
Religious Coping and Life Satisfaction during the COVID-19 Pandemic among Polish Catholics. The Mediating Effect of Coronavirus Anxiety

 ,
,  , , and
, , and
Abstract
:1. Introduction
1.1. Life Satisfaction and Religious Coping
1.2. The Anxiety of COVID-19 as a Mediator between Religious Coping and Life Satisfaction
1.3. Study Purpose
2. Method
2.1. Subjects and Procedure
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Minihan, E.; Gavin, B.; Kelly, B.D.; McNicholas, F. COVID-19, mental health and psychological first aid. Ir. J. Psychol. Med. 2020, 37, 259–263. [Google Scholar] [CrossRef]
- Deilamizade, A.; Moghanibashi-Mansourieh, A. Challenges of providing COVID-19 prevention services to homeless people who use drugs in Iran. Int. J. Drug Policy 2020, 83, 102806. [Google Scholar] [CrossRef] [PubMed]
- Moghanibashi-Mansourieh, A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102076. [Google Scholar] [CrossRef] [PubMed]
- Ran, L.; Wang, W.; Ai, M.; Kong, Y.; Chen, J.; Kuang, L. Psychological resilience, depression, anxiety, and somatization symptoms in response to COVID-19: A study of the general population in China at the peak of its epidemic. Soc. Sci. Med. 2020, 262, 113261. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 1–11. [Google Scholar] [CrossRef]
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Khaledi-Paveh, B.; Kazeminia, M.; Mohammadi, M.; Shohaimi, S.; Daneshkhah, A.; Eskandari, S. The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: A systematic review and meta-regression. Hum. Resour. Health 2020, 18, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bendau, A.; Petzold, M.B.; Pyrkosch, L.; Maricic, L.M.; Betzler, F.; Rogoll, J.; Große, J.; Ströhle, A.; Plag, J. Associations between COVID-19 related media consumption and symptoms of anxiety, depression and COVID-19 related fear in the general population in Germany. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 283–291. [Google Scholar] [CrossRef]
- Casagrande, M.; Favieri, F.; Tambelli, R.; Forte, G. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef]
- Fontanesi, L.; Marchetti, D.; Mazza, C.; Di Giandomenico, S.; Roma, P.; Verrocchio, M.C. The effect of the COVID-19 lockdown on parents: A call to adopt urgent measures. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S79–S81. [Google Scholar] [CrossRef]
- Mazza, M.; Marano, G.; Lai, C.; Janiri, L.; Sani, G. Danger in danger: Interpersonal violence during COVID-19 quarantine. Psychiatry Res. 2020, 289, 113046. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Sinyor, M.; Knipe, D.; Borges, G.; Ueda, M.; Pirkis, J.; Phillips, M.R.; Gunnell, D. Suicide risk and prevention during the COVID-19 pandemic. Arch. Suicide Res. 2021, 7, 468–471. [Google Scholar] [CrossRef]
- Imber-Black, E. Rituals in the Time of COVID 19: Imagination, Responsiveness and the Human Spirit. Fam. Process 2020, 59, 912–921. [Google Scholar] [CrossRef]
- John, A.; Pirkis, J.; Gunnell, D.; Appleby, L.; Morrissey, J. Trends in suicide during the COVID-19 pandemic. BMJ 2020, 371, m4352. [Google Scholar] [CrossRef]
- Arslan, G.; Yıldırım, M.; Tanhan, A.; Buluş, M.; Allen, K.-A. Coronavirus stress, optimism-pessimism, psychological inflexibility, and psychological health: Psychometric properties of the Coronavirus Stress Measure. Int. J. Ment. Health Addict. 2020, 1–17. [Google Scholar] [CrossRef]
