
The National Strategies for and Challenges in Infection Prevention and Control of the Healthcare System in the Kingdom of Saudi Arabia (Review Study)


Abstract
1. Introduction
2. Organisation of the Healthcare System in KSA
3. Infection Prevention and Control in Healthcare System in KSA
4. Challenges in Hospital Infection Control in KSA
5. Hajj and Pilgrimages as a Challenge
6. The Increasing Burden of Emerging Infectious Disease
7. Limited Budget Resources
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ayed, H.B.; Yaich, S.; Trigui, M.; Jemaa, M.B.; Hmida, M.B.; Karray, R.; Kassis, M.; Mejdoub, Y.; Feki, H.; Jedidi, J. Prevalence and risk factors of health care–associated infections in a limited resources country: A cross-sectional study. Am. J. Infect. Control 2019, 47, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Abalkhail, M.S.; Alzahrany, M.S.; Alghamdi, K.A.; Alsoliman, M.A.; Alzahrani, M.A.; Almosned, B.S.; Gosadi, I.M.; Tharkar, S. Uptake of influenza vaccination, awareness and its associated barriers among medical students of a University Hospital in Central Saudi Arabia. J. Infect. Public Health 2017, 10, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Cruz, J.P.; Bashtawi, M.A. Predictors of Hand Hygiene Practice Among Saudi Nursing Students: A Cross-Sectional Self-reported study. J. Infect. Public Health 2016, 9, 485–493. [Google Scholar] [CrossRef]
- Allegranzi, B.; Gayet-Ageron, A.; Damani, N.; Bengaly, L.; McLaws, M.-L.; Moro, M.-L.; Memish, Z.; Urroz, O.; Richet, H.; Storr, J. Global implementation of WHO’s multimodal strategy for improvement of hand hygiene: A quasi-experimental study. Lancet Infect. Dis. 2013, 13, 843–851. [Google Scholar] [CrossRef]
- Kurtz, S.L. Demographic Factors Associated with Consistent Hand Hygiene Adherence among ICU Nurses. Ph.D. Thesis, Walden University, Minneapolis, MN, USA, 2017. [Google Scholar]
- Fineschi, V. Healthcare-associated infections: Antibiotic poly-therapies, antibiotic prophylaxis and appropriate policy for the risk management to fight adverse events. Curr. Pharm. Biotechnol. 2019, 20, 606–608. [Google Scholar] [CrossRef]
- Almalki, M.; FitzGerald, G.; Clark, M. Health care system in Saudi Arabia: An overview. East. Mediterr. Health J. 2011, 17, 784–793. [Google Scholar] [CrossRef]
- Ministry of Health. Health Statistical Yearbook. 2017. Available online: http://www.moh.gov.sa/en/Ministry/Statistics/book/Pages/default.aspx (accessed on 25 May 2017).
- Ministry of Health. The Basics of Tuberculosis Control in Saudi Arabia, 1st ed.; Ministry of Health: Riyadh, Saudi Arabia, 2019.
