

The Changes in Nickel and Chromium Ion Levels in Saliva with Fixed Orthodontic Appliances: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
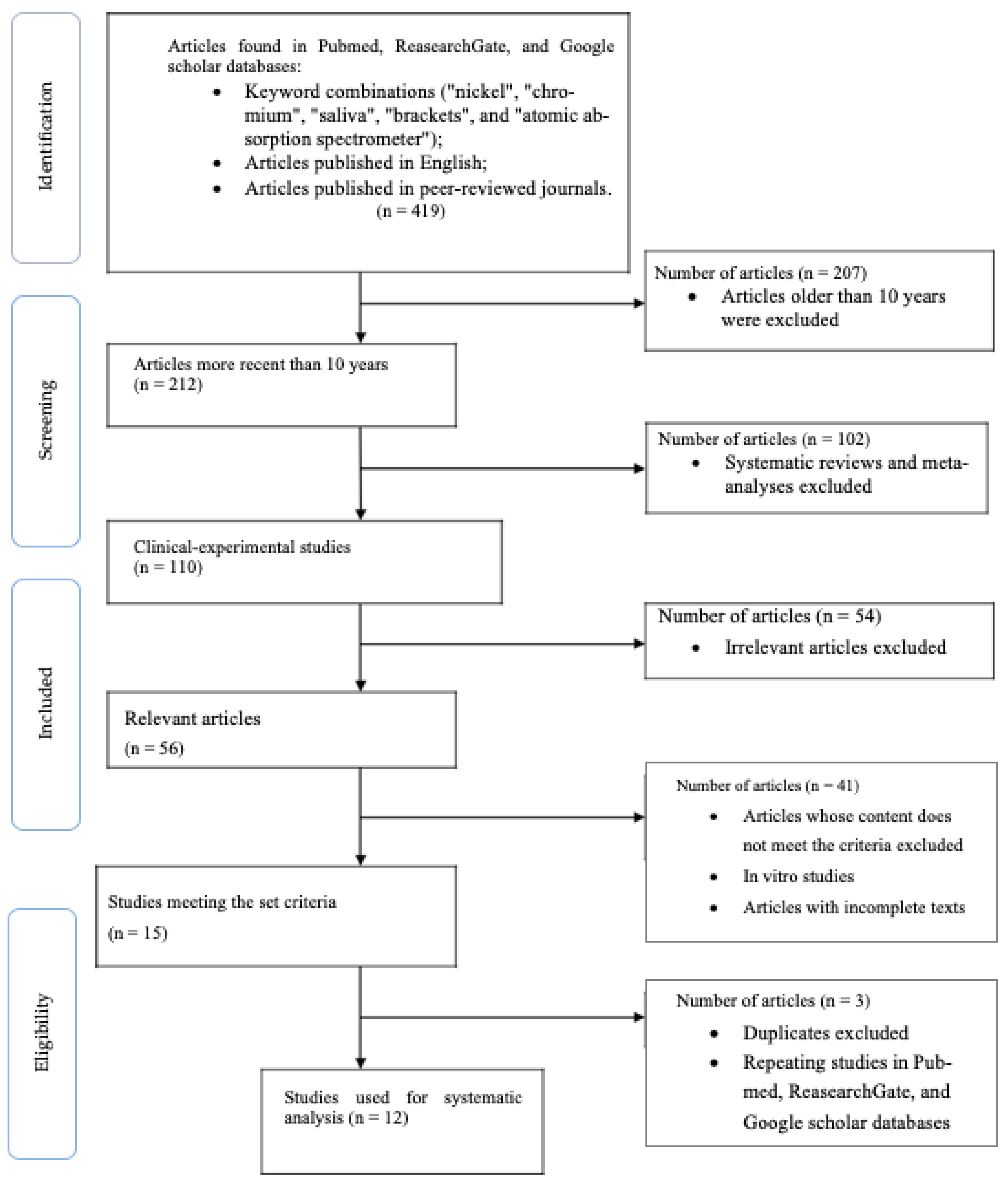
2.1. Search Protocol
2.2. Article Screening
2.3. Criteria for the Inclusion of Articles in a Systematic Literature Review
- Articles no older than 10 years (published between 11 September 2012 and 11 September 2022).
- Clinical trials.
- Articles published in English.
- Articles published in peer-reviewed journals.
- Research conducted on human subjects.
