

The Feasibility and User Experience of a Program of Progressive Cued Activity to Promote Functional Upper Limb Activity in the Inpatient Rehabilitation Setting with Follow-Up at Home
 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
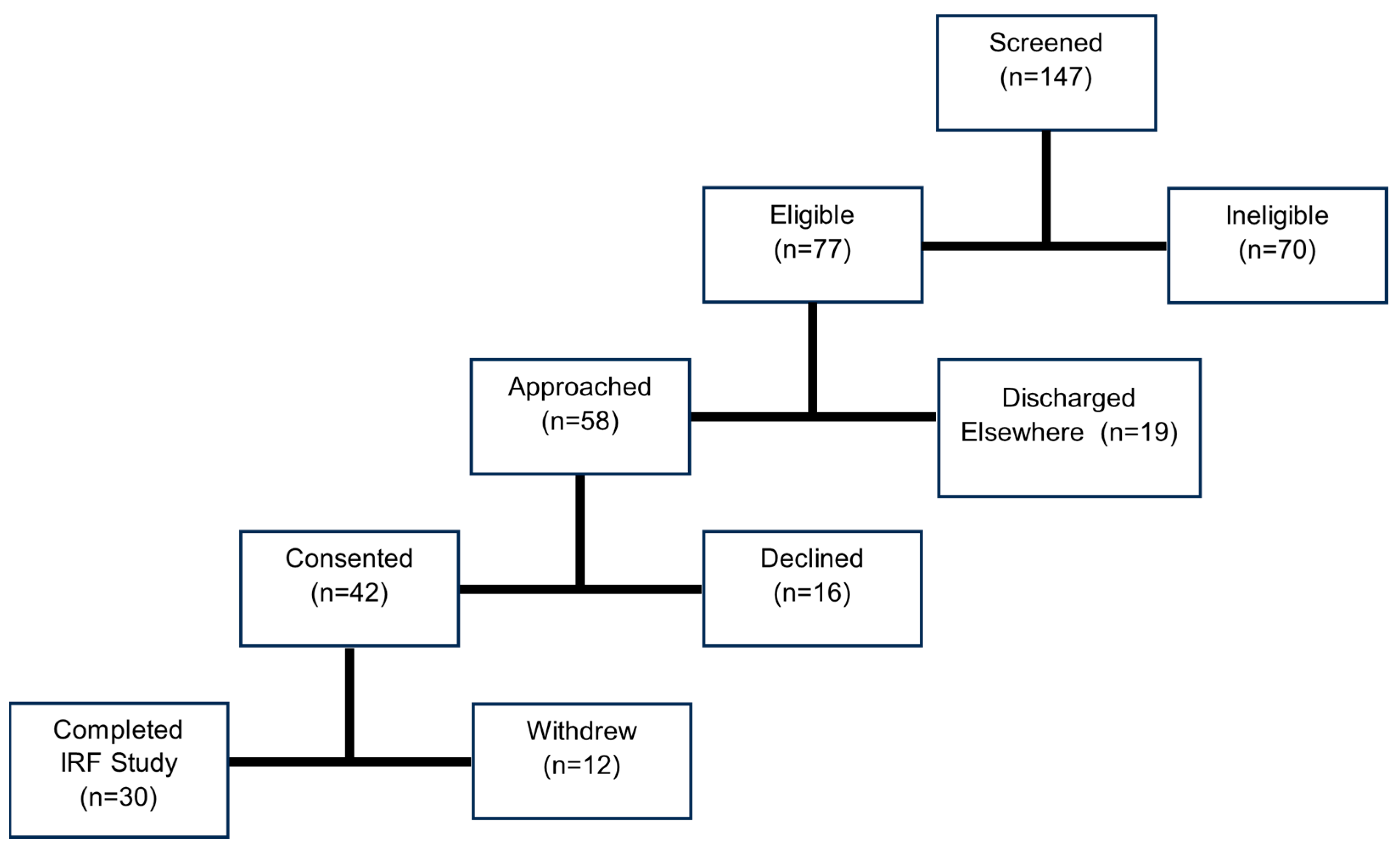
2.1. Participant Recruitment
2.2. Materials
2.3. Experimental Protocol
2.3.1. Baseline Assessment Phase
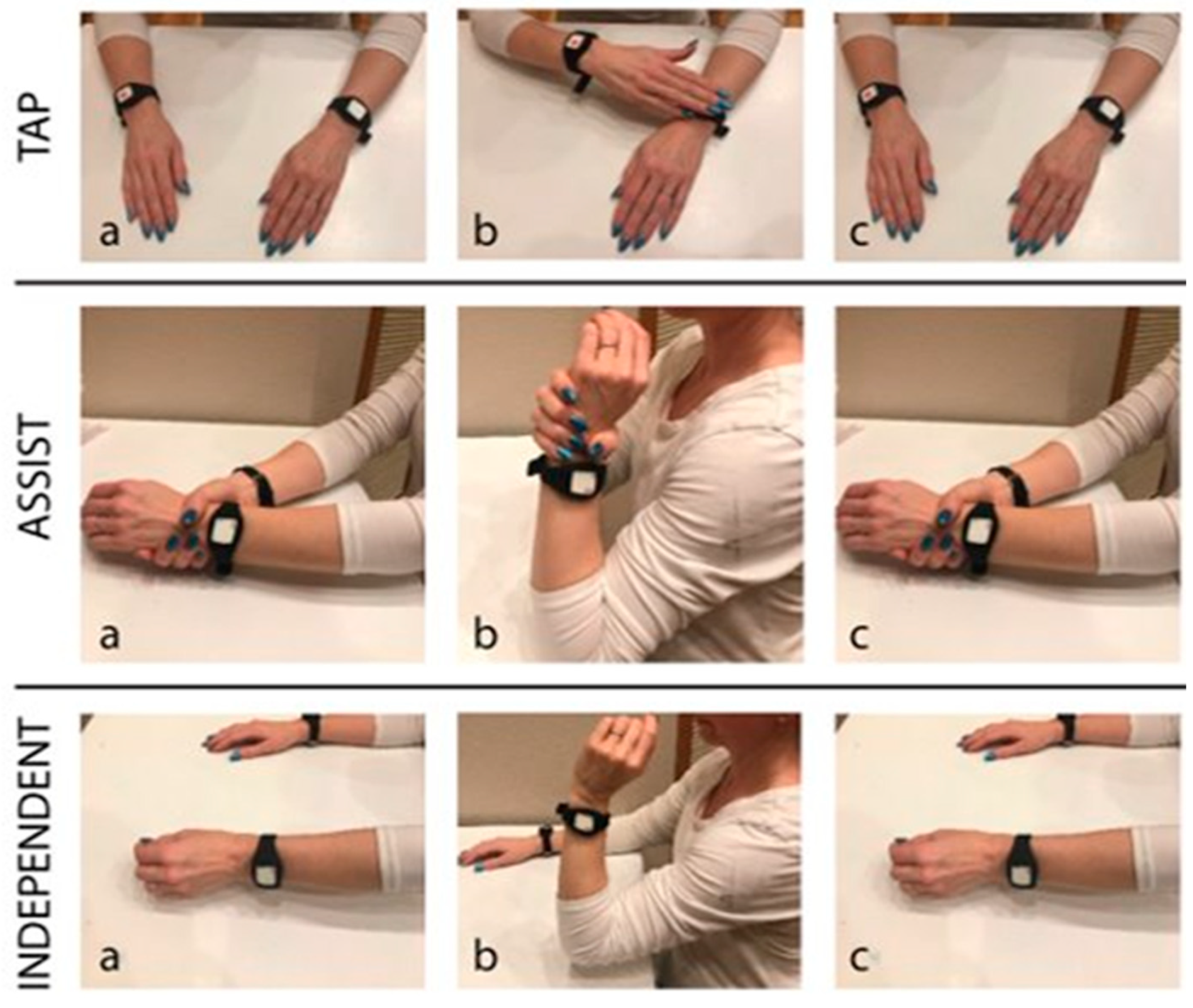
2.3.2. IRF Feasibility Testing Phase: Progressive-Challenge Cue Activity Program and Passive Activity Monitoring
2.3.3. Final Day Prior to Discharge from IRF
2.3.4. Follow-Up Phase at Home: Attrition and Passive Activity Monitoring
2.3.5. Data Curation and Analysis
2.3.6. Statistical Hypothesis Testing
3. Results
3.1. Feasibility and User Experience in an Inpatient Rehabilitation Facility
3.1.1. Compliance
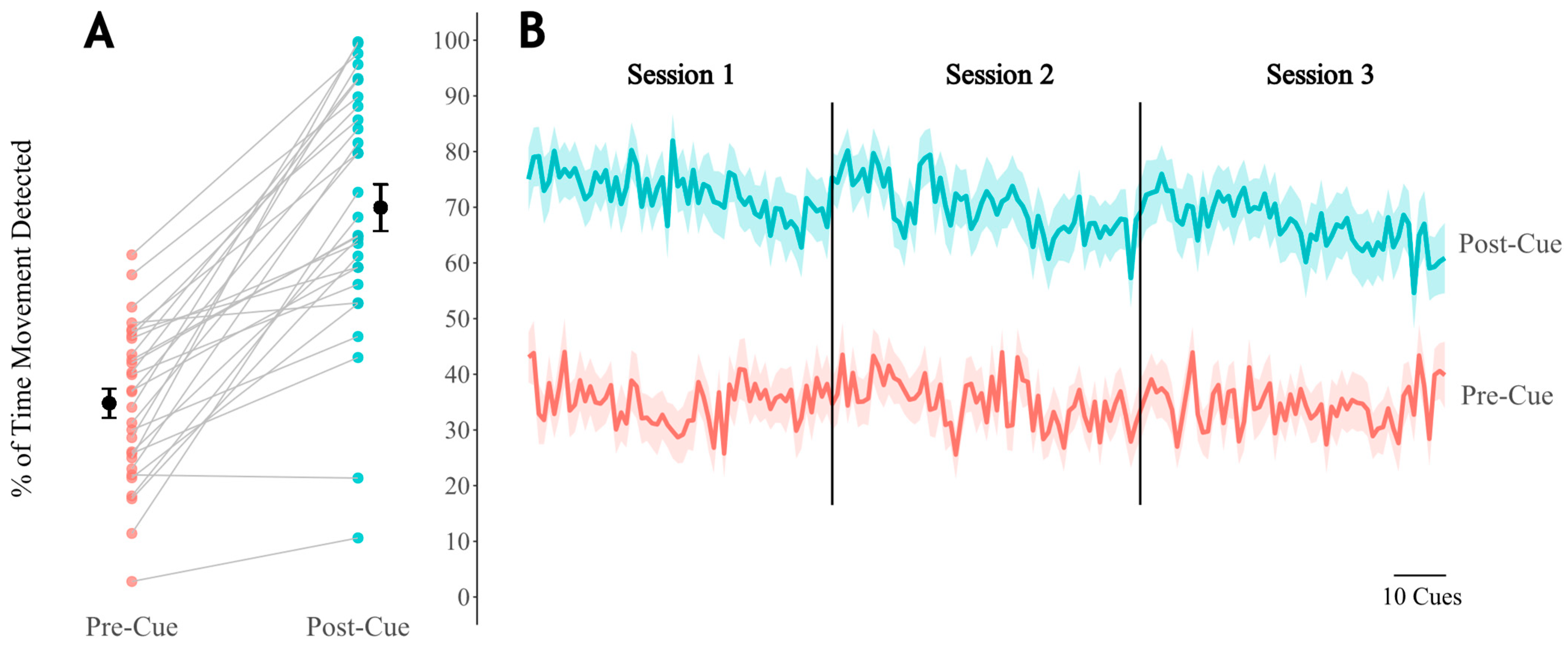
3.1.2. Cue Response Rate
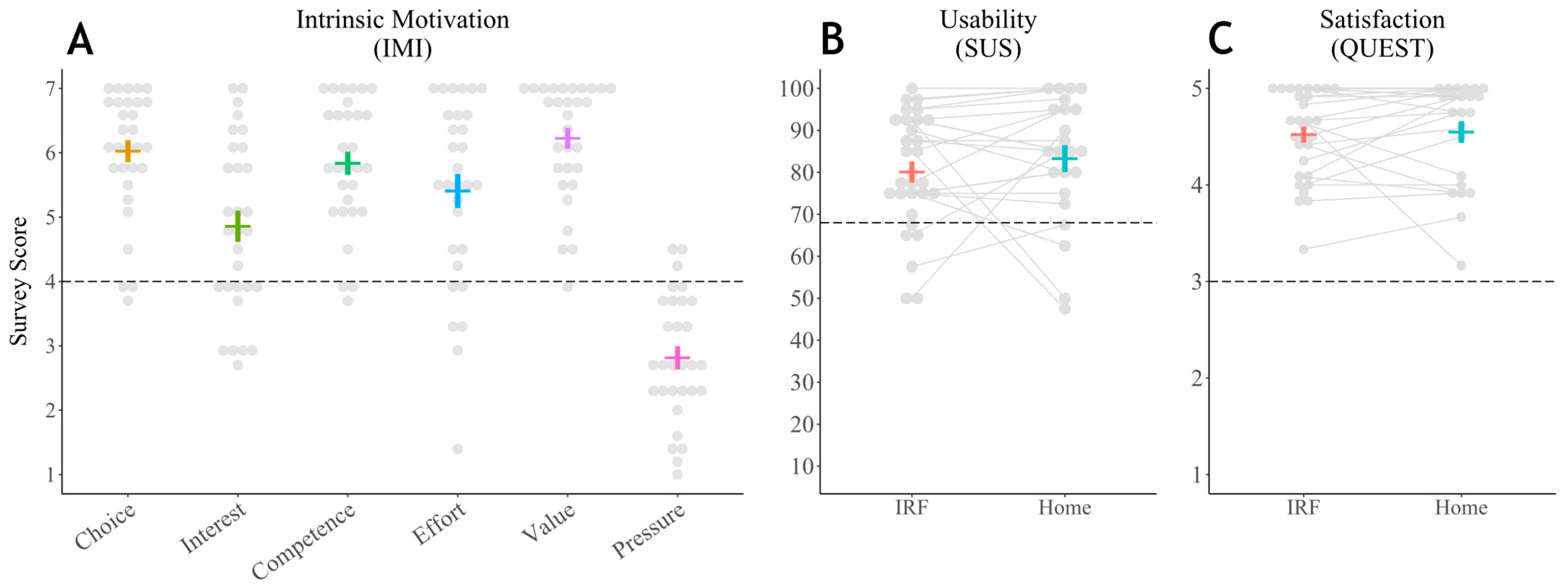
3.1.3. User Experience Surveys
3.2. Feasibility and User Experience During Follow-Up at Home
3.2.1. Compliance
3.2.2. User Experience Surveys
4. Discussion
4.1. Reclaiming Lost Opportunities: Current Approaches to Subacute Rehabilitation
4.2. Opportunities and Future Directions
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADLs | Activities of daily living. |
| IRF | Inpatient rehabilitation facility. |
| MI | More involved. |
| LI | Less involved. |
| CIMT | Constraint induced movement therapy. |
| MoCA | Montreal Cognitive Assessment. |
| FMA-UE | Fugl Meyer Assessment—Upper Extremity. |
| SUS | System Usability Scale. |
| QUEST | Quebec User Experience and Satisfaction with Assistive Technology. |
| IMI | Intrinsic Motivation Inventory. |
Appendix A
References
- Martin, S.S.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Barone Gibbs, B.; Beaton, A.Z.; Boehme, A.K.; et al. 2024 Heart Disease and Stroke Statistics: A Report of US and Global Data from the American Heart Association. Circulation 2024, 149, E347–E913. [Google Scholar] [CrossRef] [PubMed]
- Ananth, C.V.; Brandt, J.S.; Keyes, K.M.; Graham, H.L.; Kostis, J.B.; Kostis, W.J. Epidemiology and Trends in Stroke Mortality in the USA, 1975–2019. Int. J. Epidemiol. 2023, 52, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Kwakkel, G.; Kollen, B.J.; Wagenaar, R.C. Therapy Impact on Functional Recovery in Stroke Rehabilitation: A Critical Review of the Literature. Physiotherapy 1999, 85, 377–391. [Google Scholar] [CrossRef]
