
Antibody Response after 3-Dose Booster against SARS-CoV-2 mRNA Vaccine in Kidney Transplant Recipients

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Analytical Methods
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, C.; Maruggi, G.; Shan, H.; Li, J. Advances in mRNA Vaccines for Infectious Diseases. Front. Immunol. 2019, 10, 594. [Google Scholar] [CrossRef] [PubMed]
- Moreira, E.D., Jr.; Kitchin, N.; Xu, X.; Dychter, S.S.; Lockhart, S.; Gurtman, A.; Perez, J.L.; Zerbini, C.; Dever, M.E.; Jennings, T.W.; et al. Safety and Efficacy of a Third Dose of BNT162b2 Covid-19 Vaccine. N. Engl. J. Med. 2022, 386, 1910–1921. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.; Foulkes, S.; Insalata, F.; Kirwan, P.; Sai, A.; Atti, A.; Wellington, E.; Khawam, J.; Munro, K.; Cole, M.; et al. Protection against SARS-CoV-2 after Covid-19 Vaccination and Previous Infection. N. Engl. J. Med. 2022, 386, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Angelico, R.; Blasi, F.; Manzia, T.M.; Toti, L.; Tisone, G.; Cacciola, R. The Management of Immunosuppression in Kidney Transplant Recipients with COVID-19 Disease: An Update and Systematic Review of the Literature. Medicina 2021, 57, 435. [Google Scholar] [CrossRef] [PubMed]
- Howard, R.J.; Patton, P.R.; Reed, A.I.; Hemming, A.W.; Van der Werf, W.J.; Pfaff, W.W.; Srinivas, T.R.; Scornik, J.C. The changing causes of graft loss and death after kidney transplantation. Transplantation 2002, 73, 1923–1928. [Google Scholar] [CrossRef] [PubMed]
- Rincon-Arevalo, H.; Choi, M.; Stefanski, A.-L.; Halleck, F.; Weber, U.; Szelinski, F.; Jahrsdörfer, B.; Schrezenmeier, H.; Ludwig, C.; Sattler, A.; et al. Impaired humoral immunity to SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients and dialysis patients. Sci. Immunol. 2021, 6, eabj1031. