Advances in Brain Tumor Surgery for Glioblastoma in Adults

Abstract
:1. Introduction
2. Newly Diagnosed and Recurrent GBM: Treatment & Management
3. Surgery for Glioblastoma: Advances and Challenges
4. Current Trends in Glioblastoma Surgery
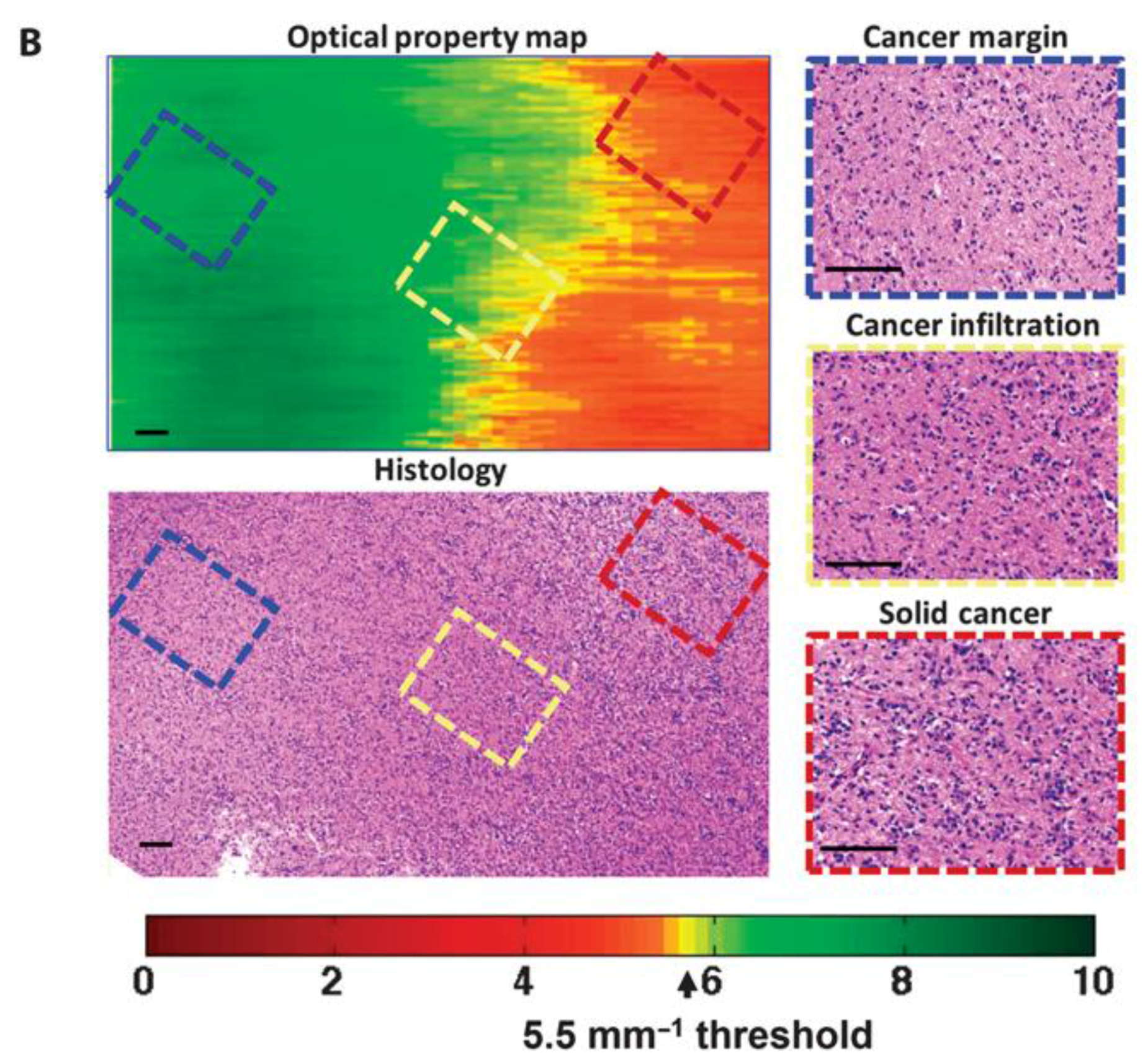
5. Optical Coherence Tomography (OCT): Future Strategy for Glioma Surgery
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; DeMonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A multivariate analysis of 416 patients with glioblastoma multiforme: Prognosis, extent of resection, and survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Laws, E.R.; Parney, I.F.; Huang, W.; Anderson, F.; Morris, A.M.; Asher, A.; Lillehei, K.O.; Bernstein, M.; Brem, H.; Sloan, A.; et al. Survival following surgery and prognostic factors for recently diagnosed malignant glioma: Data from the glioma outcomes project. J. Neurosurg. 2003, 99, 467–473. [Google Scholar] [CrossRef] [PubMed]
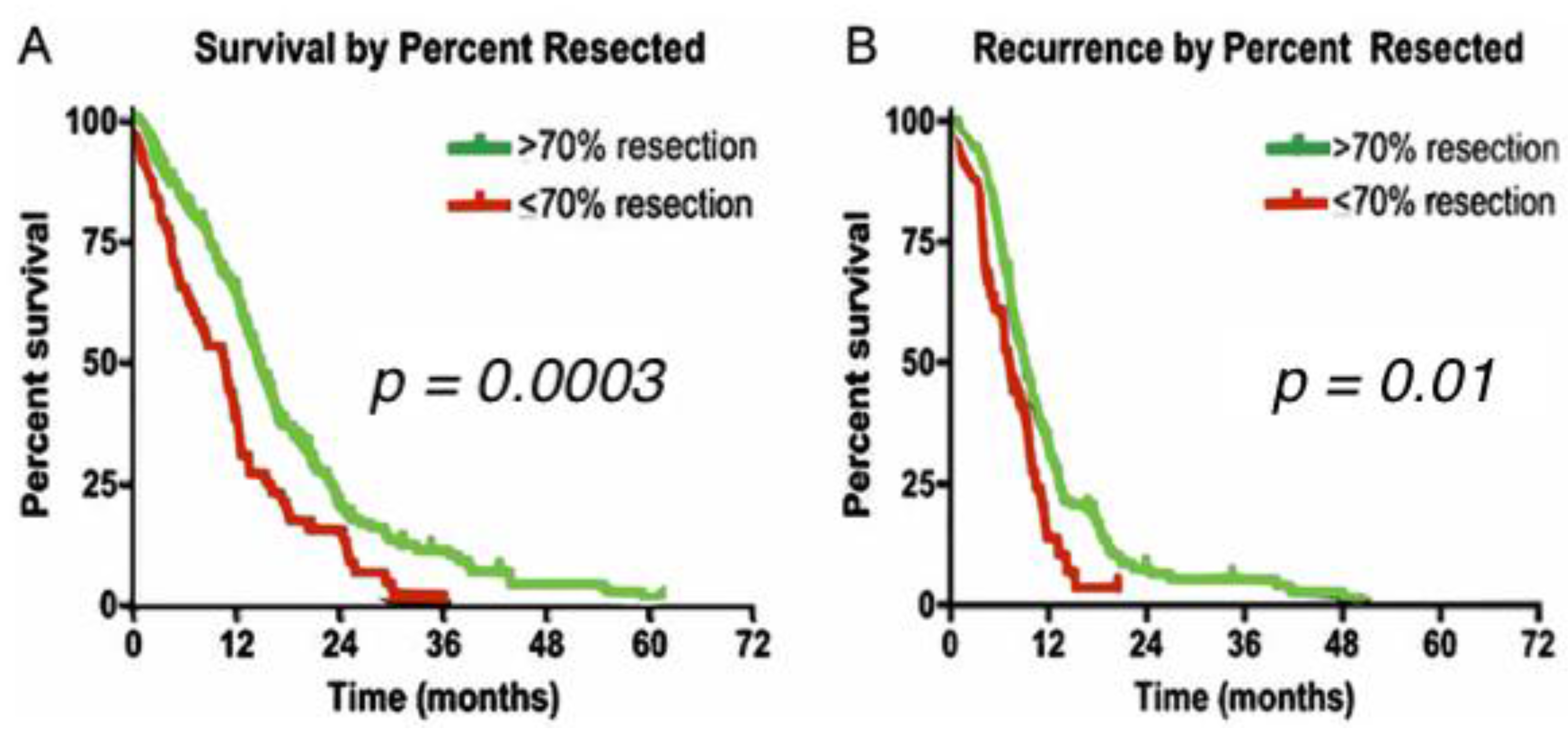
- Sanai, N.; Polley, M.Y.; McDermott, M.W.; Parsa, A.T.; Berger, M.S. An extent of resection threshold for newly diagnosed glioblastomas. J. Neurosurg. 2011, 115, 3–8. [Google Scholar] [CrossRef] [PubMed]
- de Robles, P.; Fiest, K.M.; Frolkis, A.D.; Pringsheim, T.; Atta, C.; St Germaine-Smith, C.; Day, L.; Lam, D.; Jette, N. The worldwide incidence and prevalence of primary brain tumors: A systematic review and meta-analysis. Neuro Oncol. 2015, 17, 776–783. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [PubMed]
- Markert, J.M. The role of early resection vs. biopsy in the management of low-grade gliomas. JAMA 2012, 308, 1918–1919. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Jusue-Torres, I.; Navarro-Ramirez, R.; Raza, S.M.; Pascual-Gallego, M.; Ibrahim, A.; Hernandez-Hermann, M.; Gomez, L.; Ye, X.; Weingart, J.D.; et al. Establishing percent resection and residual volume thresholds affecting survival and recurrence for patients with newly diagnosed intracranial glioblastoma. Neuro Oncol. 2014, 16, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Jusue-Torres, I.; Lemos, A.M.; Gokaslan, A.; Cabrera-Aldana, E.E.; Ashary, A.; Olivi, A.; Quinones-Hinojosa, A. The butterfly effect on glioblastoma: Is volumetric extent of resection more effective than biopsy for these tumors? J. Neurooncol. 2014, 120, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Senft, C.; Bink, A.; Franz, K.; Vatter, H.; Gasser, T.; Seifert, V. Intraoperative mri guidance and extent of resection in glioma surgery: A randomised, controlled trial. Lancet Oncol. 2011, 12, 997–1003. [Google Scholar] [CrossRef]