- Alkhamis, A. Health care system in Saudi Arabia: An overview. East. Mediterr. Health J. 2012, 18, 1078–1080. [Google Scholar] [CrossRef] [PubMed]
- Alkabba, A.F.; Hussein, G.M.; Albar, A.A.; Bahnassy, A.A.; Qadi, M. The major medical ethical challenges facing the public and healthcare providers in Saudi Arabia. J. Fam. Community Med. 2012, 19, 1–6. [Google Scholar] [CrossRef]
- Al-Hanawi, M.K.; Khan, S.A.; Al-Borie, H.M. Healthcare human resource development in Saudi Arabia: Emerging challenges and opportunities—A critical review. Public Health Rev. 2019, 40, 1–19. [Google Scholar] [CrossRef]
- Albejaidi, F.M. Healthcare system in Saudi Arabia: An analysis of structure, total quality management and future challenges. J. Altern. Perspect. Soc. Sci. 2010, 2, 794–818. [Google Scholar]
- Colet, P.C.; Cruz, J.P.; Cacho, G.; Al-Qubeilat, H.; Soriano, S.S.; Cruz, C.P. Perceived infection prevention climate and its predictors among nurses in Saudi Arabia. J. Nurs. Scholarsh. 2018, 50, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Ronald, A.; Memish, Z. Infectious diseases: Career preparation. J. Chemother. 2001, 13 (Suppl. 1), 50–53. [Google Scholar] [CrossRef] [PubMed]
- Assiri, A.M.; Choudhry, A.J.; Alsaleh, S.S.; Alanazi, K.H.; Alsaleh, S.S. Evaluation of infection prevention and control programmes (IPC), and assessment tools for IPC-programmes at MOH-health facilities in Saudi Arabia. Open J. Nurs. 2014, 4, 46633. [Google Scholar] [CrossRef][Green Version]
- Al-Jedai, A.; Qaisi, S.; Al-Meman, A. Pharmacy practice and the health care system in Saudi Arabia. Can. J. Hosp. Pharm. 2016, 69, 231–237. [Google Scholar] [CrossRef]
- Mazi, W.; Senok, A.C.; Al-Kahldy, S.; Abdullah, D. Implementation of the world health organization hand hygiene improvement strategy in critical care units. Antimicrob. Resist. Infect. Control 2013, 2, 15. [Google Scholar] [CrossRef]
- Haridi, H.K.; Al-Ammar, A.S.; Al-Mansour, M.I. Compliance with infection control standard precautions guidelines: A survey among dental healthcare workers in Hail Region, Saudi Arabia. J. Infect. Prev. 2016, 17, 268–276. [Google Scholar] [CrossRef]
- Rabaan, A.A.; Alhani, H.M.; Bazzi, A.M.; Al-Ahmed, S.H. Questionnaire-based analysis of infection prevention and control in healthcare facilities in Saudi Arabia in regards to Middle East Respiratory Syndrome. J. Infect. Public Health 2017, 10, 548–563. [Google Scholar] [CrossRef]