- Burke, J.; Arslan, G. Positive Education and School Psychology During COVID-19 Pandemic. J. Posit. Sch. Psychol. 2020, 4, 137–139. [Google Scholar] [CrossRef]
- Van der Kaap-Deeder, J.; Vermote, B.; Waterschoot, J.; Soenens, B.; Morbée, S.; Vansteenkiste, M. The role of ego integrity and despair in older adults well-being during the COVID-19 crisis: The mediating role of need-based experiences. Eur. J. Ageing 2021, 1–13. [Google Scholar] [CrossRef]
- Sozańska, D. Chrześcijańska Demokracja w Polsce: Przyczyny s Labości i Szanse Rozwoju; Oficyna Wydawnicza AFM: Krakow, Poland, 2011. [Google Scholar]
- Brown, E.; Gray, R.; Lo Monaco, S.; O’Donoghue, B.; Nelson, B.; Thompson, A.; Francey, S.; McGorry, P. The potential impact of COVID-19 on psychosis: A rapid review of contemporary epidemic and pan-demic research. Schizophr. Res. 2020, 222, 79–87. [Google Scholar] [CrossRef]
- Roman, N.V.; Mthembu, T.G.; Hoosen, M. Spiritual care—“A deeper immunity”—A response to COVID-19 pandemic. Afr. J. Prim. Health Care Fam. Med. 2020, 12, 1. [Google Scholar] [CrossRef]
- Diener, E.D.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Veenhoven, R. The Overall Satisfaction with Life: Subjective Approaches (1). In Global Handbook of Quality of Life; Springer: Berlin/Heidelberg, Germany, 2015; pp. 207–238. [Google Scholar] [CrossRef] [Green Version]
- Fergusson, D.M.; McLeod, G.F.H.; Horwood, L.J.; Swain, N.R.; Chapple, S.; Poulton, R. Life satisfaction and mental health problems (18 to 35 years). Psychol. Med. 2015, 45, 2427–2436. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, P.; Jones, W.; Wang, L.; Shen, X.; Goldner, E.M. The fundamental association between mental health and life satisfaction: Results from successive waves of a Canadian national survey. BMC Public Health 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, J.M.; Fontaine, A.M.; Neri, A.L. The influence of physical and mental health on life satisfaction is mediated by self-rated health: A study with Brazilian elderly. Arch. Gerontol. Geriatr. 2016, 65, 104–110. [Google Scholar] [CrossRef]
- Arslan, G.; Yıldırım, M.; Zangeneh, M. Coronavirus Anxiety and Psychological Adjustment in College Students: Exploring the Role of College Belongingness and Social Media Addiction. Int. J. Ment. Health Addict. 2021, 1–14. [Google Scholar] [CrossRef]
- Yıldırım, M.; Arslan, G.; Wong, P.T.P. Meaningful living, resilience, affective balance, and psychological health problems among Turkish young adults during coronavirus pandemic. Curr. Psychol. 2021, 1–12. [Google Scholar] [CrossRef]
- Koenig, H.G. Maintaining Health and Well-Being by Putting Faith into Action During the COVID-19 Pandemic. J. Relig. Health 2020, 59, 2205–2214. [Google Scholar] [CrossRef]
- Láng, A. Impact of attachment to God and religious coping on life satisfaction. Orvosi Hetil. 2013, 154, 1843–1847. [Google Scholar] [CrossRef]
- Laxamana, R.D. A Phenomenological Study in the Diversity of Understanding about Spirituality of the Nurse Educators: The Core to Pedagogical Quality of Nursing Education. Int. J. Nurs. Sci. Clin. Pract. 2020, 1, 1–11. [Google Scholar]
- Alwala, B. What Has Science to Do with Religion? A Looming Challenge of Traditional and Religious Practices on Curbing the Spread of COVID-19 Pandemic in Kenya. East Afr. J. Tradit. Cult. Relig. 2020, 2, 23–33. [Google Scholar] [CrossRef]