- Tilghman, J.; Wu, H.; Sang, Y.; Shi, X.; Guerrero-Cazares, H.; Quinones-Hinojosa, A.; Eberhart, C.G.; Laterra, J.; Ying, M. Hmmr maintains the stemness and tumorigenicity of glioblastoma stem-like cells. Cancer Res. 2014, 74, 3168–3179. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Cheng, L.; Guryanova, O.A.; Wu, Q.; Bao, S. Cancer stem cells in glioblastoma-molecular signaling and therapeutic targeting. Protein Cell 2010, 1, 638–655. [Google Scholar] [CrossRef] [PubMed]
- Iacob, G.; Dinca, E.B. Current data and strategy in glioblastoma multiforme. J. Med. Life 2009, 2, 386–393. [Google Scholar] [PubMed]
- Lara-Velazquez, M.; Akinduro, O.O.; Reimer, R.; Woodmansee, W.W.; Quinones-Hinojosa, A. Stem cell therapy and its potential role in pituitary disorders. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Lathia, J.D.; Liu, H. Overview of cancer stem cells and stemness for community oncologists. Target. Oncol. 2017, 12, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Amelot, A.; De Cremoux, P.; Quillien, V.; Polivka, M.; Adle-Biassette, H.; Lehmann-Che, J.; Françoise, L.; Carpentier, A.F.; George, B.; Mandonnet, E.; et al. Idh-mutation is a weak predictor of long-term survival in glioblastoma patients. PLoS ONE 2015. [Google Scholar] [CrossRef] [PubMed]
- Verhaak, R.G.; Hoadley, K.A.; Purdom, E.; Wang, V.; Qi, Y.; Wilkerson, M.D.; Miller, C.R.; Ding, L.; Golub, T.; Mesirov, J.P.; et al. Integrated genomic analysis identifies clinically relevant subtypes of glioblastoma characterized by abnormalities in PDGFRA, IDH1, EGFR, and NF1. Cancer Cell 2010, 17, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.T.; Cho, H.J.; Kim, J.; Lee, J.H.; Rho, K.; Seo, Y.J.; Choi, Y.S.; Jung, H.J.; Song, H.S.; Kong, D.S.; et al. Translational validation of personalized treatment strategy based on genetic characteristics of glioblastoma. PLoS ONE 2014, 9, e103327. [Google Scholar] [CrossRef] [PubMed]
- Phillips, H.S.; Kharbanda, S.; Chen, R.; Forrest, W.F.; Soriano, R.H.; Wu, T.D.; Misra, A.; Nigro, J.M.; Colman, H.; Soroceanu, L.; et al. Molecular subclasses of high-grade glioma predict prognosis, delineate a pattern of disease progression, and resemble stages in neurogenesis. Cancer Cell 2006, 9, 157–173. [Google Scholar] [CrossRef] [PubMed]