- Khan, K.; Arino, J.; Hu, W.; Raposo, P.; Sears, J.; Calderon, F.; Heidebrecht, C.; Macdonald, M.; Liauw, J.; Chan, A. Spread of a novel influenza A (H1N1) virus via global airline transportation. N. Engl. J. Med. 2009, 361, 212–214. [Google Scholar] [CrossRef]
- Azizkhan, Z. An insight into the challenges posed by communicable diseases during pilgrimage seasons. Public Health Front. 2015, 38–44. [Google Scholar] [CrossRef]
- Memish, Z.A.; Assiri, A.M.; Eldalatony, M.M.; Hathout, H.M.; Alzoman, H.; Undaya, M. Risk analysis of needle stick and sharp object injuries among health care workers in a tertiary care hospital (Saudi Arabia). J. Epidemiol. Glob. Health 2013, 3, 123–129. [Google Scholar] [CrossRef]
- Shibl, A.M.; Memish, Z.A.; Al-Kattan, K.M. Antibiotic resistance and serotype distribution of invasive pneumococcal diseases before and after introduction of pneumococcal conjugate vaccine in the Kingdom of Saudi Arabia (KSA). Vaccine 2012, 30, G32–G36. [Google Scholar] [CrossRef]
- Badahdah, A.; Alfelali, M.; Alqahtani, A.; Alsharif, S.; Barasheed, O.; Team, H. Mandatory meningococcal vaccine, and other recommended immunisations: Uptake, barriers, and facilitators among health care workers and trainees at Hajj. World J. Clin. Cases 2018, 6, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Benkouiten, S.; Charrel, R.; Belhouchat, K.; Drali, T.; Salez, N.; Nougairede, A.; Zandotti, C.; Memish, Z.A.; al Masri, M.; Gaillard, C. Circulation of respiratory viruses among pilgrims during the 2012 Hajj pilgrimage. Clin. Infect. Dis. 2013, 57, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Sampathkumar, P. Middle East respiratory syndrome: What clinicians need to know. Mayo Clin. Proc. 2014, 89, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A.; Zumla, A.; Memish, Z.A. Travel implications of emerging coronaviruses: SARS and MERS-CoV. Travel Med. Infect. Dis. 2014, 12, 422–428. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Memish, Z.A. Potential risk for drug resistance globalization at the Hajj. Clin. Microbiol. Infect. 2015, 21, 109–114. [Google Scholar] [CrossRef]
- Alomi, Y.A.; Alghamdi, S.J.; Alattyh, R.A. Strategic plan of general administration of pharmaceutical care at ministry of health in Saudi Arabia 2012–2022. J. Pharm. Pharm. Sci. 2015, 1, 1–8. [Google Scholar] [CrossRef]
