
The Relationship Between Mood, Competitive Anxiety, and Injuries: A Longitudinal Analysis in High-Performance Female Volleyball Players

 , ,
, ,  , and
, and 
Abstract
1. Introduction
- To describe the psychological profile of the sample in terms of mood states, pre-competitive anxiety levels, and injury occurrence.
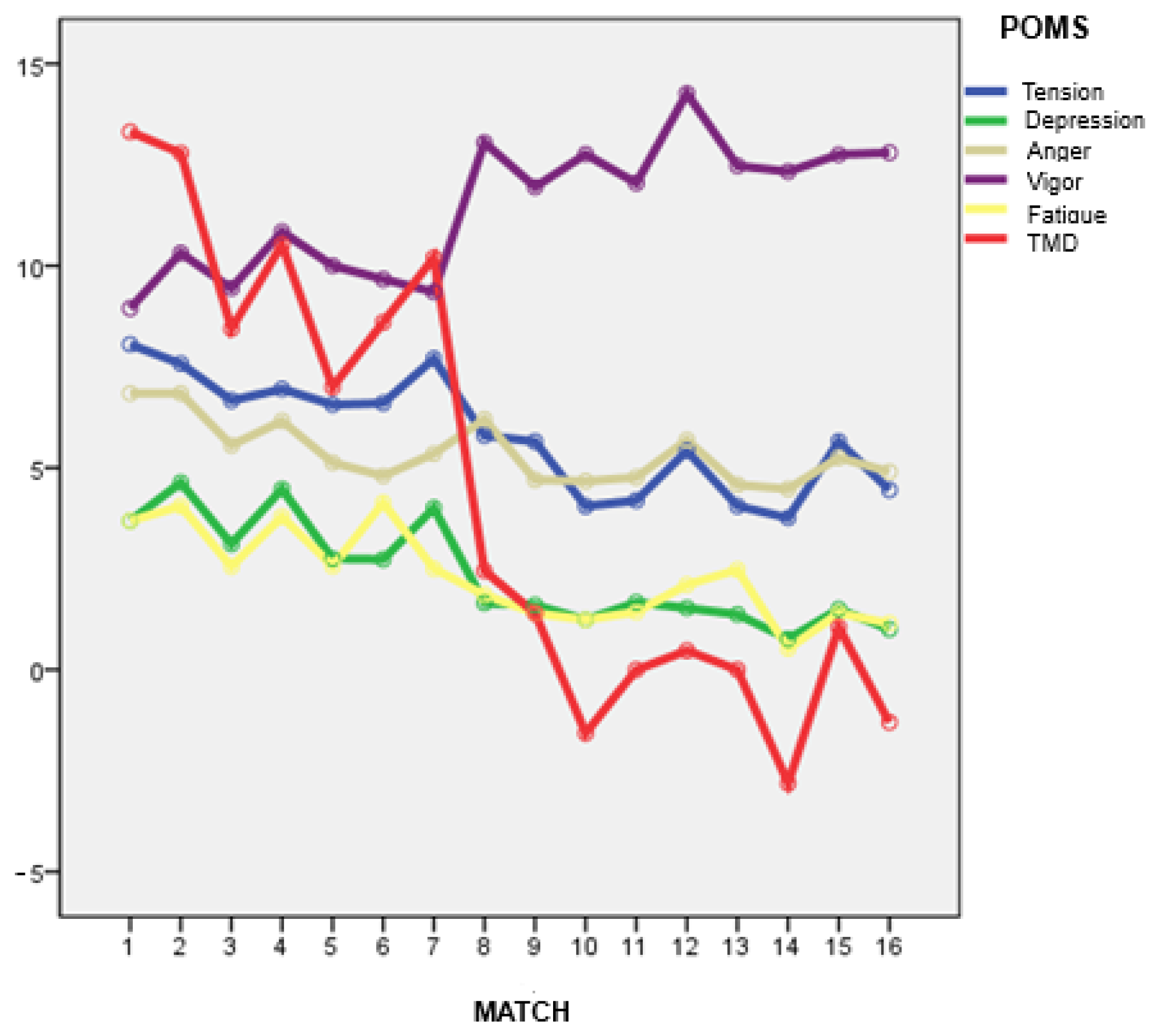
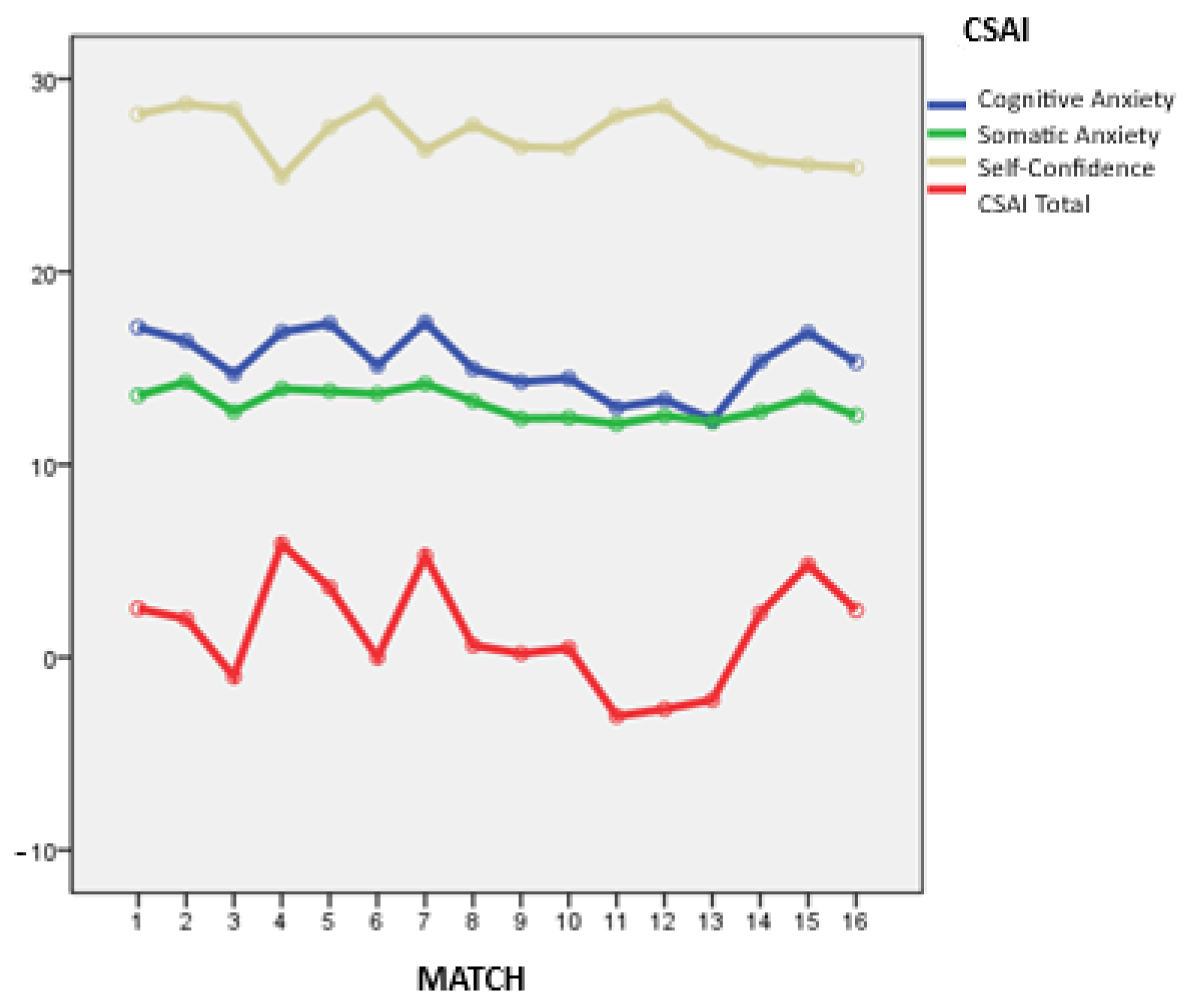