- Theeler, B.J.; Gilbert, M.R. Advances in the treatment of newly diagnosed glioblastoma. BMC Med. 2015, 13, 293. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Gittleman, H.; Liao, P.; Rouse, C.; Chen, Y.; Dowling, J.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J. Cbtrus statistical report: Primary brain and central nervous system tumors diagnosed in the united states in 2007–2011. Neuro Oncol. 2014, 16, iv1–iv63. [Google Scholar] [CrossRef] [PubMed]
- Rivera, A.L.; Pelloski, C.E.; Gilbert, M.R.; Colman, H.; De La Cruz, C.; Sulman, E.P.; Bekele, B.N.; Aldape, K.D. Mgmt promoter methylation is predictive of response to radiotherapy and prognostic in the absence of adjuvant alkylating chemotherapy for glioblastoma. Neuro Oncol. 2010, 12, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, M.; Gandhi, A.K.; Devnani, B.; Kumar, P.; Sharma, D.N.; Julka, P.K. Comparative study of adjuvant temozolomide six cycles versus extended 12 cycles in newly diagnosed glioblastoma multiforme. J. Clin. Diagn. Res. 2017, 11, XC04–XC08. [Google Scholar] [CrossRef] [PubMed]
- Olar, A.; Aldape, K.D. Using the molecular classification of glioblastoma to inform personalized treatment. J. Pathol. 2014, 232, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, L.E.; Fisher, B.J.; Macdonald, D.R.; LeBer, D.V.; Halperin, E.C.; Schold, S.C., Jr.; Cairncross, J.G. Supratentorial malignant glioma: Patterns of recurrence and implications for external beam local treatment. Int. J. Radiat. Oncol. Biol. Phys. 1992, 24, 55–57. [Google Scholar] [CrossRef]
- Wong, E.T.; Hess, K.R.; Gleason, M.J.; Jaeckle, K.A.; Kyritsis, A.P.; Prados, M.D.; Levin, V.A.; Yung, W.K. Outcomes and prognostic factors in recurrent glioma patients enrolled onto phase ii clinical trials. J. Clin. Oncol. 1999, 17, 2572–2578. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Zadnik, P.; Weingart, J.D.; Olivi, A.; Gallia, G.L.; Blakeley, J.; Lim, M.; Brem, H.; Quinones-Hinojosa, A. Multiple resections for patients with glioblastoma: Prolonging survival. J. Neurosurg. 