
Determinants of Cue-Elicited Alcohol Craving and Perceived Realism in Virtual Reality Environments among Patients with Alcohol Use Disorder

 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
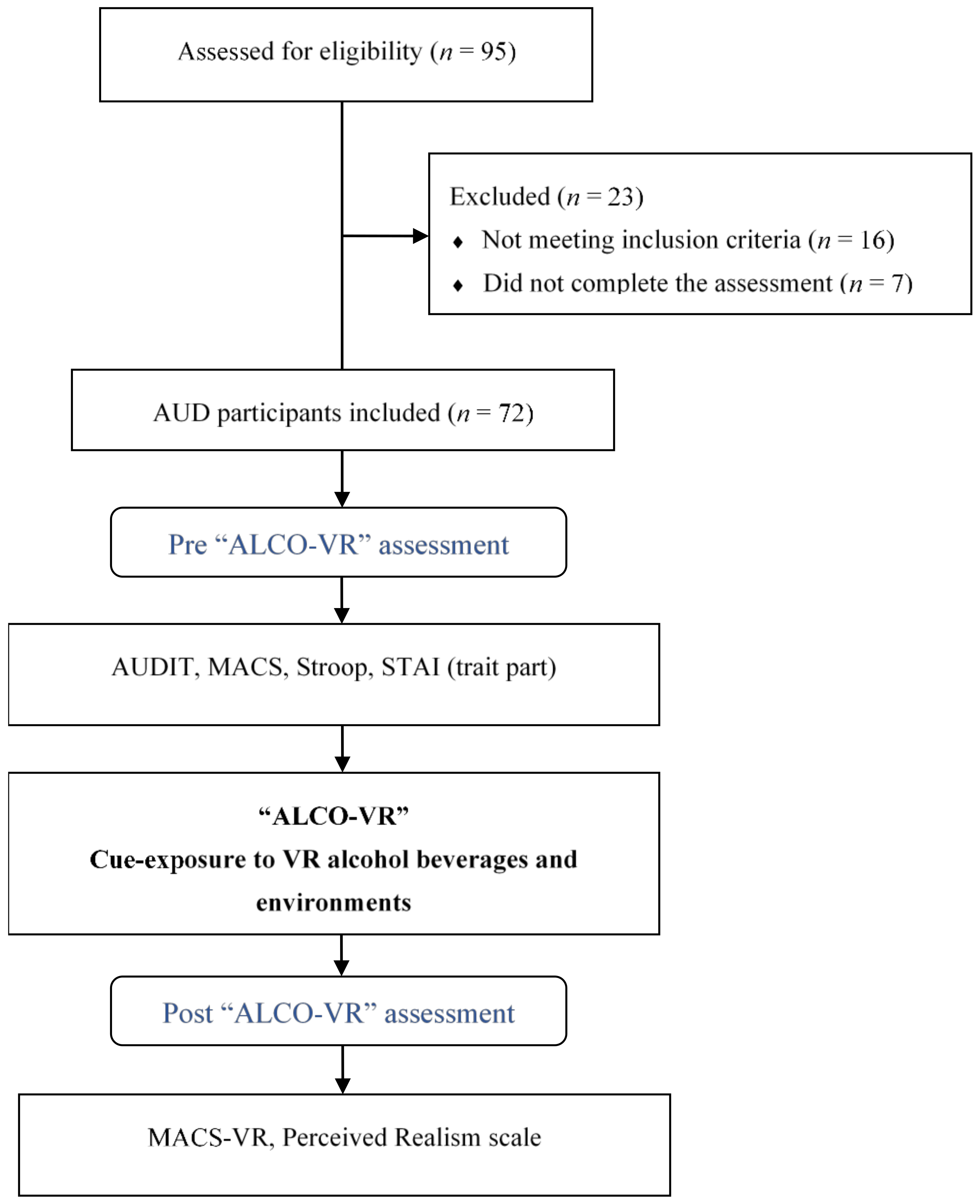
2.1. Participants
2.2. Measures
2.3. Instruments
2.3.1. Hardware
2.3.2. Software
2.4. Procedure
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hone-Blanchet, A.; Wensing, T.; Fecteau, S. The use of virtual reality in craving assessment and cue-exposure therapy in substance use disorders. Front. Hum. Neurosci. 2014, 8, 1–15. [Google Scholar] [CrossRef]
- Keyes, K.M.; Krueger, R.F.; Grant, B.F.; Hasin, D.S. Alcohol craving and the dimensionality of alcohol disorders. Psychol. Med. 2011, 41, 629–640. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stohs, M.E.; Schneekloth, T.D.; Geske, J.R.; Biernacka, J.M.; Karpyak, V.M. Alcohol craving predicts relapse after residential addiction treatment. Alcohol Alcohol. 2019, 54, 167–172. [Google Scholar] [CrossRef]
- Drummond, D.C. Theories of drugs craving, ancient and modern. Addiction 2001, 96, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Hartwell, E.E.; Ray, L.A. Craving as a DSM-5 symptom of alcohol use disorder in non-treatment seekers. Alcohol Alcohol. 2018, 53, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Van Lier, H.G.; Pieterse, M.E.; Schraagen, J.M.C.; Postel, M.G.; Vollenbroek-Hutten, M.M.R.; de Haan, H.A.; Noordzij, M.L. Identifying viable theoretical frameworks with essential parameters for real-time and real world alcohol craving research: A systematic review of craving models. Addict. Res. Theory 2018, 26, 35–51. [Google Scholar] [CrossRef]
- Carvalho, A.F.; Heilig, M.; Perez, A.; Probst, C.; Rehm, J. Alcohol use disorders. Lancet 2019, 781–792. [Google Scholar] [CrossRef]
- Grodin, E.N.; Sussman, L.; Sundby, K.; Brennan, G.M.; Diazgranados, N.; Heilig, M.; Momenan, R. Neural correlates of compulsive alcohol seeking in heavy drinkers. Biol. Psychiatry Cogn. Neurosci. 2018, 3, 1022–1031. [Google Scholar] [CrossRef]
- Berridge, K.C.; Robinson, T.E. Liking, Wanting and the Incentive-Sensitization theory of addiction. Am. Psychol. 2016, 71, 670–679. [Google Scholar] [CrossRef]
- Quintana, D.S.; Guastella, A.J.; McGregor, I.S.; Hickie, I.B.; Kemp, A.H. Heart rate variability predicts alcohol craving in alcohol dependent outpatients: Further evidence for HRV as a psychophysiological marker of self-regulation. Drug. Alcohol Depend. 2013, 132, 359–398. [Google Scholar] [CrossRef]
- Schlauch, R.C.; Gwynn-Shapiro, D.; Stasiewicz, P.R.; Molnar, D.S.; Lang, A.R. Affect and craving: Positive and negative affect are differentially associated with approach and avoidance inclinations. Addict. Behav. 2013, 38, 1970–1979. [Google Scholar] [CrossRef]
- Field, M.; Mogg, K.; Bradley, B.P. Craving and cognitive biases for alcohol cues in social drinkers. Alcohol Alcohol. 2005, 40, 504–510. [Google Scholar] [CrossRef][Green Version]
- Blaine, S.K.; Nautiyal, N.; Hart, R.; Guarnaccia, J.B.; Sinha, R. Craving, cortisol and behavioral alcohol motivation responses to stress and alcohol cue contexts and discrete cues in binge and non-binge drinkers. Addict. Biol. 2018, 24, 1–14. [Google Scholar] [CrossRef]