- Lawrence, E.S.; Coshall, C.; Dundas, R.; Stewart, J.; Rudd, A.G.; Howard, R.; Wolfe, C.D.A. Estimates of the Prevalence of Acute Stroke Impairments and Disability in a Multiethnic Population. Stroke 2001, 32, 1279–1284. [Google Scholar] [CrossRef]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed Definitions and a Shared Vision for New Standards in Stroke Recovery Research: The Stroke Recovery and Rehabilitation Roundtable Taskforce. Int. J. Stroke 2017, 12, 444–450. [Google Scholar] [CrossRef]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery. Stroke 2016, 47, E98–E169. [Google Scholar] [CrossRef]
- Lang, C.E.; MacDonald, J.R.; Reisman, D.S.; Boyd, L.; Jacobson Kimberley, T.; Schindler-Ivens, S.M.; Hornby, T.G.; Ross, S.A.; Scheets, P.L. Observation of Amounts of Movement Practice Provided During Stroke Rehabilitation. Arch. Phys. Med. Rehabil. 2009, 90, 1692–1698. [Google Scholar] [CrossRef]
- Wyller, T.B.; Sveen, U.; Sedring, K.M.; Pettersen, A.M.; Bautz-Holter, E. Subjective Well-Being One Year after Stroke. Clin. Rehabil. 1997, 11, 139–145. [Google Scholar] [CrossRef]
- van Lieshout, E.C.C.; van de Port, I.G.; Dijkhuizen, R.M.; Visser-Meily, J.M.A. Does Upper Limb Strength Play a Prominent Role in Health-Related Quality of Life in Stroke Patients Discharged from Inpatient Rehabilitation? Top Stroke Rehabil. 2020, 27, 525–533. [Google Scholar] [CrossRef]
- Hubbard, I.J.; Parsons, M.W.; Neilson, C.; Carey, L.M. Task-Specific Training: Evidence for and Translation to Clinical Practice. Occup. Ther. Int. 2009, 16, 175–189. [Google Scholar] [CrossRef]
- Waddell, K.J.; Strube, M.J.; Bailey, R.R.; Klaesner, J.W.; Birkenmeier, R.L.; Dromerick, A.W.; Lang, C.E. Does Task-Specific Training Improve Upper Limb Performance in Daily Life Poststroke? Neurorehabil. Neural. Repair. 2017, 31, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Thomas, L.H.; French, B.; Coupe, J.; McMahon, N.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive Task Training for Improving Functional Ability after Stroke: A Major Update of a Cochrane Review. Stroke 2017, 48, e102–e103. [Google Scholar] [CrossRef]
- Newton, S.P.; Dalton, E.J.; Ang, J.Y.; Klaic, M.; Thijs, V.; Hayward, K.S. Dose, Content, and Context of Usual Care in Stroke Upper Limb Motor Interventions: A Systematic Review. Clin. Rehabil. 2023, 37, 1437–1450. [Google Scholar] [CrossRef] [PubMed]
