
Metformin Use before Influenza Vaccination May Lower the Risks of Influenza and Related Complications
 ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Methods
2.1. Data Sources
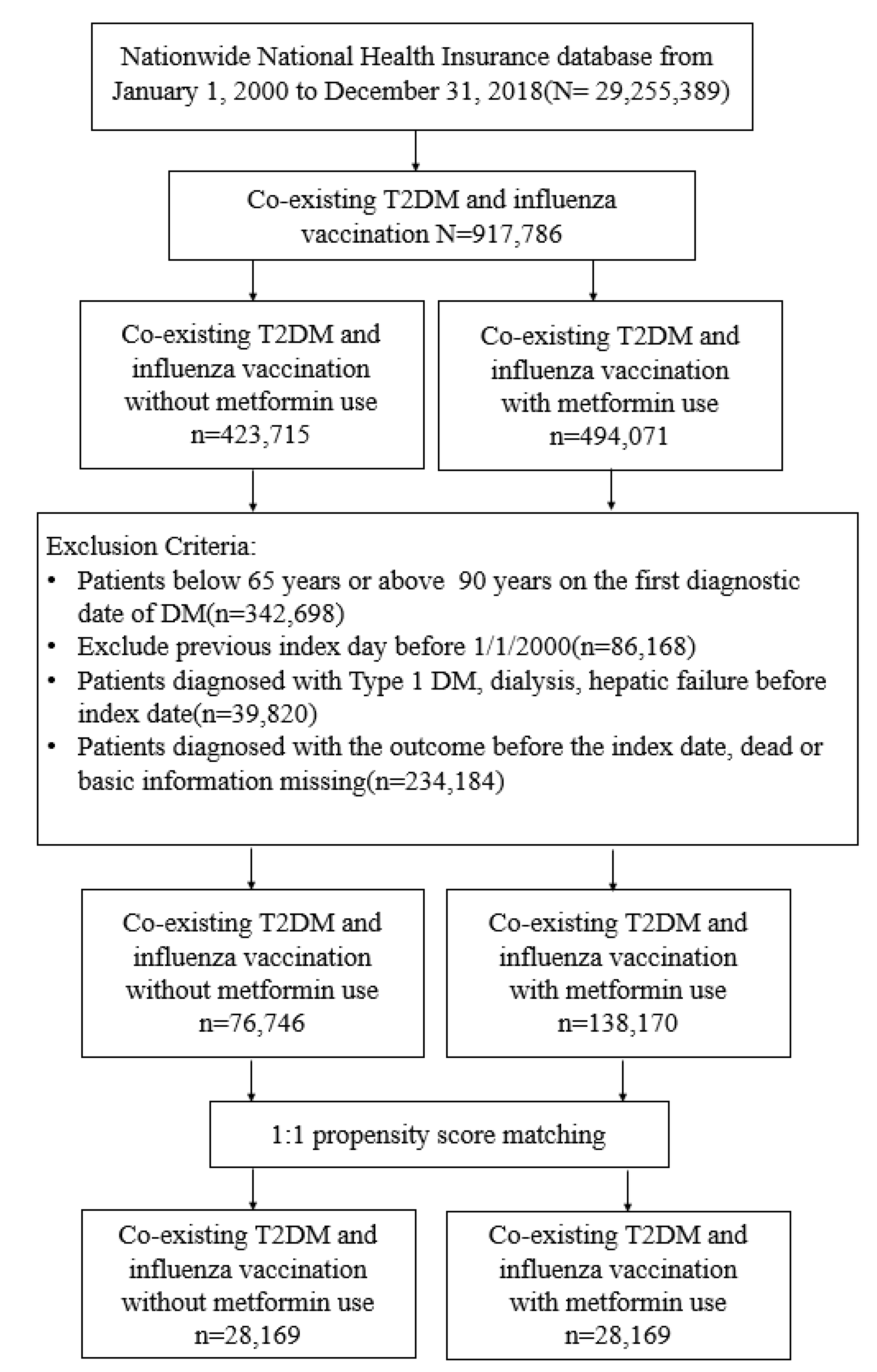
2.2. Study Population
2.3. Study Design and Procedures
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Participants
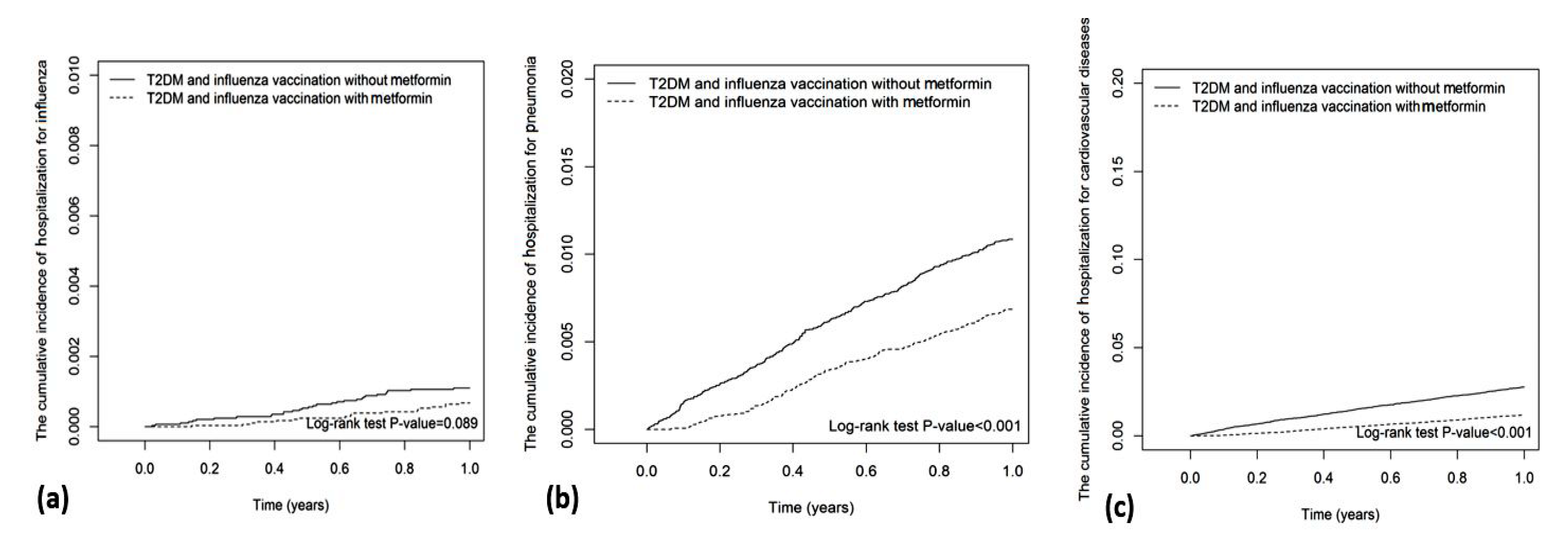
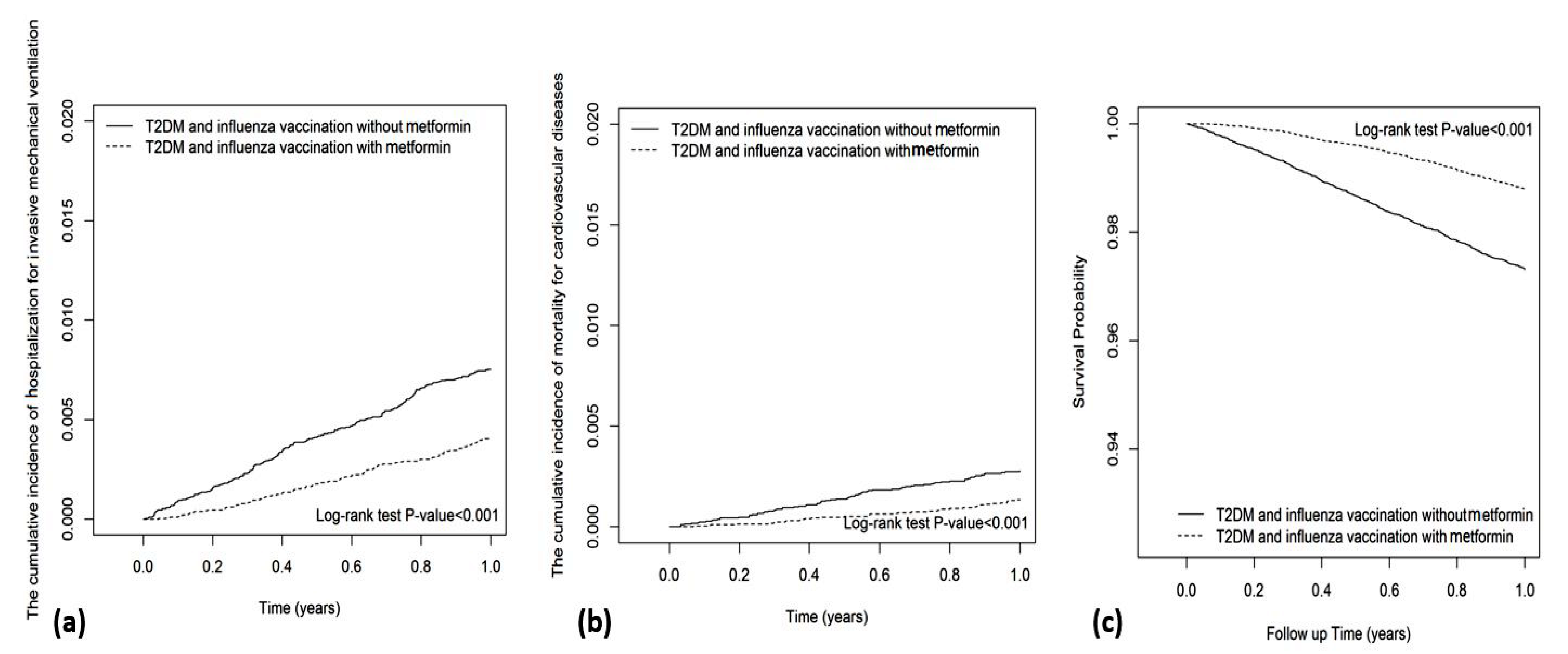
3.2. Main Outcomes
3.3. Cumulative Duration of Metformin Use
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coll, P.P.; Costello, V.W.; Kuchel, G.A.; Bartley, J.; McElhaney, J.E. The prevention of infections in older adults: Vaccination. J. Am. Geriatr. Soc. 2020, 68, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.W.; Shay, D.K.; Weintraub, E.; Brammer, L.; Cox, N.; Anderson, L.J.; Fukuda, K. Mortality associated with influenza and respiratory syncytial virus in the United States. JAMA 2003, 289, 179–186. [Google Scholar] [CrossRef] [PubMed]
- The Institute for Health Metrics and Evaluation (IHME). Global Health Data Exchange; GBD Results Tool. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 19 August 2022).
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Allard, R.; Leclerc, P.; Tremblay, C.; Tannenbaum, T.N. Diabetes and the severity of pandemic influenza A (H1N1) infection. Diabetes Care 2010, 33, 1491–1493. [Google Scholar] [CrossRef]
- Samson, S.I.; Konty, K.; Lee, W.N.; Quisel, T.; Foschini, L.; Kerr, D.; Liska, J.; Mills, H.; Hollingsworth, R.; Greenberg, M.; et al. Quantifying the Impact of Influenza Among Persons with Type 2 Diabetes Mellitus: A New Approach to Determine Medical and Physical Activity Impact. J. Diabetes Sci. Technol. 2021, 15, 44–52. [Google Scholar] [CrossRef]
- Valdez, R.; Narayan, K.M.; Geiss, L.S.; Engelgau, M.M. Impact of diabetes mellitus on mortality associated with pneumonia and influenza among non-Hispanic black and white US adults. Am. J. Public Health 1999, 89, 1715–1721. [Google Scholar] [CrossRef]
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Efficacy and effectiveness of influenza vaccines: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 36–44. [Google Scholar] [CrossRef]
- Grijalva, C.G.; Zhu, Y.; Williams, D.J.; Self, W.H.; Ampofo, K.; Pavia, A.T.; Stockmann, C.R.; McCullers, J.; Arnold, S.R.; Wunderink, R.G.; et al. Association between hospitalization with community-acquired laboratory-confirmed influenza pneumonia and prior receipt of influenza vaccination. JAMA 2015, 314, 1488–1497. [Google Scholar] [CrossRef]
