barnett-Griness, O.; Rubinshtein, R.; Zafrir, B.; Azencot, M.; Lewis, B.S. Plaque Morphology as Predictor of Late Plaque Events in Patients with Asymptomatic Type 2 Diabetes: A Long-Term Observational Study. JACC Cardiovasc. Imaging 2019, 12, 1353–1363. [Google Scholar] [CrossRef] [PubMed]
- Andreini, D.; Pontone, G.; Mushtaq, S.; Bertella, E.; Conte, E.; Baggiano, A.; Veglia, F.; Agostoni, P.; Annoni, A.; Formenti, A.; et al. Prognostic value of multidetector computed tomography coronary angiography in diabetes: Excellent long-term prognosis in patients with normal coronary arteries. Diabetes Care 2013, 36, 1834–1841. [Google Scholar] [CrossRef] [PubMed]
- Magnoni, M.; Masson, S.; Andreini, D.; Moccetti, T.; Modena, M.G.; Canestrari, M.; Berti, S.; Casolo, G.; Gabrielli, D.; Marraccini, P.; et al. Usefulness of High-Sensitivity Cardiac Troponin T for the Identification of Outlier Patients with Diffuse Coronary Atherosclerosis and Low-Risk Factors. Am. J. Cardiol. 2016, 117, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Conte, E.; Andreini, D.; Magnoni, M.; Masson, S.; Mushtaq, S.; Berti, S.; Canestrari, M.; Casolo, G.; Gabrielli, D.; Latini, R.; et al. Association of high-risk coronary atherosclerosis at CCTA with clinical and circulating biomarkers: Insight from CAPIRE study. J. Cardiovasc. Comput. Tomogr. 2020. [Google Scholar] [CrossRef]
- Braber, T.L.; Reitsma, J.B.; Mosterd, A.; Willemink, M.J.; Prakken, N.H.J.; Halle, M.; Sharma, S.; Velthuis, B.K. Cardiac imaging to detect coronary artery disease in athletes aged 35 years and older. A scoping review. Scand. J. Med. Sci. Sports 2018, 28, 1036–1047. [Google Scholar] [CrossRef]
- Puri, R.; Nicholls, S.J.; Shao, M.; Kataoka, Y.; Uno, K.; Kapadia, S.R.; Tuzcu, E.M.; Nissen, S.E. Impact of statins on serial coronary calcification during atheroma progression and regression. J. Am. Coll. Cardiol. 2015, 65, 1273–1282. [Google Scholar] [CrossRef]
- Lee, S.E.; Chang, H.J.; Sung, J.M.; Park, H.B.; Heo, R.; Rizvi, A.; Lin, F.Y.; Kumar, A.; Hadamitzky, M.; Kim, Y.J.; et al. Effects of Statins on Coronary Atherosclerotic Plaques: The PARADIGM Study. JACC Cardiovasc. Imaging 2018, 11, 1475–1484. [Google Scholar] [CrossRef]
- Vaidya, K.; Arnott, C.; Martínez, G.J.; Ng, B.; McCormack, S.; Sullivan, D.R.; Celermajer, D.S.; Patel, S. Colchicine Therapy and Plaque Stabilization in Patients with Acute Coronary Syndrome: A CT Coronary Angiography Study. JACC Cardiovasc. Imaging 2018, 11, 305–316. [Google Scholar] [CrossRef]