- To analyze the evolution and variability of mood states and pre-competitive anxiety across 16 league matches, comparing injured and non-injured players.
- To explore the relationship between pre-competitive anxiety and mood, analyzing potential patterns of interaction between both constructs.
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Instruments
2.4. Procedure
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- The psychological profile of high-performance female athletes aligns with the “iceberg profile”, characterized by high vigor and self-confidence and low levels of negative emotions and anxiety. This profile may serve as a protective factor against injury.
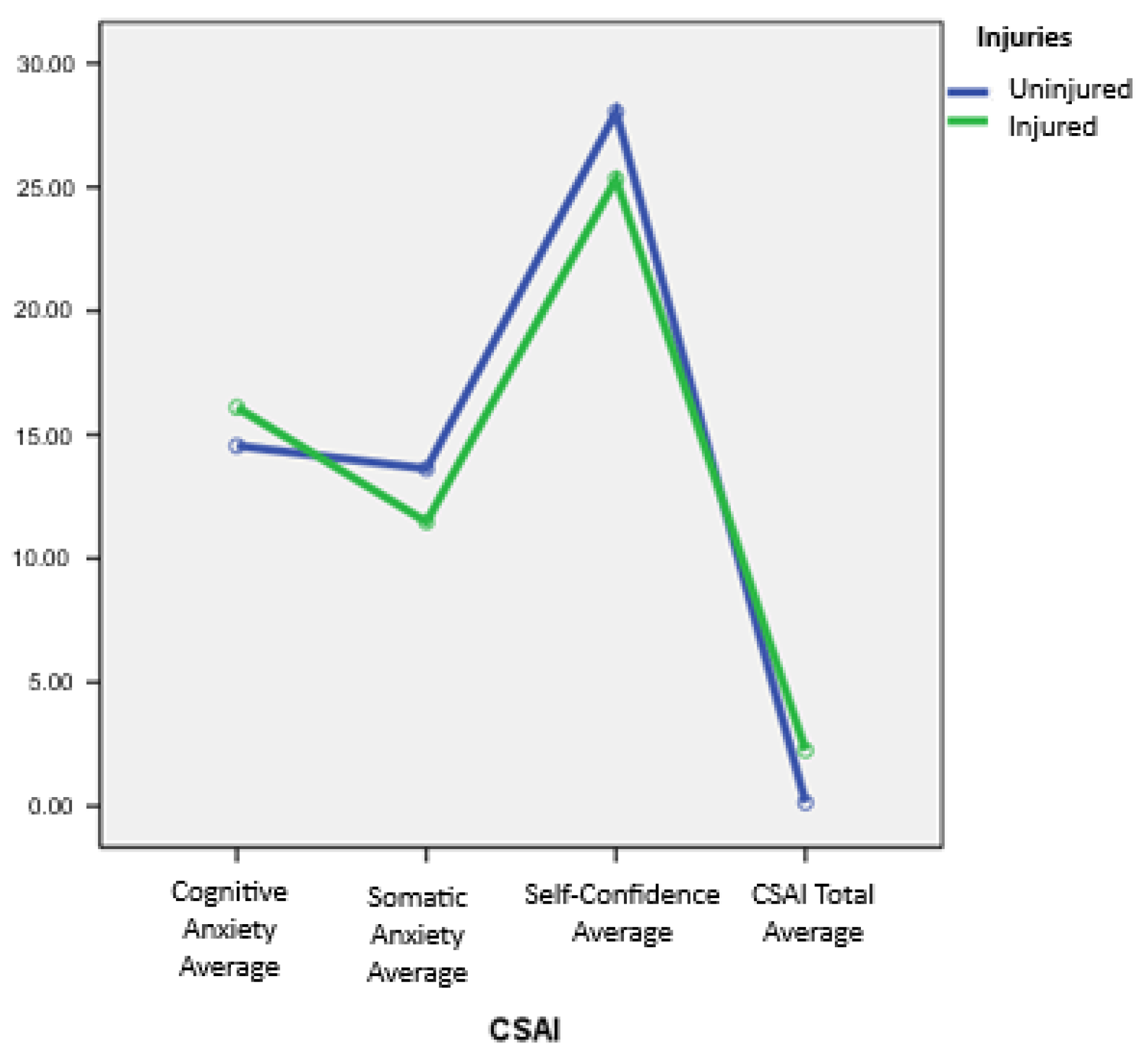
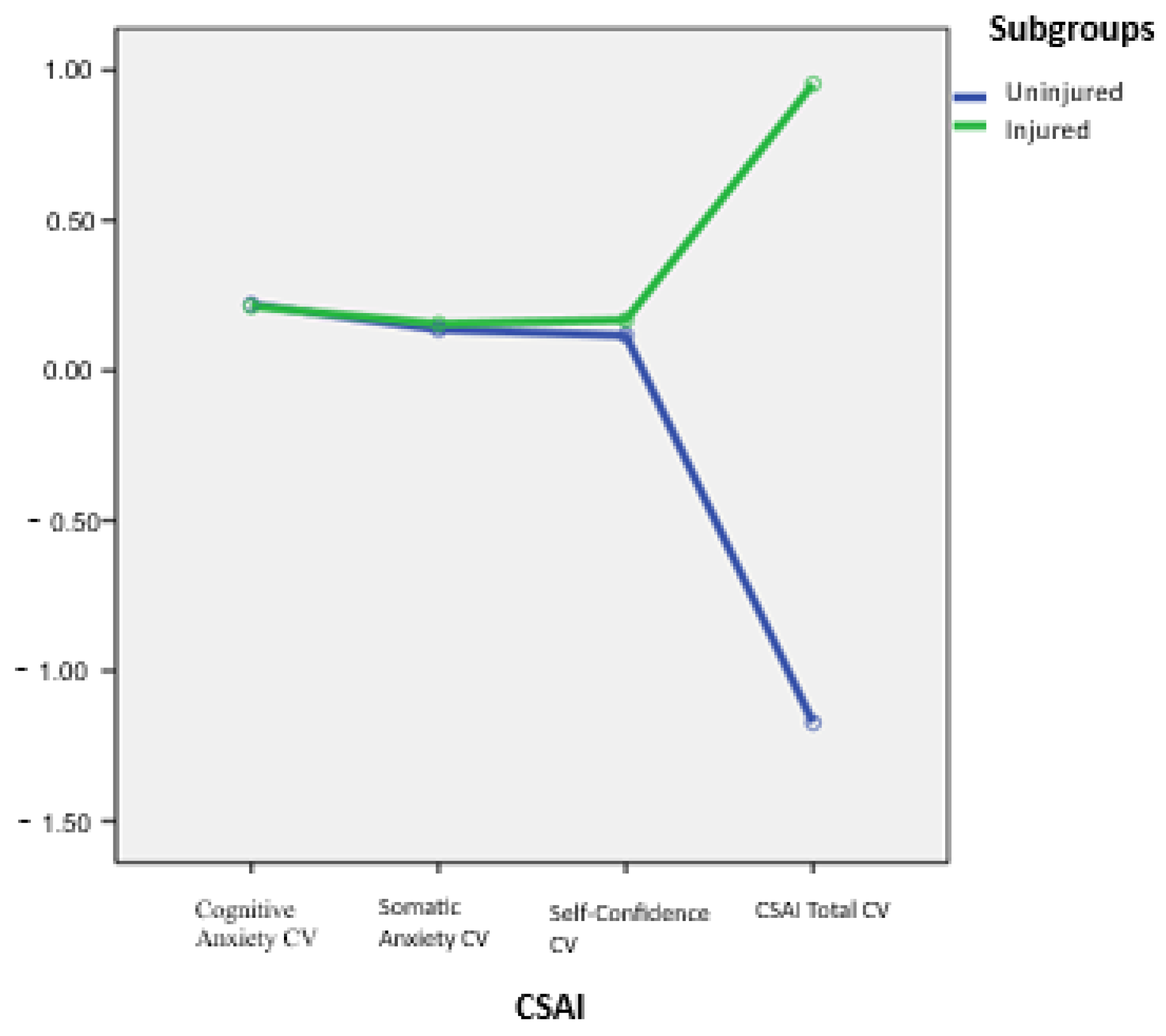
- Cognitive anxiety emerged as a specific vulnerability factor. Injured players displayed higher levels of this variable, supporting its role as a psychological risk indicator.