- Hartwell, E.E. Alcohol Craving: Clinical, Assessment, and Genetic Considerations; University of California: Los Angeles, CA, USA, 2018. [Google Scholar]
- Kavanagh, D.J.; Statham, D.J.; Feeney, G.F.X.; Young, R.M.D.; May, J.; Andrade, J.; Connor, J.P. Measurement of alcohol craving. Addict. Behav. 2013, 38, 1572–1584. [Google Scholar] [CrossRef]
- Szeto, E.H.; Schoenmakers, T.M.; van de Mheen, D.; Snelleman, M.; Waters, A.J. Associations between dispositional mindfulness, craving, and drinking in alcohol-dependent patients: An ecological momentary assessment study. Psychol. Addict. Behav. 2019, 33, 431–441. [Google Scholar] [CrossRef]
- Dulin, P.L.; Gonzalez, V.M. Smartphone-based, momentary intervention for alcohol cravings amongst individuals with an alcohol use disorder. Psychol. Addict. Behav. 2017, 31, 601–607. [Google Scholar] [CrossRef]
- Son, J.H.; Lee, S.H.; Seok, J.W.; Kee, B.S.; Lee, H.W.; Kim, H.J. Virtual reality therapy for the treatment of alcohol dependence: A preliminary investigation with positron emission tomography/computerized tomography. J. Stud. Alcohol Drugs 2015, 76, 620–627. [Google Scholar] [CrossRef]
- Witkiewitz, K.; Bowen, S.; Donovan, D.M. Moderating effects of a craving intervention on the relation between negative mood and heavy drinking following treatment for alcohol dependence. J. Consult. Clin. Psychol. 2011, 79, 54–63. [Google Scholar] [CrossRef]
- Bowen, S.; Chawla, N.; Collins, S.E.; Witkiewitz, K.; Hsu, S.; Grow, J.; Clifasefi, S.; Garner, M.; Douglass, A.; Larimer, M.E.; et al. Mindfulness-based relapse prevention for substance use disorders: A pilot efficacy trial. Subst. Abus. 2009, 30, 295–305. [Google Scholar] [CrossRef]
- Boswell, R.G.; Kober, H. Food cue reactivity and craving predict eating and weight gain: A meta-analytic review. Obes. Rev. 2016, 17, 159–177. [Google Scholar] [CrossRef]
- Drummond, D.C. What does cue-reactivity have to offer clinical research? Addiction 2000, 95, 124–144. [Google Scholar] [CrossRef] [PubMed]
- Mellentin, A.I.; Skøt, L.; Nielsen, B.; Schippers, G.M.; Nielsen, A.S. Cue exposure therapy for the treatment of alcohol use disorders: A meta-analytic review. Clin. Psychol. Rev. 2017, 57, 195–207. [Google Scholar] [CrossRef] [PubMed]
- Pavlov, I.P. Conditioned reflexes: An investigation of the physiological activity of the cerebral cortex. Ann. Neurosci. 1927, 17, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Mahlberg, J.; Weidemann, G.; Hogarth, L.; Moustafa, A.A. Cue-elicited craving and human Pavlovian-to-instrumental transfer. Addict. Res. Theory. 2019, 27, 482–488. [Google Scholar] [CrossRef]
- Ghita, A.; Hernández-Serrano, O.; Fernández-Ruiz, Y.; Monras, M.; Ortega, L.; Mondon, S.; Teixidor, L.; Gual, A.; Porras-García, B.; Ferrer-García, M.; et al. Cue-elicited anxiety and alcohol craving as indicators of the validity of ALCO-VR software: A Virtual Reality study. J. Clin. Med. 2019, 8, 1153. [Google Scholar] [CrossRef]
- Papachristou, H.; Nederkoorn, C.; Corstjens, J.; Jansen, A. The role of impulsivity and perceived availability on cue-elicited craving for alcohol in social drinkers. J. Psychopharmacol. 2012, 224, 145–153. [Google Scholar] [CrossRef][Green Version]