- Nicholls, S.J.; Puri, R.; Anderson, T.; Ballantyne, C.M.; Cho, L.; Kastelein, J.J.P.; Koenig, W.; Somaratne, R.; Kassahun, H.; Yang, J.; et al. Effect of Evolocumab on Coronary Plaque Composition. J. Am. Coll. Cardiol. 2018, 72, 2012–2021. [Google Scholar] [CrossRef] [PubMed]
- Villines, T.C.; Hulten, E.A.; Shaw, L.J.; Goyal, M.; Dunning, A.; Achenbach, S.; Al-Mallah, M.; Berman, D.S.; Budoff, M.J.; Cademartiri, F.; et al. CONFIRM Registry Investigators. Prevalence and severity of coronary artery disease and adverse events among symptomatic patients with coronary artery calcification scores of zero undergoing coronary computed tomography angiography: Results from the CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter) registry. J. Am. Coll. Cardiol. 2011, 58, 2533–2540. [Google Scholar] [CrossRef] [PubMed]
- Conte, E.; Mushtaq, S.; Pontone, G.; Li Piani, L.; Ravagnani, P.; Galli, S.; Collet, C.; Sonck, J.; Di Odoardo, L.; Guglielmo, M.; et al. Plaque quantification by coronary computed tomography angiography using intravascular ultrasound as a reference standard: A comparison between standard and last generation computed tomography scanners. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Min, J.K.; Jones, E.C.; Peña, J.M. The Future from the Past: A Chance for Change. J. Am. Coll. Cardiol. 2016, 67, 1769–1771. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Left-Dominance | Right-Dominance | Balanced-Dominance | |
|---|---|---|---|
| Coronary Segments | |||
| Left main | 5 | 6 | 5.5 |
| LAD proximal | 3.5 | 3.5 | 3.5 |
| LAD mid | 2.5 | 2.5 | 2.5 |
| LAD distal/1st diagonal | 1 | 1 | 1 |
| 2nd diagonal | 0.5 | 0.5 | 0.5 |
| LCX proximal | 1.5 | 2.5 | 2 |
| LCX distal | 0.5 | 1.5 | 1 |
| 1st and 2nd marginal | 1 | 1 | 1 |
| RCA (all segments) | 1 | 0 | 0.5 |
| PDA | 1 | Not applicable | 0.5 |
| PDA from LCA | Not applicable | 1 | Not applicable |
| PL from RCA | 0.5 | Not applicable | Not applicable |
| PL from LCA | Not applicable | 0.5 | 0.5 |
| Intermedium | 1 | 1 | 1 |
| Stenosis Severity | |||
| Obstructive CAD | 1 | 1 | 1 |
| Nonobstructive CAD | 0.615 | 0.615 | 0.615 |
| Plaque composition | |||
| Noncalcified or mixed | 1.5 | 1.5 | 1.5 |
| Calcified | 1 | 1 | 1 |
| Patient-Based | Segment-Based | ||
|---|---|---|---|