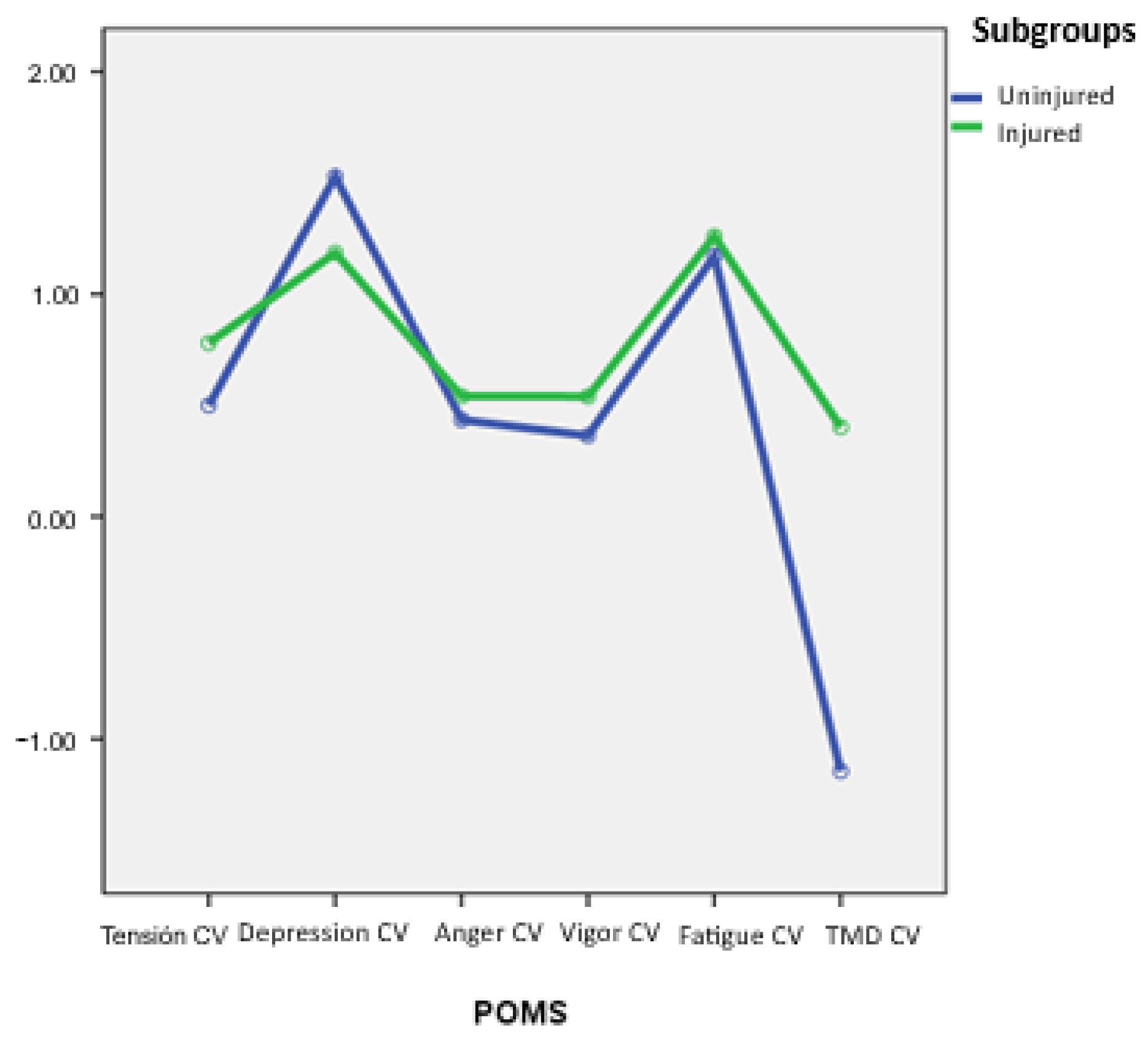
- Emotional instability over time was associated with injury occurrence. Injured players showed more fluctuating moods and anxiety profiles across the season, suggesting that emotional variability may impair regulation and increase injury risk.
- Interdependence between mood and anxiety was confirmed. Higher negative emotions were related to greater somatic anxiety, while higher self-confidence was associated with greater vigor and lower Total Mood Disturbance (TMD).
- Regular monitoring of emotional variables may serve a preventive function by enabling the early identification of psychological risk profiles.
6. Limitations and Future Directions
7. Practical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| POMS | Profile of Mood States |
| TMD | Total Mood Disturbance |
| CSAI-2 | Competitive State Anxiety Inventory-2 |
References
- Rogers, D.L.; Tanaka, M.J.; Cosgarea, A.J.; Ginsburg, R.D.; Dreher, G.M. How mental health affects injury risk and outcomes in athletes. Sports Health 2024, 16, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Trainor, L.R.; Crocker, P.R.; Bundon, A.; Ferguson, L. The rebalancing act: Injured varsity women athletes’ experiences of global and sport psychological well-being. Psychol. Sport Exerc. 2020, 49, 101713. [Google Scholar] [CrossRef]
- Prieto-González, P.; Martínez-Castillo, J.L.; Fernández-Galván, L.M.; Casado, A.; Soporki, S.; Sánchez-Infante, J. Epidemiology of Sports-Related Injuries and Associated Risk Factors in Spanish Competitive Athletes: A Retrospective Study. Int. J. Environ. Res. Public Health 2021, 18, 4857. [Google Scholar] [CrossRef] [PubMed]
- Peña, J.; Gil-Puga, B.; Piedra, A.; Altarriba-Bartés, A.; Loscos-Fàbregas, E.; Chulvi-Medrano, I.; García-de-Alcaraz, A. Epidemiología y factores de riesgo en chicas jóvenes deportistas: Baloncesto, fútbol y voleibol. Apunts. Educ. Fís. Deportes. 2023, 2, 1–12. [Google Scholar]
- Arvinen-Barrow, M.; Clement, D. (Eds.) The Psychology of Sport Injury and Rehabilitation; Routledge: London, UK, 2024. [Google Scholar]
- McClean, Z.J.; Pasanen, K.; Lun, V.; Charest, J.; Herzog, W.; Werthner, P.; Black, A.; Vleuten, R.V.; Lacoste, E.; Jordan, M.J. A biopsychosocial model for understanding training load, fatigue, and musculoskeletal sport injury in university athletes: A scoping review. J. Strength Cond. Res. 2024, 38, 1177–1188. [Google Scholar] [CrossRef]
- Olmedilla, A.; García-Mas, A. Psycholight: Protocolo de evaluación e intervención psicológica para la prevención y la rehabilitación de lesiones deportivas. Rev. Psicol. Apl. Deporte Ejerc. Fís. 2023, 8, 1–11. [Google Scholar] [CrossRef]
- Catalá, P.; Peñacoba, C. Factores psicológicos asociados a la vulnerabilidad de lesiones. Estudio de caso en un equipo de fútbol semi-profesional. Rev. Psicol. Apl. Deporte Ejerc. Fís. 2020, 5, e3. [Google Scholar] [CrossRef]
- Ivarsson, A.; Tranaeus, U.; Johnson, U.; Stenling, A. Negative psychological responses of injury and rehabilitation adherence effects on return to play in competitive athletes: A systematic review and meta-analysis. Open Access J. Sports Med. 2017, 8, 27–32. [Google Scholar] [CrossRef]
- Ríos-Garit, J.; Berengüí, R.; Solé-Cases, S.; Pérez-Surita, Y.; Cañizares Hernández, M.; Rodríguez, R.C. Ansiedad, estados de ánimo y habilidades psicológicas en jóvenes deportistas lesionados en proceso de rehabilitación. Rev. Psicol. Apl. Deporte Ejerc. Fís. 2024, 9, e10. [Google Scholar] [CrossRef]
- Andersen, M.B.; Williams, J.M. A model of stress and athletic injury: Prediction and prevention. J. Sport Exerc. Psychol. 1988, 10, 294–306. [Google Scholar] [CrossRef]