- Chow, S.; Francis, B.; Ng, Y.; Naim, N.; Beh, H.; Ariffin, M.; Yusuf, M.; Lee, J.; Sulaiman, A. Religious Coping, Depression and Anxiety among Healthcare Workers during the COVID-19 Pandemic: A Malaysian Perspective. Healthcare 2021, 9, 79. [Google Scholar] [CrossRef]
- Dein, S.; Loewenthal, K.; Lewis, C.A.; Pargament, K.I. COVID-19, mental health and religion: An agenda for future research. Ment. Health Relig. Cult. 2020, 23, 1–9. [Google Scholar] [CrossRef]
- Fardin, M.A. COVID-19 and Anxiety: A Review of Psychological Impacts of Infectious Disease Outbreaks. Arch. Clin. Infect. Dis. 2020, 15. [Google Scholar] [CrossRef] [Green Version]
- Peteet, J.R. COVID-19 Anxiety. J. Relig. Health 2020, 59, 2203–2204. [Google Scholar] [CrossRef]
- Pirutinsky, S.; Cherniak, A.D.; Rosmarin, D.H. COVID-19, Mental Health, and Religious Coping Among American Orthodox Jews. J. Relig. Health 2020, 59, 2288–2301. [Google Scholar] [CrossRef]
- Thomas, J.; Barbato, M. Positive Religious Coping and Mental Health among Christians and Muslims in Response to the COVID-19 Pandemic. Religions 2020, 11, 498. [Google Scholar] [CrossRef]
- Walsh, F. Loss and resilience in the time of COVID-19: Meaning making, hope, and transcendence. Fam. Process 2020, 59, 898–911. [Google Scholar] [CrossRef]
- Dymecka, J.; Gerymski, R.; Machnik-Czerwik, A. How does stress affect life satisfaction during the COVID-19 pandemic? Moderated mediation analysis of sense of coherence and fear of coronavirus. Psychol. Health Med. 2021, 1–9. [Google Scholar] [CrossRef]
- Krok, D.; Zarzycka, B.; Telka, E. Religiosity, Meaning-Making and the Fear of COVID-19 Affecting Well-Being Among Late Adolescents in Poland: A Moderated Mediation Model. J. Relig. Health 2021, 60, 3265–3281. [Google Scholar] [CrossRef]
- Mahamid, F.A.; Bdier, D. The Association Between Positive Religious Coping, Perceived Stress, and Depressive Symptoms During the Spread of Coronavirus (COVID-19) Among a Sample of Adults in Palestine: Across Sectional Study. J. Relig. Health 2021, 60, 34–49. [Google Scholar] [CrossRef] [PubMed]
- Piwko, A.M. Islam and the COVID-19 Pandemic: Between Religious Practice and Health Protection. J. Relig. Health 2021, 60, 3291–3308. [Google Scholar] [CrossRef]
- Beasley, M.; Thompson, T.; Davidson, J. Resilience in response to life stress: The effects of coping style and cognitive hardiness. Pers. Individ. Differ. 2003, 34, 77–95. [Google Scholar] [CrossRef]
- Buser, J.K.; Kearney, A. Stress, adaptive coping, and life satisfaction. J. Coll. Couns. 2017, 20, 224–236. [Google Scholar] [CrossRef]
- Di Marco, S.; Feggi, A.; Cammarata, E.; Girardi, L.; Bert, F.; Scaioli, G.; Gramaglia, C.; Zeppegno, P. Schizophrenia and major depression: Resilience, coping styles, personality traits, self-esteem and quality of life. Eur. Psychiatry 2017, 41, S192–S193. [Google Scholar] [CrossRef]
- Carver, C.S.; Connor-Smith, J. Personality and Coping. Annu. Rev. Psychol. 2010, 61, 679–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Pers. Soc. Psychol. 1989, 56, 267. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S.; Scheier, M.F. Situational coping and coping dispositions in a stressful transaction. J. Pers. Soc. Psychol. 1994, 66, 184. [Google Scholar] [CrossRef]