- Zhornitsky, S.; Zhang, S.; Ide, J.S.; Chao, H.H.; Wang, W.; Le, T.M.; Leeman, R.F.; Bi, G.; Krystal, J.H.; Li, C.-S.R. Alcohol expectancy and cerebral responses to cue-elicited craving in adult nondependent drinkers. Biol. Psychiatry Cogn. Neurosci. 2019, 4, 493–504. [Google Scholar] [CrossRef]
- Mellentin, A.I.; Nielsen, B.; Nielsen, A.S.; Yu, F.; Stenager, E. A randomized controlled study of exposure therapy as aftercare for alcohol use disorder: Study protocol. BMC Psychiatry 2016, 16, 112–120. [Google Scholar] [CrossRef]
- Vollstädt-Klein, S.; Loeber, S.; Kirsch, M.; Bach, P.; Richter, A.; Bhler, M.; von der Goltz, C.; Hermann, D.; Mann, K.; Kiefer, F. Effects of cue-exposure treatment on neural cue reactivity in alcohol dependence: A randomized trial. Biol. Psychiatry 2011, 69, 1160–1176. [Google Scholar] [CrossRef]
- Mellentin, A.I.; Stenager, E.; Nielsen, B.; Nielsen, A.S.; Yu, F. A smarter pathway for delivering cue exposure therapy? The design and development of a smartphone app targeting alcohol use disorder. JMIR mHealth uHealth 2017, 5, 1–12. [Google Scholar] [CrossRef]
- Martin, T.; Larowe, S.D.; Malcolm, R. Progress in cue exposure therapy for the treatment of addictive disorders: A review update. Open Addict. J. 2010, 3, 92–101. [Google Scholar] [CrossRef]
- Conklin, C.A.; Tiffany, S.T. Applying extinction research and theory to cue-exposure addiction treatments. Addiction 2002, 97, 155–167. [Google Scholar] [CrossRef]
- Ghiţă, A.; Gutiérrez-Maldonado, J. Applications of virtual reality in individuals with alcohol misuse: A systematic review. Addict. Behav. 2018, 81, 1–11. [Google Scholar] [CrossRef]
- Segawa, T.; Baudry, T.; Bourla, A.; Blanc, J.V.; Peretti, C.S.; Mouchabac, S.; Ferreri, F. Virtual reality (VR) in assessment and treatment of addictive disorders: A systematic review. Front. Neurosci. 2019, 13, 1409–1423. [Google Scholar] [CrossRef]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat. Rev. Neurosci. 2011, 12, 752–762. [Google Scholar] [CrossRef]
- Gutiérrez-Maldonado, J.; Ferrer-García, M.; Dakanalis, A.; Riva, G. Virtual Reality: Applications to eating disorders. Oxford Hand Eat Disor. 2018, 470–491. [Google Scholar]
- Iachini, T.; Maffei, L.; Masullo, M.; Senese, V.P.; Rapuano, M.; Pascale, A.; Sorrentino, F.; Ruggiero, G. The experience of virtual reality: Are individual differences in mental imagery associated with sense of presence? Cogn. Process. 2019, 20, 291–298. [Google Scholar] [CrossRef]
- Riva, G. Virtual reality: An experiential tool for clinical psychology. Br. J. Guid. Counc. 2009, 37, 335–343. [Google Scholar] [CrossRef]
- Lee, J.; Kim, M.; Kim, J. A study on immersion and VR sickness in walking interaction for immersive virtual reality applications. Symmetry 2017, 9, 78–95. [Google Scholar]
- Bordnick, P.S.; Traylor, A.; Copp, H.L.; Graap, K.M.; Carter, B.; Ferrer, M.; Waton, A.P. Assessing reactivity to virtual reality alcohol based cues. Addict. Behav. 2008, 33, 743–756. [Google Scholar] [CrossRef]