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, J.; Schwöbel, J.; Lindner, T.; Anders, L.; Siepmann, T.; Karger, C.; Hüther, J.; Martin, H.; Müller, P.; Faulhaber-Walter, R.; et al. Risk of strong antibody decline in dialysis and transplant patients after SARS-CoV-2mRNA vaccination: Six months data from the observational Dia-Vacc study. Lancet Reg. Health Eur. 2022, 17, 100371. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health Eur. 2021, 9, 100178. [Google Scholar] [CrossRef] [PubMed]
- Caillard, S.; Chavarot, N.; Bertrand, D.; Kamar, N.; Thaunat, O.; Moal, V.; Masset, C.; Hazzan, M.; Gatault, P.; Sicard, A.; et al. Occurrence of severe COVID-19 in vaccinated transplant patients. Kidney Int. 2021, 100, 477–479. [Google Scholar] [CrossRef] [PubMed]
- Pang, N.Y.-L.; Pang, A.S.-R.; Chow, V.T.; Wang, D.-Y. Understanding neutralising antibodies against SARS-CoV-2 and their implications in clinical practice. Mil. Med. Res. 2021, 8, 47. [Google Scholar] [CrossRef] [PubMed]
- Błaszczuk, A.; Michalski, A.; Malm, M.; Drop, B.; Polz-Dacewicz, M. Antibodies to NCP, RBD and S2 SARS-CoV-2 in Vaccinated and Unvaccinated Healthcare Workers. Vaccines 2022, 10, 1169. [Google Scholar] [CrossRef] [PubMed]
- La Milia, V.; Tonolo, S.; Luzzaro, F.; Bonato, C.; Casartelli, D.; Limardo, M.; Longhi, S.; Ravasi, C.; Viganò, S.; Cavalli, A. Humoral and T-cell response to SARS-CoV-2 mRNA BNT162b2 vaccination in a cohort of kidney transplant recipients and their cohabitant living kidney donor partners. Clin. Kidney J. 2022, 15, 820–821. [Google Scholar] [CrossRef] [PubMed]
- Dimeglio, C.; Herin, F.; Martin-Blondel, G.; Miedougé, M.; Izopet, J. Antibody titers and protection against a SARS-CoV-2 infection. J. Infect. 2022, 84, 248–288. [Google Scholar] [CrossRef] [PubMed]
- Sulejmani, A.; Giacobone, C.; Spiti, S.; Pozzobon, C.; Dominici, R.; Mascagni, P.; Falbo, R.; Brambilla, P.; Leoni, V. Antibody response after two doses of the SARS-CoV-2 Comirnaty vaccine in a Covid-19 positive and Covid-19 negative Italian healthcare workers cohort. Scand. J. Clin. Lab. Investig. 