2.4. Criteria for the Exclusion of Articles
- Systematic literature reviews and meta-analyses.
- Studies conducted on animals.
- In vitro studies.
- Descriptions of one or more clinical cases.
- Articles published in a language other than English.
- Incomplete texts of articles.
2.5. Data Accumulation
2.6. General Overview of the Articles
3. Results
4. Discussion
Limitations of the Review
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Velasco-Ibáñez, R.; Lara-Carrillo, E.; Morales-Luckie, R.A.; Romero-Guzmán, E.T.; Toral-Rizo, V.H.; Ramírez-Cardona, M.; García-Hernández, V.; Medina-Solís, C.E. Evaluation of the release of nickel and titanium under orthodontic treatment. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, A.; Tikku, T.; Khanna, R.; Maurya, R.P.; Geeta Verma, R.C. Murthy Release of nickel and chromium ions in the saliva of patients with fixed orthodontic appliance: An in-vivo study. Natl. J. Maxillofac. Surg. 2015, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Hafez, H.S.; Selim, E.M.N.; Eid, F.H.K.; Tawfik, W.A.; Al Ashkar, E.; Mostafa, Y.A. Cytotoxicity, genotoxicity, and metal release in patients with fixed orthodontic appliances: A longitudinal in-vivo study. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Hussain, H.D.; Ajith, S.D.; Goel, P. Nickel release from stainless steel and nickel titanium archwires—An in vitro study. J. Oral Biol. Craniofacial Res. 2016, 6, 213–218. [Google Scholar] [CrossRef]
- Syed, M.; Chopra, R.; Sachdev, V. Allergic Reactions to Dental Materials—A Systematic Review. JCDR 2015, 9, ZE04. [Google Scholar] [CrossRef]
- Schuttelaar, M.L.A.; Ofenloch, R.F.; Bruze, M.; Cazzaniga, S.; Elsner, P.; Gonçalo, M.; Naldi, L.; Svensson, Å.; Diepgen, T.L. Prevalence of contact allergy to metals in the European general population with a focus on nickel and piercings: The EDEN Fragrance Study. Contact Dermat. 2018, 79, 1–9. [Google Scholar] [CrossRef]
- Wang, Y.; Su, H.; Gu, Y.; Song, X.; Zhao, J. Carcinogenicity of chromium and chemoprevention: A brief update. OncoTargets Ther. 2017, 16, 4065–4079. [Google Scholar] [CrossRef]
- Chakravarthi, S.; Chitharanjan, A.; Padmanabhan, S. Allergy and orthodontics. J. Orthod. Sci. 2012, 1, 83–87. [Google Scholar] [CrossRef]
- Saito, M.; Arakaki, R.; Yamada, A.; Tsunematsu, T.; Kudo, Y.; Ishimaru, N. Molecular Mechanisms of Nickel Allergy. Int. J. Mol. Sci. 2016, 17, 202. [Google Scholar] [CrossRef]
- Pazzini, C.A.; Pereira, L.J.; Marques, L.S.; Generoso, R.; de Oliveira, G., Jr. Allergy to nickel in orthodontic patients: Clinical and histopathologic evaluation. Gen Dent. 2010, 58, 58–61. [Google Scholar]
- Pazzini, C.A.; Júnior, G.O.; Marques, L.S.; Pereira, C.V.; Pereira, L.J. Prevalence of Nickel Allergy and Longitudinal Evaluation of Periodontal Abnormalities in Orthodontic Allergic Patients. Angle Orthod. 2009, 79, 922–927. [Google Scholar] [CrossRef]
- Martín-Cameán, A.; Jos, A.; Solano, E.; Iglesias-Linares, A. Genotoxic and cytotoxic effects and gene expression changes induced by fixed orthodontic appliances in oral mucosa cells of patients: A systematic review. Toxicol. Mech. Methods 2015, 25, 1–8. [Google Scholar] [CrossRef]
- Talic, N.F.; Alnahwi, H.H.; Al-Faraj, A.S. Nickel and chromium levels in the saliva of a Saudi sample treated with fixed orthodontic appliances. Saudi Dent. J. 2013, 25, 129–133. [Google Scholar] [CrossRef]
