Association of Periodontal Status, Number of Teeth, and Obesity: A Cross-Sectional Study in Japan

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical Examinations
2.3. Statistical Analysis
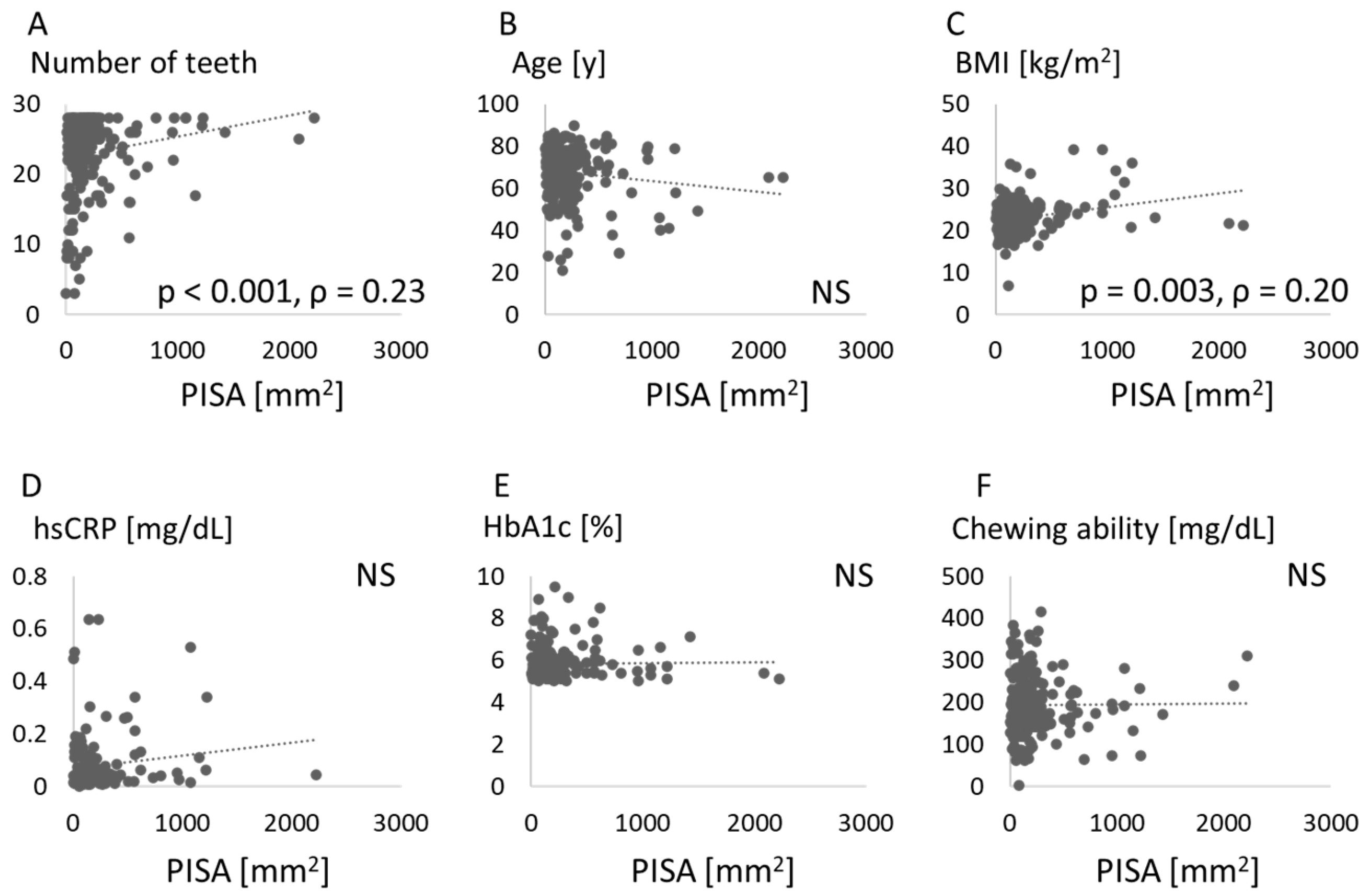
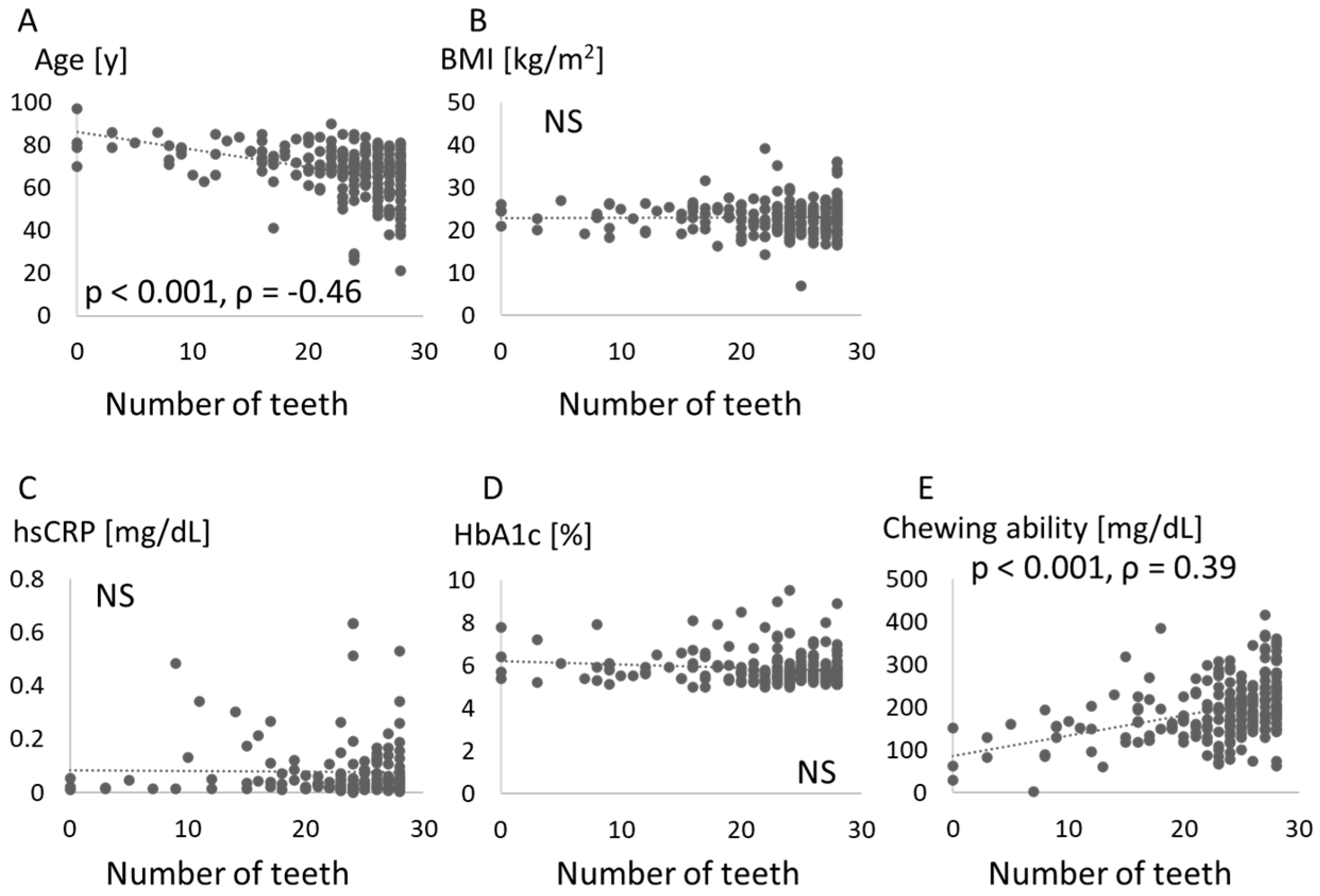
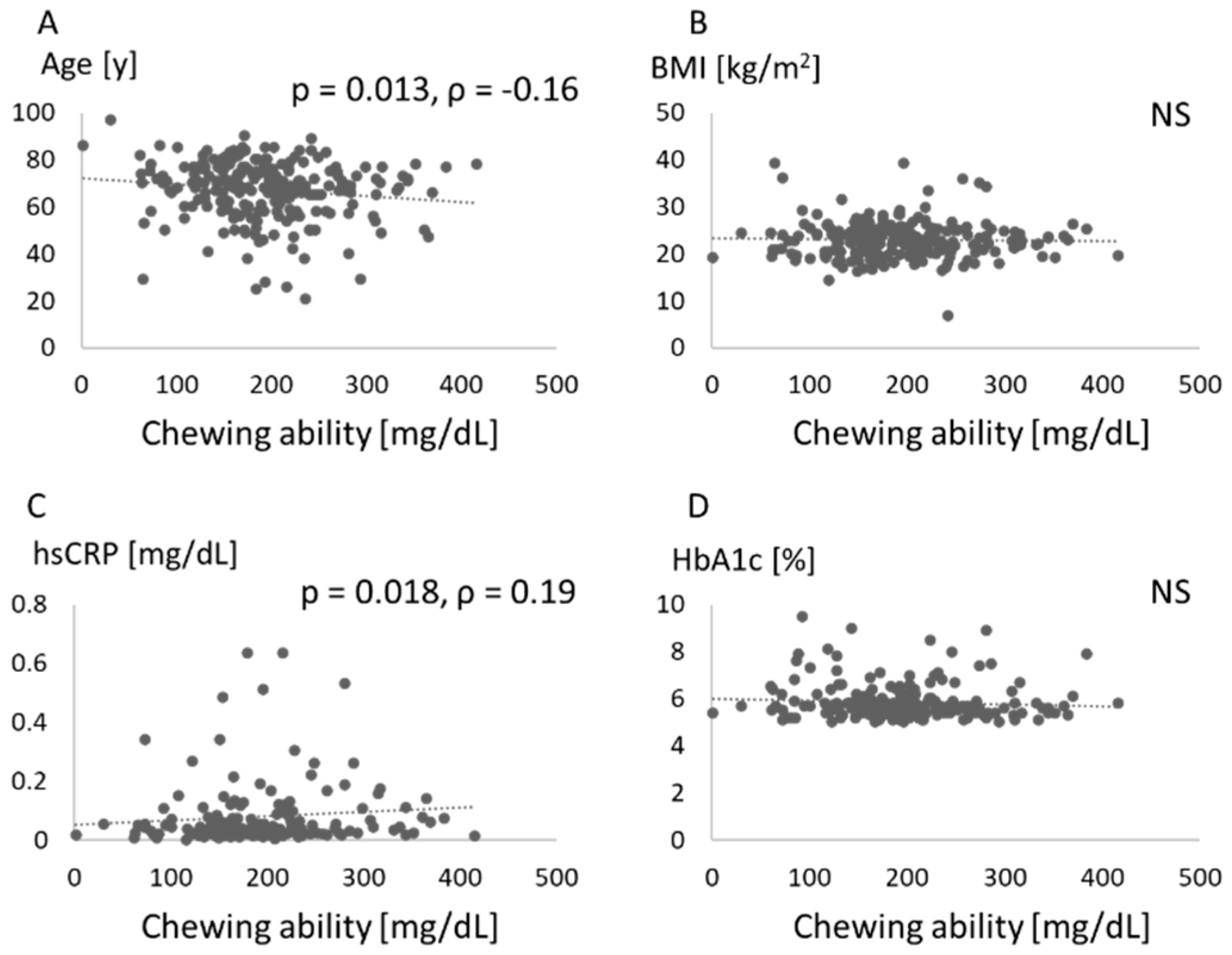
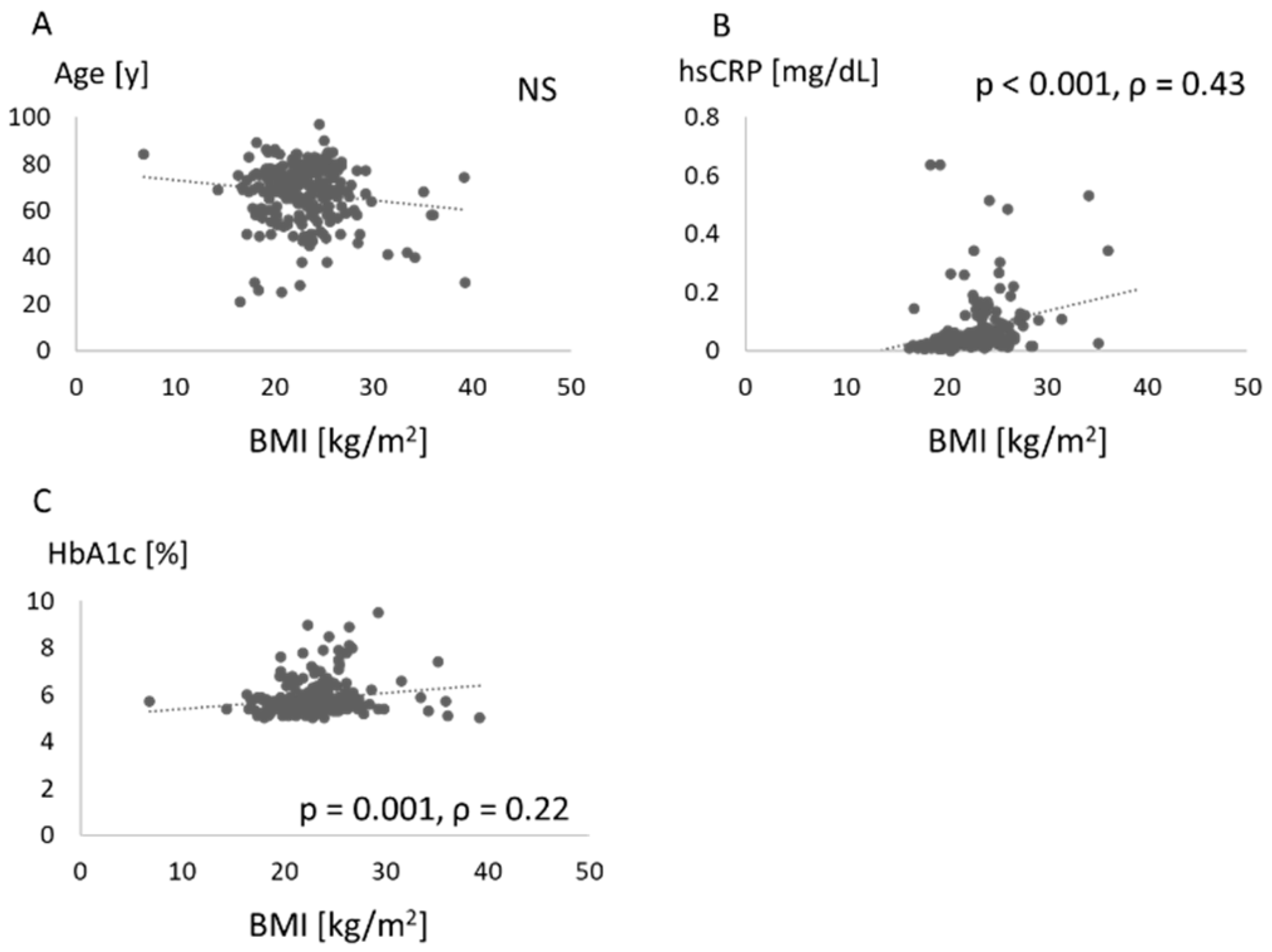
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kopelman, P.G. Obesity as a medical problem. Nature 2000, 404, 635–643. [Google Scholar]
- Bouldin, M.J.; Ross, L.A.; Sumrall, C.D.; Loustalot, F.V.; Low, A.K.; Land, K.K. The effect of obesity surgery on obesity comorbidity. Am. J. Med. Sci. 2006, 331, 183–193. [Google Scholar] [CrossRef]
- Williams, R.C. Periodontal disease. N. Engl. J. Med. 1990, 322, 373–382. [Google Scholar] [CrossRef]
- Dietrich, T.; Jimenez, M.; Krall Kaye, E.A.; Vokonas, P.S.; Garcia, R.I. Age-dependent associations between chronic periodontitis/edentulism and risk of coronary heart disease. Circulation 2008, 117, 1668–1674. [Google Scholar]
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality from ischemic heart disease. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef]
- Sanz, M.; Del Castillo, A.M.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar]
- Jepsen, S.; Suvan, J.; Deschner, J. The association of periodontal diseases with metabolic syndrome and obesity. Periodontology 2000 2020, 83, 125–153. [Google Scholar]
- Martens, L.; De Smet, S.; Yusof, M.Y.P.M.; Rajasekharan, S. Association between overweight/obesity and periodontal disease in children and adolescents: A systematic review and meta-analysis. Eur. Arch. Paediatr. Dent. 2017, 18, 69–82. [Google Scholar] [CrossRef]