2022, 82, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Werbel, W.A.; Boyarsky, B.J.; Ou, M.T.; Massie, A.B.; Tobian, A.A.; Garonzik-Wang, J.M.; Segev, D.L. Safety and Immunogenicity of a Third Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Case Series. Ann. Intern. Med. 2021, 174, 1330–1332. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.G.; Ferreira, V.H.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Chaparro, C.; Selzner, N.; Schiff, J.; McDonald, M.; Tomlinson, G.; et al. Randomized Trial of a Third Dose of mRNA-1273 Vaccine in Transplant Recipients. N. Engl. J. Med. 2021, 385, 1244–1246. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, D.; Hamzaoui, M.; Lemée, V.; Lamulle, J.; Hanoy, M.; Laurent, C.; Lebourg, L.; Etienne, I.; Lemoine, M.; Le Roy, F.; et al. Antibody and T Cell Response to SARS-CoV-2 Messenger RNA BNT162b2 Vaccine in Kidney Transplant Recipients and Hemodialysis Patients. J. Am. Soc. Nephrol. 2021, 32, 2147–2152. [Google Scholar] [CrossRef] [PubMed]
- Dogan, M.; Kozhaya, L.; Placek, L.; Gunter, C.; Yigit, M.; Hardy, R.; Plassmeyer, M.; Coatney, P.; Lillard, K.; Bukhari, Z.; et al. SARS-CoV-2 specific antibody and neutralization assays reveal the wide range of the humoral immune response to virus. Commun. Biol. 2021, 4, 129. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient | Gender | Age | Infection Pre 3° Dose | Infection Post 3° Dose | Immunosuppressive Therapy * | Creatinine (mg/dL) | eGFR (mL/min) |
|---|---|---|---|---|---|---|---|
| KTR1 | F | 47 | NO | YES | TAC, MMF | 1.48 | 64.4 |
| KTR2 | F | 39 | NO | NO | TAC, MMF, CORT | 1.38 | 48 |
| KTR3 | F | 78 | NO | NO | TAC, CORT | 1.63 | 29.9 |
| KTR4 | F | 71 | NO | NO | MMF, CORT, SRL | 1.04 | 54 |
| KTR5 | F | 57 | NO | NO | TAC, MMF | 1.16 | 52.2 |
| KTR6 | F | 84 | NO | NO | SRL | 0.98 | 54 |
| KTR7 | F | 64 | NO | NO | TAC, MMF | 1 | 59.5 |
| KTR8 | F | 78 | YES | YES | MMF, SRL | 1.85 | 26 |
| KTR9 | M | 63 | NO | NO | TAC, MMF | 1.49 | 49.2 |