- Hayward, K.S.; Brauer, S.G. Dose of Arm Activity Training during Acute and Subacute Rehabilitation Post Stroke: A Systematic Review of the Literature. Clin. Rehabil. 2015, 29, 1234–1243. [Google Scholar] [CrossRef]
- Taub, E.; Miller, N.E.; Novack, T.A.; Cook, E.W.; Fleming, W.C.; Nepomuceno, C.S.; Connell, J.S.; Crago, J.E. Technique to Improve Chronic Motor Deficit after Stroke. Arch. Phys. Med. Rehabil. 1993, 74, 347–354. [Google Scholar]
- Taub, E.; Uswatte, G.; Mark, V.W.; Morris, D.M. The Learned Nonuse Phenomenon: Implications for Rehabilitation. Eur. Medicophys. 2006, 42, 241–256. [Google Scholar]
- Taub, E.; Uswatte, G.; Mark, V.W.; Morris, D.M.; Barman, J.; Bowman, M.H.; Bryson, C.; Delgado, A.; Bishop-Mckay, S. Method for Enhancing Real-World Use of a More Affected Arm in Chronic Stroke: Transfer Package of Constraint-Induced Movement Therapy. Stroke 2013, 44, 1383–1388. [Google Scholar] [CrossRef]
- Wolf, S.L.; Winstein, C.J.; Miller, J.P.; Thompson, P.A.; Taub, E.; Uswatte, G.; Morris, D.; Blanton, S.; Nichols-Larsen, D.; Clark, P.C. Retention of Upper Limb Function in Stroke Survivors Who Have Received Constraint-Induced Movement Therapy: The EXCITE Randomised Trial. Lancet Neurol. 2008, 7, 33–40. [Google Scholar] [CrossRef]
- Pedlow, K.; Lennon, S.; Wilson, C. Application of Constraint-Induced Movement Therapy in Clinical Practice: An Online Survey. Arch. Phys. Med. Rehabil. 2014, 95, 276–282. [Google Scholar] [CrossRef]
- Childs, J.D.; Benz, L.N.; Arellano, A.; Briggs, A.A.; Walker, M.J. Challenging Assumptions about the Future Supply and Demand of Physical Therapists in the United States. Phys. Ther. 2022, 102, pzab239. [Google Scholar] [CrossRef]
- Patel, R.M.; Bartholomew, J. Impact of Job Resources and Job Demands on Burnout among Physical Therapy Providers. Int. J. Environ. Res. Public Health 2021, 18, 12521. [Google Scholar] [CrossRef] [PubMed]
- Sjöholm, A.; Skarin, M.; Churilov, L.; Nilsson, M.; Bernhardt, J.; Lindén, T. Sedentary Behaviour and Physical Activity of People with Stroke in Rehabilitation Hospitals. Stroke Res. Treat. 2014, 2014, 591897. [Google Scholar] [CrossRef] [PubMed]
- Hayward, K.S.; Eng, J.J.; Boyd, L.A.; Lakhani, B.; Bernhardt, J.; Lang, C.E. Exploring the Role of Accelerometers in the Measurement of Real World Upper-Limb Use after Stroke. Brain Impair. 2016, 17, 16–33. [Google Scholar] [CrossRef]