- Lin, C.S.; Chang, C.C.; Yeh, C.C.; Chang, Y.C.; Chen, T.L.; Liao, C.C. Outcomes following diabetes admission in patients who had influenza vaccination: A population-based cohort study. Diabetes Res. Clin. Pract. 2022, 189, 109930. [Google Scholar] [CrossRef]
- Modin, D.; Claggett, B.; Køber, L.; Schou, M.; Jensen, J.U.S.; Solomon, S.D.; Vardeny, O.; Knop, F.K.; Nielsen, S.D.; Fralick, M.; et al. Influenza Vaccination Is Associated with Reduced Cardiovascular Mortality in Adults with Diabetes: A Nationwide Cohort Study. Diabetes Care 2020, 43, 2226–2233. [Google Scholar] [CrossRef]
- Bechini, A.; Ninci, A.; Del Riccio, M.; Biondi, I.; Bianchi, J.; Bonanni, P.; Mannucci, E.; Monami, M. Impact of Influenza Vaccination on All-Cause Mortality and Hospitalization for Pneumonia in Adults and the Elderly with Diabetes: A Meta-Analysis of Observational Studies. Vaccines 2020, 8, 263. [Google Scholar] [CrossRef]
- Brydak, L.B.; Machala, M. Humoral immune response to influenza vaccination in patients from high risk groups. Drugs 2000, 60, 35–53. [Google Scholar] [CrossRef]
- McElhaney, J.E.; Kuchel, G.A.; Zhou, X.; Swain, S.L.; Haynes, L. T-cell immunity to influenza in older adults: A pathophysiological framework for development of more effective vaccines. Front. Immunol. 2016, 7, 41. [Google Scholar] [CrossRef]
- Nakaya, H.I.; Hagan, T.; Duraisingham, S.S.; Lee, E.K.; Kwissa, M.; Rouphael, N.; Frasca, D.; Gersten, M.; Mehta, A.K.; Gaujoux, R.; et al. Systems analysis of immunity to influenza vaccination across multiple years and in diverse populations reveals shared molecular signatures. Immunity 2015, 43, 1186–1198. [Google Scholar] [CrossRef]
- Bailey, C.J. Metformin: Historical overview. Diabetologia 2017, 60, 1566–1576. [Google Scholar] [CrossRef]
- Justice, J.N.; Gubbi, S.; Kulkarni, A.S.; Bartley, J.M.; Kuchel, G.A.; Barzilai, N. A geroscience perspective on immune resilience and infectious diseases: A potential case for metformin. Geroscience 2021, 43, 1093–1112. [Google Scholar] [CrossRef]
- Mannick, J.B.; Del Giudice, G.; Lattanzi, M.; Valiante, N.M.; Praestgaard, J.; Huang, B.; Lonetto, M.A.; Maecker, H.T.; Kovarik, J.; Carson, S.; et al. mTOR inhibition improves immune function in the elderly. Sci. Transl. Med. 2014, 6, 268ra179. [Google Scholar] [CrossRef]