| KTR10 | M | 47 | NO | NO | TAC, MMF, CORT | 1.89 | 42 |
| KTR11 | M | 69 | NO | NO | AZA, CYCLO | 0.82 | 90.2 |
| KTR12 | M | 73 | NO | NO | MMF, CYCLO | 1.11 | 66 |
| KTR13 | M | 75 | NO | NO | MMF, CORT | 1.95 | 33 |
| KTR14 | M | 52 | NO | NO | EVL | 1.29 | 64 |
| KTR15 | M | 68 | NO | YES | TAC, MMF, CORT | 1.12 | 68 |
| KTR16 | M | 67 | NO | NO | TAC, MMF, CORT | 3.24 | 19 |
| KTR17 | M | 59 | NO | YES | TAC, MMF, CORT | 1.62 | 46 |
| KTR18 | M | 54 | NO | NO | TAC, MMF | 1.13 | 73 |
| KTR19 | M | 59 | NO | NO | TAC, MMF, CORT | 1 | 82 |
| KTR20 | M | 73 | NO | YES | TAC, MMF, CORT | 1.25 | 57 |
| KTR21 | M | 53 | NO | NO | TAC, MMF, CORT | 1.07 | 80 |
| KTR22 | M | 62 | NO | NO | CORT, SRL, CYCLO | 2.17 | 32 |
| KTR23 | M | 74 | NO | NO | TAC, MMF | 1.32 | 55 |
| KTR24 | M | 79 | NO | NO | MMF, CORT, SRL | 1.98 | 31 |
| KTR25 | M | 38 | NO | YES | TAC, MMF, CORT | 1.3 | 70 |
| KTR26 | M | 56 | NO | NO | TAC, MMF, CORT | 2.19 | 33 |
| KTR27 | M | 70 | NO | NO | TAC, MMF | 1.52 | 46 |
| KTR28 | M | 69 | NO | YES | TAC, MMF | 1.73 | 30 |
| KTR29 | M | 76 | NO | NO | CORT, EVL, CYCLO | 1.49 | 45 |
| KTR30 | M | 59 | NO | NO | MMF, CYCLO | 1.5 | 48 |
| KTR31 | M | 57 | NO | NO | MMF, CYCLO | 2.56 | 25 |
| KTR32 | M | 64 | YES | YES | TAC, MMF | 1.43 | 52 |
| Follow-Up of Vaccination | ||
|---|---|---|
| Calculate the mean OD 450 nm of NC and then the percentage of neutralization of the sample (NS%) with the following formulation NS % = 100 – [ | ||
| % of Neutralization (Nsample%) | Neutralizing | WHO IU/mL range |
| <20% | Lower or reactive | <10 |
| 20% < NS % < 30% | Moderate | 10–100 |
| 30% < NS % < 60% | Good | 100–400 |
| 60% < NS % < 100% | Excellent | >400 |
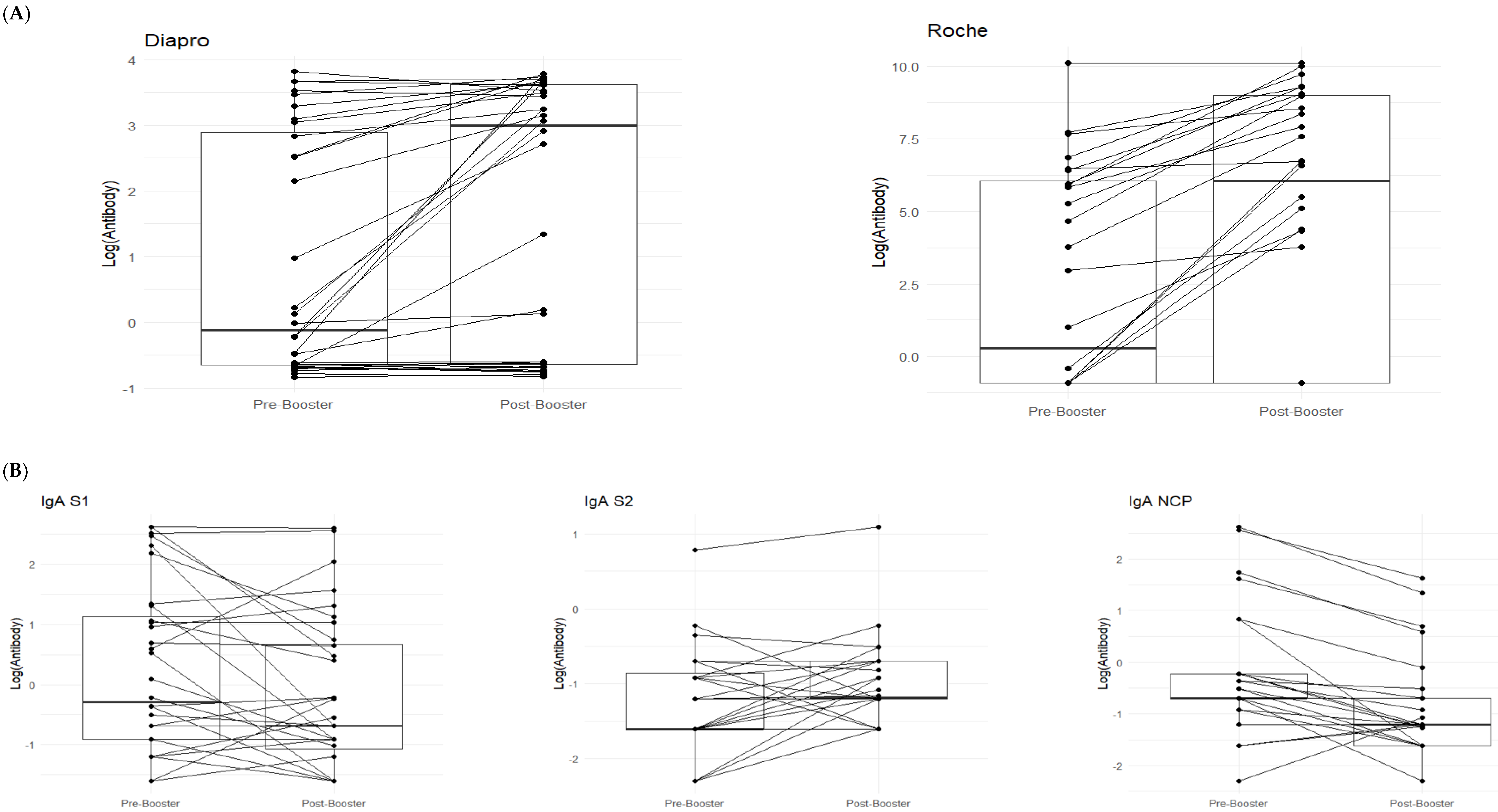
| Diapro | Pre-Booster (T0) | Post-Booster (T1) | p-Value | Roche | Pre-Booster (T0) | Post-Booster T1) | p-Value |
|---|---|---|---|---|---|---|---|
| (N = 32) | (N = 32) | (N = 32) | (N = 32) | ||||