- Galambos, S.A.; Terry, P.C.; Moyle, G.M.; Locke, S.A. Psychological predictors of injury among elite athletes. Br. J. Sports Med. 2005, 39, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Olmedilla, A.; Aguilar, J.M.; Ramos, L.M.; Trigueros, R.; Cantón, E. Perfectionism, mental health, and injuries in women footballers. J. Sport Psychol. 2022, 31, 49–56. [Google Scholar]
- Sánchez-Beleña, F.; García-Naveira, A.G.N. Sobreentrenamiento y deporte desde una perspectiva psicológica: Estado de la cuestión. Rev. Psicol. Apl. Deporte Ejerc. Fís. 2017, 2, 1–12. [Google Scholar] [CrossRef]
- Christakou, A.; Gkiokas, G.; Valsamis, N.; Paraskevopoulos, E.; Papandreou, M. Examining the Relationship and the Gender Differences between Re-Injury Worry, Confidence, and Attention after a Sport Musculoskeletal Injury. J. Clin. Med. 2024, 13, 4428. [Google Scholar] [CrossRef]
- García-Naveira, A.; Ruiz-Barquín, R. Adaptación del ISRA-B a la población deportiva a través de jugadores de fútbol de rendimiento. Ansiedad Estrés 2015, 21, 83–94. [Google Scholar]
- Martens, R.; Vealey, R.; Burton, D. Competitive Anxiety in Sport; Human Kinetics: Champaign, IL, USA, 1990. [Google Scholar]
- Reardon, C.L.; Gorczynski, P.; Hainline, B.; Hitchcock, M.; Rice, S. Anxiety disorders in athletes. Clin. Sports Med. 2024, 43, 33–52. [Google Scholar] [CrossRef]
- Lane, A.M.; Beedie, C.J.; Devonport, T.J.; Stanley, D.M. Instrumental emotion regulation in sport: Relationships between beliefs about emotion and emotion regulation strategies used by athletes. Scand. J. Med. Sci. Sports 2011, 21, e445–e451. [Google Scholar] [CrossRef]
- Mojtahedi, D.; Dagnall, N.; Denovan, A.; Clough, P.; Dewhurst, S.; Hillier, M.; Papageorgiou, K.; Perry, J. Competition anxiety in combat sports and the importance of mental toughness. Behav. Sci. 2023, 13, 713. [Google Scholar] [CrossRef]
- Robazza, C.; Pellizzari, M.; Hanin, Y. Emotion self-regulation and athletic performance: An application of the IZOF model. Psychol. Sport Exerc. 2004, 5, 379–404. [Google Scholar] [CrossRef]
- Habekost, T.; Ovesen, J.; Madsen, J.B. Cognition in elite soccer players: A general model. Front. Psychol. 2024, 15, 1477262. [Google Scholar] [CrossRef]
- Wu, C.H.; Zhao, Y.D.; Yin, F.Q.; Yi, Y.; Geng, L.; Xu, X. Mental fatigue and sports performance of athletes: Theoretical explanation, influencing factors, and intervention methods. Behav. Sci. 2024, 14, 1125. [Google Scholar] [CrossRef]
- Martínez-Gallego, R.; Villafaina, S.; Crespo, M.; Fuentes-García, J.P. Gender and age influence in pre-competitive and post-competitive anxiety in young tennis players. Sustainability 2022, 14, 4966. [Google Scholar] [CrossRef]
- Pranoto, N.W.; Fauziah, V.; Ockta, Y.; Zarya, F.; Iswanto, A.; Hermawan, H.A.; Fitriady, G.; Geantă, V.A.; Orhan, B.E.; Karaçam, A.; et al. Comparison of anxiety levels of individual and group athletes. Retos 2024, 60, 263–268. [Google Scholar] [CrossRef]
- García-Naveira, A.; Ruiz-Barquín, R. Personalidad y rendimiento deportivo en jugadores de fútbol desde el modelo de Millón. Anu. Psicol. 2020, 50, 135–148. [Google Scholar]
- Hanin, Y.L. Emotions in Sport; Human Kinetics: Champaign, IL, USA, 2000. [Google Scholar]
- Ato, M.; López-García, J.J.; Benavente, A. Un sistema de clasificación de los diseños de investigación en psicología. An. Psicol. 2013, 29, 1038–1059. [Google Scholar] [CrossRef]
- Olmedilla, A.; García-Alarcón, M.; Ortega, E. Relaciones entre lesiones deportivas y estrés en fútbol 11 y fútbol sala femenino. J. Sport Health Res. 2018, 10, 339–348. [Google Scholar]
- Gabbett, T.J. The Training—Injury Prevention Paradox: Should Athletes Be Training Smarter and Harder? Br. J. Sports Med. 2016, 50, 273–280. [Google Scholar] [CrossRef]