- Diaz, A.; Romero, M.; Vazquez, T.; Lechner, S.; Blomberg, B.B.; Frasca, D. Metformin improves in vivo and in vitro B cell function in individuals with obesity and type-2 diabetes. Vaccine 2017, 35, 2694–2700. [Google Scholar] [CrossRef]
- Cheng, T.M. Taiwan’s new national health insurance program: Genesis and experience so far. Health Aff. 2003, 22, 61–76. [Google Scholar] [CrossRef]
- Lin, C.C.; Lai, M.S.; Syu, C.Y.; Chang, S.C.; Tseng, F.Y. Accuracy of diabetes diagnosis in health insurance claims data in Taiwan. J. Formos. Med. Assoc. 2005, 104, 157–163. [Google Scholar]
- Meduru, P.; Helmer, D.; Rajan, M.; Tseng, C.L.; Pogach, L.; Sambamoorthi, U. Chronic illness with complexity: Implications for performance measurement of optimal glycemic control. J. Gen. Intern. Med. 2007, 22, 408–418. [Google Scholar] [CrossRef]
- Young, B.A.; Lin, E.; Von Korff, M.; Simon, G.; Ciechanowski, P.; Ludman, E.J.; Everson-Stewart, S.; Kinder, L.; Oliver, M.; Boyko, E.J.; et al. Diabetes complications severity index and risk of mortality, hospitalization, and health care utilization. Am. J. Manag. Care 2008, 14, 15–23. [Google Scholar]
- D’Agostino, R.B., Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat. Med. 1998, 17, 2265–2281. [Google Scholar] [CrossRef]
- Thijs, C.; Beyer, W.E.; Govaert, P.M.; Sprenger, M.J.; Dinant, G.J.; Knottnerus, A. Mortality benefits of influenza vaccination in elderly people. Lancet Infect. Dis. 2008, 8, 460–461. [Google Scholar] [CrossRef]
- Talbot, H.K.; Griffin, M.R.; Chen, Q.; Zhu, Y.; Williams, J.V.; Edwards, K.M. Effectiveness of seasonal vaccine in preventing confirmed influenza-associated hospitalizations in community dwelling older adults. J. Infect. Dis. 2011, 203, 500–508. [Google Scholar] [CrossRef]
- Kwong, J.C.; Campitelli, M.A.; Gubbay, J.B.; Peci, A.; Winter, A.L.; Olsha, R.; Turner, R.; Rosella, L.C.; Crowcroft, N.S. Vaccine effectiveness against laboratory-confirmed influenza hospitalizations among elderly adults during the 2010–2011 season. Clin. Infect. Dis. 2013, 57, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Saenwongsa, W.; Nithichanon, A.; Chittaganpitch, M.; Buayai, K.; Kewcharoenwong, C.; Thumrongwilainet, B.; Butta, P.; Palaga, T.; Takahashi, Y.; Ato, M.; et al. Metformin-induced suppression of IFN-α via mTORC1 signalling following seasonal vaccination is associated with impaired antibody responses in type 2 diabetes. Sci. Rep. 2020, 10, 3229. [Google Scholar] [CrossRef]