2013, 118, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Lahiri, D.; Maji, T.; Biswas, J. Recurrent glioblastoma: Where we stand. South Asian J. Cancer 2015, 4, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Stockelmaier, L.; Renovanz, M.; Konig, J.; Nickel, K.; Hickmann, A.K.; Mayer-Steinacker, R.; Nadji-Ohl, M.; Ganslandt, O.; Bullinger, L.; Wirtz, C.R.; et al. Therapy for recurrent high-grade gliomas: Results of a prospective multicenter study on health-related quality of life. World Neurosurg. 2017, 102, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Rahmathulla, G.; Hovey, E.J.; Hashemi-Sadraei, N.; Ahluwalia, M.S. Bevacizumab in high-grade gliomas: A review of its uses, toxicity assessment, and future treatment challenges. OncoTargets Ther. 2013, 6, 371–389. [Google Scholar] [CrossRef] [PubMed]
- Vredenburgh, J.J.; Desjardins, A.; Herndon, J.E., 2nd; Dowell, J.M.; Reardon, D.A.; Quinn, J.A.; Rich, J.N.; Sathornsumetee, S.; Gururangan, S.; Wagner, M.; et al. Phase ii trial of bevacizumab and irinotecan in recurrent malignant glioma. Clin. Cancer Res. 2007, 13, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Friedman, H.S.; Prados, M.D.; Wen, P.Y.; Mikkelsen, T.; Schiff, D.; Abrey, L.E.; Yung, W.K.; Paleologos, N.; Nicholas, M.K.; Jensen, R.; et al. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J. Clin. Oncol. 2009, 27, 4733–4740. [Google Scholar] [CrossRef] [PubMed]
- Attenello, F.J.; Mukherjee, D.; Datoo, G.; McGirt, M.J.; Bohan, E.; Weingart, J.D.; Olivi, A.; Quinones-Hinojosa, A.; Brem, H. Use of gliadel (BCNU) wafer in the surgical treatment of malignant glioma: A 10-year institutional experience. Ann. Surg. Oncol. 2008, 15, 2887–2893. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Kone, L.; Bettegowda, C.; Weingart, J.D.; Olivi, A.; Lim, M.; Quinones-Hinojosa, A.; Gallia, G.L.; Brem, H. Risk of surgical site infection in 401 consecutive patients with glioblastoma with and without carmustine wafer implantation. Neurol. Res. 2015, 37, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Zaidi, H.; Pendleton, C.; McGirt, M.J.; Grossman, R.; Weingart, J.D.; Olivi, A.; Quinones-Hinojosa, A.; Brem, H. The efficacy of carmustine wafers for older patients with glioblastoma multiforme: Prolonging survival. Neurol. Res. 2011, 33, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Grossman, R.; Burger, P.; Soudry, E.; Tyler, B.; Chaichana, K.L.; Weingart, J.; Olivi, A.; Gallia, G.L.; Sidransky, D.; Quinones-Hinojosa, A.; et al. Mgmt inactivation and clinical response in newly diagnosed gbm patients treated with gliadel. J. Clin. Neurosci. 