| Mean (SD) | 10.1 (14.3) | 18.8 (17.5) | <0.001 | Mean (SD) | 2600 (7340) | 5270 (8360) | <0.001 |
| Median [Min, Max] | 0.893 [0.430, 45.7] | 20.0 [0.435, 43.8] | Median [Min, Max] | 1.70 [0.400, 25,000] | 486 [0.400, 25,000] |
| IgA | Pre-Booster | Post-Booster | p-Value | IgM | Pre-Booster | Post-Booster | p-Value | IgG | Pre-Booster | Post-Booster | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (N = 32) | (N = 32) | (N = 32) | (N = 32) | (N = 32) | (N = 32) | ||||||
| IgA S1 | IgM_S1 | IgG S1 | |||||||||
| Mean (SD) | 3.14 (4.42) | 2.00 (3.36) | 0.119 | Mean (SD) | 2.70 (4.14) | 1.68 (1.76) | 0.742 | Mean (SD) | 4.35 (5.12) | 6.37 (6.28) | 0.023 |
| Median [Min, Max] | 0.750 [0.200, 13.8] | 0.500 [0.200, 13.5] | Median [Min, Max] | 0.400 [0.100, 13.5] | 0.900 [0.100, 5.60] | Median [Min, Max] | 1.50 [0.200, 13.8] | 3.41 [0.200, 14.0] | |||
| IgA S2 | IgM S2 | IgG S2 | |||||||||
| Mean (SD) | 0.375 (0.384) | 0.450 (0.486) | 0.076 | Mean (SD) | 0.366 (0.657) | 0.450 (0.563) | 0.031 | Mean (SD) | 1.46 (2.95) | 1.25 (2.79) | 0.013 |
| Median [Min, Max] | 0.200 [0.100, 2.20] | 0.307 [0.200, 3.00] | Median [Min, Max] | 0.200 [0.100, 3.80] | 0.315 [0.100, 3.20] | Median [Min, Max] | 0.500 [0.200, 13.2] | 0.400 [0.200, 13.1] | |||
| IgA NCP | IgM NCP | IgG NCP | |||||||||
| Mean (SD) | 1.73 (3.29) | 0.669 (1.09) | <0.001 | Mean (SD) | 0.963 (1.39) | 0.502 (0.858) | <0.001 | Mean (SD) | 1.77 (3.09) | 1.74 (3.12) | 0.153 |
| Median [Min, Max] | 0.500 [0.100, 13.8] | 0.300 [0.100, 5.10] | Median [Min, Max] | 0.500 [0.120, 6.50] | 0.300 [0.100, 4.90] | Median [Min, Max] | 0.500 [0.200, 14.4] | 0.500 [0.200, 14.3] |
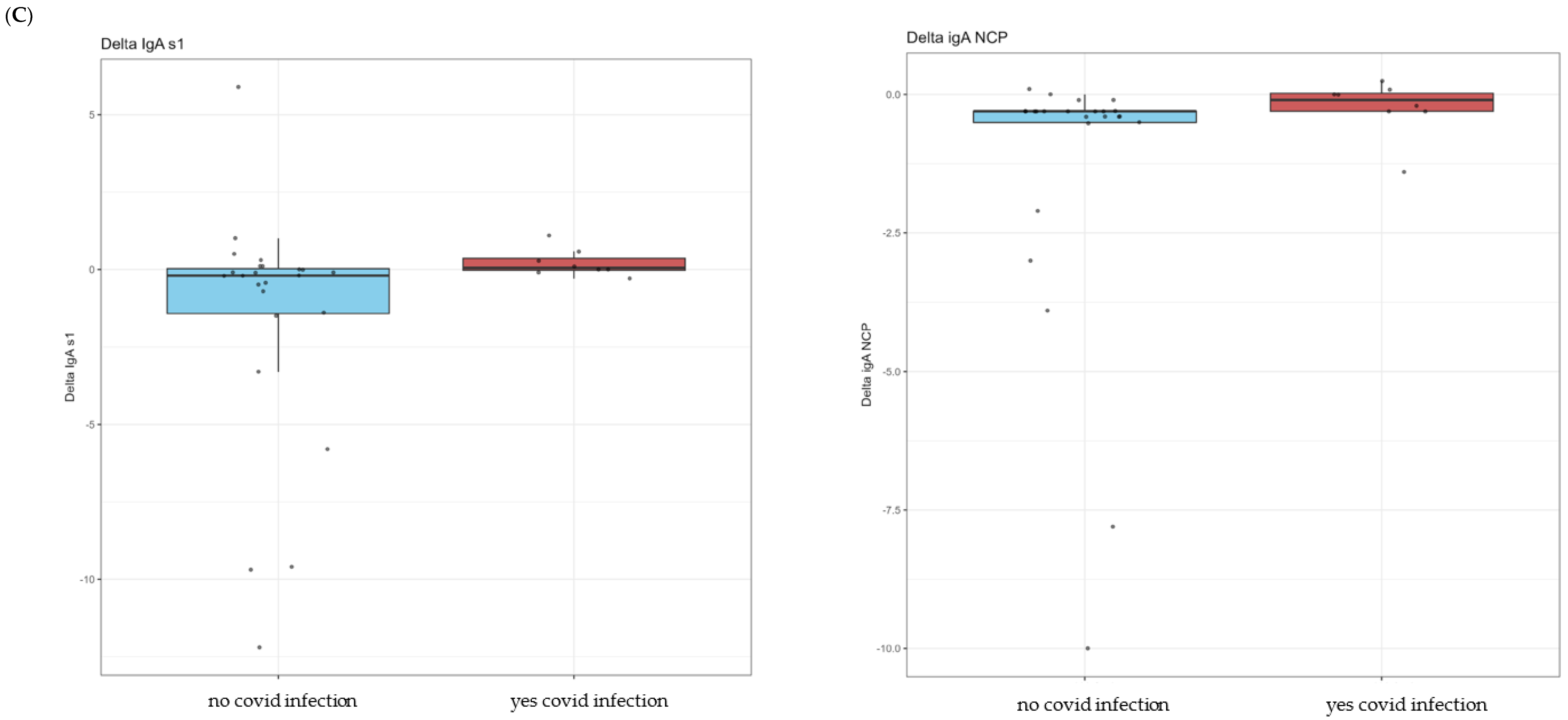
| No COVID Infection | Yes COVID Infection | p-Value | |
|---|---|---|---|
| (N = 24) | (N = 8) | ||
| Sex | |||
| F | 6 (25.0%) | 2 (25.0%) | 1 |
| M | 18 (75.0%) | 6 (75.0%) | |
| Age | |||
| Mean (SD) | 65.4 (10.9) | 58.1 (12.7) | 0.177 |
| Median [Min, Max] | 65.5 [39.0, 84.0] | 61.5 [38.0, 73.0] | |