| Conventional Reading | Advanced Analysis | Conventional Reading | Advanced Analysis |
|
|
|
|
| High-Risk Feature | Definition | Example |
|---|---|---|
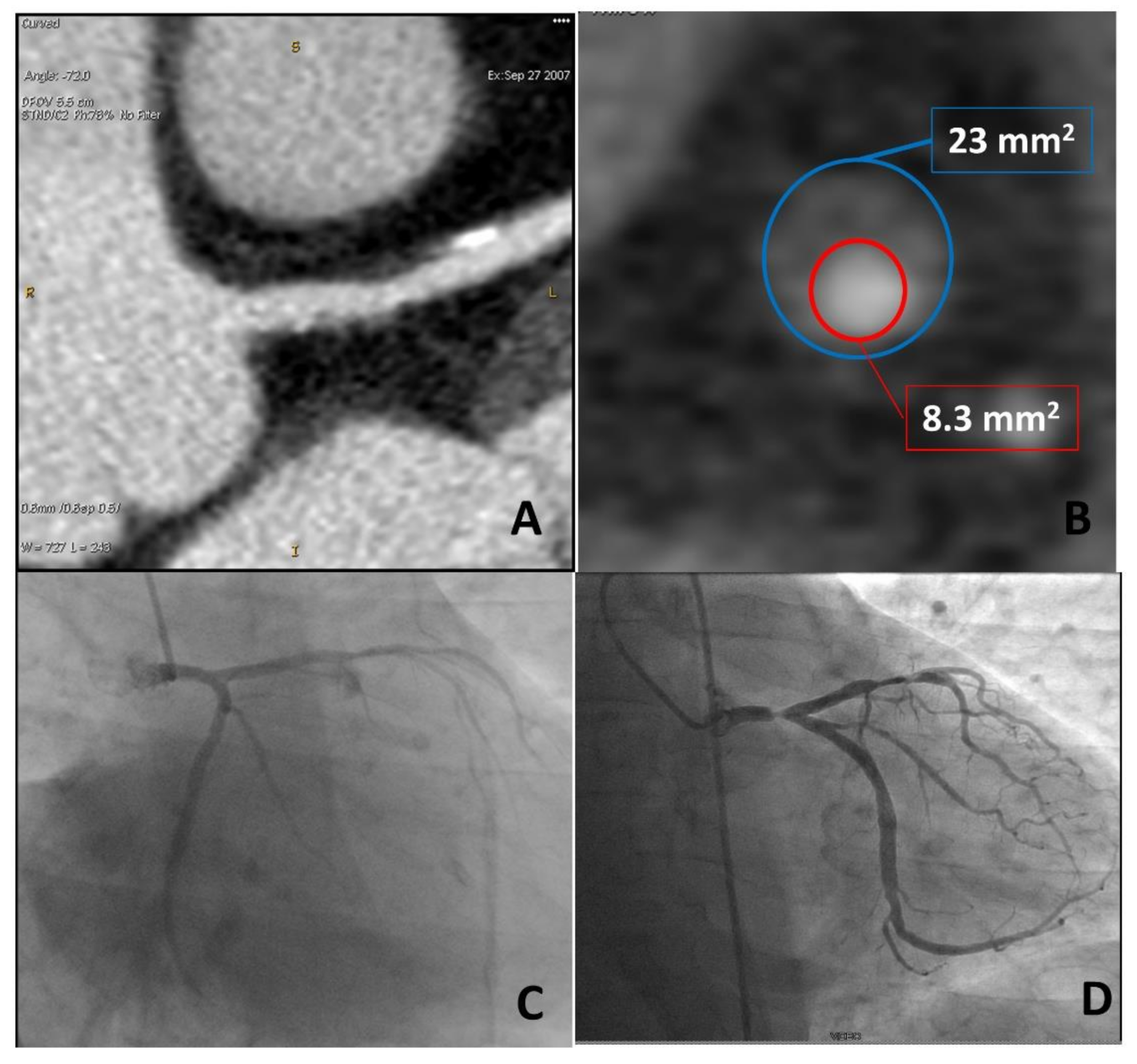
| Remodeling index (RI) | Ratio between lesion plaque area (red circle) and reference lumen area (blue circle). Positive remodeling is defined as RI > 1.1. |  |
| Low-attenuation plaque (LAP) | Presence of any voxel < 30 HU in a coronary plaque. |  |
| Plaque burden (PB) | Derived by the following formula: (lesion plaque area (red circle)—lesion lumen area (blue circle))/lesion plaque area (red circle). |  |
| Napkin-ring sign (NRS) | Presence of rim-like thin enhancement (no more than 130 HU) distributed along the outer contour of the vessel and surrounding a fibro-lipidic plaque. |  |
| Small spotty calcifications (SC) | Any discrete calcification ≤ 3 mm in length and occupying ≤ 90° arc when viewed on short axis. |  |
| Authors | Publication Year | PopulationNumber | CACS/CCTA | Endpoints | Follow-Up | Main Results | Ref |
|---|---|---|---|---|---|---|---|
| Kondos et al. | 2003 | 8855 | CACS | (1) Death (2) MI (3) Revascularization procedure | 37 ± 12 months | CACS provides incremental information vs. conventional CAD risk assessment. | [14] |
| Taylor et al. | 2005 | 2000 | CACS | (1) ACS (2) Sudden cardiac death | 3 ± 1.4 years | CACS provides substantial, cost-effective, independent prognostic value incremental coronary risk factors. | [6] |
| Budoff et al. | 2007 | 25,253 | CACS | All-cause mortality | 6 ± 3 years | CACS provides independent incremental information in addition to traditional risk factors in the prediction of all-cause mortality. | [15] |
| Detrano et al. | 2008 | 6722 | CACS | (1) MI (2) Death due to coronary heart disease | 3.8 years | CACS provides predictive information beyond that provided by standard risk factors. | [41] |
| Muhlestein et al. | 2014 | 900 | CCTA | (1) ACS (2) All causes of death | 4 years | Among asymptomatic patients with type 1 or type 2 diabetes, use of CCTA to screen for CAD did not reduce cardiovascular events. | [38] |
| Cho et al. | 2015 | 3217 | CACS and CCTA | (1) MI (2) All causes of death | 24 months | CCTA provides incremental prognostic utility for asymptomatic individuals with moderately high CACS, but not for lower or higher CACS. | [39] |