- KPMG. Kingdom of Saudi Arabia Budget Report a Review of KSA 2019 Budget and Recent Economic Developments. 2018. Available online: https://home.kpmg/content/dam/kpmg/sa/pdf/2018/kingdom-of-saudi-arabia-budget-report.pdf (accessed on 21 February 2020).


{kind=link}
| Categories of Healthcare Professionals | Total Workforce | Percentage of Saudi Workforce | Percentage of Foreign Workforce |
|---|---|---|---|
| Allied Health | 98,074 | 29.5 | 71.5 |
| Personnel | |||
| Pharmacists | 185,693 | 36.7 | 63.3 |
| Nurses | 28,312 | 22.2 | 77.8 |
| Physicians | 111,861 | 74.7 | 25.3 |
| Total | 423,940 | 44.1 | 56.9 |
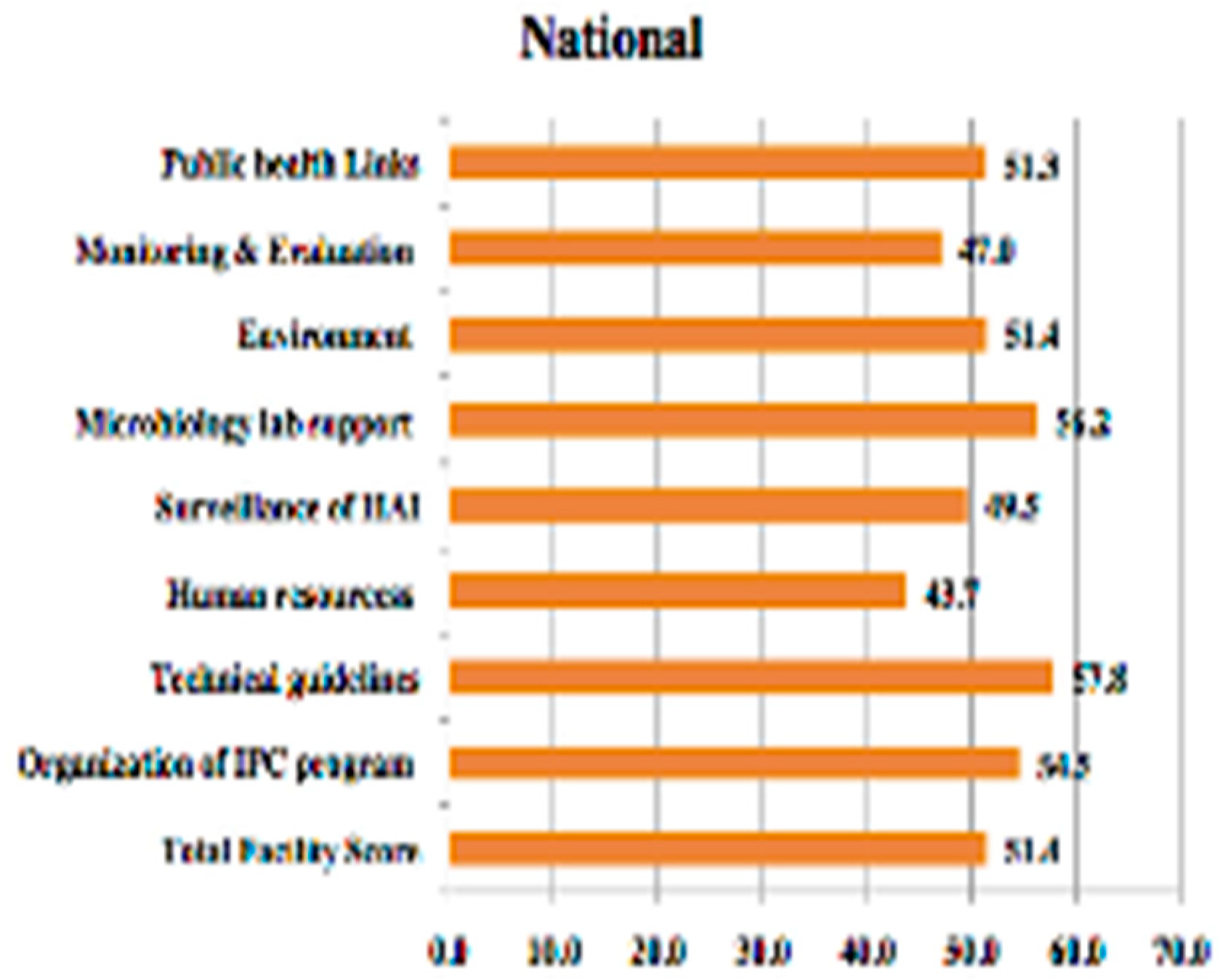
| Infection Control and Prevention Components | North Area | East Area | Central Area | West Area | South Area | National Level |
|---|---|---|---|---|---|---|
| Organisation of IPC Program | 50.6% | 50.1% | 61.7% | 57.1% | 55.6% | 54.5% |
| Technical Guidelines | 53.6% | 53.1% | 64.9% | 60.8% | 57.3% | 57.8% |
| Human Resources | 39.6% | 42.1% | 46.7% | 46.0% | 45.0% | 43.7% |
| Surveillance of HAI | 43.9% | 44.6% | 55.5% | 52.8% | 52.3% | 49.5% |
| Microbiology Lab Support | 49.3% | 52.8% | 63.7% | 60.5% | 57.8% | 56.2% |
| Environment | 45.8% | 42.0% | 59.8 | 57.4% | 53.4% | 51.4% |
| Monitoring and Evaluation | 40.0% | 43.3% | 54.4% | 50.0% | 50.6% | 47.0% |
| Public Health Links | 44.3% | 42.6% | 59.0% | 54.1% | 57.8% | 51.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alslamah, T.; Abalkhail, A. The National Strategies for and Challenges in Infection Prevention and Control of the Healthcare System in the Kingdom of Saudi Arabia (Review Study). Vaccines 2022, 10, 1302. https://doi.org/10.3390/vaccines10081302
Alslamah T, Abalkhail A. The National Strategies for and Challenges in Infection Prevention and Control of the Healthcare System in the Kingdom of Saudi Arabia (Review Study). Vaccines. 2022; 10(8):1302. https://doi.org/10.3390/vaccines10081302
Chicago/Turabian StyleAlslamah, Thamer, and Adil Abalkhail. 2022. "The National Strategies for and Challenges in Infection Prevention and Control of the Healthcare System in the Kingdom of Saudi Arabia (Review Study)" Vaccines 10, no. 8: 1302. https://doi.org/10.3390/vaccines10081302
APA StyleAlslamah, T., & Abalkhail, A. (2022). The National Strategies for and Challenges in Infection Prevention and Control of the Healthcare System in the Kingdom of Saudi Arabia (Review Study). Vaccines, 10(8), 1302. https://doi.org/10.3390/vaccines10081302