- Pargament, K.I.; Brant, C.R. Religion and Coping. In Handbook of Religion and Mental Health; Elsevier: Amsterdam, The Netherlands, 1998; pp. 111–128. [Google Scholar]
- Roesch, S.C.; Ano, G. Testing an Attribution and Coping Model of Stress: Religion as an Orienting System. J. Psychol. Christ. 2003, 22, 3. [Google Scholar]
- Tarakeshwar, N.; Pargament, K.I. Religious Coping in Families of Children with Autism. Focus Autism Dev. Disabil. 2001, 16, 247–260. [Google Scholar] [CrossRef]
- Ano, G.G.; Vasconcelles, E.B. Religious coping and psychological adjustment to stress: A meta-analysis. J. Clin. Psychol. 2005, 61, 461–480. [Google Scholar] [CrossRef]
- Scandrett, K.G.; Mitchell, S.L. Religiousness, religious coping, and psychological well-being in nursing home residents. J. Am. Med. Dir. Assoc. 2009, 10, 581–586. [Google Scholar] [CrossRef] [Green Version]
- Rosmarin, D.H.; Pargament, K.I.; Flannelly, K.J. Do Spiritual Struggles Predict Poorer Physical/Mental Health Among Jews? Int. J. Psychol. Relig. 2009, 19, 244–258. [Google Scholar] [CrossRef]
- Rosmarin, D.H.; Pargament, K.I.; Krumrei, E.J.; Flannelly, K.J. Religious coping among jews: Development and initial validation of the JCOPE. J. Clin. Psychol. 2009, 65, 670–683. [Google Scholar] [CrossRef] [PubMed]
- Abu Raiya, H.; Pargament, K.I.; Mahoney, A.; Stein, C. A psychological measure of Islamic religiousness: Development and evidence for reliability and validity. Int. J. Psychol. Relig. 2008, 18, 291–315. [Google Scholar] [CrossRef]
- Abu Raiya, H.; Pargament, K.I. Religiously integrated psychotherapy with Muslim clients: From research to practice. Prof. Psychol. Res. Pract. 2010, 41, 181–188. [Google Scholar] [CrossRef]
- Phillips, R.E., III; Cheng, C.M.; Pargament, K.I.; Oemig, C.; Colvin, S.D.; Abarr, A.N.; Dunn, M.W.; Reed, A.S. Spiritual coping in American Buddhists: An exploratory study. Int. J. Psychol. Relig. 2009, 19, 231–243. [Google Scholar] [CrossRef]
- Tarakeshwar, N.; Pargament, K.I.; Mahoney, A. Initial development of a measure of religious coping among Hindus. J. Community Psychol. 2003, 31, 607–628. [Google Scholar] [CrossRef]
- Toussaint, L.L.; Williams, D.R. National Survey Results for Protestant, Catholic, and Nonreligious Experiences of Seeking Forgiveness and of Forgiveness of Self, of Others, and by God. J. Psychol. Christ. 2008, 27, 2. [Google Scholar]
- Szcześniak, M.; Kroplewski, Z.; Szałachowski, R. The Mediating Effect of Coping Strategies on Religious/Spiritual Struggles and Life Satisfaction. Religions 2020, 11, 195. [Google Scholar] [CrossRef]
- Zarzycka, B.; Ziętek, P. Spiritual Growth or Decline and Meaning-Making as Mediators of Anxiety and Satisfaction with Life During Religious Struggle. J. Relig. Health 2018, 58, 1072–1086. [Google Scholar] [CrossRef] [Green Version]
- Hebert, R.; Zdaniuk, B.; Schulz, R.; Scheier, M. Positive and Negative Religious Coping and Well-Being in Women with Breast Cancer. J. Palliat. Med. 2009, 12, 537–545. [Google Scholar] [CrossRef]
- Krok, D. Religijny system znaczeń i religijne radzenie sobie ze stresem a eudajmonistyczny dobrostan psychiczny. Rocz. Psychol. 2014, 17, 647–664. [Google Scholar]