- Genco, R.J.; Grossi, S.G.; Ho, A.; Nishimura, F.; Murayama, Y. A proposed model linking inflammation to obesity, diabetes, and periodontal infections. J. Periodontol. 2005, 76, 2075–2084. [Google Scholar]
- Thanakun, S.; Izumi, Y. Effect of periodontitis on adiponectin, C-reactive protein, and immunoglobulin G against Porphyromonas gingivalis in Thai people with overweight or obese status. J. Periodontol. 2016, 87, 566–576. [Google Scholar] [CrossRef]
- Martinez-Herrera, M.; Silvestre-Rangil, J.; Silvestre, F.J. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e708–e715. [Google Scholar] [CrossRef]
- Vallim, A.C.; Gaio, E.J.; Oppermann, R.V.; Rösing, C.K.; Albandar, J.M.; Susin, C.; Haas, A.N. Obesity as a risk factor for tooth loss over 5 years: A population-based cohort study. J. Clin. Periodontol. 2021, 48, 14–23. [Google Scholar] [CrossRef]
- Isola, G. Current evidence of natural agents in oral and periodontal health. Nutrients 2020, 12, 585. [Google Scholar] [CrossRef]
- Almoznino, G.; Gal, N.; Levin, L.; Mijiritsky, E.; Weinberg, G.; Lev, R.; Zini, A.; Touger-Decker, R.; Chebath-Taub, D.; Shay, B. Diet practices, body mass index, and oral health-related quality of life in adults with periodontitis—A case-control study. Int. J. Environ. Res. Public Health 2020, 17, 2340. [Google Scholar] [CrossRef]
- Kanasi, E.; Ayilavarapu, S.; Jones, J. The aging population: Demographics and the biology of aging. Periodontology 2000 2016, 72, 13–18. [Google Scholar] [CrossRef]
- Nishi, N. Monitoring obesity trends in health Japan 21. J. Nutr. Sci. Vitaminol. 2015, 61, S17–S19. [Google Scholar] [CrossRef]