- Quadras, D.D.; Nayak, U.S.K.; Kumari, N.S.; Priyadarshini, H.; Gowda, S.; Fernandes, B. In vivo study on the release of nickel, chromium, and zinc in saliva and serum from patients treated with fixed orthodontic appliances. Dent. Res. J. 2019, 16, 209–215. [Google Scholar] [CrossRef]
- Sunny, B.; Muddaiah, S.; Reddy, G.; Somaiah, S.; Shetty, B.; Akshatha, M.V. Comparative Evaluation Of Human Saliva For The Presence of Nickel And Chromium Released From Orthodontic Appliances Due To Radio Frequency Electromagnetic Radiation (Cell Phone Usage)—A Clinical Study. IJDSIR 2020, 3, 274–282. [Google Scholar]
- Amini, F.; Jafari, A.; Amini, P.; Sepasi, S. Metal ion release from fixed orthodontic appliances—An in vivo study. Eur. J. Orthod. 2011, 34, 126–130. [Google Scholar] [CrossRef]
- Nayak, R.S.; Khanna, B.; Pasha, A.; Vinay, K.; Narayan, A.; Chaitra, K. Evaluation of Nickel and Chromium Ion Release During Fixed Orthodontic Treatment Using Inductively Coupled Plasma-Mass Spectrometer: An In Vivo Study. J. Int. Oral Health 2015, 7, 14–20. [Google Scholar]
- Fróis, A.; Mendes, A.R.; Pereira, S.A.; Louro, C.S. Metal Release and Surface Degradation of Fixed Orthodontic Appliances during the Dental Levelling and Aligning Phase: A 12-Week Study. Coatings 2022, 12, 554. [Google Scholar] [CrossRef]
- Raina, S.; Adarshika; Raina, R.; Babbar, A.; Shriram, P. Assessment of salivary nickel levels in patients undergoing fixed orthodontic treatment. J. Adv. Med. Dent. Sci. Res. 2018, 6, 134–137. [Google Scholar]
- Nanjannawar, L.G.; Girme, T.S.; Agrawal, J.M.; Agrawal, M.S.; Fulari, S.G.; Shetti, S.S.; Kagi, V.A. Effect of Mobile Phone Usage on Nickel Ions Release and pH of Saliva in Patients Undergoing Fixed Orthodontic Treatment. J. Clin. Diagn. Res. 2017, 11, ZC84–ZC87. [Google Scholar] [CrossRef]
- Bengleil, M.S.; Orfi, J.M.; Abdelgader, I. Evaluation of Salivary Nickel Level During Orthodontic Treatment. Int. J. Med. Health Sci. 2013, 8, 12. [Google Scholar] [CrossRef]
- Singh, D.P.; Thakur, S.; Abrol, T.; Vashisht, S.; Manhas, K.J. Assessment salivary nickel level in patients with fixed orthodontic treatment- A clinical study. J. Adv. Med. Dent. Sci. Res 2020, 8, 219–222. [Google Scholar]
- Jurela, A.; Verzak, Ž.; Brailo, V.; Škrinjar, I.; Sudarević, K.; Janković, B. Salivary Electrolytes in Patients with Metallic and Ceramic Orthodontic Brackets. Acta Stomatol. Croat. 2018, 52, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Michalke, B.; Rossbach, B.; Göen, T.; Schäferhenrich, A.; Scherer, G. Saliva as a matrix for human biomonitoring in occupational and environmental medicine. Int. Arch. Occup. Environ. Health 2014, 88, 1–44. [Google Scholar] [CrossRef]
- Sfondrini, M.F.; Cacciafesta, V.; Maffia, E.; Scribante, A.; Alberti, G.; Biesuz, R.; Klersy, C. Nickel release from new conventional stainless steel, recycled, and nickel-free orthodontic brackets: An in vitro study. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 809–815. [Google Scholar] [CrossRef]
- Petoumenou, E.; Arndt, M.; Keilig, L.; Reimann, S.; Hoederath, H.; Eliades, T.; Jäger, A.; Bourauel, C. Nickel concentration in the saliva of patients with nickel-titanium orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 59–65. [Google Scholar] [CrossRef]
- Crossner, C.G. Salivary flow rate in children and adolescents. Swed. Dent. J. 1984, 8, 271–276. [Google Scholar]
- Baraceloux, D.G. Nickel. J. Clin. Toxicol. 1999, 37, 239–258. [Google Scholar] [CrossRef]