- Wang, I.K.; Lin, C.L.; Chang, Y.C.; Lin, P.C.; Liang, C.C.; Liu, Y.L.; Chang, C.T.; Yen, T.H.; Huang, C.C.; Sung, F.C. Effectiveness of influenza vaccination in elderly diabetic patients: A retrospective cohort study. Vaccine 2013, 31, 718–724. [Google Scholar] [CrossRef]
- Vasamsetti, S.B.; Karnewar, S.; Kanugula, A.K.; Thatipalli, A.R.; Kumar, J.M.; Kotamraju, S. Metformin inhibits monocyte-to-macrophage differentiation via AMPK-mediated inhibition of STAT3 activation: Potential role in atherosclerosis. Diabetes 2015, 64, 2028–2041. [Google Scholar] [CrossRef]
- Baxter, R.; Ray, G.T.; Fireman, B.H. Effect of influenza vaccination on hospitalizations in persons aged 50 years and older. Vaccine 2010, 28, 7267–7272. [Google Scholar] [CrossRef]
- Yen, F.S.; Wei, J.C.; Shih, Y.H.; Hsu, C.C.; Hwu, C.M. Metformin use and the risk of bacterial pneumonia in patients with type 2 diabetes. Sci. Rep. 2022, 12, 3270. [Google Scholar] [CrossRef] [PubMed]
- Low Wang, C.C.; Hess, C.N.; Hiatt, W.R.; Goldfine, A.B. Clinical update: Cardiovascular disease in diabetes mellitus: Atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus—Mechanisms, management, and clinical considerations. Circulation 2016, 133, 2459–2502. [Google Scholar] [CrossRef] [PubMed]
- Behrouzi, B.; Bhatt, D.L.; Cannon, C.P.; Vardeny, O.; Lee, D.S.; Solomon, S.D.; Udell, J.A. Association of influenza vaccination with cardiovascular risk: A meta-analysis. JAMA Netw. Open 2022, 5, e228873. [Google Scholar] [CrossRef]
- Darvishian, M.; van den Heuvel, E.R.; Bissielo, A.; Castilla, J.; Cohen, C.; Englund, H.; Gefenaite, G.; Huang, W.T.; la Bastide-van Gemert, S.; Martinez-Baz, I.; et al. Effectiveness of seasonal influenza vaccination in community-dwelling elderly people: An individual participant data meta-analysis of test-negative design case-control studies. Lancet Respir. Med. 2017, 5, 200–211. [Google Scholar] [CrossRef]
- Nesti, L.; Natali, A. Metformin effects on the heart and the cardiovascular system: A review of experimental and clinical data. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 657–669. [Google Scholar] [CrossRef]
- Lang, P.O.; Govind, S.; Mitchell, W.A.; Siegrist, C.A.; Aspinall, R. Vaccine effectiveness in older individuals: What has been learned from the influenza-vaccine experience. Ageing Res. Rev. 2011, 10, 389–395. [Google Scholar] [CrossRef]