- Nesse, W.; Abbas, F.; van der Ploeg, I.; Spijkervet, F.K.; Dijkstra, P.U.; Vissink, A. Periodontal inflamed surface area: Quantifying inflammatory burden. J. Clin. Periodontol. 2008, 35, 668–673. [Google Scholar] [CrossRef]
- Kameyama, A.; Ishii, K.; Tomita, S.; Tatsuta, C.; Sugiyama, T.; Ishizuka, Y.; Takahashi, T.; Tsunoda, M. Correlations between Perceived Oral Malodor Levels and Self-Reported Oral Complaints. Int. J. Dent. 2015, 2015, 343527. [Google Scholar]
- Caballero, B. Humans against obesity: Who will win? Adv. Nutr. 2019, 10, S4–S9. [Google Scholar] [CrossRef]
- Aoyama, N.; Suzuki, J.I.; Thanakun, S.; Izumi, Y.; Minabe, M.; Isobe, M. Elevated concentrations of specific periodontopathic pathogens associated with severe periodontitis in Japanese patients with cardiovascular disease and concomitant obesity. J. Oral Biosci. 2018, 60, 54–58. [Google Scholar]
- Botero, J.E.; Yepes, F.L.; Roldán, N.; Castrillón, C.A.; Hincapie, J.P.; Ochoa, S.; Ospina, C.A.; Becerra, M.A.; Jaramillo, A.; Gutierrez, S.J.; et al. Tooth and periodontal clinical attachment loss are associated with hyperglycemia in patients with diabetes. J. Periodontol. 2012, 83, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, S.; Nitta, H.; Nagasawa, T.; Uchimura, I.; Izumiyama, H.; Inagaki, K.; Kikuchi, T.; Noguchi, T.; Kanazawa, M.; Matsuo, A.; et al. Multi-center intervention study on glycohemoglobin (HbA1c) and serum, high-sensitivity CRP (hs-CRP) after local anti-infectious periodontal treatment in type 2 diabetic patients with periodontal disease. Diabetes Res. Clin. Pract. 2009, 83, 308–315. [Google Scholar] [CrossRef] [PubMed]