- Culbertson, C.; Nicolas, S.; Zaharovits, I.; London, E.D.; Garza, R.; Brody, A.L.; Newton, T.F. Methamphetamine craving induced in an online virtual reality environment. Pharmacol. Biochem. Behav. 2010, 96, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Saladin, M.E.; Brady, K.T.; Graap, K.; Rothbaum, B.O. A preliminary report on the use of virtual reality technology to elicit craving and cue reactivity in cocaine dependent individuals. Addict. Behav. 2006, 31, 1881–1894. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, S.B. Perceived realism of virtual environments depends on authenticity. Presence Teleoper. Virtual Environ. 2016, 24, 322–324. [Google Scholar] [CrossRef]
- Freeman, D.; Reeve, S.; Robinson, A.; Ehlers, A.; Clark, D.; Spanlang, B.; Slater, M. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 2017, 47, 2393–2400. [Google Scholar] [CrossRef] [PubMed]
- Papachristou, H.; Nederkoorn, C.; Havermans, R.; Bongers, P.; Beunen, S.; Jansen, A. Higher levels of trait impulsiveness and a less effective response inhibition are linked to more intense cue-elicited craving for alcohol in alcohol-dependent patients. Psychopharmacology 2013, 228, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Doran, N. Sex differences in smoking cue reactivity: Craving, negative affect, and preference for immediate smoking. Am. J. Addict. 2013, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lundahl, L.H.; Johanson, C.E. Cue-induced craving for marijuana in cannabis-dependent adults. Exp. Clin. Psychopharmacol. 2011, 19, 224–230. [Google Scholar] [CrossRef]
- Yarmush, D.E.; Manchery, L.; Luehring-Jones, P.; Erblich, J. Gender and impulsivity: Effects on cue-induced alcohol craving. Alcohol. Clin. Exp. Res. 2016, 40, 1052–1067. [Google Scholar] [CrossRef]
- Tolliver, B.K.; McRae-Clark, A.L.; Saladin, M.; Price, K.L.; Simpson, A.N.; Desantis, S.M.; Baker, N.L.; Brady, K.T. Determinants of cue-elicited craving and physiologic reactivity in methamphetamine-dependent subjects in the laboratory. Am. J. Drug Alcohol Abuse 2010, 36, 106–113. [Google Scholar] [CrossRef]
- Higley, A.E.; Crane, N.A.; Spadoni, A.D.; Quello, S.B.; Goodell, V.; Mason, B.J. Craving in response to stress induction in a human laboratory paradigm predicts treatment outcome in alcohol-dependent individuals. Psychopharmacology 2011, 218, 121–129. [Google Scholar] [CrossRef]
- MacKillop, J.; Miranda, R.; Monti, P.M.; Ray, L.A.; Murphy, J.G.; Rohsenow, D.J.; McGeary, J.E.; Swift, R.M.; Tidey, J.W.; Gwaltney, C.J. Alcohol demand, delayed reward discounting, and craving in relation to drinking and alcohol use disorders. J. Abnorm. Psychol. 2010, 119, 106–114. [Google Scholar] [CrossRef]
- Petit, G.; Cimochowska, A.; Cevallos, C.; Cheron, G.; Kornreich, C.; Hanak, C.; Schroder, E.; Verbanck, P.; Campanella, S. Reduced processing of alcohol cues predicts abstinence in recently detoxified alcoholic patients in a three-month follow up period: An ERP study. Behav. Brain Res. 2015, 282, 84–94. [Google Scholar] [CrossRef]
- Breese, G.R.; Sinha, R.; Heilig, M. Chronic alcohol neuroadaptation and stress contribute to susceptibility for alcohol craving and relapse. Pharmacol. Therapeut. 2011, 129, 149–171. [Google Scholar] [CrossRef]
- Brière, F.N.; Rohde, P.; Seeley, J.R.; Klein, D.; Lewinsohn, P.M. Comorbidity between major depression and alcohol use disorder from adolescence to adulthood. Compr. Psychiatry 2014, 55, 526–533. [Google Scholar] [CrossRef]