- Fireman, B.; Lee, J.; Lewis, N.; Bembom, O.; van der Laan, M.; Baxter, R. Influenza vaccination and mortality: Differentiating vaccine effects from bias. Am. J. Epidemiol. 2009, 170, 650–656. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Disease | ICD-9 cm Codes | ICD-10 cm Codes |
|---|---|---|
| Type 2 diabetes mellitus | 250.xx, except 250.1x | E11 |
| Type 1 diabetes mellitus | 250.1x | E10 |
| Hepatic failure | 570, 572.2, 572.4, 572.8 | K72.00, K72.01, K72.10, K72.11, K72.90, K76.2, K72.90, K72.91, K76.7, K76.81 |
| Dialysis | V56.0, V56.8, V45.1 | Z49.31, Z49.32, Z99.2 |
| Obesity | 278.02, 783.1, V85.2, 278.00, 649.1, V77.8, V85.3, 278.01, 649.2, V45.86, V85.4 | R63.5, E66.09, E66.1, E66.8, E66.9, Z13.89, E66.01, E66.2 |
| Smoking status | 305.1, 649.0, V15.82 | F17.200, F17.201, F17.210, F17.220, F17.221, F17.290, F17.291, Z87.891 |
| Alcohol-related disorders | 291, 303, 305.0, 571.0-571.3, V11.3, V79.1 | F10, K70.40, K70.41, K70.9 |
| Hypertension | 401–405, A26 | I10, I11, I12, I13, I15, N26 |
| Dyslipidemia | 272 | E71.30, E71.31, E71.32, E71.39, E75.21, E75.22, E75.23, E75.24, E75.25, E75.29, E75.3, E75.4, E75.5, E75.6, E77, E78.0, E78.1, E78.2, E78.3, E78.4, E78.5, E78.6, E78.70, E78.71, E78.72, E78.79, E78.8, E78.9 |
| Coronary artery disease | 410–414 | I20, I21, I22, I24, I25.1, I25.2, I25.3, I25.4, I25.5, I25.6, I25.7, I25.81, I25.82, I25.83, I25.84, I25.89, I25.9 |
| Chronic kidney disease | 250.4x, 403.xx, 404.xx, 585.xx, 586.xx, 581.8x, 791.0x, 593.9x | E10.2, E10.65, E11.2, E11.65, E13.2, I12, I13, N03, N08, E10.21, E11.21, N05, N06, N07, N14, N15.0, N15.8, N15.9, N16, N17.1, N17.2, N18, N19 |
| Stroke | 430–438 | G45.0, G45.1, G45.2, G45.3, G45.4, G45.8, G45.9, G46, I60, I61, I62, I63, I65, I66, I67.0, I67.1, I67.2, I67.3, I67.4, I67.5, I67.6, I67.7, I67.8, I67.9, I68, I69 |
| Atrial fibrillation | 427 | I45.0, I45.1, I45.2, I45.3, I45.4, I45.5, I45.6 |
| Heart failure | 428 | I50 |
| Peripheral arterial disease | 440.0, 440.20, 440.21, 440.22, 440.23, 440.24, 440.3, 440.4, 443.9, 443.81, 443.89 | I70.2, I70.92, I75.0, I73.9 |
| Chronic obstructive pulmonary disease | 491, 492, or 496 | J41, J42, J44, J43, or J44.9 |
| Pneumonia | 480–486 | J12-18 |
| Liver cirrhosis | 571.5, 571.2, 571.6 | K70.2, K70.30, K70.31, K74.0, K74.1, K74.2, K74.60, K74.69, K74.3, K74.4, K74.5 |