- Barth, J.; Lohse, K.R.; Konrad, J.D.; Bland, M.D.; Lang, C.E. Sensor-Based Categorization of Upper Limb Performance in Daily Life of Persons with and Without Neurological Upper Limb Deficits. Front. Rehabil. Sci. 2021, 2, 741393. [Google Scholar] [CrossRef]
- Held, J.P.; Klaassen, B.; van Beijnum, B.J.F.; Luft, A.R.; Veltink, P.H. Usability Evaluation of a VibroTactile Feedback System in Stroke Subjects. Front. Bioeng. Biotechnol. 2017, 4, 98. [Google Scholar] [CrossRef]
- Holden, A.; McNaney, R.; Balaam, M.; Thompson, R.; Hammerla, N.; Ploetz, T.; Jackson, D.; Price, C.; Brkic, L.; Olivier, P. CueS: Cueing for Upper Limb Rehabilitation in Stroke. In Proceedings of the British Computer Society Conference on Human-Computer Interaction 2015, Lincoln, UK, 13–17 July 2015; Association for Computing Machinery (ACM): New York, NY, USA, 2015. [Google Scholar]
- Horder, J.; Mrotek, L.A.; Casadio, M.; Bassindale, K.D.; McGuire, J.; Scheidt, R.A. Utility and Usability of a Wearable System and Progressive-Challenge Cued Exercise Program for Encouraging Use of the More Involved Arm at-Home after Stroke—A Feasibility Study with Case Reports. J. Neuroeng. Rehabil. 2024, 21, 66. [Google Scholar] [CrossRef]
- Schwerz de Lucena, D.; Rowe, J.B.; Okita, S.; Chan, V.; Cramer, S.C.; Reinkensmeyer, D.J. Providing Real-Time Wearable Feedback to Increase Hand Use after Stroke: A Randomized, Controlled Trial. Sensors 2022, 22, 6938. [Google Scholar] [CrossRef]
- Toh, S.F.M.; Gonzalez, P.C.; Fong, K.N.K. Usability of a Wearable Device for Home-Based Upper Limb Telerehabilitation in Persons with Stroke: A Mixed-Methods Study. Digit. Health 2023, 9, 1–15. [Google Scholar] [CrossRef]
- Chen, Y.A.; Demers, M.; Lewthwaite, R.; Schweighofer, N.; Monterosso, J.R.; Fisher, B.E.; Winstein, C. A Novel Combination of Accelerometry and Ecological Momentary Assessment for Post-Stroke Paretic Arm/Hand Use: Feasibility and Validity. J. Clin. Med. 2021, 10, 1328. [Google Scholar] [CrossRef]
- Kim, Y.; Jung, H.T.; Park, J.; Kim, Y.; Ramasarma, N.; Bonato, P.; Choe, E.K.; Lee, S.I. Towards the Design of a Ring Sensor-Based MHealth System to Achieve Optimal Motor Function in Stroke Survivors. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2019, 3, 138. [Google Scholar] [CrossRef]
