

Innovative Approaches to Eating Disorders Treatment: A Systematic Review on the Effectiveness of Virtual Reality


Abstract
1. Introduction
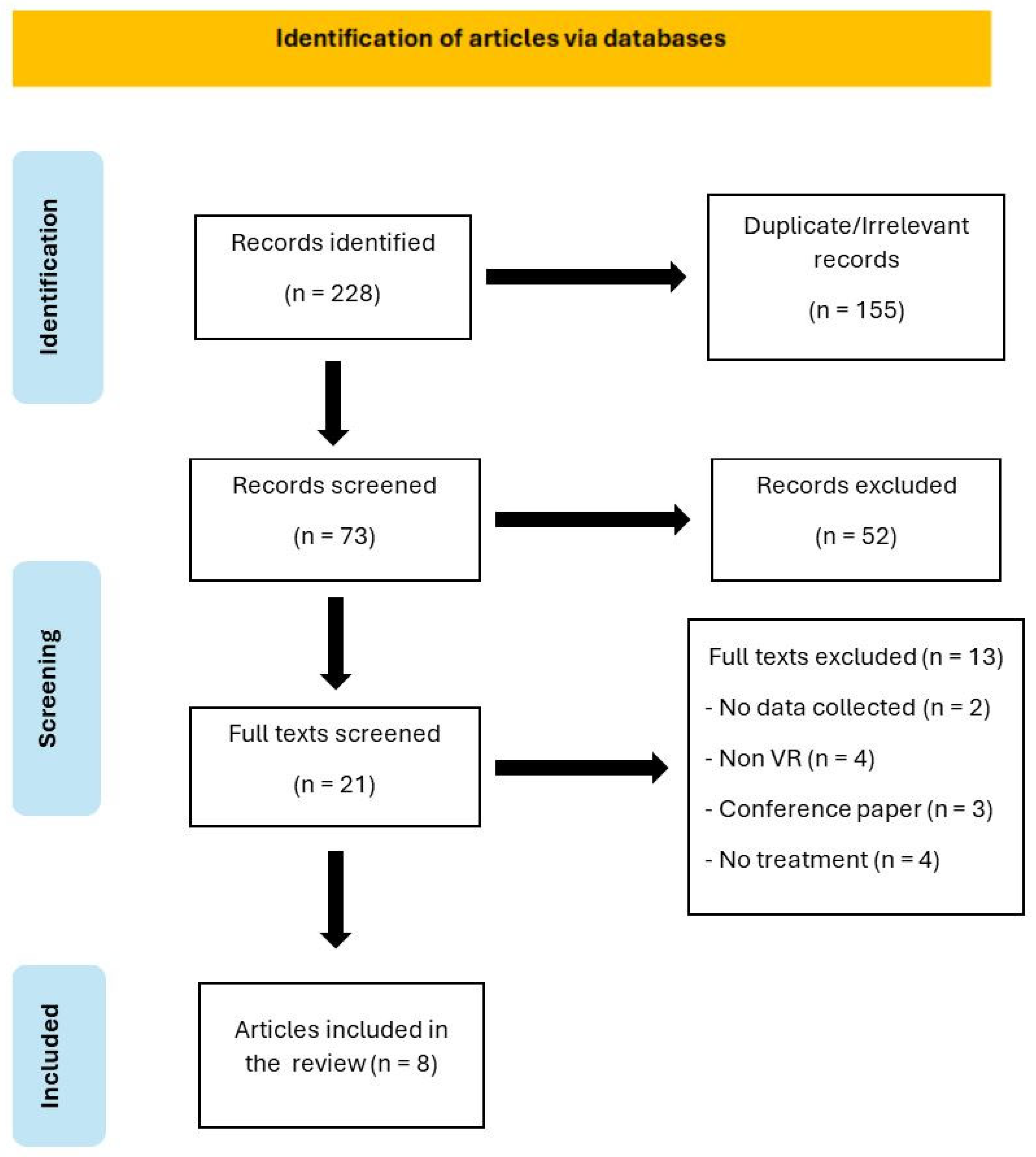
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategies and Data Extraction
2.3. Quality Analyses of the Studies
3. Results
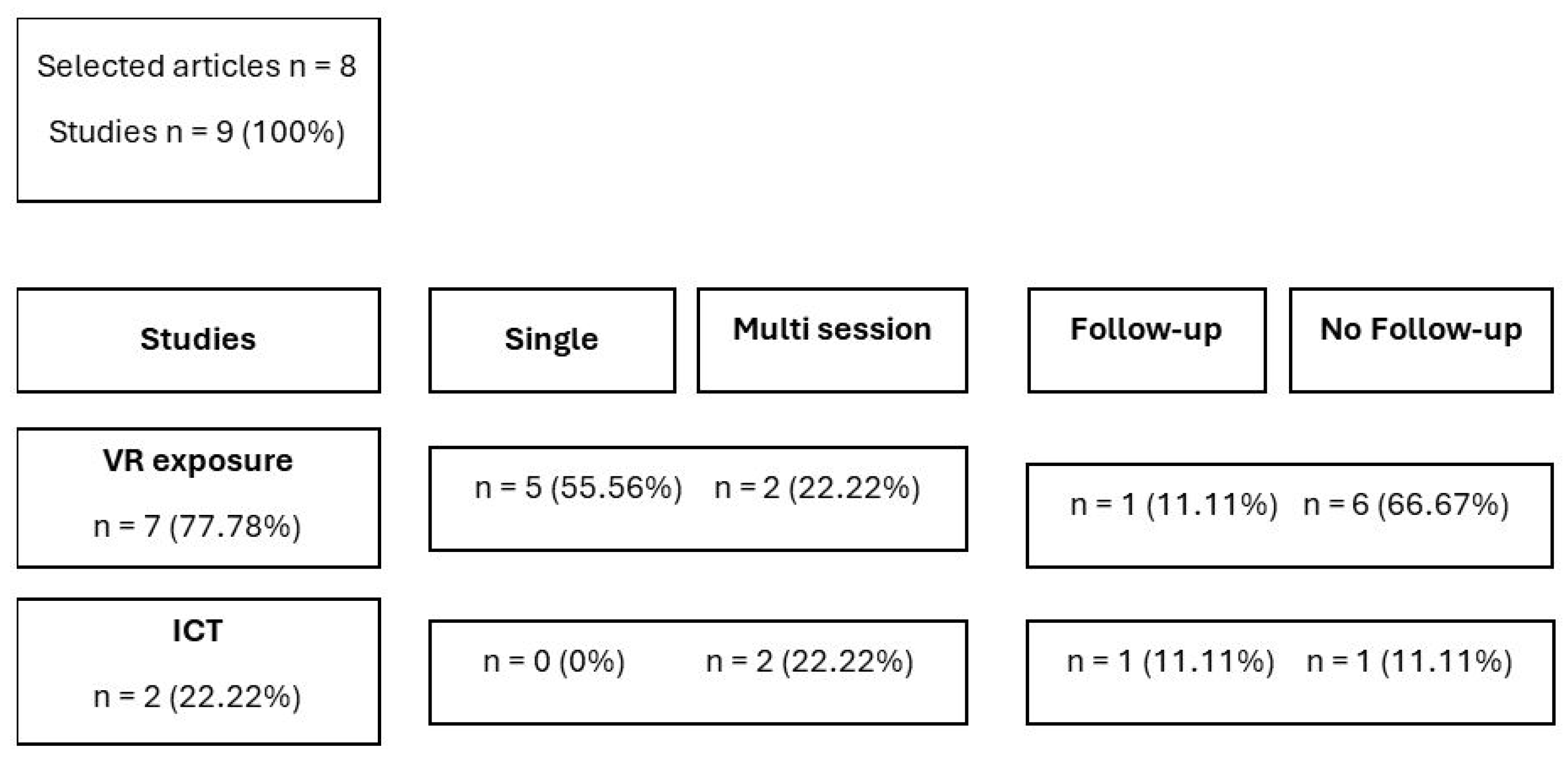
3.1. Articles Description
3.2. Quality Analyses
3.3. VR Exposure Intervention
3.4. VR-ICT Intervention
4. Discussion
4.1. Effectiveness of VR Exposure Intervention
4.2. Effectiveness of VR-ICT Intervention
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Hilty, D.M.; Randhawa, K.; Maheu, M.M.; McKean, A.J.S.; Pantera, R.; Mishkind, M.C.; Rizzo, A. A Review of Telepresence, Virtual Reality, and Augmented Reality Applied to Clinical Care. J. Technol. Behav. Sci. 2020, 5, 178–205. [Google Scholar] [CrossRef]
- Cieślik, B.; Mazurek, J.; Rutkowski, S.; Kiper, P.; Turolla, A.; Szczepańska-Gieracha, J. Virtual Reality in Psychiatric Disorders: A Systematic Review of Reviews. Complement. Ther. Med. 2020, 52, 102480. [Google Scholar] [CrossRef]
- Clus, D.; Larsen, M.E.; Lemey, C.; Berrouiguet, S. The Use of Virtual Reality in Patients with Eating Disorders: Systematic Review. J. Med. Internet Res. 2018, 20, e157. [Google Scholar] [CrossRef]
- Rauschnabel, P.A.; Felix, R.; Hinsch, C.; Shahab, H.; Alt, F. What Is XR? Towards a Framework for Augmented and Virtual Reality. Comput. Human Behav. 2022, 133, 107289. [Google Scholar] [CrossRef]
- Riva, G.; Malighetti, C.; Serino, S. Virtual Reality in the Treatment of Eating Disorders. Clin. Psychol. Psychother. 2021, 28, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Ciążyńska, J.; Maciaszek, J. Various Types of Virtual Reality-Based Therapy for Eating Disorders: A Systematic Review. J. Clin. Med. 2022, 11, 4956. [Google Scholar] [CrossRef]
- Silén, Y.; Keski-Rahkonen, A. Worldwide Prevalence of DSM-5 Eating Disorders among Young People. Curr. Opin. Psychiatry 2022, 35, 362–371. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 0-89042-555-8. [Google Scholar]
- American Psychiatric Association. The American Psychiatric Association Practice Guideline for the Treatment of Patients with Eating Disorders; American Psychiatric Association Publishing: Washington, DC, USA, 2023; ISBN 0-89042-584-1. [Google Scholar]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality Rates in Patients With Anorexia Nervosa and Other Eating Disorders. Arch. Gen. Psychiatry 2011, 68, 724. [Google Scholar] [CrossRef]