- Olmedilla, A.; Rubio, V.J.; Ortega, E.; García-Mas, A. Effectiveness of a stress management pilot program aimed at reducing the incidence of sports injuries in young football (soccer) players. Phys. Ther. Sport 2017, 24, 53–59. [Google Scholar] [CrossRef]
- Fuentes, I.; Balaguer, I.; Meliá, J.; García-Merita, M. Forma abreviada del Perfil de Estado de Ánimo (POMS). In V Congreso Nacional de Psicología de la Actividad Física y el Deporte; Cantón, E., Ed.; Universitat de València: Valencia, Spain, 1995; pp. 19–26. [Google Scholar]
- McNair, D.; Lorr, M.; Dropplemann, L. Manual of the Profile of Mood Status (POMS); Educational and Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- Balaguer Solá, I.; Fuentes, I.; Meliá, J.L.; García-Merita, M.; Pérez Recio, G. El perfil de los estados de ánimo (POMS): Baremo para estudiantes valencianos y su aplicación en el contexto deportivo. Rev. Psicol. Deporte 1993, 2, 39–52. [Google Scholar]
- Meyers, M.C.; Sterling, J.C.; Leunes, A.D. Psychological characterization of the collegiate rodeo athlete. J. Sport Behav. 1988, 11, 59–65. [Google Scholar]
- Morgan, W.P.; Brown, D.R.; Raglin, J.S.; O’Connor, P.J.; Ellickson, K.A. Psychological monitoring of overtraining and staleness. Br. J. Sports Med. 1987, 21, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Tabernero, B.; Márquez, S. Efectos de un programa de gimnasia de mantenimiento sobre el perfil de estados emocionales. Apunt. Educ. Fís. Deportes 1996, 4, 19–28. [Google Scholar]
- Prapavessis, H.; Grove, J.R. Personality variables as antecedents of precompetitive mood state temporal patterning. Int. J. Sport Psychol. 1994, 22, 347–365. [Google Scholar]
- Prusaczyk, W.K.; Dishman, R.K.; Cureton, K.J. No effects of glycogen depleting exercise and altered diet composition on mood states. Med. Sci. Sports Exerc. 1992, 24, 708–713. [Google Scholar] [CrossRef]
- Fernández, E.M.A.; Río, G.L.; Fernández, C.A. Propiedades psicométricas de la versión española del Inventario de Ansiedad Competitiva CSAI-2R en deportistas. Psicothema 2007, 19, 150–155. [Google Scholar]
- Buceta, J.M.; De La Llave, A.L.; Llantada, M.D.C.P.; Vallejo, M.; del Pino, M.D. Estado psicológico de los corredores populares de maratón en los días anteriores a la prueba. Psicothema 2003, 15, 273–277. [Google Scholar]
- Bošnjak, S. The declaration of Helsinki: The cornerstone of research ethics. Arch. Oncol. 2001, 9, 179–184. [Google Scholar]
- Tyebkhan, G. Declaration of Helsinki: The ethical cornerstone of human clinical research. Indian J. Dermatol. Venereol. Leprol. 2003, 69, 245–247. [Google Scholar]
- World Medical Association (WMA). Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. In Proceedings of the 52nd WMA General Assembly, Edinburgh, UK, 3–7 October 2000; Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 20 May 2025).
- Harriss, D.J.; MacSween, A.; Atkinson, G. Ethical Standards in Sport and Exercise Science Research: 2020 Update. Int. J. Sports Med. 2019, 40, 813–817. [Google Scholar] [CrossRef]
- Pardo, A.; Ruiz, M.A. Análisis de Datos Con SPSS 13.0; McGraw-Hill: Madrid, Spain, 2005. [Google Scholar]
- Eysenck, M.W.; Derakshan, N.; Santos, R.; Calvo, M.G. Anxiety and Cognitive Performance: Attentional Control Theory. Emotion 2007, 7, 336–353. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Match | Tension M (SD) | Depression M (SD) | Anger M (SD) | Vigor M (SD) | Fatigue M (SD) | TMD M (SD) |
|---|---|---|---|---|---|---|
| 1 | 8.05 (3.70) | 3.68 (3.70) | 6.84 (4.54) | 8.95 (6.44) | 3.68 (3.67) | 13.32 (16.76) |
| 2 | 7.58 (4.74) | 4.63 (5.42) | 6.84 (5.69) | 10.32 (5.33) | 4.05 (4.30) | 12.79 (20.19) |