| Cancers | 140–178, 190–199, 209 | C00-C63, C69-C80, C7A-C7B |
| Influenza | 487 | J09-11 |
| Noninvasive positive pressure ventilation | 93.90 and 93.91 | Z99.81 |
| Invasive mechanical ventilation | 96.7 | Z99.1 |
| Variables | Influenza Vaccination without Metformin | Influenza Vaccination with Metformin | SMD | ||
|---|---|---|---|---|---|
| (N = 28,169) | (N = 28,169) | ||||
| n | % | n | % | ||
| Sex | |||||
| female | 14,808 | 52.57 | 14,531 | 51.59 | 0.020 |
| male | 13,361 | 47.43 | 13,638 | 48.41 | 0.020 |
| Age | |||||
| 65–69 | 21,579 | 76.61 | 21,311 | 75.65 | 0.022 |
| 70–74 | 4480 | 15.90 | 4614 | 16.38 | 0.013 |
| 75–79 | 2110 | 7.49 | 2244 | 7.97 | 0.018 |
| mean, (SD) † | 67.99 | 3.92 | 68.05 | 3.97 | 0.015 |
| Obesity | 696 | 2.47 | 674 | 2.39 | 0.005 |
| Smoking status | 663 | 2.35 | 686 | 2.44 | 0.005 |
| Comorbidities | |||||
| Hypertension | 21,976 | 78.01 | 21,795 | 77.37 | 0.015 |
| Dyslipidemia | 21,189 | 75.22 | 20,729 | 73.59 | 0.037 |
| Coronary artery disease | 10,163 | 36.08 | 10,067 | 35.74 | 0.007 |
| Stroke | 4984 | 17.69 | 5062 | 17.97 | 0.007 |
| Atrial fibrillation | 23 | 0.08 | 28 | 0.10 | 0.006 |
| PAD | 2486 | 8.83 | 2453 | 8.71 | 0.004 |
| CKD | 4852 | 17.22 | 4861 | 17.26 | 0.001 |
| Retinopathy | 434 | 1.54 | 478 | 1.70 | 0.012 |
| COPD | 7328 | 26.01 | 7322 | 25.99 | 0.001 |
| Liver cirrhosis | 486 | 1.73 | 519 | 1.84 | 0.009 |
| Cancers | 1771 | 6.29 | 1815 | 6.44 | 0.006 |
| Alcohol-related disorder | 1191 | 4.23 | 1249 | 4.43 | 0.010 |
| CCI scores | |||||
| 1 | 24,457 | 86.82 | 24,325 | 86.35 | 0.014 |
| 2–3 | 3150 | 11.18 | 3226 | 11.45 | 0.009 |
| >3 | 562 | 2.00 | 618 | 2.19 | 0.014 |
| DCSI scores | |||||
| 0 | 5935 | 21.07 | 6019 | 21.37 | 0.007 |
| 1 | 4664 | 16.56 | 4643 | 16.48 | 0.002 |
| ≥2 | 17,570 | 62.37 | 17,507 | 62.15 | 0.005 |
| Medication | |||||
| Sulfonylureas | 4549 | 16.15 | 4731 | 16.80 | 0.017 |
| Thiazolidinedione | 426 | 1.51 | 500 | 1.78 | 0.021 |
| DPP-4 inhibitor | 619 | 2.20 | 710 | 2.52 | 0.021 |
| AGI | 1120 | 3.98 | 1110 | 3.94 | 0.002 |
| Number of oral antidiabetic drugs | |||||
| 1 | 27,337 | 97.05 | 27,143 | 96.36 | 0.039 |
| 2 | 817 | 2.90 | 995 | 3.53 | 0.036 |
| ≧3 | 15 | 0.05 | 31 | 0.11 | 0.020 |
| Insulin | 11,923 | 42.33 | 11,854 | 42.08 | 0.005 |
| Statin | 16,823 | 59.72 | 16,582 | 58.87 | 0.017 |
| Aspirin | 13,749 | 48.81 | 13,703 | 48.65 | 0.003 |