- Micali, N.; Martini, M.G.; Thomas, J.J.; Eddy, K.T.; Kothari, R.; Russell, E.; Bulik, C.M.; Treasure, J. Lifetime and 12-Month Prevalence of Eating Disorders amongst Women in Mid-Life: A Population-Based Study of Diagnoses and Risk Factors. BMC Med. 2017, 15, 12. [Google Scholar] [CrossRef]
- Tanner, A.B. Unique Considerations for the Medical Care of Restrictive Eating Disorders in Children and Young Adolescents. J. Eat. Disord. 2023, 11, 33. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Bailey-Straebler, S.; Basden, S.; Doll, H.A.; Jones, R.; Murphy, R.; O’Connor, M.E.; Cooper, Z. A Transdiagnostic Comparison of Enhanced Cognitive Behaviour Therapy (CBT-E) and Interpersonal Psychotherapy in the Treatment of Eating Disorders. Behav. Res. Ther. 2015, 70, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Södersten, P.; Bergh, C.; Leon, M.; Brodin, U.; Zandian, M. Cognitive Behavior Therapy for Eating Disorders versus Normalization of Eating Behavior. Physiol. Behav. 2017, 174, 178–190. [Google Scholar] [CrossRef]
- Zipfel, S.; Giel, K.E.; Bulik, C.M.; Hay, P.; Schmidt, U. Anorexia Nervosa: Aetiology, Assessment, and Treatment. Lancet Psychiatry 2015, 2, 1099–1111. [Google Scholar] [CrossRef]
- Lock, J.; Le Grange, D. Family-based Treatment: Where Are We and Where Should We Be Going to Improve Recovery in Child and Adolescent Eating Disorders. Int. J. Eat. Disord. 2019, 52, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Keizer, A.; van Elburg, A.; Helms, R.; Dijkerman, H.C. A Virtual Reality Full Body Illusion Improves Body Image Disturbance in Anorexia Nervosa. PLoS ONE 2016, 11, e0163921. [Google Scholar] [CrossRef]
- Porras-Garcia, B.; Ferrer-Garcia, M.; Serrano-Troncoso, E.; Carulla-Roig, M.; Soto-Usera, P.; Miquel-Nabau, H.; Shojaeian, N.; de la Montaña Santos-Carrasco, I.; Borszewski, B.; Díaz-Marsá, M.; et al. Validity of Virtual Reality Body Exposure to Elicit Fear of Gaining Weight, Body Anxiety and Body-Related Attentional Bias in Patients with Anorexia Nervosa. J. Clin. Med. 2020, 9, 3210. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Garcia, M.; Pla-Sanjuanelo, J.; Dakanalis, A.; Vilalta-Abella, F.; Riva, G.; Fernandez-Aranda, F.; Forcano, L.; Riesco, N.; Sánchez, I.; Clerici, M.; et al. A Randomized Trial of Virtual Reality-Based Cue Exposure Second-Level Therapy and Cognitive Behavior Second-Level Therapy for Bulimia Nervosa and Binge-Eating Disorder: Outcome at Six-Month Followup. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 60–68. [Google Scholar] [CrossRef]