| Creatinine | |||
| Mean (SD) | 1.54 (0.580) | 1.48 (0.258) | 0.845 |
| Median [Min, Max] | 1.44 [0.820, 3.24] | 1.46 [1.12, 1.89] | |
| eGFR | |||
| Mean (SD) | 49.8 (19.3) | 53.7 (13.9) | 0.542 |
| Median [Min, Max] | 48.6 [19.0, 90.2] | 54.5 [30.0, 70.0] | |
| N. of immunosuppressive drugs | |||
| one | 2 (8.3%) | 0 (0%) | 0.55 |
| two | 13 (54.2%) | 3 (37.5%) | |
| three | 9 (37.5%) | 5 (62.5%) | |
| Delta Diapro | |||
| Mean (SD) | 10.6 (14.3) | 2.77 (5.11) | 0.188 |
| Median [Min, Max] | 5.99 [−11.8, 43.2] | 0.0272 [−0.0485, 11.8] | |
| Delta_Roche | |||
| Mean (SD) | 2670 (4250) | 2700 (7620) | 0.088 |
| Median [Min, Max] | 218 [0, 15,600] | 0 [0, 21,600] | |
| Delta IgG S1 | |||
| Mean (SD) | 2.53 (4.23) | 0.471 (1.58) | 0.214 |
| Median [Min, Max] | 1.05 [−2.30, 12.1] | −0.100 [−0.200, 4.37] | |
| Delta IgG S2 | |||
| Mean (SD) | −0.265 (0.530) | −0.0500 (0.160) | 0.239 |
| Median [Min, Max] | −0.100 [−2.20, 0.200] | 0 [−0.400, 0.100] | |
| Delta_IgG NCP | |||
| Mean (SD) | −0.0467 (0.419) | 0.0375 (0.200) | 0.337 |
| Median [Min, Max] | −0.0500 [−0.800, 1.40] | 0 [−0.100, 0.500] | |
| Delta_IgM S1 | |||
| Mean (SD) | −1.20 (3.05) | −0.502 (3.46) | 0.326 |
| Median [Min, Max] | −0.0500 [−8.90, 2.30] | 0.250 [−8.60, 3.40] | |
| Delta_IgM S2 | |||
| Mean (SD) | 0.118 (0.275) | −0.0158 (0.260) | 0.278 |
| Median [Min, Max] | 0.100 [−0.500, 0.700] | 0.0650 [−0.600, 0.200] | |
| Delta_IgM NCP | |||
| Mean (SD) | −0.465 (0.796) | −0.449 (0.676) | 0.878 |
| Median [Min, Max] | −0.250 [−3.10, 0.300] | −0.200 [−1.50, 0.227] | |
| Delta_IgA S1 | |||
| Mean (SD) | −1.59 (3.96) | 0.208 (0.446) | 0.045 |
| Median [Min, Max] | −0.200 [−12.2, 5.90] | 0.0500 [−0.300, 1.10] | |
| Delta_IgA S2 | |||
| Mean (SD) | 0.0308 (0.241) | 0.207 (0.286) | 0.356 |
| Median [Min, Max] | 0.100 [−0.500, 0.400] | 0.100 [−0.0590, 0.800] | |
| Delta_IgA NCP | |||
| Mean (SD) | −1.34 (2.54) | −0.233 (0.509) | 0.022 |
| Median [Min, Max] | −0.300 [−10.0, 0.100] | −0.100 [−1.40, 0.245] | |