| NSAIDs | 27,772 | 98.59 | 27,677 | 98.25 | 0.027 |
| Outcome | Influenza Vaccination without Metformin | Influenza Vaccination with Metformin | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | PY | IR | n | PY | IR | cHR | (95% CI) | p-Value | aHR† | (95% CI) | p-Value | |
| Hospitalization for influenza | 31 | 28,153 | 1.1 | 19 | 28,162 | 0.7 | 0.61 | (0.35, 1.08) | 0.0927 | 0.6 | (0.34, 1.06) | 0.0766 |
| Hospitalization for pneumonia | 306 | 28,002 | 10.9 | 193 | 28,080 | 6.9 | 0.63 | (0.53, 0.75) | <0.001 | 0.63 | (0.53, 0.76) | <0.001 |
| Hospitalization for CVD | 783 | 27,753 | 28.2 | 334 | 28,018 | 11.9 | 0.42 | (0.37, 0.48) | <0.001 | 0.41 | (0.36, 0.47) | <0.001 |
| NIPPV | 58 | 28,137 | 2.1 | 43 | 28,151 | 1.5 | 0.74 | (0.5, 1.1) | 0.1363 | 0.75 | (0.5, 1.11) | 0.1543 |
| IMV | 212 | 28,057 | 7.6 | 114 | 28,119 | 4.1 | 0.54 | (0.43, 0.67) | <0.001 | 0.56 | (0.45, 0.71) | <0.001 |
| CVD mortality | 78 | 28,129 | 2.8 | 38 | 28,154 | 1.3 | 0.49 | (0.33, 0.72) | <0.001 | 0.49 | (0.33, 0.73) | <0.001 |
| All-cause mortality | 758 | 27,796 | 27.3 | 339 | 28,039 | 12.1 | 0.44 | (0.39, 0.5) | <0.001 | 0.44 | (0.39, 0.51) | <0.001 |
| Variables | n | PY | IR | cHR | (95% CI) | aHR† | (95% CI) |
|---|---|---|---|---|---|---|---|
| Hospitalization for influenza | |||||||
| Metformin no-use | 31 | 28,153 | 1.10 | 1.00 | (Reference) | 1.00 | (Reference) |
| Cumulative duration of metformin use (days) | |||||||
| 28–89 | 11 | 3754 | 2.93 | 2.66 | (1.34, 5.29) ** | 2.3 | (1.14, 4.62) * |
| ≥90 | 8 | 16,276 | 0.49 | 0.45 | (0.21, 0.97) * | 0.44 | (0.2, 0.96) * |
| Hospitalization for pneumonia | |||||||
| Metformin no-use | 306 | 28,002 | 10.93 | 1.00 | (Reference) | 1.00 | (Reference) |
| Cumulative duration of metformin use (days) | |||||||
| 28–89 | 106 | 3742 | 28.32 | 2.59 | (2.08, 3.23) *** | 2.29 | (1.83, 2.87) *** |
| 90–179 | 60 | 11,575 | 5.18 | 0.47 | (0.36, 0.63) *** | 0.54 | (0.41, 0.71) *** |
| >179 | 27 | 4609 | 5.86 | 0.54 | (0.36, 0.79) ** | 0.43 | (0.29, 0.64) *** |
| Hospitalization for cardiovascular diseases | |||||||
| Metformin no-use | 783 | 27,753 | 28.21 | 1.00 | (Reference) | 1.00 | (Reference) |
| Cumulative duration of metformin use (days) | |||||||
| 28–89 | 196 | 3139 | 62.44 | 2.21 | (1.89, 2.59) *** | 2.3 | (1.97, 2.7) *** |
| 90–179 | 101 | 9591 | 10.53 | 0.37 | (0.3, 0.46) *** | 0.43 | (0.35, 0.53) *** |