- Nameth, K.; Brown, T.; Bullock, K.; Adler, S.; Riva, G.; Safer, D.; Runfola, C. Translating Virtual Reality Cue Exposure Therapy for Binge Eating into a Real-World Setting: An Uncontrolled Pilot Study. J. Clin. Med. 2021, 10, 1511. [Google Scholar] [CrossRef]
- Matsangidou, M.; Otkhmezuri, B.; Ang, C.S.; Avraamides, M.; Riva, G.; Gaggioli, A.; Iosif, D.; Karekla, M. “Now I Can See Me” Designing a Multi-User Virtual Reality Remote Psychotherapy for Body Weight and Shape Concerns. Hum. Comput. Interact. 2022, 37, 314–340. [Google Scholar] [CrossRef]
- Manasse, S.M.; Lampe, E.W.; Juarascio, A.S.; Zhu, J.; Forman, E.M. Using Virtual Reality to Train Inhibitory Control and Reduce Binge Eating: A Proof-of-Concept Study. Appetite 2021, 157, 104988. [Google Scholar] [CrossRef]
- Vlahovic, S.; Suznjevic, M.; Skorin-Kapov, L. A Survey of Challenges and Methods for Quality of Experience Assessment of Interactive VR Applications. J. Multimodal User Interfaces 2022, 16, 257–291. [Google Scholar] [CrossRef]
- Dane, A.; Bhatia, K. The Social Media Diet: A Scoping Review to Investigate the Association between Social Media, Body Image and Eating Disorders amongst Young People. PLoS Glob. Public Health 2023, 3, e0001091. [Google Scholar] [CrossRef] [PubMed]
- Gusenbauer, M.; Haddaway, N.R. Which Academic Search Systems Are Suitable for Systematic Reviews or Meta-analyses? Evaluating Retrieval Qualities of Google Scholar, PubMed, and 26 Other Resources. Res. Synth. Methods 2020, 11, 181–217. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; the PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Behrens, S.C.; Tesch, J.; Sun, P.J.B.; Starke, S.; Black, M.J.; Schneider, H.; Pruccoli, J.; Zipfel, S.; Giel, K.E. Virtual Reality Exposure to a Healthy Weight Body Is a Promising Adjunct Treatment for Anorexia Nervosa. Psychother. Psychosom. 2023, 92, 170–179. [Google Scholar] [CrossRef]