| Linear Regression Model Comparison | Nominal p-Value | Adjusted p-Value (FDR) | Beta Coefficient |
|---|---|---|---|
| IgG S1~Creatinine | 0.88 | 0.97 | −0.20 |
| IgG S2~Creatinine | 0.96 | 0.97 | −0.01 |
| IgG NCP~Creatinine | 0.49 | 0.97 | 0.09 |
| IgM S1~Creatinine | 0.77 | 0.97 | −0.13 |
| IgM S2~Creatinine | 0.97 | 0.97 | 0.00 |
| IgM NCP~Creatinine | 0.02 | 0.27 | −0.35 |
| IgA S1~Creatinine | 0.27 | 0.97 | −1.05 |
| IgA S2~Creatinine | 0.68 | 0.97 | −0.04 |
| IgA NCP~Creatinine | 0.31 | 0.97 | −0.10 |
| Roche~Creatinine | 0.73 | 0.97 | −684.87 |
| Diapro~Creatinine | 0.96 | 0.97 | −0.22 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tripodi, D.; Dominici, R.; Sacco, D.; Santorelli, G.; Rivera, R.; Acquaviva, S.; Marchisio, M.; Brambilla, P.; Battini, G.; Leoni, V. Antibody Response after 3-Dose Booster against SARS-CoV-2 mRNA Vaccine in Kidney Transplant Recipients. Vaccines 2024, 12, 264. https://doi.org/10.3390/vaccines12030264
Tripodi D, Dominici R, Sacco D, Santorelli G, Rivera R, Acquaviva S, Marchisio M, Brambilla P, Battini G, Leoni V. Antibody Response after 3-Dose Booster against SARS-CoV-2 mRNA Vaccine in Kidney Transplant Recipients. Vaccines. 2024; 12(3):264. https://doi.org/10.3390/vaccines12030264
Chicago/Turabian StyleTripodi, Domenico, Roberto Dominici, Davide Sacco, Gennaro Santorelli, Rodolfo Rivera, Sandro Acquaviva, Marino Marchisio, Paolo Brambilla, Graziana Battini, and Valerio Leoni. 2024. "Antibody Response after 3-Dose Booster against SARS-CoV-2 mRNA Vaccine in Kidney Transplant Recipients" Vaccines 12, no. 3: 264. https://doi.org/10.3390/vaccines12030264
APA StyleTripodi, D., Dominici, R., Sacco, D., Santorelli, G., Rivera, R., Acquaviva, S., Marchisio, M., Brambilla, P., Battini, G., & Leoni, V. (2024). Antibody Response after 3-Dose Booster against SARS-CoV-2 mRNA Vaccine in Kidney Transplant Recipients. Vaccines, 12(3), 264. https://doi.org/10.3390/vaccines12030264