- King, D.E.; Mainous, A.G., 3rd; Buchanan, T.A.; Pearson, W.S. C-reactive protein and glycemic control in adults with diabetes. Diabetes Care 2003, 26, 1535–1539. [Google Scholar] [CrossRef] [PubMed]
- Susanto, H.; Nesse, W.; Dijkstra, P.U.; Hoedemaker, E.; van Reenen, Y.H.; Agustina, D.; Vissink, A.; Abbas, F. Periodontal inflamed surface area and C-reactive protein as predictors of HbA1c: A study in Indonesia. Clin. Oral Investig. 2012, 16, 1237–1242. [Google Scholar] [CrossRef]
- Nomura, Y.; Kakuta, E.; Okada, A.; Otsuka, R.; Shimada, M.; Tomizawa, Y.; Taguchi, C.; Arikawa, K.; Daikoku, H.; Sato, T.; et al. Effects of self-assessed chewing ability, tooth loss and serum albumin on mortality in 80-year-old individuals: A 20-year follow-up study. BMC Oral Health 2020, 20, 122. [Google Scholar] [CrossRef]
- Kosaka, T.; Ono, T.; Kida, M.; Kikui, M.; Yamamoto, M.; Yasui, S.; Nokubi, T.; Maeda, Y.; Kokubo, Y.; Watanabe, M.; et al. A multifactorial model of masticatory performance: The Suita study. J. Oral Rehabil. 2016, 43, 340–347. [Google Scholar] [CrossRef]
- Barbe, A.G.; Javadian, S.; Rott, T.; Scharfenberg, I.; Deutscher, H.C.D.; Noack, M.J.; Derman, S.H.M. Objective masticatory efficiency and subjective quality of masticatory function among patients with periodontal disease. J. Clin. Periodontol. 2020, 47, 1344–1353. [Google Scholar] [CrossRef]
- Okamoto, N.; Amano, N.; Nakamura, T.; Yanagi, M. Relationship between tooth loss, low masticatory ability, and nutritional indices in the elderly: A cross-sectional study. BMC Oral Health 2019, 19, 110. [Google Scholar] [CrossRef]