2015, 22, 1938–1942. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Than, K.D.; Weingart, J.D.; Chaichana, K.L.; Attenello, F.J.; Olivi, A.; Laterra, J.; Kleinberg, L.R.; Grossman, S.A.; Brem, H.; et al. Gliadel (BCNU) wafer plus concomitant temozolomide therapy after primary resection of glioblastoma multiforme. J. Neurosurg. 2009, 110, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Kaloshi, G.; Diamandi, P.; Cakani, B.; Brace, G.; Rroji, A.; Petrela, M. The added value of bevacizumab concomitantly administered with carboplatin versus carboplatin alone in patients with recurrent glioblastomas. Tumori 2015, 101, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Elizabeth, G. Cediranib Maleate and Cilengitide in Treating Patients with Progressive or Recurrent Glioblastoma. 2009. Available online: https://clinicaltrials.gov/ct2/show/NCT00979862 (accessed on 12 November 2017).
- Vogelbaum, M.A. Erlotinib in Treating Patients with Recurrent or Progressive Glioblastoma Multiforme. 2002. Available online: https://clinicaltrials.gov/ct2/show/study/NCT00979862 (accessed on 15 November 2017).
- Rich, J.N.; Reardon, D.A.; Peery, T.; Dowell, J.M.; Quinn, J.A.; Penne, K.L.; Wikstrand, C.J.; Duyn, L.B.V.; Dancey, J.E.; McLendon, R.E.; et al. Phase ii trial of gefitinib in recurrent glioblastoma. J. Clin. Oncol. 2004, 22, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Gil-Gil, M.J.; Mesia, C.; Rey, M.; Bruna, J. Bevacizumab for the treatment of glioblastoma. Clin. Med. Insights Oncol. 2013, 7, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.M.; Weinberg, U.; Palti, Y. Tumor treating fields: A new frontier in cancer therapy. Ann. N. Y. Acad. Sci. 2013, 1291, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Taillibert, S.; Kanner, A.A.; Kesari, S.; Steinberg, D.M.; Toms, S.A.; Taylor, L.P.; Lieberman, F.; Silvani, A.; Fink, K.L.; et al. Maintenance therapy with tumor-treating fields plus temozolomide vs. temozolomide alone for glioblastoma: A randomized clinical trial. JAMA 2015, 314, 2535–2543. [Google Scholar] [CrossRef] [PubMed]
- US Cancer Statistics Working Group. United States Cancer Statistics: 1999–2014 Incidence and Mortality Web-Based Report; Department of Health and Human Services, Centers for Disease Control and Prevention, and National Cancer Institute: Atlanta, GA, USA, 2017.