- Friberg, L. International Programme on Chemical Safety 1991 Environmental Health Criteria Nickel; World Health Organization: Geneva, Switzerland, 1991; pp. 16–17. [Google Scholar]
- Pillai, A.R.; Gangadharan, A.; Gangadharan, J.; Kumar, N.V. Cytotoxic effects of the nickel release from the stainless steel brackets: An in vitro study. J. Pharm. Bioallied Sci. 2013, 5, S1–S4. [Google Scholar] [CrossRef]
- Bhaskar, V.; Reddy, V.V. Biodegradation of nickel and chromium from stainless steel crowns and space maintainers—An in vitro study. Ann. Dent. Univ. Malaya 1997, 4, 17–21. [Google Scholar] [CrossRef]
- Barret, R.D.; Bishara, S.E.; Quinn, J.K. Biodegradation of nickel and chromium invitro. Am. J. Orthod. Dentofac. Orthop. 2015, 8, 37–41. [Google Scholar]


{kind=link}
| Component | Description |
|---|---|
| Population (P) | Subjects included in the study were undergoing orthodontic treatment with brackets on both jaws; with permanent dentition; those without metal crowns or restorations containing nickel or chromium; no history of orthodontic treatment; and patients of both sexes. |
| Exposure (E) | Saliva samples of subjects undergoing orthodontic treatment with brackets were analyzed by using atomic absorption spectrometry. |
| Comparison (C) | Nickel and chromium levels in saliva before and during orthodontic treatment were compared. |
| Outcomes (O) | Nickel and chromium levels in the saliva of patients wearing fixed orthodontic appliances (brackets) on both jaws increased. |
| Study design | Cohort studies that assessed and compared nickel and chromium levels in saliva before and during orthodontic treatment. |
| Keyword Combinations | Number of Articles | ||
|---|---|---|---|
| Pubmed | ReasearchGate | Google Scholar | |
| nickel [MeSH Terms] OR nickel [All Fields] AND chromium [MeSH Terms] OR chromium [All Fields] AND saliva [MeSH Terms] OR saliva [All Fields]) | 159 | 36 | 26 |
| saliva [All Fields] AND brackets [All Fields] AND atomic absorption spectrometer [All Fields] | 5 | 5 | 0 |
| nickel [All Fields] AND chromium [All Fields] AND saliva [All Fields] AND fixed orthodontic appliances [All Fields] | 40 | 12 | 9 |
| nickel [All Fields] AND chromium [All Fields] AND saliva [All Fields] AND in-vivo [All Fields] | 26 | 3 | 1 |
| nickel [All Fields] AND chromium [All Fields] AND brackets [All Fields] | 79 | 9 | 9 |
| Total | 309 | 65 | 45 |
| Final number of articles | 419 | ||
| Author | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting |
|---|---|---|---|---|---|---|
| A. Dwivedi et al. [2] | ? | ? | + | + | + | + |
| N. F. Talic et al. [13] | ? | ? | + | + | + | + |
| D. Quadras et al. [14] | ? | ? | + | + | + | + |
| B. Sunny et al. [15] | ? | ? | + | + | + | + |
| F. Amini et al. [16] | ? | + | + | + | + | + |
| R. S. Nayak et al. [17] | ? | + | + | + | + | + |
| A. Frois et al. [18] | ? | ? | + | + | + | + |
| S. Raina et al. [19] | ? | + | ? | + | + | + |
| L. Nanjanawar et al. [20] | ? | + | ? | + | + | + |
| M.S. Bengleil et al. [21] | + | + | + | + | + | + |
| D.P. Singhi et al. [22] | + | + | ? | + | ? | + |
| A. Jurela et al. [23] | ? | + | ? | + | ? | + |
| Author | Subject Groups (Number of Subjects) | Age of Subjects in Years | Time of Sampling | Results | Main Outcomes | |
|---|---|---|---|---|---|---|
| N.F. Talic [13] | EG (40) CG (50) | EG—20.1 ± 3.4 | After 1–32 months | After 1–32 months | Statistically significant differences were found in both nickel (p < 0.05) and chromium (p < 0.05) levels between EG and CG. | |