- Da-Silva, R.H.; van Wijck, F.; Shaw, L.; Rodgers, H.; Balaam, M.; Brkic, L.; Ploetz, T.; Jackson, D.; Ladha, K.; Price, C.I. Prompting Arm Activity after Stroke: A Clinical Proof of Concept Study of Wrist-Worn Accelerometers with a Vibrating Alert Function. J. Rehabil. Assist. Technol. Eng. 2018, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.X.J.; Fong, K.N.K.; Chung, R.C.K.; Cheung, H.K.Y.; Chow, E.S.L. “Remind-to-Move” for Promoting Upper Extremity Recovery Using Wearable Devices in Subacute Stroke: A Multi-Center Randomized Controlled Study. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Langerak, A.J.; Regterschot, G.R.H.; Evers, M.; van Beijnum, B.J.F.; Meskers, C.G.M.; Selles, R.W.; Ribbers, G.M.; Bussmann, J.B.J. A Sensor-Based Feedback Device Stimulating Daily Life Upper Extremity Activity in Stroke Patients: A Feasibility Study. Sensors 2023, 23, 5868. [Google Scholar] [CrossRef] [PubMed]
- Signal, N.; Olsen, S.; Rashid, U.; McLaren, R.; Vandal, A.; King, M.; Taylor, D. Haptic Nudging Using a Wearable Device to Promote Upper Limb Activity during Stroke Rehabilitation: Exploring Diurnal Variation, Repetition, and Duration of Effect. Behav. Sci. 2023, 13, 995. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The Post-Stroke Hemiplegic Patient. 1. a Method for Evaluation of Physical Performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [CrossRef]
- Hamilton, G.F.; McDonald, C.; Chenier, T.C. Measurement of Grip Strength: Validity and Reliability of the Sphygmomanometer and Jamar Grip Dynamometer. J. Orthop. Sports Phys. Ther. 1992, 16, 215–219. [Google Scholar] [CrossRef]
- Brooke, J. SUS—A Quick and Dirty Usability Scale Usability and Context. In Usability Evaluation in Industry; Taylor & Francis: Abingdon, UK, 1996; pp. 189–194. [Google Scholar]
- Demers, L.; Weiss-Lambrou, R.; Ska, B. (Eds.) Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST): A New Outcome Measure; RESNA: Arlington, DC, USA, 1997. [Google Scholar]
- Demers, L.; Monette, M.; Lapierre, Y.; Arnold, D.L.; Wolfson, C. Reliability, Validity, and Applicability of the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0) for Adults with Multiple Sclerosis. Disabil. Rehabil. 2002, 24, 21–30. [Google Scholar] [CrossRef]
- McAuley, E.D.; Duncan, T.; Tammen, V.V. Psychometric Properties of the Intrinsic Motivation Inventoiy in a Competitive Sport Setting: A Confirmatory Factor Analysis. Res. Q. Exerc. Sport 1989, 60, 48–58. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)-A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Bailey, R.R.; Klaesner, J.W.; Lang, C.E. An Accelerometry-Based Methodology for Assessment of Real-World Bilateral Upper Extremity Activity. PLoS ONE 2014, 9, e103135. [Google Scholar] [CrossRef] [PubMed]