- Tragesser, S.L.; Trull, T.J.; Sher, K.J.; Park, A. Drinking motives ad mediators in the relation between personality disorder symptoms and alcohol use disorder. J. Pers. Disord 2008, 22, 525–537. [Google Scholar] [CrossRef]
- Franko, D.L.; Dorer, D.J.; Keel, P.K.; Jackson, S.; Manzo, M.P.; Herzog, D.B. How do eating disorders and alcohol use disorder influence each other? Int. J. Eat Disord. 2005, 38, 200–207. [Google Scholar] [CrossRef]
- Saha, T.D.; Grant, B.F.; Chou, S.P.; Kerridge, B.T.; Pickering, R.P.; Ruan, W.J. Concurrent use of alcohol with other drugs and DSM-5 alcohol use disorder comorbid with other drug use disorders: Sociodemographic characteristics, severity, and psychopathology. Drug Alcohol Depend. 2018, 187, 261–269. [Google Scholar] [CrossRef]
- Field, M.; Cox, W.M. Attentional bias in addictive behaviors: A review of its development, causes, and consequences. Drug Alcohol Depend. 2008, 97, 1–20. [Google Scholar] [CrossRef]
- Simon, J.; Etienne, A.M.; Bouchard, S.; Quertemont, E. Alcohol craving in heavy and occasional alcohol drinkers after cue exposure in a virtual environment: The role of the sense of presence. Front. Hum. Neurosci. 2020, 124, 1–9. [Google Scholar] [CrossRef]
- Ferrer-García, M.; García-Rodríguez, O.; Gutiérrez-Maldonado, J.; Pericot-Valverde, I.; Secades-Villa, R. Efficacy of Virtual Reality in triggering the craving to smoke: Its relation to level of presence and nicotine dependence. Annu. Rev. Cybertherapy Telemed. 2010, 8, 99–106. [Google Scholar]
- Du Sert, O.P.; Potvin, S.; Lipp, O.; Dellazizzo, L.; Laurelli, M.; Breton, R.; Lalonde, P.; Phraxayavong, K.; O′Connor, K.; Pelletier, J.-F.; et al. Virtual reality therapy for refractory auditory verbal hallucinations in schizophrenia: A pilot clinical trial. Schizophr. Res. 2019, 197, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, S.; Robillard, G.; Giroux, I.; Jacques, C.; Loranger, C.; St-Pierre, M.; Chrétien, M.; Goulet, A. Using virtual reality in the treatment of gambling disorder: The development of a new tool for cognitive behavior therapy. Front. Psychiatry. 2017, 8, 1–10. [Google Scholar] [CrossRef]
- Diemer, J.; Lohkamp, N.; Mühlberger, A.; Zwanzger, P. Fear and physiological arousal during a virtual height challenge—effects in patients with acrophobia and healthy controls. J. Anxiety Disord 2016, 37, 30–39. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Contel Guillamón, M.; Gual Solé, A.; Colom Farran, J. Test para la identificación de trastornos por uso de alcohol (AUDIT): Traducción y validación del AUDIT al catalán y castellano. Adicciones 1999, 11, 337–347. [Google Scholar] [CrossRef]
- Donovan, D.M.; Kivlahan, D.R.; Doyle, S.R.; Longabaugh, R.; Greenfield, S.F. Concurrent validity of the Alcohol Use Disorders Identification Test (AUDIT) and AUDIT zones in defining levels of severity among out-patients with alcohol dependence in the COMBINE study. Addiction 2006, 101, 1696–1704. [Google Scholar] [CrossRef] [PubMed]
- Guardia Serecigni, J.; Segura García, L.; Gonzalvo Cirac, B.; Trujols Albet, J.; Tejero Pociello, A.; Suárez González, A.; Martí Gil, A. Estudio de validación de la Escala Multidimensional de Craving de Alcohol. Med. Clin. 2004, 123, 211–216. [Google Scholar] [CrossRef]