- Nakazawa, M.; Yamamoto, T.; Muto, E.; Seino, H.; Sasaki, S.; Kakugawa, T.; Shirai, Y.; Mochida, Y.; Fuchida, S.; Minabe, M. Association of glycosylated hemoglobin a1c with the masticatory function and periodontitis in type 2 diabetes patients hospitalized for an education program: A cross-sectional study. J. Jpn. Soc. Periodontol. 2020, 62, 74–81. (In Japanese) [Google Scholar] [CrossRef]
- Brennan, D.S.; Spencer, A.J.; Roberts-Thomson, K.F. Tooth loss, chewing ability and quality of life. Qual. Life Res. 2008, 17, 227–235. [Google Scholar] [CrossRef]
- Darnton-Hill, I.; Nishida, C.; James, W.P. A life course approach to diet, nutrition and the prevention of chronic diseases. Public Health Nutr. 2004, 7, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Herman, D.R.; Baer, M.T.; Adams, E.; Cunningham-Sabo, L.; Duran, N.; Johnson, D.B.; Yakes, E. Life Course Perspective: Evidence for the role of nutrition. Matern. Child Health J. 2014, 18, 450–461. [Google Scholar] [CrossRef] [PubMed]
- Nesse, W.; Linde, A.; Abbas, F.; Spijkervet, F.; Dijkstra, P.U.; de Brabander, E.C.; Gerstenbluth, I.; Vissink, A. Dose-response relationship between periodontal inflamed surface area and HbA1c in type 2 diabetics. J. Clin. Periodontol. 2009, 36, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Temelli, B.; Yetkin Ay, Z.; Aksoy, F.; Büyükbayram, H.İ.; Kumbul Doğuç, D.; Uskun, E.; Varol, E. Platelet indices (mean platelet volume and platelet distribution width) have correlations with periodontal inflamed surface area in coronary artery disease patients: A pilot study. J. Periodontol. 