| Joong Kim et al. | 2013 | 2133 | CCTA | (1) ACS (2) Cardiac death (3) Coronary revascularization | 29.3 ± 14.9 months | CCTA might have the potential to identify high-risk groups in the selected subjects regarded as a minimal-risk group according toNational Cholesterol Education Program NCEP guidelines. | [40] |
| Min et al. | 2014 | 27,125 | CCTA | (1) ACS (2) Cardiac death (3) Coronary revascularization | 2.4 ± 1.1 years | For asymptomatic diabetic individuals, CCTA measures of CAD severity confer incremental risk prediction. | [42] |
| Kang et al. | 2016 | 591 | CCTA | (1) Cardiac deaths (2) Nonfatal MI (3) UA (4) Late coronary revascularizations | 6 years | Results suggested long-term prognostic value of coronary CCTA for asymptomatic type 2 diabetes mellitus. | [43] |
| Halon et al. | 2019 | 630 | CCTA | ACS | 9.2 years | In asymptomatic patients with type 2 diabetes, CCTA plaque volume, percent low-density plaque content, and mild calcification predicted late plaque events. | [44] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conte, E.; Mushtaq, S.; Marchetti, D.; Mallia, V.; Belmonte, M.; Melotti, E.; Pontone, G.; Pepi, M.; Andreini, D. Potential Application of Cardiac Computed Tomography for Early Detection of Coronary Atherosclerosis: From Calcium Score to Advanced Atherosclerosis Analysis. J. Clin. Med. 2021, 10, 521. https://doi.org/10.3390/jcm10030521
Conte E, Mushtaq S, Marchetti D, Mallia V, Belmonte M, Melotti E, Pontone G, Pepi M, Andreini D. Potential Application of Cardiac Computed Tomography for Early Detection of Coronary Atherosclerosis: From Calcium Score to Advanced Atherosclerosis Analysis. Journal of Clinical Medicine. 2021; 10(3):521. https://doi.org/10.3390/jcm10030521
Chicago/Turabian StyleConte, Edoardo, Saima Mushtaq, Davide Marchetti, Vincenzo Mallia, Marta Belmonte, Eleonora Melotti, Gianluca Pontone, Mauro Pepi, and Daniele Andreini. 2021. "Potential Application of Cardiac Computed Tomography for Early Detection of Coronary Atherosclerosis: From Calcium Score to Advanced Atherosclerosis Analysis" Journal of Clinical Medicine 10, no. 3: 521. https://doi.org/10.3390/jcm10030521
APA StyleConte, E., Mushtaq, S., Marchetti, D., Mallia, V., Belmonte, M., Melotti, E., Pontone, G., Pepi, M., & Andreini, D. (2021). Potential Application of Cardiac Computed Tomography for Early Detection of Coronary Atherosclerosis: From Calcium Score to Advanced Atherosclerosis Analysis. Journal of Clinical Medicine, 10(3), 521. https://doi.org/10.3390/jcm10030521