- Pargament, K.I.; Koenig, H.G.; Tarakeshwar, N.; Hahn, J. Religious struggle as a predictor of mortality among medically ill elderly patients: A 2-year longitudinal study. Arch. Intern. Med. 2001, 161, 1881–1885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wnuk, M. Duchowy charakter Programu Dwunastu Kroków a jakość życia Anonimowych Alkoholików. Alkohol. Narkom. 2007, 20, 289–301. [Google Scholar]
- Taheri-Kharameh, Z.; Zamanian, H.; Montazeri, A.; Asgarian, A.; Esbiri, R. Negative Religious Coping, Positive Religious Coping, and Quality of Life Among Hemodialysis Patients. Nephro-Urol. Mon. 2016, 8, e38009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, B.S. Spiritually-focused psychotherapy for people diagnosed with cancer: A pilot outcome study. Ment. Health Relig. Cult. 2005, 8, 217–226. [Google Scholar] [CrossRef]
- Feder, A.; Ahmad, S.; Lee, E.J.; Morgan, J.; Singh, R.; Smith, B.W.; Southwick, S.M.; Charney, D.S. Coping and PTSD symptoms in Pakistani earthquake survivors: Purpose in life, religious coping and social support. J. Affect. Disord. 2013, 147, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Ng, G.C.; Mohamed, S.; Sulaiman, A.H.; Zainal, N.Z. Anxiety and Depression in Cancer Patients: The Association with Religiosity and Religious Coping. J. Relig. Health 2016, 56, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Habib, H.A.; Hussain, S. Religious Coping as a Predictor of Positive Affect and Life Satisfaction during Epidemic Conditions of COVID-19. Sir Syed J. Educ. Soc. Res. 2020, 3, 42–48. [Google Scholar] [CrossRef]
- Henslee, A.M.; Coffey, S.F.; Schumacher, J.A.; Tracy, M.; Norris, F.H.; Galea, S. Religious Coping and Psychological and Behavioral Adjustment After Hurricane Katrina. J. Psychol. 2014, 149, 630–642. [Google Scholar] [CrossRef] [Green Version]
- Aflakseir, A.; Mahdiyar, M. The Role of Religious Coping Strategies in Predicting Depression among a Sample of Women with Fertility Problems in Shiraz. J. Reprod. Infertil. 2016, 17, 117–122. [Google Scholar]
- Nikmanesh, Z.; Azaraein, S. The Role of Religious Coping in Perception of Suffering among Patients Undergoing Dialysis. Jundishapur J. Chronic Dis. Care 2016, 6, e40063. [Google Scholar] [CrossRef] [Green Version]
- Pérez, J.E.; Smith, A.R. Intrinsic religiousness and well-being among cancer patients: The mediating role of control-related religious coping and self-efficacy for coping with cancer. J. Behav. Med. 2015, 38, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Park, C.L.; Holt, C.L.; Le, D.; Christie, J.; Williams, B.R. Positive and Negative Religious Coping Styles as Prospective Predictors of Well-Being in African Americans. Psycholog. Relig. Spiritual. 2018, 10, 318–326. [Google Scholar] [CrossRef]
- Bjorck, J.P.; Kim, J.-W. Religious coping, religious support, and psychological functioning among short-term missionaries. Ment. Health Relig. Cult. 2009, 12, 611–626. [Google Scholar] [CrossRef]
- Greenglass, E.R.; Fiksenbaum, L. Proactive coping, positive affect, and well-being: Testing for mediation using path analysis. Eur. Psychol. 2009, 14, 29–39. [Google Scholar] [CrossRef]
- Rosmarin, D.H.; Leidl, B. Spirituality, religion, and anxiety disorders. Handb. Spiritual. Relig. Ment. Health 2020, 41–60. [Google Scholar]
- Lee, S.A.; Mathis, A.A.; Jobe, M.C.; Pappalardo, E.A. Clinically significant fear and anxiety of COVID-19: A psychometric examination of the Coronavirus Anxiety Scale. Psychiatry Res. 2020, 290, 113112. [Google Scholar] [CrossRef] [PubMed]