- Sánchez-López, A.; Quinto-Guillen, R.; Pérez-Lucas, J.; Jurado-Barba, R.; Martínez-Grass, I.; Ponce-Alfaro, G.; Rubio-Valladolid, G. Validación de la versión española del Test Stroop de Alcohol. An. Psicol. 2015, 31, 504–523. [Google Scholar]
- Spielberger, C.D.; Gonzalez-Reigosa, F.; Martinez-Urrutia, A.; Natalicio, L.F.S.; Natalicio, D.S. Development of the Spanish Edition of the State-Trait Anxiety Inventory. Interam. J. Psychol. 1971, 145–158. [Google Scholar]
- Ghiţă, A.; Teixidor, L.; Monras, M.; Ortega, L.; Mondon, S.; Gual, A.; Paredes, S.M.; Urgell, L.V.; Porras-García, B.; Ferrer-García, M.; et al. Identifying triggers of alcohol craving to develop effective virtual environments for cue exposure therapy. Front. Psychol. 2019, 10, 1–11. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guildford Publications: New York, NY, USA, 2017. [Google Scholar]
- Yoon, G.; Kim, S.W.; Thuras, P.; Grant, J.E.; Westermeyer, J. Alcohol craving in outpatients with alcohol dependence: Rate and clinical correlates. J. Stud. Alcohol Drugs 2006, 67, 770–777. [Google Scholar] [CrossRef]
- Wapp, M.; Burren, Y.; Znoj, H.; Moggi, F. Association of alcohol craving and proximal outcomes of a residential treatment program for patients with alcohol use disorders. J. Subst. Use 2015, 20, 11–15. [Google Scholar] [CrossRef]
- Shiyko, M.; Naab, P.; Shiffman, S.; Li, R. Modeling complexity of EMA data: Time-varying lagged effects of negative affect on smoking urges for subgroups of nicotine addiction. Nicotine Tob. Res. 2014, 16, 144–150. [Google Scholar] [CrossRef]
- Piasecki, T.M.; Jahng, S.; Wood, P.K.; Robertson, B.M.; Epler, A.J.; Cronk, N.J.; Rohrbaugh, J.W.; Heath, A.C.; Shiffman, S.; Sher, K.J. The subjective effects of alcohol-tobacco co-use: An ecological momentary assessment investigation. J. Abnorm. Psychol. 2011, 120, 557–571. [Google Scholar] [CrossRef]
- Carter, B.L.; Tiffany, S.T. Meta-analysis of cue-reactivity in addiction research. Addiction 1999, 94, 327–340. [Google Scholar] [CrossRef]
- Munyan, B.C.; Neer, S.M.; Beidel, D.C.; Jentsch, F. Olfactory stimuli increase presence in virtual environments. PLoS ONE 2016, 11, e0157568. [Google Scholar] [CrossRef]
- Conklin, C.A.; Robin, N.; Perkins, K.A.; Salkeld, R.P.; McClernon, F.J. Proximal versus distal cues to smoke: The effects of environments on smokers’ cue-reactivity. Exp. Clin. Psychopharmacol. 2008, 16, 207–214. [Google Scholar] [CrossRef]
- Zhao, X.; Lynch, J.G.; Chen, Q. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Meule, A. Contemporary understanding of mediation testing. Meta-Psychology 2019, 3, 1–7. [Google Scholar] [CrossRef]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef]
- Buckingham, D.; Willett, R. Digital Generations: Children, Young People, and the New Media; Routledge: New York, NY, USA, 2013. [Google Scholar]
- García Peñalvo, F.J.; Gonçalvez Estella, J.M.; Sánchez Ledesma, M.J.; Ruisoto Palomera, P. Virtual Reality as an educational and training tool for medicine. J. Med. Syst. 2018, 42, 1–5. [Google Scholar]