2018, 89, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Leira, Y.; Rodríguez-Yáñez, M.; Arias, S.; López-Dequidt, I.; Campos, F.; Sobrino, T.; D’Aiuto, F.; Castillo, J.; Blanco, J. Periodontitis is associated with systemic inflammation and vascular endothelial dysfunction in patients with lacunar infarct. J. Periodontol. 2019, 90, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, J. Usefulness of salivary testing machine on oral care management: Pilot study. Int. J. Clin. Prev. Dent. 2018, 14, 89–94. [Google Scholar] [CrossRef]
- Świątkowska, M.; Piekoszewska-Ziętek, P.; Gozdowski, D.; Olczak-Kowalczyk, D. The usefulness of Spotchem® Analyser (Arkray) in determining the risk in oral diseases in adolescents—A pilot study. Nowa Stomatol. 2018, 23, 9–17. [Google Scholar]
- Irie, Y.; Tatsukawa, N.; Iwamoto, Y.; Nakano, M.; Ogasawara, T.; Sakurai, K.; Mitsuhata, C.; Kozai, K. Investigation of pediatric specifications for the Salivary Multi Test® saliva test system. Pediatric. Dent. J. 2018, 28, 148–153. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), S162–S170. [Google Scholar]
- Offenbacher, S.; Barros, S.P.; Beck, J.D. Rethinking periodontal inflammation. J. Periodontol. 2008, 79, 1577–1584. [Google Scholar] [CrossRef]
- Loos, B.G.; Van Dyke, T.E. The role of inflammation and genetics in periodontal disease. Periodontology 2000 2020, 83, 26–39. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| N | 235 |
| Female (n, (%)) | 155 (66%) |
| Age (years) | 67.2 ± 12.6 1 |
| Height (cm) | 157.5 ± 8.6 1 |
| Weight (kg) | 57.6 ± 11.7 1 |
| BMI (kg/m2) | 23.1 ± 3.9 1 |
| Overweight (BMI 25–29.9 kg/m2) (n, (%)) | 55 (23%) |