- Bloch, O.; Han, S.J.; Cha, S.; Sun, M.Z.; Aghi, M.K.; McDermott, M.W.; Berger, M.S.; Parsa, A.T. Impact of extent of resection for recurrent glioblastoma on overall survival: Clinical article. J. Neurosurg. 2012, 117, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Eseonu, C.I.; ReFaey, K.; Garcia, O.; Raghuraman, G.; Quinones-Hinojosa, A. Volumetric analysis of extent of resection, survival, and surgical outcomes for insular gliomas. World Neurosurg. 2017, 103, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Eseonu, C.I.; Eguia, F.; ReFaey, K.; Garcia, O.; Rodriguez, F.J.; Chaichana, K.; Quinones-Hinojosa, A. Comparative volumetric analysis of the extent of resection of molecularly and histologically distinct low grade gliomas and its role on survival. J. Neurooncol. 2017, 134, 65–74. [Google Scholar] [CrossRef] [PubMed]
- McGirt, M.J.; Chaichana, K.L.; Gathinji, M.; Attenello, F.J.; Than, K.; Olivi, A.; Weingart, J.D.; Brem, H.; Quinones-Hinojosa, A.R. Independent association of extent of resection with survival in patients with malignant brain astrocytoma. J. Neurosurg. 2009, 110, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.J.; Brennan, M.C.; Li, M.; Church, E.W.; Brandmeir, N.J.; Rakszawski, K.L.; Patel, A.S.; Rizk, E.B.; Suki, D.; Sawaya, R.; et al. Association of the extent of resection with survival in glioblastoma: A systematic review and meta-analysis. JAMA Oncol. 2016, 2, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Hervey-Jumper, S.L.; Berger, M.S. Role of surgical resection in low- and high-grade gliomas. Curr. Treat. Opt. Neurol. 2014, 16, 284. [Google Scholar] [CrossRef] [PubMed]
- Reyns, N.; Leroy, H.A.; Delmaire, C.; Derre, B.; Le-Rhun, E.; Lejeune, J.P. Intraoperative mri for the management of brain lesions adjacent to eloquent areas. Neurochirurgie 2017, 63, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Ronkainen, J.; Tervonen, O. Cost analysis of an open low-field (0.23t) mri unit: Effect of procedure shares in combined imaging, interventional, and neurosurgical use. Acta Radiol. 2006, 47, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Eseonu, C.I.; ReFaey, K.; Garcia, O.; John, A.; Quinones-Hinojosa, A.; Tripathi, P. Awake craniotomy anesthesia: A comparison of the monitored anesthesia care and asleep-awake-asleep techniques. World Neurosurg. 2017, 104, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Eseonu, C.I.; Rincon-Torroella, J.; ReFaey, K.; Lee, Y.M.; Nangiana, J.; Vivas-Buitrago, T.; Quinones-Hinojosa, A. Awake craniotomy vs. craniotomy under general anesthesia for perirolandic gliomas: Evaluating perioperative complications and extent of resection. Neurosurgery 2017, 81, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Eseonu, C.I.; Rincon-Torroella, J.; ReFaey, K.; Quinones-Hinojosa, A. The cost of brain surgery: Awake vs. asleep craniotomy for perirolandic region tumors. Neurosurgery 2017, 81, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Quinones-Hinojosa, A.; Ojemann, S.G.; Sanai, N.; Dillon, W.P.; Berger, M.S. Preoperative correlation of intraoperative cortical mapping with magnetic resonance imaging landmarks to predict localization of the broca area. J. Neurosurg. 2003, 99, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.A.; Quinones-Hinojosa, A.; Berger, M.S. Intraoperative speech mapping in 17 bilingual patients undergoing resection of a mass lesion. Neurosurgery 2004, 54, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Southwell, D.G.; Hervey-Jumper, S.L.; Perry, D.W.; Berger, M.S. Intraoperative mapping during repeat awake craniotomy reveals the functional plasticity of adult cortex. J. Neurosurg. 2016, 124, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; McCutcheon, I.E.; Suki, D.; Weinberg, J.S.; Sawaya, R.; Lang, F.F.; Ferson, D.; Heimberger, A.B.; DeMonte, F.; Prabhu, S.S. Awake craniotomy for brain tumors near eloquent cortex: Correlation of intraoperative cortical mapping with neurological outcomes in 309 consecutive patients. Neurosurgery 2009, 64, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.; Hervey-Jumper, S.L.; Han, S.J.; Berger, M.S. Intraoperative perception and estimates on extent of resection during awake glioma surgery: Overcoming the learning curve. J. Neurosurg. 2017, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bebawy, J. Quality of Recovery Awake versus Asleep Craniotomy. 2014. Available online: https://clinicaltrials.gov/ct2/show/NCT02228993 (accessed on 8 October 2017).