| CG—23.1 ± 4.2 | Nickel level: EG—4.197 lg/L CG—2.3 lg/L | Chromium level: EG—2.9 lg/L CG—3.3 lg/L | ||||
| D. Quadras [14] | EG (50) CG (30) | EG—24 ± 1.2 | Before the treatment; | Before the treatment | A significant increase in the metal ion levels were seen in participants before and after insertion of the appliance (p < 0.001). | |
| Nickel level: EG—4.24 ± 0.009 ng/mL CG—4.33 ± 0.002 | Chromium level: EG—1.18 ± 0.01 ng/mL CG—1.13 ± 0.03 | |||||
| after 1 week; | After 1 week | |||||
| CG—24 ± 1.2 | Nickel level: EG—4.34 ± 0.008 ng/mL CG—4.33 ± 0.002 ng/mL | Chromium level: EG—0.59 ± 0.026 ng/mL CG—1.13 ± 0.03 ng/mL | ||||
| after 3 months; | After 3 months | |||||
| Nickel level: EG—11.1 ± 0.009 ng/mL CG—4.33 ± 0.002 ng/mL | Chromium level: EG—1.57 ± 0.08 ng/mL CG—1.13 ± 0.03 ng/mL | |||||
| after 1 year; | After 1 year | |||||
| Nickel level: EG—6.84 ± 0.005 ng/mL CG—4.73 ± 0.002 ng/mL | Chromium level: EG—0.94 ±0.069 ng/mL CG—1.18 ± 0.03 ng/mL | |||||
| after 1.5 years. | After 1.5 years | |||||
| Nickel level: EG—67 ± 10.08 ng/mL CG—5.02 ± 0.001 ng/mL | Chromium level: EG—30.8 ± 4.3 ng/mL CG—1.27 ± 0.9 ng/mL | |||||
| B. Sunny [15] | CG (30) | 15–20 | Before the treatment | A statistically significant difference (p < 0.01) was found in CG in nickel ion levels. | ||
| Nickel level: CG—3.8 ng/mL | Chromium level: CG—13 ng/mL | |||||
| After 1 month | ||||||
| Nickel level: CG—5 ng/mL | Chromium level: CG—14.9 ng/mL | |||||
| F. Amini [16] | EG (28) CG (28) | 16–19 | After 12–18 months | After 12–18 months | A statistically significant difference (p < 0.035) was found between EG and CG in nickel levels. However, the difference in chromium levels between EG and CG was statistically insignificant. | |
| Nickel level: EG—18.5 ± 13.1 ng/mL CG—11.9 ± 11.4 ng/mL | Chromium level: EG—2.6 ± 1.6 ng/mL CG—2.2 ± 1.6 ng/mL | |||||
| A. Dwivedi [2] | EG (13) | 15–33 | Before the treatment; | Before the treatment | Statistically significant differences were found in both nickel (p < 0.05) and chromium (p < 0.05) levels between EG and CG before the treatment and after 1 week. | |
| Nickel level: EG—1.156 ± 0.675 ng/mL | Chromium level: EG—11.570 ± 2.145 ng/mL | |||||
| after 1 week; | After 1 week | |||||
| Nickel level: EG—6.841 ± 1.326 ng/mL | Chromium level: EG—70.386 ± 6.884 ng/mL | |||||
| after 1 month; | After 1 month | |||||
| Nickel level: EG—3.403 ± 1.631 ng/mL | Chromium level: EG—21.254 ± 5.099 ng/mL | |||||
| after 3 months. | After 3 months | |||||
| Nickel level: EG—3.124 ± 1.321 ng/mL | Chromium level: EG—20.002 ± 3.684 ng/mL | |||||
| R. S. Nayak [17] | EG (30) | 10–25 | Before the treatment; | Before the treatment | Statistically significant differences between EG and CG in nickel (p < 0.05) were found after 1 week and insignificant differences after 10–12 months. Statistically significant differences (p < 0.05) between EG and CG in chromium were found after 1 week and after 10–12 months. | |
| Nickel level: EG—48.78 ± 35.75 ng/mL | Chromium level: EG—69.74 ± 62.33 ng/mL | |||||
| after 1 week; | After 1 week | |||||
| Nickel level: EG—59.19 ± 32.82 ng/mL | Chromium level: EG—102.68 ± 68.65 ng/ml | |||||
| after 10–12 months. | After 10–12 months | |||||
| Nickel level: EG—46.33 ± 26.95 ng/mL | Chromium level: EG—87.07 ± 63.47 ng/mL | |||||
| A. Frois [18] | EG (17) | 20 ± 8 | Before the treatment; | Before the treatment | No statistically significant variations were observed between the different study times (p > 0.05). | |