| Obese (BMI ≥ 30 kg/m2) (n, (%)) | 8 (3.4%) |
| Number of teeth | 25 (21, 27) 2 |
| hsCRP (mg/dL) | 0.078 ± 0.112 1 |
| HbA1c (%) | 5.85 ± 0.75 1 |
| Chewing ability (mg/dL) | 192.0 ± 69.5 1 |
| Methyl-mercaptan | 9 (4, 28) 2 |
| Protein score | 61.3 ± 25.0 1 |
| Leukocyte score | 47.1 ± 23.4 1 |
| HbA1c < 7% | HbA1c ≥ 7% | p | |
|---|---|---|---|
| Insufficient chewing ability 1 | 22% | 44% | 0.047 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aoyama, N.; Fujii, T.; Kida, S.; Nozawa, I.; Taniguchi, K.; Fujiwara, M.; Iwane, T.; Tamaki, K.; Minabe, M. Association of Periodontal Status, Number of Teeth, and Obesity: A Cross-Sectional Study in Japan. J. Clin. Med. 2021, 10, 208. https://doi.org/10.3390/jcm10020208
Aoyama N, Fujii T, Kida S, Nozawa I, Taniguchi K, Fujiwara M, Iwane T, Tamaki K, Minabe M. Association of Periodontal Status, Number of Teeth, and Obesity: A Cross-Sectional Study in Japan. Journal of Clinical Medicine. 2021; 10(2):208. https://doi.org/10.3390/jcm10020208
Chicago/Turabian StyleAoyama, Norio, Toshiya Fujii, Sayuri Kida, Ichirota Nozawa, Kentaro Taniguchi, Motoki Fujiwara, Taizo Iwane, Katsushi Tamaki, and Masato Minabe. 2021. "Association of Periodontal Status, Number of Teeth, and Obesity: A Cross-Sectional Study in Japan" Journal of Clinical Medicine 10, no. 2: 208. https://doi.org/10.3390/jcm10020208
APA StyleAoyama, N., Fujii, T., Kida, S., Nozawa, I., Taniguchi, K., Fujiwara, M., Iwane, T., Tamaki, K., & Minabe, M. (2021). Association of Periodontal Status, Number of Teeth, and Obesity: A Cross-Sectional Study in Japan. Journal of Clinical Medicine, 10(2), 208. https://doi.org/10.3390/jcm10020208