- Kothgassner, O.D.; Goreis, A.; Kafka, J.X.; Hlavacs, H.; Beutl, L.; Kryspin-Exner, I.; Felnhofer, A. Agency and gender influence older adults’ presence-related experiences in an interactive virtual environment. Cyberpsychol Behav. Soc. Netw. 2018, 21, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Zibrek, K.; Kokkinara, E.; McDonnell, R. The effect of realistic appearance of virtual characters in immersive environments-Does the character’s personality play a role? IEEE Transactions on Visualization and Computer Graphics. IEEE Comput. Soc. 2018, 24, 1681–1690. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Sample |
|---|---|
| N (%) | |
| Gender | |
| Female | 32 (44.4%) |
| Male | 40 (55.6%) |
| Psychiatric comorbidity (presence) | |
| Yes | 33 (45.8%) |
| No | 39 (54.2%) |
| Current smoker | |
| Yes | 35 (48.6%) |
| No | 34 (47.2%) |
| Illicit drug use in the month prior to baseline | |
| Yes | 21 (29.2%) |
| No | 50 (69.4%) |
| Education | |
| Elementary | 0 (0.0%) |
| High school | 25 (34.7%) |
| Junior college associate degree | 12 (16.7%) |
| University | 30 (41.7%) |
| Master’s degree | 4 (5.6%) |
| Doctoral studies | 1 (1.4%) |
| Socioeconomic status | |
| Low | 11 (15.3%) |
| Medium | 58 (80.6%) |
| High | 2 (2.8%) |
| Civil status | |
| Single | 11 (15.3%) |
| Married/in a relationship | 33 (45.8%) |
| Separated/divorced | 21 (29.2%) |
| Widower | 6 (8.3%) |
| M (SD) | |
| Age | 52.17 (8.83) |
| AUDIT | 15.94 (10.28) |
| Abstinence duration (days) | 90.83 (110.77) |
| STAI-trait | 27.13 (11.85) |
| Stroop Task | 33.96 (155.92) |
| MACS | 24.15 (7.90) |
| Characteristics | MACS-VR | PR of Environments | PR of Beverages | |||
|---|---|---|---|---|---|---|
| M (SD) | t (p) | M (SD) | t (p) | M (SD) | t (p) | |
| Gender | −1.552 (0.125) | −0.257 (0.798) | −0.919 (0.361) | |||
| Female | 30.50 (13.86) | 7.96 (1.78) | 7.18 (2.45) | |||
| Male | 25.77 (11.95) | 7.86 (1.70) | 6.72 (1.81) | |||
| Psychiatric comorbidity | −0.564 (0.575) | −1.098 (0.276) | −0.635 (0.528) | |||
| Yes | 23.39 (9.84) | 7.66 (1.89) | 6.75 (2.27) | |||
| No | 24.79 (11.02) | 8.11 (1.57) | 7.07 (1.99) | |||
| Current smoker | 0.235 (0.815) | 0.860 (393) | 1.316 (0.193) | |||
| Yes | 27.91 (14.05) | 8.08 (1.68) | 7.20 (2.36) | |||
| No | 27.17 (11.96) | 7.72 (1.83) | 6.52 (1.82) | |||
| Illicit drug use in the month prior to baseline | 3.340 (0.831) | 998. (321) | −0.357 (0.722) | |||
| Yes | 35.42 (12.50) | 7.16 (1.91) | 6.76 (2.27) | |||
| No | 24.86 (12.03) | 8.22 (1.58) | 6.96 (2.06) | |||
| M (SD) | F (p) | M (SD) | F (p) | M (SD) | F (p) | |
| Education | 0.997 (0.427) | 3.406 (0.008) * | 1.837 (0.118) | |||
| Elementary | 24.30 (12.34) | 8.60 (1.34) | 6.30 (2.31) | |||
| High School | 33.13 (15.72) | 8.77 (1.48) | 7.86 (1.64) | |||
| Junior college associate degree | 30.41 (14.58) | 7.58 (1.16) | 7.16 (1.33) | |||
| University | 25.30 (11.07) | 7.58 (1.89) | 6.86 (2.30) | |||
| Master’s degree | 29.50 (11.03) | 7.75 (0.95) | 5.75 (2.62) | |||
| Doctoral studies | 25.00 (NA) | 3.00 (NA) | 3.00 (NA) | |||
| Socioeconomic status | 0.318 (0.729) | 1.295 (0.281) | 1.337 (0.270) | |||
| Low | 30.63 (14.65) | 8.09 (1.22) | 7.00 (2.19) | |||
| Medium | 27.60 (12.94) | 7.95 (1.81) | 6.98 (2.10) | |||
| High | 24.50 (7.77) | 6.00 (1.41) | 4.50 (2.12) | |||
| Civil status | 0.2694 (0.049) * | 1.826 (0.151) | 0.719 (0.544) | |||
| Single | 33.09 (11.60) | 7.00 (2.09) | 6.63 (2.01) | |||
| Married/in a relationship | 25.21 (12.56) | 8.34 (1.47) | 7.03 (2.22) | |||
| Separated/divorced | 32.00 (13.92) | 7.80 (1.83) | 7.19 (2.29) | |||