- Ascione, M.; Carulla-Roig, M.; Miquel-Nabau, H.; Porras-Garcia, B.; Meschberger-Annweiler, F.-A.; Serrano-Troncoso, E.; Ferrer-Garcia, M.; Moreno-Sánchez, M.; Gutierrez-Maldonado, J. Attentional Bias Modification Training Based on Virtual Reality and Eye Tracking in Anorexia Nervosa Patients. J. Clin. Med. 2023, 12, 5932. [Google Scholar] [CrossRef]
- Manasse, S.M.; Trainor, C.; Payne-Reichert, A.; Abber, S.R.; Lampe, E.W.; Gillikin, L.M.; Juarascio, A.S.; Forman, E.M. Does Virtual Reality Enhance the Effects of Inhibitory Control Training for Loss-of-Control Eating? A Pilot Factorial Experiment. Eat. Behav. 2023, 50, 101749. [Google Scholar] [CrossRef]
- Max, S.M.; Schag, K.; Giel, K.E.; Plewnia, C. Behavioural Biases in the Interaction with Food Objects in Virtual Reality and Its Clinical Implication for Binge Eating Disorder. Eat. Weight Disord. 2023, 28, 46. [Google Scholar] [CrossRef]
- Meschberger-Annweiler, F.-A.; Ascione, M.; Porras-Garcia, B.; Ferrer-Garcia, M.; Moreno-Sanchez, M.; Miquel-Nabau, H.; Serrano-Troncoso, E.; Carulla-Roig, M.; Gutiérrez-Maldonado, J. An Attentional Bias Modification Task, through Virtual Reality and Eye-Tracking Technologies, to Enhance the Treatment of Anorexia Nervosa. J. Clin. Med. 2023, 12, 2185. [Google Scholar] [CrossRef]
- Miquel-Nabau, H.; Briseño-Oloriz, N.; Porras-Garcia, B.; Ascione, M.; Meschberger-Annweiler, F.-A.; Ferrer-Garcia, M.; Moreno-Sanchez, M.; Serrano-Troncoso, E.; Carulla-Roig, M.; Gutiérrez Maldonado, J. Modification of Body-Related Attentional Bias through Virtual Reality and Eye-Tracking in Healthy Participants: Implications for Anorexia Nervosa Treatments. Brain Sci. 2023, 13, 764. [Google Scholar] [CrossRef] [PubMed]
- Natali, L.; Meregalli, V.; Rowlands, K.; Di Pietro, J.; Treasure, J.; Collantoni, E.; Meneguzzo, P.; Tenconi, E.; Favaro, A.; Fontana, F.; et al. Virtual Food Exposure with Positive Mood Induction or Social Support to Reduce Food Anxiety in Anorexia Nervosa: A Feasibility Study. Int. J. Eat. Disord. 2024, 57, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Sansoni, M.; Varallo, G.; Malighetti, C.; Tuena, C.; Di Lernia, D.; Cesa, G.L.; Manzoni, G.M.; Castelnuovo, G.; Riva, G. Unlocking the Potential of Virtual Reality to Expand Treatment Frontiers for Bulimia Nervosa: A Pilot Study to Explore the Impact of Virtual Reality-Enhanced Cognitive-Behavioral Therapy. Virtual Real. 2024, 28, 79. [Google Scholar] [CrossRef]