- Skalski, S.; Uram, P.; Dobrakowski, P.; Kwiatkowska, A. The link between ego-resiliency, social support, SARS-CoV-2 anxiety and trauma effects. Polish adaptation of the Coronavirus Anxiety Scale. Pers. Individ. Differ. 2020, 171, 110540. [Google Scholar] [CrossRef]
- Wang, C.; Zhao, H. The Impact of COVID-19 on Anxiety in Chinese University Students. Front. Psychol. 2020, 11, 1168. [Google Scholar] [CrossRef]
- Hamm, A.O. Fear, anxiety, and their disorders from the perspective of psychophysiology. Psychophysiology 2019, 57, e13474. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Paluszek, M.M.; Landry, C.A.; Rachor, G.S.; McKay, D.; Taylor, S. Do pre-existing anxiety-related and mood disorders differentially impact COVID-19 stress responses and coping? J. Anxiety Disord. 2020, 74, 102271. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Taylor, S. Coronaphobia: Fear and the 2019-nCoV outbreak. J. Anxiety Disord. 2020, 70, 102196. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Taylor, S. How health anxiety influences responses to viral outbreaks like COVID-19: What all decision-makers, health authorities, and health care professionals need to know. J. Anxiety Disord. 2020, 71, 102211. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A.; Jobe, M.C.; Mathis, A.A.; Gibbons, J.A. Incremental validity of coronaphobia: Coronavirus anxiety explains depression, generalized anxiety, and death anxiety. J. Anxiety Disord. 2020, 74, 102268. [Google Scholar] [CrossRef] [PubMed]
- Skalski, S.; Uram, P.; Dobrakowski, P.; Kwiatkowska, A. Thinking too much about the novel coronavirus. The link between persistent thinking about COVID-19, SARS-CoV-2 anxiety and trauma effects. Curr. Issues Pers. Psychol. 2020, 8, 169–174. [Google Scholar] [CrossRef]
- George, L.K.; Ellison, C.G.; Larson, D.B. Explaining the Relationships Between Religious Involvement and Health. Psychol. Inq. 2002, 13, 190–200. [Google Scholar] [CrossRef]
- Chapman, L.K.; Steger, M.F. Race and religion: Differential prediction of anxiety symptoms by religious coping in African American and European American young adults. Depression Anxiety 2008, 27, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Francis, B.; Gill, J.S.; Han, N.Y.; Petrus, C.F.; Azhar, F.L.; Sabki, Z.A.; Said, M.A.; Hui, K.O.; Guan, N.C.; Sulaiman, A.H. Religious Coping, Religiosity, Depression and Anxiety among Medical Students in a Multi-Religious Setting. Int. J. Environ. Res. Public Health 2019, 16, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugas, M.J.; Laugesen, N.; Bukowski, W.M. Intolerance of uncertainty, fear of anxiety, and adolescent worry. J. Abnorm. Child Psychol. 2012, 40, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Skalski, S.; Konaszewski, K.; Dobrakowski, P.; Surzykiewicz, J.; Lee, S.A. Pandemic grief in Poland: Adaptation of a measure and its relationship with social support and resilience. Curr. Psychol. 2021, 1–9. [Google Scholar] [CrossRef]
- Arora, A.; Jha, A.K.; Alat, P.; Das, S.S. Understanding coronaphobia. Asian J. Psychiatry 2020, 54, 102384. [Google Scholar] [CrossRef]