- Uswatte, G.; Taub, E. Constraint-Induced Movement Therapy: A Method for Harnessing Neuroplasticity to Treat Motor Disorders. Prog. Brain Res. 2013, 207, 379–401. [Google Scholar] [PubMed]
- Uswatte, G.; Giuliani, C.; Winstein, C.; Zeringue, A.; Hobbs, L.; Wolf, S.L. Validity of Accelerometry for Monitoring Real-World Arm Activity in Patients with Subacute Stroke: Evidence from the Extremity Constraint-Induced Therapy Evaluation Trial. Arch. Phys. Med. Rehabil. 2006, 87, 1340–1345. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of Time Spent in Sedentary Behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Powell, K.E.; Jakicic, J.M.; Troiano, R.P.; Piercy, K.; Tennant, B. Sedentary Behavior and Health: Update from the 2018 Physical Activity Guidelines Advisory Committee. Med. Sci. Sports Exerc. 2019, 51, 1227–1241. [Google Scholar] [CrossRef]
- Ashizawa, R.; Honda, H.; Take, K.; Yoshizawa, K.; Kameyama, Y.; Yamashita, S.; Wakabayashi, T.; Yoshimoto, Y. Post-Discharge Sedentary Behavior and Light-Intensity Physical Activity-Associated Stroke Recurrence in Patients with Minor Ischemic Stroke: A Preliminary Retrospective Observational Study. Physiother. Res. Int. 2024, 29, e2110. [Google Scholar] [CrossRef]
- Pate, R.R.; O’Neill, J.R.; Lobelo, F. The Evolving Definition of “Sedentary”. Exerc. Sport Sci. Rev. 2008, 36, 173–178. [Google Scholar] [CrossRef]
- Liampas, A.; Velidakis, N.; Georgiou, T.; Vadalouca, A.; Varrassi, G.; Hadjigeorgiou, G.M.; Tsivgoulis, G.; Zis, P. Prevalence and Management Challenges in Central Post-Stroke Neuropathic Pain: A Systematic Review and Meta-Analysis. Adv. Ther. 2020, 37, 3278–3291. [Google Scholar] [CrossRef]
- Chen, W.; Jiang, T.; Huang, H.; Zeng, J. Post-Stroke Fatigue: A Review of Development, Prevalence, Predisposing Factors, Measurements, and Treatments. Front. Neurol. 2023, 14, 1298915. [Google Scholar] [CrossRef]
- Miller, K.K.; Porter, R.E.; DeBaun-Sprague, E.; Van Puymbroeck, M.; Schmid, A.A. Exercise after Stroke: Patient Adherence and Beliefs after Discharge from Rehabilitation. Top. Stroke Rehabil. 2017, 24, 142–148. [Google Scholar] [CrossRef]
- Deterding, S.; Dixon, D.; Khaled, R.; Nacke, L. From Game Design Elements to Gamefulness: Defining “Gamification”. In Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments, MindTrek 2011, Tampere, Finland, 28–30 September 2011. [Google Scholar]
