
Effect of Anti-Pronation Athletic Tape Types: A Randomized Crossover Trial on Ankle Strength, Gait Parameters, and Balance Control Ability in Women with Flexible Flat Feet



Abstract
1. Introduction
2. Materials and Methods
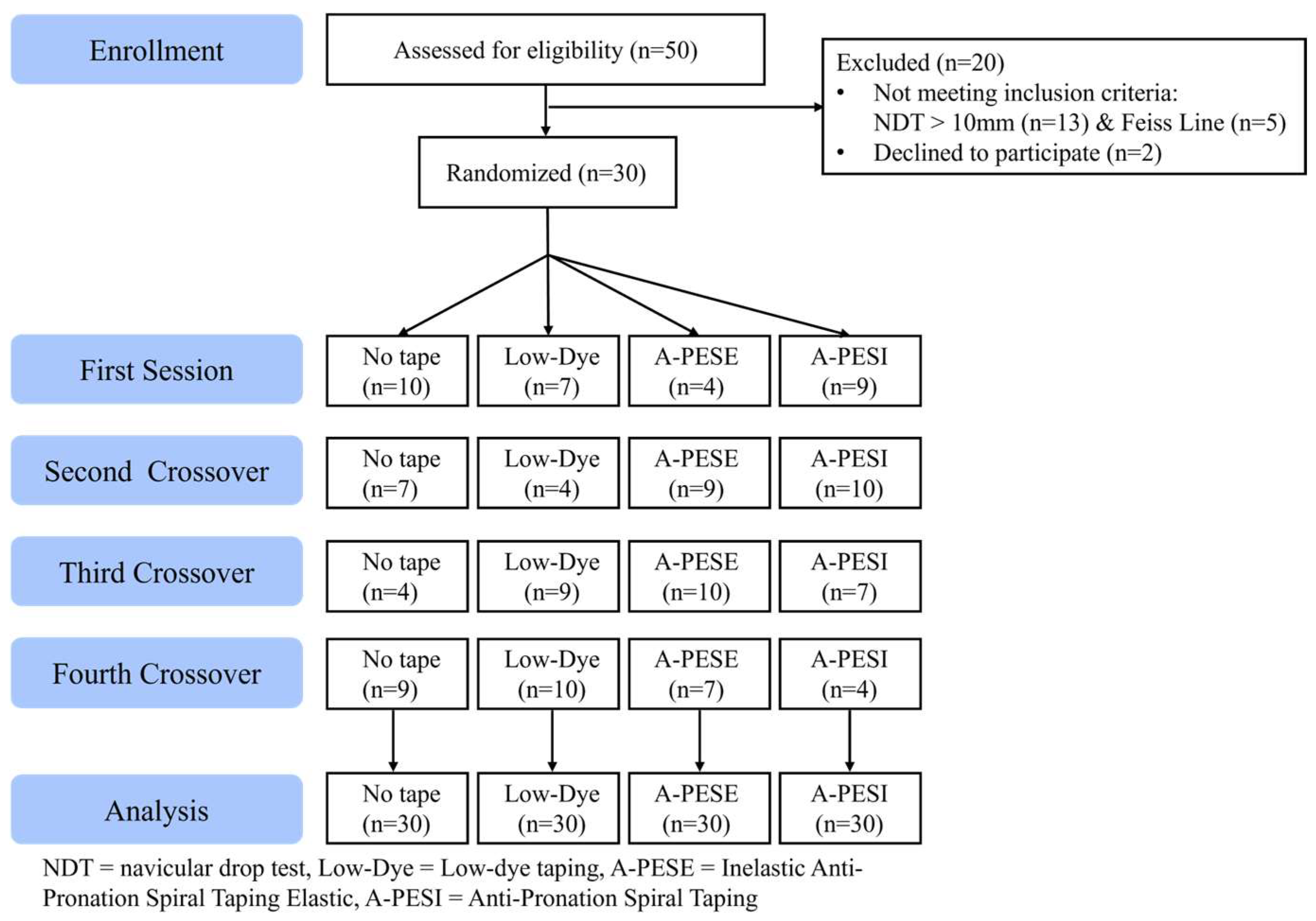
2.1. Participants
2.2. Experimental Procedure
2.3. Screening Methods for Flexible Flat Feet
2.4. Interventions
2.4.1. Low-Dye Taping
2.4.2. Anti-Pronation Spiral Taping
2.5. Measurements
2.5.1. Gait Parameters
2.5.2. Balance Control Ability
2.5.3. Ankle Strength
2.6. Statistical Analysis
3. Results
3.1. Differences in Ankle Muscle Strength Based on the Type of Taping
3.2. Analysis of Gait Parameters Based on the Type of Taping
3.3. Analysis of Balance Control Ability Based on the Type of Taping
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MLA | medial longitudinal arch |
| NDT | navicular drop test |
| HHD | handheld dynamometer |
| LOS | limits of stability |
References
- McKeon, P.O.; Fourchet, F. Freeing the foot: Integrating the foot core system into rehabilitation for lower extremity injuries. Clin. Sports Med. 2015, 34, 347–361. [Google Scholar] [CrossRef] [PubMed]
- Welte, L.; Kelly, L.A.; Lichtwark, G.A.; Rainbow, M.J. Influence of the windlass mechanism on arch-spring mechanics during dynamic foot arch deformation. J. R. Soc. 2018, 15, 20180270. [Google Scholar] [CrossRef] [PubMed]
- Pourhoseingholi, E.; Pourhoseingholi, M.A. Comparison of arch index of flat foot and healthy foot in pre-school children. Thrita 2013, 2, 15–18. [Google Scholar] [CrossRef]
- de Cesar Netto, C.; Schon, L.C.; Thawait, G.K.; da Fonseca, L.F.; Chinanuvathana, A.; Zbijewski, W.B.; Siewerdsen, J.H.; Demehri, S. Flexible adult acquired flatfoot deformity: Comparison between weight-bearing and non-weight-bearing measurements using cone-beam computed tomography. J. Bone Joint Surg. Am. 2017, 99, e98. [Google Scholar] [CrossRef]
- Kido, M.; Ikoma, K.; Imai, K.; Maki, M.; Takatori, R.; Tokunaga, D.; Inoue, N.; Kubo, T. Load response of the tarsal bones in patients with flatfoot deformity: In vivo 3D study. Foot Ankle Int. 2011, 32, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Aydin, M.; Mutlu, R.; Singh, D.; Sariyildiz, E.; Coman, R.; Mayland, E.; Shemmell, J.; Lee, W. Novel soft haptic biofeedback—Pilot study on postural balance and proprioception. Sensors 2022, 22, 3779. [Google Scholar] [CrossRef]
- Yu, I.; Ko, M.; Oh, J. The effects of biofeedback training for efficient activation of infraspinatus on proprioception and EMG activity during shoulder external rotation. J. Electromyogr. Kinesiol. 2023, 71, 102798. [Google Scholar] [CrossRef]