| 3 | 6.67 (3.76) | 3.11 (3.77) | 5.56 (3.94) | 9.44 (6.64) | 2.56 (3.07) | 8.44 (17.38) |
| 4 | 6.95 (3.95) | 4.47 (5.08) | 6.16 (5.22) | 10.84 (5.25) | 3.79 (4.16) | 10.53 (20.08) |
| 5 | 6.50 (3.74) | 2.94 (3.45) | 5.13 (4.72) | 9.81 (6.30) | 2.50 (3.48) | 7.25 (16.51) |
| 6 | 6.73 (3.75) | 2.67 (2.74) | 4.80 (3.51) | 9.67 (6.61) | 4.13 (4.90) | 8.67 (15.17) |
| 7 | 7.70 (4.77) | 4.00 (3.93) | 5.35 (3.39) | 9.35 (6.67) | 2.50 (2.80) | 10.20 (16.96) |
| 8 | 5.80 (3.83) | 1.65 (1.76) | 6.20 (5.46) | 13.05 (4.81) | 1.85 (1.93) | 2.45 (10.32) |
| 9 | 5.65 (4.36) | 1.60 (2.14) | 4.70 (2.25) | 11.95 (5.12) | 1.40 (2.06) | 1.40 (11.15) |
| 10 | 4.05 (3.64) | 1.24 (2.26) | 4.67 (3.94) | 12.76 (4.72) | 1.24 (1.89) | −1.57 (11.50) |
| 11 | 4.19 (2.89) | 1.67 (2.92) | 4.76 (3.62) | 12.05 (4.02) | 1.43 (1.99) | 7.26 (14.99) |
| 12 | 5.42 (3.52) | 1.53 (1.95) | 5.68 (5.27) | 14.26 (3.74) | 2.11 (2.90) | 0.47 (12.19) |
| 13 | 4.05 (3.29) | 1.37 (1.74) | 4.58 (3.78) | 12.47 (4.81) | 2.47 (3.34) | −2.74 (7.12) |
| 14 | 3.76 (2.49) | 0.76 (0.70) | 4.48 (2.89) | 12.33 (5.94) | 0.52 (1.21) | −4.33 (5.94) |
| 15 | 5.65 (2.78) | 1.50 (2.46) | 5.25 (3.65) | 12.75 (5.21) | 1.40 (1.73) | −1.95 (7.58) |
| 16 | 4.45 (3.24) | 1.00 (1.17) | 4.90 (4.24) | 12.80 (5.29) | 1.15 (1.50) | −1.30 (9.66) |
| Match | Cognitive Anxiety M (SD) | Somatic Anxiety M (SD) | Self-Confidence M (SD) | CSAI Total M (SD) |
|---|---|---|---|---|
| 1 | 17.12 (4.86) | 13.59 (2.60) | 28.18 (3.17) | 1.65 (7.99) |
| 2 | 16.41 (5.35) | 14.29 (4.25) | 28.71 (3.12) | 2.00 (7.92) |
| 3 | 14.68 (3.68) | 12.74 (2.02) | 28.42 (4.31) | −1.00 (6.49) |
| 4 | 16.88 (4.95) | 13.94 (4.25) | 24.94 (5.85) | 5.88 (8.85) |
| 5 | 17.44 (6.44) | 13.81 (3.95) | 27.19 (5.38) | 4.06 (9.13) |
| 6 | 6.73 (3.75) | 2.67 (2.74) | 4.80 (3.51) | 0.33 (7.57) |
| 7 | 17.38 (4.36) | 14.19 (3.95) | 26.31 (4.74) | 5.25 (6.91) |
| 8 | 14.95 (4.17) | 13.29 (4.06) | 27.62 (4.32) | 0.62 (7.85) |
| 9 | 14.29 (4.26) | 12.38 (3.22) | 26.48 (5.19) | 0.19 (7.12) |
| 10 | 14.48 (4.42) | 12.43 (3.06) | 26.43 (6.31) | 0.48 (7.88) |
| 11 | 12.95 (3.72) | 12.10 (2.99) | 28.10 (4.84) | −3.05 (6.29) |
| 12 | 13.37 (4.60) | 12.53 (3.06) | 28.58 (5.43) | 4.79 (33.92) |
| 13 | 12.32 (3.06) | 12.21 (2.86) | 26.74 (6.17) | −1.84 (7.19) |
| 14 | 15.35 (5.89) | 12.75 (2.95) | 25.80 (6.98) | 2.75 (10.79) |
| 15 | 16.85 (6.56) | 13.50 (3.22) | 25.55 (5.74) | 5.00 (10.20) |
| 16 | 15.30 (6.62) | 12.55 (3.32) | 25.40 (6.59) | 3.10 (9.96) |
| Factor | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|
| Tension | 1.64 | 12.00 | 5.70 | 2.58 |
| Depression | 0.00 | 7.50 | 2.25 | 2.10 |
| Anger | 2.19 | 14.50 | 5.28 | 3.02 |
| Vigor | 3.71 | 17.31 | 11.58 | 3.88 |
| Fatigue | 0.00 | 7.13 | 2.17 | 2.05 |
| TMD | −9.25 | 29.75 | 3.75 | 10.88 |
| Factor | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|
| Cognitive Anxiety | 9.67 | 22.50 | 15.07 | 3.67 |
| Somatic Anxiety | 10.00 | 21.25 | 12.91 | 2.62 |
| Self-Confidence | 20.47 | 35.00 | 27.13 | 3.84 |
| CSAI-2 Total | −9.33 | 11.93 | 0.85 | 6.25 |
| Factors | Status | M | SD | Standard Error of the Mean | Z |
|---|---|---|---|---|---|
| Tension | Uninjured | 6.54 | 2.44 | 0.65 | −1.557 |
| Injured | 4.02 | 2.08 | 0.79 | ||
| Depression | Uninjured | 2.36 | 2.23 | 0.59 | −0.078 |
| Injured | 2.03 | 1.95 | 0.74 | ||
| Anger | Uninjured | 5.62 | 3.31 | 0.89 | −0.389 |
| Injured | 4.62 | 2.40 | 0.91 | ||
| Vigor | Uninjured | 12.53 | 3.19 | 0.85 | −0.778 |
| Injured | 9.69 | 4.68 | 1.77 | ||
| Fatigue | Uninjured | 2.22 | 1.98 | 0.53 | 0.000 |
| Injured | 2.07 | 2.35 | 0.89 | ||
| TMD | Uninjured | 4.04 | 10.55 | 2.82 | −0.389 |
| Injured | 3.18 | 12.36 | 4.67 |
| Factor | State | M | SD | Standard Error of the Mean | Z |