- Sweetser, P.; Wyeth, P. GameFlow: A Model for Evaluating Player Enjoyment in Games. Comput. Entertain. 2005, 3, 3. [Google Scholar] [CrossRef]
- Shah, N.; Basteris, A.; Amirabdollahian, F. Design Parameters in Multimodal Games for Rehabilitation. Games Health J. 2014, 3, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Duarte, J.E.; Baur, K.; Riener, R. Flowing to the Optimal Challenge: An Adaptive Challenge Framework for Multiplayer Games. In Biosystems and Biorobotics; Springer: Berlin/Heidelberg, Germany, 2017; Volume 15. [Google Scholar]
- Nirme, J.; Duff, A.; Verschure, P.F.M.J. Adaptive Rehabilitation Gaming System: On-Line Individualization of Stroke Rehabilitation. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Boston, MA, USA, 30 August–3 September 2011. [Google Scholar]
- Pinto, J.F.; Carvalho, H.R.; Chambel, G.R.R.; Ramiro, J.; Gonçalves, A. Adaptive Gameplay and Difficulty Adjustment in a Gamified Upper-Limb Rehabilitation. In Proceedings of the 2018 IEEE 6th International Conference on Serious Games and Applications for Health, SeGAH 2018, Vienna, Austria, 16–18 May 2018. [Google Scholar]
- Rossol, N.; Cheng, I.; Bischof, W.F.; Basu, A. A Framework for Adaptive Training and Games in Virtual Reality Rehabilitation Environments. In Proceedings of the VRCAI 2011: 10th International Conference on Virtual-Reality Continuum and its Applications to Industry, Hong Kong, China, 11–12 December 2011. [Google Scholar]
- Missura, O. Dynamic Difficulty Adjustment. Ph.D. Thesis, Rheinische Friedrich-Wilhelms-Universität Bonn, Bonn, Germany, 2015. [Google Scholar]
- Lee, S.I.; Adans-Dester, C.P.; Grimaldi, M.; Dowling, A.V.; Horak, P.C.; Black-Schaffer, R.M.; Bonato, P.; Gwin, J.T. Enabling Stroke Rehabilitation in Home and Community Settings: A Wearable Sensor-Based Approach for Upper-Limb Motor Training. IEEE J. Transl. Eng. Health Med. 2018, 6, 2100411. [Google Scholar] [CrossRef] [PubMed]
- Seo, N.J.; Coupland, K.; Finetto, C.; Scronce, G. Wearable Sensor to Monitor Quality of Upper Limb Task Practice for Stroke Survivors at Home. Sensors 2024, 24, 554. [Google Scholar] [CrossRef]
- Khan, A.; Hammerla, N.; Mellor, S.; Plötz, T. Optimising Sampling Rates for Accelerometer-Based Human Activity Recognition. Pattern Recognit. Lett. 2016, 73, 33–40. [Google Scholar] [CrossRef]