- Maurer, C.; Mergner, T.; Bolha, B.; Hlavacka, F. Human balance control during cutaneous stimulation of the plantar soles. Neurosci. Lett. 2001, 302, 45–48. [Google Scholar] [CrossRef]
- Zijlstra, A.; Mancini, M.; Chiari, L.; Zijlstra, W. Biofeedback for training balance and mobility tasks in older populations: A systematic review. J. Neuroeng. Rehabilit. 2010, 7, 58. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Iqbal, Z.A. Effect of deep cervical flexor muscle training using pressure biofeedback on pain and forward head posture in school teachers with neck pain: An observational study. BioMed Res. Int. 2021, 2021, 5588580. [Google Scholar] [CrossRef]
- Brijwasi, T.; Borkar, P. A comprehensive exercise program improves foot alignment in people with flexible flat foot: A randomised trial. J. Physiother. 2023, 69, 42–46. [Google Scholar] [CrossRef]
- MacKenzie, A.J.; Rome, K.; Evans, A.M. The efficacy of nonsurgical interventions for pediatric flexible flat foot: A critical review. J. Pediatr. Orthop. 2012, 32, 830–834. [Google Scholar] [CrossRef] [PubMed]
- Siu, W.; Shih, Y.; Lin, H. Effects of kinesio tape on supporting medial foot arch in runners with functional flatfoot: A preliminary study. Res. Sports Med. 2020, 28, 168–180. [Google Scholar] [CrossRef] [PubMed]
- Vicenzino, B.; Franettovich, M.; McPoil, T.; Russell, T.; Skardoon, G.; Bartold, S.J. Initial effects of anti-pronation tape on the medial longitudinal arch during walking and running. Br. J. Sports Med. 2005, 39, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Kachanathu, S.J.; Algarni, F.S.; Nuhmani, S.; Alenazi, A.M.; Hafez, A.R.; Algarni, A.D. Functional outcomes of kinesio taping versus standard orthotics in the management of shin splint. J. Sports Med. Phys. Fit. 2018, 58, 1666–1670. [Google Scholar] [CrossRef]
- Radford, J.A.; Landorf, K.B.; Buchbinder, R.; Cook, C. Effectiveness of low-dye taping for the short-term treatment of plantar heel pain: A randomised trial. BMC Musculoskelet. Disord. 2006, 7, 64. [Google Scholar] [CrossRef]
- Chen, T.L.; Wong, D.W.; Peng, Y.; Zhang, M. Prediction on the plantar fascia strain offload upon fascia taping and low-dye taping during running. J. Orthop. Transl. 2020, 20, 113–121. [Google Scholar] [CrossRef]
- Landorf, K.B.; Radford, J.A.; Keenan, A.-M.; Redmond, A.C. Effectiveness of low-dye taping for the short-term management of plantar fasciitis. J. Am. Podiatr. Med. Assoc. 2005, 95, 525–530. [Google Scholar] [CrossRef]
- Russo, S.J.; Chipchase, L.S. The effect of low-dye taping on peak plantar pressures of normal feet during gait. Aust. J. Physiother. 2001, 47, 239–244. [Google Scholar] [CrossRef]