- Bajunaid, K.M.; Ajlan, A.M. Awake craniotomy. A patient’s perspective. Neurosciences 2015, 20, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Martirosyan, N.L.; Cavalcanti, D.D.; Eschbacher, J.M.; Delaney, P.M.; Scheck, A.C.; Abdelwahab, M.G.; Nakaji, P.; Spetzler, R.F.; Preul, M.C. Use of in vivo near-infrared laser confocal endomicroscopy with indocyanine green to detect the boundary of infiltrative tumor. J. Neurosurg. 2011, 115, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Eschbacher, J.; Martirosyan, N.L.; Nakaji, P.; Sanai, N.; Preul, M.C.; Smith, K.A.; Coons, S.W.; Spetzler, R.F. In vivo intraoperative confocal microscopy for real-time histopathological imaging of brain tumors. J. Neurosurg. 2012, 116, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.E.; Peyton, W.T.; French, L.A.; Walker, W.W. The clinical use of fluorescein in neurosurgery; the localization of brain tumors. J. Neurosurg. 1948, 5, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Murray, K.J. Improved surgical resection of human brain tumors: Part I. A preliminary study. Surg. Neurol. 1982, 17, 316–319. [Google Scholar] [CrossRef]
- Senders, J.T.; Muskens, I.S.; Schnoor, R.; Karhade, A.V.; Cote, D.J.; Smith, T.R.; Broekman, M.L. Agents for fluorescence-guided glioma surgery: A systematic review of preclinical and clinical results. Acta Neurochir. 2017, 159, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Q.T.; Tsien, R.Y. Fluorescence-guided surgery with live molecular navigation—A new cutting edge. Nat. Rev. Cancer 2013, 13, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Mansouri, A.; Mansouri, S.; Hachem, L.D.; Klironomos, G.; Vogelbaum, M.A.; Bernstein, M.; Zadeh, G. The role of 5-aminolevulinic acid in enhancing surgery for high-grade glioma, its current boundaries, and future perspectives: A systematic review. Cancer 2016, 122, 2469–2478. [Google Scholar] [CrossRef] [PubMed]
- Norred, S.E.; Johnson, J.A. Magnetic resonance-guided laser induced thermal therapy for glioblastoma multiforme: A review. Biomed. Res. Int. 2014, 2014, 761312. [Google Scholar] [CrossRef] [PubMed]
- Rahmathulla, G.; Recinos, P.F.; Valerio, J.E.; Chao, S.; Barnett, G.H. Laser interstitial thermal therapy for focal cerebral radiation necrosis: A case report and literature review. Stereotact. Funct. Neurosurg. 2012, 90, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Laidler, K.J. The development of the arrhenius equation. J. Chem. Educ. 1984, 61, 949. [Google Scholar] [CrossRef]
- Schwarzmaier, H.J.; Eickmeyer, F.; von Tempelhoff, W.; Fiedler, V.U.; Niehoff, H.; Ulrich, S.D.; Yang, Q.; Ulrich, F. Mr-guided laser-induced interstitial thermotherapy of recurrent glioblastoma multiforme: Preliminary results in 16 patients. Eur. J. Radiol. 2006, 59, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Carpentier, A.; Chauvet, D.; Reina, V.; Beccaria, K.; Leclerq, D.; McNichols, R.J.; Gowda, A.; Cornu, P.; Delattre, J.Y. Mr-guided laser-induced thermal therapy (LITT) for recurrent glioblastomas. Lasers Surg. Med. 2012, 44, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.M.; Hawasli, A.H.; Rodriguez, A.; Schroeder, J.L.; Laxton, A.W.; Elson, P.; Tatter, S.B.; Barnett, G.H.; Leuthardt, E.C. The role of laser interstitial thermal therapy in enhancing progression-free survival of difficult-to-access high-grade gliomas: A multicenter study. Cancer Med. 2014, 3, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Agar, N.Y.; Golby, A.J.; Ligon, K.L.; Norton, I.; Mohan, V.; Wiseman, J.M.; Tannenbaum, A.; Jolesz, F.A. Development of stereotactic mass spectrometry for brain tumor surgery. Neurosurgery 2011, 68, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Pacholski, M.L.; Winograd, N. Imaging with mass spectrometry. Chem. Rev. 1999, 99, 2977–3006. [Google Scholar] [CrossRef] [PubMed]
- Stoeckli, M.; Chaurand, P.; Hallahan, D.E.; Caprioli, R.M. Imaging mass spectrometry: A new technology for the analysis of protein expression in mammalian tissues. Nat. Med. 2001, 7, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Karas, M.; Bachmann, D.; Bahr, U.E.; Hillenkamp, F. Matrix-assisted ultraviolet laser desorption of non-volatile compounds. Int. J. Mass Spectrom. Ion Process. 1987, 78, 53–68. [Google Scholar] [CrossRef]