- Dondzilo, L.; Basanovic, J.; Grafton, B.; Bell, J.; Turnbull, G.; MacLeod, C. A Serial Mediation Model of Attentional Engagement with Thin Bodies on Body Dissatisfaction: The Role of Appearance Comparisons and Rumination. Curr. Psychol. 2023, 42, 1896–1904. [Google Scholar] [CrossRef]
- Williamson, D.A.; White, M.A.; York-Crowe, E.; Stewart, T.M. Cognitive-Behavioral Theories of Eating Disorders. Behav. Modif. 2004, 28, 711–738. [Google Scholar] [CrossRef]
- Lindner, P. Better, Virtually: The Past, Present, and Future of Virtual Reality Cognitive Behavior Therapy. Int. J. Cogn. Ther. 2021, 14, 23–46. [Google Scholar] [CrossRef]
- Tang, W.S.W.; Ng, T.J.Y.; Wong, J.Z.A.; Ho, C.S.H. The Role of Serious Video Games in the Treatment of Disordered Eating Behaviors: Systematic Review. J. Med. Internet Res. 2022, 24, e39527. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| ED | Description |
|---|---|
| Anorexia nervosa | It is characterized by an intense fear of gaining weight and a distorted body image. Individuals with anorexia often restrict their food intake severely, leading to significant weight loss and malnutrition |
| Bulimia nervosa | Involves cycles of binge eating followed by compensatory behaviors such as self-induced vomiting, excessive exercise, or misuse of laxatives |
| Binge eating disorder | It is characterized by recurrent episodes of eating large quantities of food, often quickly and to the point of discomfort. There are no regular compensatory behaviors to counteract binge eating |
| Author | Sample | Method | Measures | Main Findings |
|---|---|---|---|---|
| Ascione et al. [29] | 23 AN, Mean age (SD): 15.30 (1.29), 100% Female | All participants underwent a single session of ABMT intervention in VR. | BD, CFT, NF | Significant post-intervention reductions in BD and time spent fixating on weight-related areas (CFT). |
| Behrens et al. [28] | Study 1: 20 high weight/shape concern, Mean age (SD): 26.36 (6.54), 100% Female Study 2: 20 AN, Mean age (SD): 30.1 (11.9), 100% Female | Study 1: Single session of psychoeducation and VR avatar exposure with 30% weight gain. Study 2: Five sessions: one educational and four VR avatar exposure with average body shape. | Study 1: BD, FGW, HRV Study 2: Arousal, BD, FGW, HRV, Salivary cortisol | Study 1: No significant changes in pre- and post-VR exposure. Study 2: Significant reduction in FGW post-VR but no session-to-session differences. |