- O’Sullivan, K.; Kennedy, N.; O’Neill, E.; Ni Mhainin, U. The effect of low-dye taping on rearfoot motion and plantar pressure during the stance phase of gait. BMC Musculoskelet. Disord. 2008, 9, 111. [Google Scholar] [CrossRef]
- Prusak, K.M.; Prusak, K.A.; Hunter, I.; Seeley, M.K.; Hopkins, J.T. Comparison of two taping techniques on navicular drop and center-of-pressure measurements during stance. Athl. Train. Sports Health Care 2014, 6, 252–260. [Google Scholar] [CrossRef]
- Hoang, N.; Chen, S.; Chou, L. The impact of foot orthoses and exercises on pain and navicular drop for adult flatfoot: A network meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 8063. [Google Scholar] [CrossRef]
- Aenumulapalli, A.; Manoj, M.K.; Achleshwar, R.G. Prevalence of flexible flat foot in adults: A cross-sectional study. J. Clin. Diagn. Res. 2017, 11, AC17–AC20. [Google Scholar] [CrossRef]
- Michelini, A.; Arezoo, E.; Jan, A. Two-dimensional video gait analysis: A systematic review of reliability, validity, and best practice considerations. Prosthet. Orthot. Int. 2020, 44, 245–262. [Google Scholar] [CrossRef] [PubMed]
- Salavati, M.; Hadian, M.R.; Mazaheri, M. Test-retest reliability of center of pressure measures of postural stability during quiet standing in a group with musculoskeletal disorders. Gait Posture 2009, 29, 382–386. [Google Scholar] [CrossRef]
- Stark, T.; Walker, B.; Phillips, J.K. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PM&R 2011, 3, 472–479. [Google Scholar]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [PubMed]
- Ho, I.M.; Weldon, A.; Yeung, N.C.Y.; Luk, J.T.C.; Cè, E. Low-dye taping may enhance physical performance and muscle activation in basketball players with overpronated feet. PLoS ONE 2022, 17, e0275178. [Google Scholar] [CrossRef]
- Bruening, D.; Messick, C.; Waid, D.; Krupp, T.D.; Stringer, J.R.; Parry, D.J.; Berry, L.J. For plantar taping, direction of elasticity matters. Sci. Rep. 2023, 13, 22811. [Google Scholar] [CrossRef]
- Choi, Y.; Nam, C.; Lee, J.; Park, Y.H. The effects of taping prior to PNF treatment on lower extremity proprioception of hemiplegic patients. J. Phys. Ther. Sci. 2013, 25, 1119–1122. [Google Scholar] [CrossRef]
- Correia, C.; Lopes, S.; Gonçalves, R.; Torres, R.; Pinho, F.; Gonçalves, P.; Rodrigues, M.; Costa, R.; Lopes, M.; Ribeiro, F. Kinesiology taping does not change fibularis longus latency time and postural sway. J. Bodyw. Mov. Ther. 2016, 20, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Calmels, P.; Escafit, M.; Domenach, M.; Minaire, P. Posturographic evaluation of the proprioceptive effect of ankle orthoses in healthy volunteers. Int. Disabil. Stud. 1991, 13, 42–45. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Mean ± SD |