|---|---|---|---|---|---|
| Cognitive anxiety | Uninjured | 14.55 | 3.13 | 0.84 | −0.234 |
| Injured | 16.10 | 4.67 | 1.76 | ||
| Somatic anxiety | Uninjured | 13.63 | 2.88 | 0.77 | −1.635 |
| Injured | 11.48 | 1.15 | 0.43 | ||
| Self-confidence | Uninjured | 28.03 | 3.16 | 0.84 | −0.778 |
| Injured | 25.32 | 4.68 | 1.77 | ||
| CSAI-2 total | Uninjured | 0.14 | 5.83 | 1.56 | −0.078 |
| Injured | 2.25 | 7.28 | 2.75 |
| Factors | Status | M | SD | Standard Error of the Mean | Z |
|---|---|---|---|---|---|
| Tension CV | Uninjured | 0.49 | 0.27 | 0.07 | −1.401 |
| Injured | 0.77 | 0.49 | 0.20 | ||
| Depression CV | Uninjured | 1.48 | 1.22 | 0.32 | −0.044 |
| Injured | 1.19 | 0.71 | 0.32 | ||
| Anger CV | Uninjured | 0.44 | 0.26 | 0.07 | −0.934 |
| Injured | 0.55 | 0.16 | 0.07 | ||
| Vigor CV | Uninjured | 0.35 | 0.28 | 0.07 | −0.934 |
| Injured | 0.47 | 0.30 | 0.12 | ||
| Fatigue CV | Uninjured | 1.22 | 0.68 | 0.18 | −0.044 |
| Injured | 1.26 | 0.91 | 0.41 | ||
| TMD CV | Uninjured | −1.14 | 4.07 | 1.09 | −0.545 |
| Injured | 0.28 | 1.01 | 0.41 |
| Factors | Status | Mean | SD | Standard Error Mean | Z |
|---|---|---|---|---|---|
| Cognitive Anxiety CV | Uninjured | 0.22 | 0.14 | 0.04 | −0.389 |
| Injured | 0.21 | 0.07 | 0.03 | ||
| Somatic Anxiety CV | Uninjured | 0.14 | 0.06 | 0.01 | −0.389 |
| Injured | 0.16 | 0.07 | 0.03 | ||
| Self-Confidence CV | Uninjured | 0.12 | 0.08 | 0.02 | −1.479 |
| Injured | 0.17 | 0.08 | 0.03 | ||
| CSAI total CV | Uninjured | −1.17 | 4.16 | 1.07 | −1.012 |
| Injured | 0.95 | 2.92 | 1.19 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Tension | 1 | |||||||||
| 2. Depression | 0.71 *** | 1 | ||||||||
| 3. Anger | 0.86 *** | 0.69 *** | 1 | |||||||
| 4. Vigor | 0.09 | –0.46 * | 0.06 | 1 | ||||||
| 5. Fatigue | 0.72 *** | 0.94 *** | 0.75 *** | –0.44 * | 1 | |||||
| 6. TMD | 0.67 *** | 0.92 *** | 0.66 *** | –0.62 ** | 0.94 *** | 1 | ||||
| 7. Cognitive Anxiety | –0.17 | –0.18 | –0.17 | 0.05 | –0.13 | –0.13 | 1 | |||
| 8. Somatic Anxiety | 0.64 *** | 0.37 † | 0.52 * | 0.20 | 0.36 | 0.35 | 0.17 | 1 | ||
| 9. Self-Confidence | 0.23 | –0.31 | 0.15 | 0.84 *** | –0.31 | –0.48 * | –0.17 | 0.27 | 1 | |
| 10. CSAI-2 Total | 0.10 | 0.32 | 0.15 | –0.46 * | 0.40 | 0.48 * | 0.65 ** | 0.24 | –0.68 ** | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boladeras, A.; Gil-Caselles, L.; Moreno-Fernández, I.; Guillén-Cots, J.; Garcia-Naveira, A.; Ruiz-Barquín, R.; Olmedilla-Zafra, A. The Relationship Between Mood, Competitive Anxiety, and Injuries: A Longitudinal Analysis in High-Performance Female Volleyball Players. Appl. Sci. 2025, 15, 7585. https://doi.org/10.3390/app15137585
Boladeras A, Gil-Caselles L, Moreno-Fernández I, Guillén-Cots J, Garcia-Naveira A, Ruiz-Barquín R, Olmedilla-Zafra A. The Relationship Between Mood, Competitive Anxiety, and Injuries: A Longitudinal Analysis in High-Performance Female Volleyball Players. Applied Sciences. 2025; 15(13):7585. https://doi.org/10.3390/app15137585
Chicago/Turabian StyleBoladeras, Ana, Laura Gil-Caselles, Isabel Moreno-Fernández, Joel Guillén-Cots, Alejo Garcia-Naveira, Roberto Ruiz-Barquín, and Aurelio Olmedilla-Zafra. 2025. "The Relationship Between Mood, Competitive Anxiety, and Injuries: A Longitudinal Analysis in High-Performance Female Volleyball Players" Applied Sciences 15, no. 13: 7585. https://doi.org/10.3390/app15137585
APA StyleBoladeras, A., Gil-Caselles, L., Moreno-Fernández, I., Guillén-Cots, J., Garcia-Naveira, A., Ruiz-Barquín, R., & Olmedilla-Zafra, A. (2025). The Relationship Between Mood, Competitive Anxiety, and Injuries: A Longitudinal Analysis in High-Performance Female Volleyball Players. Applied Sciences, 15(13), 7585. https://doi.org/10.3390/app15137585