- Fiske, S.T.; Taylor, S.E. Social Cognition: From Brains to Culture; SAGE Publishing: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Pargament, K.I.; Smith, B.W.; Koenig, H.G.; Perez, L. Patterns of Positive and Negative Religious Coping with Major Life Stressors. J. Sci. Study Relig. 1998, 37, 710–724. [Google Scholar] [CrossRef]
- Jarosz, M. Skala religijnego radzenia sobie-wersja skrócona (Brief RCOPE). Psychol. Pomiar Relig. 2011, 293–316. [Google Scholar]
- Büssing, A.; Fischer, J.; Haller, A.; Heusser, P.; Ostermann, T.; Matthiessen, P.F. Validation of the brief multidimensional life satisfaction scale in patients with chronic diseases. Eur. J. Med Res. 2009, 14, 171–177. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming, 3rd ed.; Routledge: Oxfordshire, UK, 2016. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Publications: New York, NY, USA, 2015. [Google Scholar] [CrossRef]
- Aten, J.D.; Shannonhouse, L.R.; Davis, D.E.; Davis, E.B.; Hook, J.N.; Van Tongeren, D.R.; Zhao, J.H.; McElroy-Heltzel, S.E.; Schruba, A.; Annan, K.; et al. Spiritual First Aid for COVID-19. J. Psychol. Christ. 2020, 39, 265–275. [Google Scholar]
- Wildman, W.J.; Bulbulia, J.; Sosis, R.; Schjoedt, U. Religion and the COVID-19 Pandemic; Taylor & Francis: Oxfordshire, UK, 2020. [Google Scholar]
- Koenig, H.G. Is religion good for your health? The effects of religion on physical and mental health. Psychol. Press 1997, 156. [Google Scholar]
- Wilt, J.A.; Takahashi, J.T.; Yun, D.; Jeong, P.; Exline, J.J.; Pargament, K.I. Personality, religious and spiritual struggles, and well-being. Psychol. Relig. Spirit. 2016, 341, 8. [Google Scholar] [CrossRef]
- Saud, M.; Ashfaq, A.; Abbas, A.; Mahmood, Q.K. Seeking social support through Religion, Psychological wellbeing and Social capital: A Global Survey on Coronavirus situational stress and coping strategies. Res. Sq. 2020, 1–12. [Google Scholar] [CrossRef]
- Yoon, D.P.; Lee, E.-K.O. The Impact of Religiousness, Spirituality, and Social Support on Psychological Well-Being Among Older Adults in Rural Areas. J. Gerontol. Soc. Work. 2006, 48, 281–298. [Google Scholar] [CrossRef]
- Holt, C.L.; Roth, D.L.; Huang, J.; Park, C.L.; Clark, E.M. Longitudinal effects of religious involvement on religious coping and health behaviors in a national sample of African Americans. Soc. Sci. Med. 2017, 187, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Cole, G.L. Existential Dissonance: A Dimension of Inauthenticity. Humanist. Psychol. 2015, 296, 44. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; Dickerhoof, R.; Boehm, J.K.; Sheldon, K.M. Becoming happier takes both a will and a proper way: An experimental longitudinal intervention to boost well-being. Emotion 2011, 11, 391–402. [Google Scholar] [CrossRef]
- Büssing, A.; Franczak, K.; Surzykiewicz, J. Frequency of Spiritual/Religious Practices in Polish Patients with Chronic Diseases: Validation of the Polish Version of the SpREUK-P Questionnaire. Religions 2014, 5, 459–476. [Google Scholar] [CrossRef] [Green Version]
- Büssing, A.; Wirth, A.G.; Reiser, F.; Zahn, A.; Humbroich, K.; Gerbershagen, K.; Schimrigk, S.; Haupts, M.; Hvidt, N.C.; Baumann, K. Experience of gratitude, awe and beauty in life among patients with multiple sclerosis and psychiatric disorders. Health Qual. Life Outcomes 2014, 12, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finogenow, M. Rozwój w okresie późnej dorosłości-szanse i zagrożenia. 297 Pomyślne starzenie się-uwarunkowania społeczne, przestrzenne i zdrowotne. Acta Univ. Lodz. Folia Oeconomica 2013, 93–104. [Google Scholar]