| Nickel level: EG—153.7 μg/L | Chromium level: EG—174.0 μg/L | |||||
| after 2 days; | After 2 days | |||||
| Nickel level: EG—135.3 μg/L | Chromium level: EG—171.4 μg/L | |||||
| after 1 week; | After 1 week | |||||
| Nickel level: EG—145.1 μg/L | Chromium level: EG—180.4 μg/L | |||||
| after 4 weeks; | After 4 weeks | |||||
| Nickel level: EG—175.1 μg/L | Chromium level: EG—192.4 μg/L | |||||
| after 12 weeks. | After 12 weeks | |||||
| Nickel level: EG—131.5 μg/L | Chromium level: EG—173.3 μg/L | |||||
| S. Raina [19] | EG (20) CG (20) | 16.5–17.5 | During the treatment | During the treatment | Statistically significant differences were found between EG and CG in nickel levels (p < 0.05). | |
| Nickel level: EG—18.9 ng/mL CG -12.3 ng/mL | ||||||
| L. Nanjannawar [20] | CG (21) | 12–25 | During the treatment | During the treatment | Statistically significant differences were not found in nickel levels (p > 0.05). | |
| Nickel level: CG—0.008 | ||||||
| Mudafara S. Bengleil [21] | EG (9) CG (9) | 15–22 | Before the treatment; | Before the treatment | Statistically significant differences were not found between EG and CG in nickel levels (p > 0.05) throughout the entire research period. | |
| Nickel level: EG—0.097 mg/L CG—0.066 mg/L | ||||||
| after braces placement; | After braces placement | |||||
| Nickel level: EG—0.097 mg/L CG—0.074 mg/L | ||||||
| after 2 weeks; | After 2 weeks | |||||
| Nickel level: EG—0.091 mg/L CG—0.079 mg/L | ||||||
| after 4 weeks; | After 4 weeks | |||||
| Nickel level: EG—0.208 mg/L CG—0.061 mg/L | ||||||
| after 8 weeks. | After 8 weeks | |||||
| Nickel level: EG—0.071 mg/L CG—0.008 mg/L | ||||||
| Depinder Pal Singh [22] | EG (32) CG (32) | 12–33 | During the treatment | During the treatment | Statistically significant differences were found between EG and CG in nickel levels (p < 0.05). | |
| Nickel level: EG—20.5 ng/mL CG—12.3 ng/mL | ||||||
| Antonija Jurela [23] | EG (42) CG (42) | 11–26 | Before the treatment | Before the treatment | Statistically significant differences between EG and CG in nickel levels (p < 0.05) were found. Statistically significant differences (p < 0.05) between EG and CG in chromium were also found. | |
| Nickel level: EG—4.24 μg/L CG—5.53 μg/L | Chromium level: EG—1.95 μg/L CG—2.77 μg/L | |||||
| After the treatment | After the treatment | |||||
| Nickel level: EG—5.04 μg/L CG—4.39 μg/L | Chromium level: EG—0.01 ng/mL CG—1.00 ± 0.9 ng/mL | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urbutytė, K.; Barčiūtė, A.; Lopatienė, K. The Changes in Nickel and Chromium Ion Levels in Saliva with Fixed Orthodontic Appliances: A Systematic Review. Appl. Sci. 2023, 13, 4739. https://doi.org/10.3390/app13084739
Urbutytė K, Barčiūtė A, Lopatienė K. The Changes in Nickel and Chromium Ion Levels in Saliva with Fixed Orthodontic Appliances: A Systematic Review. Applied Sciences. 2023; 13(8):4739. https://doi.org/10.3390/app13084739
Chicago/Turabian StyleUrbutytė, Klaudija, Andrė Barčiūtė, and Kristina Lopatienė. 2023. "The Changes in Nickel and Chromium Ion Levels in Saliva with Fixed Orthodontic Appliances: A Systematic Review" Applied Sciences 13, no. 8: 4739. https://doi.org/10.3390/app13084739
APA StyleUrbutytė, K., Barčiūtė, A., & Lopatienė, K. (2023). The Changes in Nickel and Chromium Ion Levels in Saliva with Fixed Orthodontic Appliances: A Systematic Review. Applied Sciences, 13(8), 4739. https://doi.org/10.3390/app13084739