| Widower | 19.83 (7.88) | 7.66 (1.75) | 5.83 (0.75) | |||
| r (p) | r (p) | r (p) | ||||
| Age | −0.229 (0.048) * | 0.228 (0.049) * | 0.015 (0.901) | |||
| AUDIT | 0.455 (<0.001) * | 0.062 (0.604) | 0.259 (0.028) * | |||
| Abstinence duration (days) | −0.132 (0.269) | 0.087 (0.467) | 0.010 (0.931) | |||
| STAI-trait | 0.367 (0.002) * | −0.069 (0.566) | 0.074 (0.537) | |||
| Stroop Task | −0.119 (0.320) | 0.076 (0.526) | 0.071 (0.555) | |||
| MACS | NA | −0.009 (0.940) | 0.128 (0.283) | |||
| M (SD) | r (p) | |||
|---|---|---|---|---|
| Characteristics | Total Sample | MACS-VR | PR of Environments | PR of Beverages |
| MACS-VR | 27.87 (12.96) | NA | 0.149 (0.213) | 0.362 (0.002) * |
| PR of environments | 7.90 (1.73) | 0.149 (0.213) | NA | 0.578 (<0.001) * |
| PR of beverages | 6.93 (2.11) | 0.362 (0.002) * | 0.578 (<0.001) * | NA |
| MACS-VR | B | SE B | β | t | p Value |
| Civil status | −0.010 | 1.702 | −0.001 | −0.006 | 0.996 |
| Age | −0.124 | 0.171 | −0.083 | −0.723 | 0.472 |
| AUDIT | 0.344 | 0.160 | 0.273 | 2.154 | 0.035 * |
| STAI-trait | 0.192 | 0.135 | 0.176 | 1.426 | 0.159 |
| PR of beverages | 1.741 | 0.655 | 0.285 | 2.660 | 0.010 * |
| PR of Environments | B | SE B | β | t | p Value |
| Education level | −0.336 | 0.129 | −0.241 | −2.603 | 0.011 * |
| Age | 0.036 | 0.018 | 0.184 | 1.999 | 0.049 * |
| PR of beverages | 0.444 | 0.075 | 0.544 | 5.933 | <0.001 * |
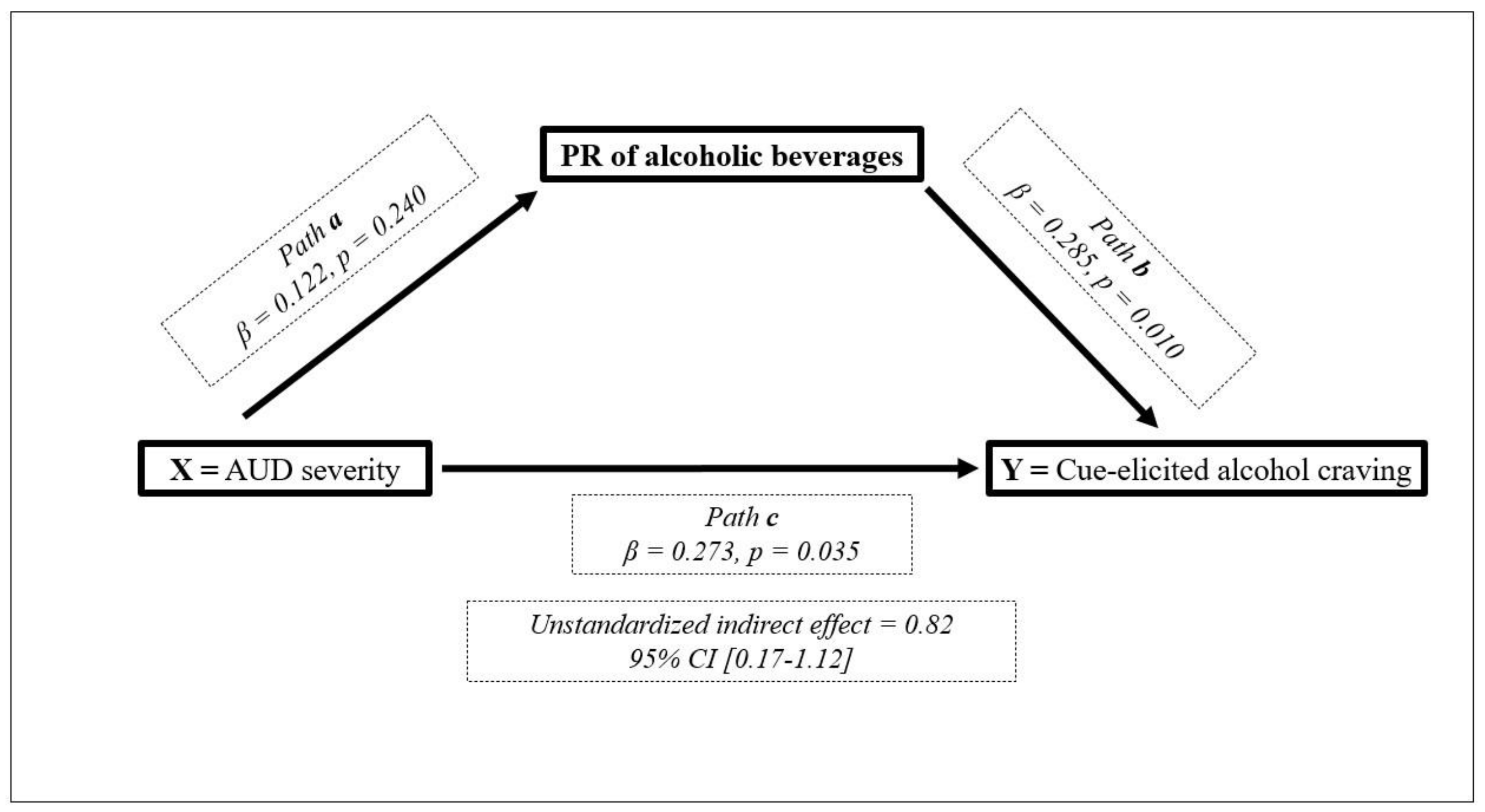
| PR of Alcoholic Beverages | B | SE B | β | t | p Value |
| MACS-VR | 0.037 | 0.017 | 0.227 | 2.174 | 0.033 * |
| AUDIT | 0.025 | 0.021 | 0.122 | 1.185 | 0.240 |
| PR of environments | 0.657 | 0.114 | 0.537 | 5.772 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Serrano, O.; Ghiţă, A.; Fernández-Ruiz, J.; Monràs, M.; Gual, A.; Gacto, M.; Porras-García, B.; Ferrer-García, M.; Gutiérrez-Maldonado, J. Determinants of Cue-Elicited Alcohol Craving and Perceived Realism in Virtual Reality Environments among Patients with Alcohol Use Disorder. J. Clin. Med. 2021, 10, 2241. https://doi.org/10.3390/jcm10112241
Hernández-Serrano O, Ghiţă A, Fernández-Ruiz J, Monràs M, Gual A, Gacto M, Porras-García B, Ferrer-García M, Gutiérrez-Maldonado J. Determinants of Cue-Elicited Alcohol Craving and Perceived Realism in Virtual Reality Environments among Patients with Alcohol Use Disorder. Journal of Clinical Medicine. 2021; 10(11):2241. https://doi.org/10.3390/jcm10112241
Chicago/Turabian StyleHernández-Serrano, Olga, Alexandra Ghiţă, Jolanda Fernández-Ruiz, Miquel Monràs, Antoni Gual, Mariano Gacto, Bruno Porras-García, Marta Ferrer-García, and José Gutiérrez-Maldonado. 2021. "Determinants of Cue-Elicited Alcohol Craving and Perceived Realism in Virtual Reality Environments among Patients with Alcohol Use Disorder" Journal of Clinical Medicine 10, no. 11: 2241. https://doi.org/10.3390/jcm10112241
APA StyleHernández-Serrano, O., Ghiţă, A., Fernández-Ruiz, J., Monràs, M., Gual, A., Gacto, M., Porras-García, B., Ferrer-García, M., & Gutiérrez-Maldonado, J. (2021). Determinants of Cue-Elicited Alcohol Craving and Perceived Realism in Virtual Reality Environments among Patients with Alcohol Use Disorder. Journal of Clinical Medicine, 10(11), 2241. https://doi.org/10.3390/jcm10112241