- Nguyen, B.; Coelho, Y.; Bastos, T.; Krishnan, S. Trends in Human Activity Recognition with Focus on Machine Learning and Power Requirements. Mach. Learn. Appl. 2021, 5, 100072. [Google Scholar] [CrossRef]
- McGill, K.; Sackley, C.M.; Godwin, J.; McGarry, J.; Brady, M.C. A Systematic Review of the Efficiency of Recruitment to Stroke Rehabilitation Randomised Controlled Trials. Trials 2020, 21, 68. [Google Scholar] [CrossRef]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of Accelerometer Wear and Nonwear Time Classification Algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 30 | Age (Years) | Days in IRF | FMA-UE Motor | FMA-UE Sensory | MoCA |
| Mean | 61.1 | 13.3 | 45.6 | 11.5 | 25.9 |
| Minimum | 25 | 7 | 2 | 5 | 16 |
| Median | 60.5 | 13 | 61 | 12 | 26.5 |
| Maximum | 82 | 26 | 66 | 12 | 30 |
| Standard Deviation | 14.8 | 5.2 | 25.1 | 1.7 | 4.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bassindale, K.; Golus, S.; Horder, J.; Winkoski, M.; Sytsma, M.; Morelli, W.A.; Casadio, M.; McGuire, J.; Scheidt, R.A. The Feasibility and User Experience of a Program of Progressive Cued Activity to Promote Functional Upper Limb Activity in the Inpatient Rehabilitation Setting with Follow-Up at Home. Appl. Sci. 2025, 15, 3010. https://doi.org/10.3390/app15063010
Bassindale K, Golus S, Horder J, Winkoski M, Sytsma M, Morelli WA, Casadio M, McGuire J, Scheidt RA. The Feasibility and User Experience of a Program of Progressive Cued Activity to Promote Functional Upper Limb Activity in the Inpatient Rehabilitation Setting with Follow-Up at Home. Applied Sciences. 2025; 15(6):3010. https://doi.org/10.3390/app15063010
Chicago/Turabian StyleBassindale, Kimberly, Sarah Golus, Jake Horder, Maureen Winkoski, Meghann Sytsma, Whitney A. Morelli, Maura Casadio, John McGuire, and Robert A. Scheidt. 2025. "The Feasibility and User Experience of a Program of Progressive Cued Activity to Promote Functional Upper Limb Activity in the Inpatient Rehabilitation Setting with Follow-Up at Home" Applied Sciences 15, no. 6: 3010. https://doi.org/10.3390/app15063010
APA StyleBassindale, K., Golus, S., Horder, J., Winkoski, M., Sytsma, M., Morelli, W. A., Casadio, M., McGuire, J., & Scheidt, R. A. (2025). The Feasibility and User Experience of a Program of Progressive Cued Activity to Promote Functional Upper Limb Activity in the Inpatient Rehabilitation Setting with Follow-Up at Home. Applied Sciences, 15(6), 3010. https://doi.org/10.3390/app15063010