- Finogenow, M. Poczucie własnej atrakcyjności a poczucie dobrostanu w okresie późnej dorosłości-moderująca rola płci, Pedagog. Społeczna 2018, 3, 109–122. [Google Scholar]
- Junik, W. Teoretyczne i empiryczne podstawy wzmacniania rezyliencji (resilience) u dzieci z rodzin z problemem alkoholowym. Dziecko Krzywdzone Teor. Badania Prakt. 2012, 11, 27–45. [Google Scholar]
- Shacham, M.; Greenblatt-Kimron, L.; Hamama-Raz, Y.; Martin, L.; Peleg, O.; Ben-Ezra, M.; Mijiritsky, E. Increased COVID-19 Vaccination Hesitancy and Health Awareness amid COVID-19 Vaccinations Programs in Israel. Int. J. Environ. Res. Public Health 2021, 18, 3804. [Google Scholar] [CrossRef]
- Aw, J.; Jie, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 Vaccine Hesitancy—A Scoping Review of Literature in High-Income Countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 1. | 2. | 3. | 4. | 5. | |
|---|---|---|---|---|---|
| 1. BMLSS | - | ||||
| 2. BMLSS SUPPORT | 0.62 ** | - | |||
| 3. CAS | −0.21 ** | −0.14 ** | - | ||
| 4. PRCOPE | 0.15 ** | 0.33 ** | 0.13 * | - | |
| 5. NRCOPE | −0.24 ** | −0.06 | 0.22 ** | 0.23 ** | - |
| M | 39.22 | 11.17 | 1.65 | 15.68 | 9.77 |
| SD | 12.48 | 6.27 | 3.60 | 7.48 | 4.11 |
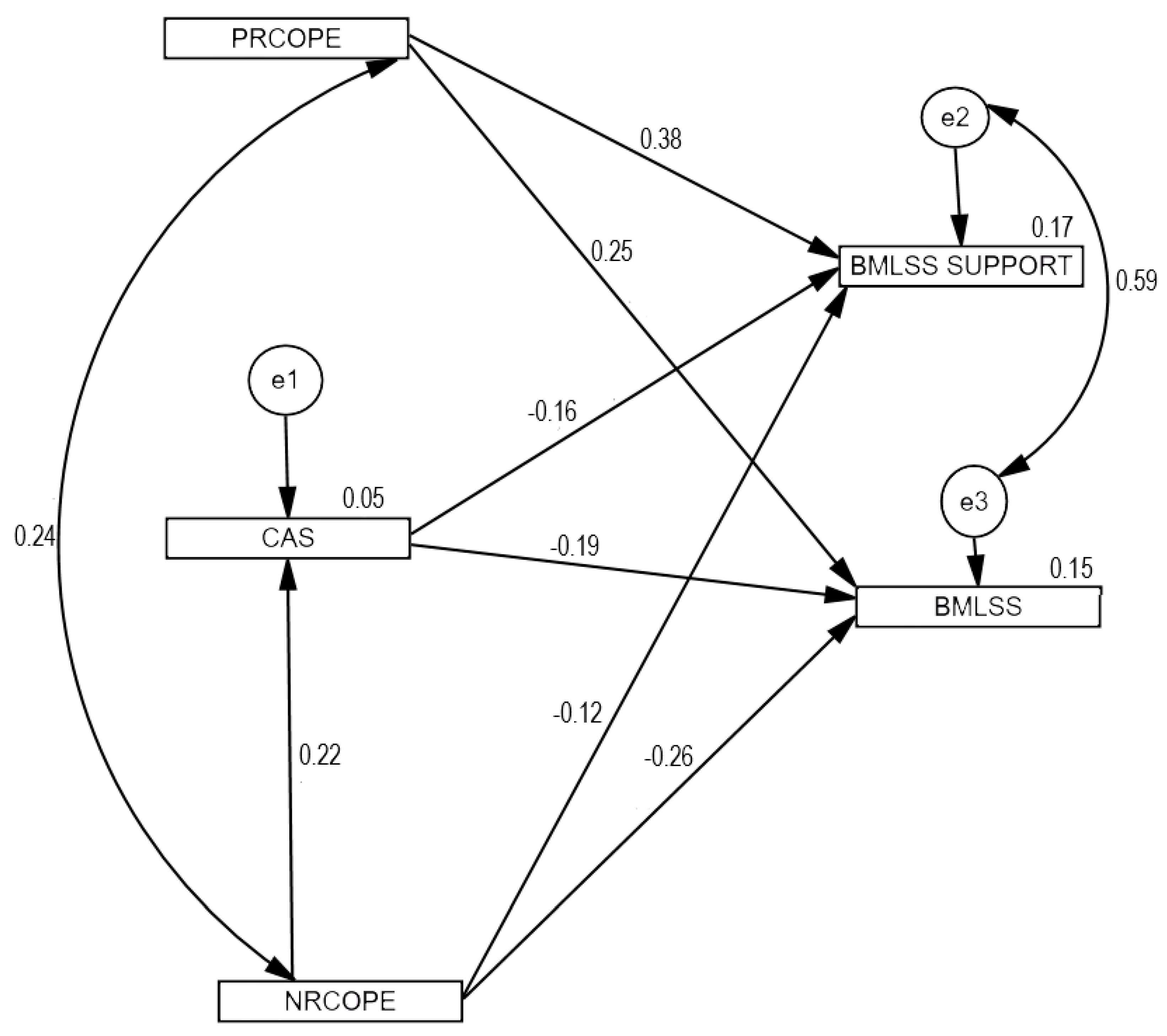
| β | B | SE | C.R. | p | |
|---|---|---|---|---|---|
| NRCOPE > CAS | 0.22 | 0.165 | 0.038 | 4.390 | *** |
| CAS > BMLSS | −0.19 | −0.725 | 0.186 | −3.895 | *** |
| RRCOPE > BMLSS SUPPORT | 0.38 | 0.352 | 0.045 | 7.746 | *** |
| PRCOPE > BMLSS | 0.25 | 0.430 | 0.087 | 4.942 | *** |
| NRCOPE > BMLSS | −0.26 | −0.712 | 0.141 | −5.060 | *** |
| CAS > BMLSS SUPPORT | −0.16 | −0.327 | 0.097 | −3.358 | *** |
| NRCOPE > BMLSS SUPPORT | −0.12 | −0.171 | 0.073 | −2.325 | 0.020 |
| 95% CI | ||||
|---|---|---|---|---|
| β | B | LL | UL | |
| NRCOPE > CAS > BMLSS_SUPPORT | −0.04 | −0.05 | −0.10 | −0.03 |
| NRCOPE > CAS> BMLSS | −0.04 | −0.12 | −0.22 | −0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrakowski, P.P.; Skalski, S.; Surzykiewicz, J.; Muszyńska, J.; Konaszewski, K. Religious Coping and Life Satisfaction during the COVID-19 Pandemic among Polish Catholics. The Mediating Effect of Coronavirus Anxiety. J. Clin. Med. 2021, 10, 4865. https://doi.org/10.3390/jcm10214865
Dobrakowski PP, Skalski S, Surzykiewicz J, Muszyńska J, Konaszewski K. Religious Coping and Life Satisfaction during the COVID-19 Pandemic among Polish Catholics. The Mediating Effect of Coronavirus Anxiety. Journal of Clinical Medicine. 2021; 10(21):4865. https://doi.org/10.3390/jcm10214865
Chicago/Turabian StyleDobrakowski, Paweł Piotr, Sebastian Skalski, Janusz Surzykiewicz, Jolanta Muszyńska, and Karol Konaszewski. 2021. "Religious Coping and Life Satisfaction during the COVID-19 Pandemic among Polish Catholics. The Mediating Effect of Coronavirus Anxiety" Journal of Clinical Medicine 10, no. 21: 4865. https://doi.org/10.3390/jcm10214865
APA StyleDobrakowski, P. P., Skalski, S., Surzykiewicz, J., Muszyńska, J., & Konaszewski, K. (2021). Religious Coping and Life Satisfaction during the COVID-19 Pandemic among Polish Catholics. The Mediating Effect of Coronavirus Anxiety. Journal of Clinical Medicine, 10(21), 4865. https://doi.org/10.3390/jcm10214865