| Manasse et al. [30] | VR-ICT: 8 BED, Non-VR-ICT: 7 BED, VR-sham *: 11 BED, Non-VR-sham *: 9 BED, 91.4% Female, 8.6% Male | Participants were randomly assigned to a 6-week training course with 3-month follow-up. | FC, UA, IAT, Last latency | Significant decrease in FC over time in all groups, but no significant differences in behavioral outcomes between groups. |
| Max et al. [31] | 31 BED, Mean age (SD): 36.26 (13.37), 77.42% Female, 22.58% Male | Participants underwent a 2-week VR-based ICT with tDCS applied to the right dorsolateral prefrontal cortex. | ED symptoms, FC, Impulsivity, TFEQ, RT | No modulatory effect of tDCS observed. Significant reduction in ED psychopathology and BED episodes post-training. |
| Meschberger-Annweiler et al. [32] | 58 Healthy, Mean age (SD): 24.83 (6.64), 100% Female | Participants completed four blocks of VR-based ABMT in one session. Pre-AB CFT and NF measures used to categorize participants into W-AB and NW-AB groups. | UA, CFT, NF | Both the NW-AB and W-AB groups required two blocks of ABMT to reduce their bias in CFT, achieving a more balanced focus. The NW-AB group also needed two blocks to decrease their NF bias, while the W-AB group required three blocks to reduce NF bias, followed by an increase in NF during the fourth block. |
| Miquel-Nabau et al. [33] | NW-AB: 13 Healthy, Mean age (SD): 22.5 (1.72) No-AB: 28 Healthy, Mean age (SD): 23 (1.77) W-AB: 13 Healthy, Mean age (SD): 23.27 (2.22) 100% Female | All participants underwent a single session of ABMT in VR, split into groups based on pre-AB measures. | BD, FGW, PASTAS, CFT, NF | W-AB and NW-AB groups significantly reduced attentional biases, moving toward more balanced CFT and NF measures post-ABMT. |
| Natali et al. [34] | Baseline *: 50 AN, Social support: 46 AN, Positive mood: 49 AN, Mean age (SD): 21.75 (6.68), 96.43% Female, 1.43% Males, 2.14% Other gender | Participants were randomly assigned to one of three VR conditions (baseline, social support, positive mood). | Anxiety, DASS-21, ED, Food-related anxiety, Hunger, Perceived social support, Positive mood, NF, N touches | The positive mood group showed less food-related anxiety during VR and post-VR compared to the baseline group, which exhibited more food-related anxiety post-exposure. |