|---|---|
| Age (years) | 21.03 ± 1.21 |
| Height (cm) | 161.51 ± 5.85 |
| Weight (kg) | 57.87 ± 11.41 |
| Taping Type | No Tape | Low-Dye | A-PESI | A-PESE | F | p | η2 (Effect Size) |
|---|---|---|---|---|---|---|---|
| Dorsiflexion (kg) | 19.36 ± 6.04 | 20.06 ± 6.81 | 20.85 ± 8.01 | 21.41 ± 7.24 | 4.24 | 0.02 * No Tape < Elastic, Low Dye < Elastic | 0.329 |
| Plantarflexion (kg) | 17.26 ± 3.62 | 19.58 ± 4.83 | 19.64 ± 6.83 | 19.69 ± 5.69 | 2.69 | 0.08 | 0.237 |
| Inversion (kg) | 12.38 ± 3.43 | 12.80 ± 2.80 | 13.38 ± 3.82 | 12.28 ± 3.82 | 0.32 | 0.47 | 0.036 |
| Eversion (kg) | 12.33 ± 2.54 | 13.53 ± 2.31 | 13.09 ± 2.75 | 12.60 ± 2.53 | 2.48 | 0.07 | 0.222 |
| Taping Type | No Tape | Low-Dye | A-PESI | A-PESE | F | p | η2 (Effect Size) |
|---|---|---|---|---|---|---|---|
| step length (cm) | 37.82 ± 7.78 | 40.03 ± 8.04 | 40.43 ± 5.63 | 40.77 ± 7.83 | 3.87 | 0.01 * No Tape < Inelastic = Elastic | 0.309 |
| stride length (cm) | 114.15 ± 18.09 | 117.64 ± 17.84 | 116.99 ± 15.67 | 120.24 ± 17.98 | 6.43 | 0.01 * No Tape < Elastic | 0.426 |
| Taping Type | No Tape | Low-Dye | A-PESI | A-PESE | F | p | η2 (Effect Size) |
|---|---|---|---|---|---|---|---|
| sway length (cm) | 12.03 ± 3.77 | 13.67 ± 6.48 | 12.82 ± 5.42 | 12.93 ± 5.99 | 1.17 | 0.34 | 0.119 |
| sway velocity (cm/s) | 0.41 ± 0.13 | 0.46 ± 0.21 | 0.43 ± 0.18 | 0.43 ± 0.20 | 1.64 | 0.20 | 0.159 |
| LOS (mm2) | 10,096.06 ± 3251.56 | 8991.61 ± 3500.21 | 9038.29 ± 2884.41 | 9245.77 ± 3019.21 | 3.84 | 0.01 *No Tape < Low Dye = Inelastic = Elastic | 0.307 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.-Y.; Kim, S.-G. Effect of Anti-Pronation Athletic Tape Types: A Randomized Crossover Trial on Ankle Strength, Gait Parameters, and Balance Control Ability in Women with Flexible Flat Feet. Appl. Sci. 2025, 15, 6858. https://doi.org/10.3390/app15126858
Park S-Y, Kim S-G. Effect of Anti-Pronation Athletic Tape Types: A Randomized Crossover Trial on Ankle Strength, Gait Parameters, and Balance Control Ability in Women with Flexible Flat Feet. Applied Sciences. 2025; 15(12):6858. https://doi.org/10.3390/app15126858
Chicago/Turabian StylePark, Sang-Young, and Seong-Gil Kim. 2025. "Effect of Anti-Pronation Athletic Tape Types: A Randomized Crossover Trial on Ankle Strength, Gait Parameters, and Balance Control Ability in Women with Flexible Flat Feet" Applied Sciences 15, no. 12: 6858. https://doi.org/10.3390/app15126858
APA StylePark, S.-Y., & Kim, S.-G. (2025). Effect of Anti-Pronation Athletic Tape Types: A Randomized Crossover Trial on Ankle Strength, Gait Parameters, and Balance Control Ability in Women with Flexible Flat Feet. Applied Sciences, 15(12), 6858. https://doi.org/10.3390/app15126858