| >179 | 37 | 3804 | 9.73 | 0.34 | (0.25, 0.48) *** | 0.33 | (0.24, 0.46) *** |
| Invasive mechanical ventilation | |||||||
| Metformin no-use | 212 | 28,057 | 7.56 | 1.00 | (Reference) | 1.00 | (Reference) |
| Cumulative duration of metformin use (days) | |||||||
| 28–89 | 65 | 3741 | 17.38 | 2.3 | (1.74, 3.04) *** | 2.08 | (1.57, 2.76) *** |
| 90–179 | 33 | 11,613 | 2.84 | 0.38 | (0.26, 0.54) *** | 0.45 | (0.31, 0.65) *** |
| >179 | 16 | 4626 | 3.46 | 0.46 | (0.28, 0.76) ** | 0.34 | (0.2, 0.56) *** |
| Cardiovascular-cause mortality | |||||||
| Metformin no-use | 78 | 28,129 | 2.77 | 1.00 | (Reference) | 1.00 | (Reference) |
| Cumulative duration of metformin use (days) | |||||||
| 28–89 | 19 | 3742 | 5.08 | 1.83 | (1.11, 3.02) * | 1.52 | (0.91, 2.54) |
| 90–179 | 11 | 11,635 | 0.95 | 0.34 | (0.18, 0.64) *** | 0.4 | (0.21, 0.76) ** |
| >179 | 8 | 4650 | 1.72 | 0.62 | (0.3, 1.28) | 0.4 | (0.19, 0.83) * |
| All-cause mortality | |||||||
| Metformin no-use | 758 | 27,796 | 27.27 | 1.00 | (Reference) | 1.00 | (Reference) |
| Cumulative duration of metformin use (days) | |||||||
| 28–89 | 150 | 3678 | 40.79 | 1.5 | (1.26, 1.78) *** | 1.46 | (1.22, 1.74) *** |
| 90–179 | 106 | 11,601 | 9.14 | 0.33 | (0.27, 0.41) *** | 0.41 | (0.33, 0.5) *** |
| >179 | 83 | 4633 | 17.92 | 0.66 | (0.52, 0.82) *** | 0.38 | (0.3, 0.47) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, F.-S.; Wei, J.C.-C.; Shih, Y.-H.; Hsu, C.Y.; Hsu, C.-C.; Hwu, C.-M. Metformin Use before Influenza Vaccination May Lower the Risks of Influenza and Related Complications. Vaccines 2022, 10, 1752. https://doi.org/10.3390/vaccines10101752
Yen F-S, Wei JC-C, Shih Y-H, Hsu CY, Hsu C-C, Hwu C-M. Metformin Use before Influenza Vaccination May Lower the Risks of Influenza and Related Complications. Vaccines. 2022; 10(10):1752. https://doi.org/10.3390/vaccines10101752
Chicago/Turabian StyleYen, Fu-Shun, James Cheng-Chung Wei, Ying-Hsiu Shih, Chung Y. Hsu, Chih-Cheng Hsu, and Chii-Min Hwu. 2022. "Metformin Use before Influenza Vaccination May Lower the Risks of Influenza and Related Complications" Vaccines 10, no. 10: 1752. https://doi.org/10.3390/vaccines10101752
APA StyleYen, F.-S., Wei, J. C.-C., Shih, Y.-H., Hsu, C. Y., Hsu, C.-C., & Hwu, C.-M. (2022). Metformin Use before Influenza Vaccination May Lower the Risks of Influenza and Related Complications. Vaccines, 10(10), 1752. https://doi.org/10.3390/vaccines10101752