| Sansoni et al. [35] | TAU *: 12 BN, Mean age (SD): 28.83 (6.48) VR-CBT: 12 BN, Mean age (SD): 29.25 (7.75) 100% Female | Participants were randomized to either TAU (5-week multimodal intervention with CBT) or VR-CBT (five CBT sessions and 10 VR sessions). Psychological measures followed up at 1 month and BMI at 3, 6, 9, and 12 months. | BD, ED symptoms, FGW, BMI | VR-CBT group showed greater reduction in weight preoccupation, FGW, binge eating, and purging, with more stable BMI post-treatment compared to TAU group. |
| Author | D1 | D2 | D3 | D4 | D5 | General Risk of Bias |
|---|---|---|---|---|---|---|
| Ascione et al. [29] | Some concerns | Low | Low | Low | Low | Some concerns |
| Behrens et al. [28] Study 1 | Some concerns | Low | Low | Low | Low | Some concerns |
| Behrens et al. [28] Study 2 | Some concerns | Low | Low | Low | Low | Some concerns |
| Manasse et al. [30] | Low | Low | Low | Low | Low | Low risk |
| Max et al. [31] | Some concerns | Low | Low | Low | Some concerns | Some concerns |
| Meschberger-Annweiler et al. [32] | Some concerns | Low | Low | Low | Low | Some concerns |
| Miquel-Nabau et al. [33] | Some concerns | Low | Low | Low | Low | Some concerns |
| Natali et al. [34] | Low | Low | Low | Low | Low | Low risk |
| Sansoni et al. [35] | Some concerns | Low | Low | Low | Low | Some concerns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arrom-Llabrés, M.; Mendoza-Medialdea, M.T.; Gutiérrez-Maldonado, J. Innovative Approaches to Eating Disorders Treatment: A Systematic Review on the Effectiveness of Virtual Reality. Appl. Sci. 2025, 15, 3334. https://doi.org/10.3390/app15063334
Arrom-Llabrés M, Mendoza-Medialdea MT, Gutiérrez-Maldonado J. Innovative Approaches to Eating Disorders Treatment: A Systematic Review on the Effectiveness of Virtual Reality. Applied Sciences. 2025; 15(6):3334. https://doi.org/10.3390/app15063334
Chicago/Turabian StyleArrom-Llabrés, Mariona, María Teresa Mendoza-Medialdea, and José Gutiérrez-Maldonado. 2025. "Innovative Approaches to Eating Disorders Treatment: A Systematic Review on the Effectiveness of Virtual Reality" Applied Sciences 15, no. 6: 3334. https://doi.org/10.3390/app15063334
APA StyleArrom-Llabrés, M., Mendoza-Medialdea, M. T., & Gutiérrez-Maldonado, J. (2025). Innovative Approaches to Eating Disorders Treatment: A Systematic Review on the Effectiveness of Virtual Reality. Applied Sciences, 15(6), 3334. https://doi.org/10.3390/app15063334