- Takats, Z.; Wiseman, J.M.; Gologan, B.; Cooks, R.G. Mass spectrometry sampling under ambient conditions with desorption electrospray ionization. Science 2004, 306, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Young, R.M.; Jamshidi, A.; Davis, G.; Sherman, J.H. Current trends in the surgical management and treatment of adult glioblastoma. Ann. Transl. Med. 2015, 3, 121. [Google Scholar] [PubMed]
- Santagata, S.; Eberlin, L.S.; Norton, I.; Calligaris, D.; Feldman, D.R.; Ide, J.L.; Liu, X.; Wiley, J.S.; Vestal, M.L.; Ramkissoon, S.H.; et al. Intraoperative mass spectrometry mapping of an onco-metabolite to guide brain tumor surgery. Proc. Natl. Acad. Sci. USA 2014, 111, 11121–11126. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Parsons, D.W.; Jin, G.; McLendon, R.; Rasheed, B.A.; Yuan, W.; Kos, I.; Batinic-Haberle, I.; Jones, S.; Riggins, G.J.; et al. IDH1 and IDH2 mutations in gliomas. N. Engl. J. Med. 2009, 360, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Pirro, V.; Alfaro, C.M.; Jarmusch, A.K.; Hattab, E.M.; Cohen-Gadol, A.A.; Cooks, R.G. Intraoperative assessment of tumor margins during glioma resection by desorption electrospray ionization-mass spectrometry. Proc. Natl. Acad. Sci. USA 2017, 114, 6700–6705. [Google Scholar] [CrossRef] [PubMed]
- Kut, C.; Chaichana, K.L.; Xi, J.; Raza, S.M.; Ye, X.; McVeigh, E.R.; Rodriguez, F.J.; Quinones-Hinojosa, A.; Li, X. Detection of human brain cancer infiltration ex vivo and in vivo using quantitative optical coherence tomography. Sci. Transl. Med. 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- Iftimia, N.; Hammer, D.X.; Mujat, M.; Desphande, V.; Cizginer, S.; Brugge, W. Optical coherence tomography imaging for cancer diagnosis and therapy guidance. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2009, 2009, 4067–4069. [Google Scholar] [PubMed]
- Sufan, R.I.; Moriyama, E.H.; Mariampillai, A.; Roche, O.; Evans, A.J.; Alajez, N.M.; Vitkin, I.A.; Yang, V.X.; Liu, F.F.; Wilson, B.C.; et al. Oxygen-independent degradation of HIF-alpha via bioengineered VHL tumour suppressor complex. EMBO Mol. Med. 2009, 1, 66–78. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Percentage of Resection | Type of Surgery | p Value | |
|---|---|---|---|
| Asleep (n = 31) | Awake (n = 27) | ||
| 100% | 2 (6.5%) | 7 (25.9%) | 0.041 |
| ≥95%, <100% | 11 (35.5%) | 10 (37.0%) | 0.902 |
| <95% | 18 (58.1%) | 10 (37.0%) | 0.110 |
| Name | Specifications |
|---|---|
| ICG | FDA approved for injection in cardiology and ophthalmology Used to determine tumor angiogenesis or vascular malformations (i.e., Hemangioblastoma) [59] Emission peak of 820 nm Depth approximately of >350 μm [55] AE: anaphylactic reactions |
| Hypericin | A red-colored fluorophore with a sensitivity of 94% and a specificity of 100% for glioma surgery [60] Emits signal at 590 nm AE: anaphylactic reactions |
| FS | Green fluorophore, used in glioma surgery to improve gross total resection (30–80% of tumor removal) Excited at 480 nm AE: anaphylactic reactions and yellow pigmentation of skin, mucosa and urine [54,61,62,63]. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lara-Velazquez, M.; Al-Kharboosh, R.; Jeanneret, S.; Vazquez-Ramos, C.; Mahato, D.; Tavanaiepour, D.; Rahmathulla, G.; Quinones-Hinojosa, A. Advances in Brain Tumor Surgery for Glioblastoma in Adults. Brain Sci. 2017, 7, 166. https://doi.org/10.3390/brainsci7120166
Lara-Velazquez M, Al-Kharboosh R, Jeanneret S, Vazquez-Ramos C, Mahato D, Tavanaiepour D, Rahmathulla G, Quinones-Hinojosa A. Advances in Brain Tumor Surgery for Glioblastoma in Adults. Brain Sciences. 2017; 7(12):166. https://doi.org/10.3390/brainsci7120166
Chicago/Turabian StyleLara-Velazquez, Montserrat, Rawan Al-Kharboosh, Stephanie Jeanneret, Carla Vazquez-Ramos, Deependra Mahato, Daryoush Tavanaiepour, Gazanfar Rahmathulla, and Alfredo Quinones-Hinojosa. 2017. "Advances in Brain Tumor Surgery for Glioblastoma in Adults" Brain Sciences 7, no. 12: 166. https://doi.org/10.3390/brainsci7120166
APA StyleLara-Velazquez, M., Al-Kharboosh, R., Jeanneret, S., Vazquez-Ramos, C., Mahato, D., Tavanaiepour, D., Rahmathulla, G., & Quinones-Hinojosa, A. (2017). Advances in Brain Tumor Surgery for Glioblastoma in Adults. Brain Sciences, 7(12), 166. https://doi.org/10.3390/brainsci7120166