
A Linkage Representation of the Human Hand Skeletal System Using CT Hand Scan Images



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. CT Data Acquisition and Processing
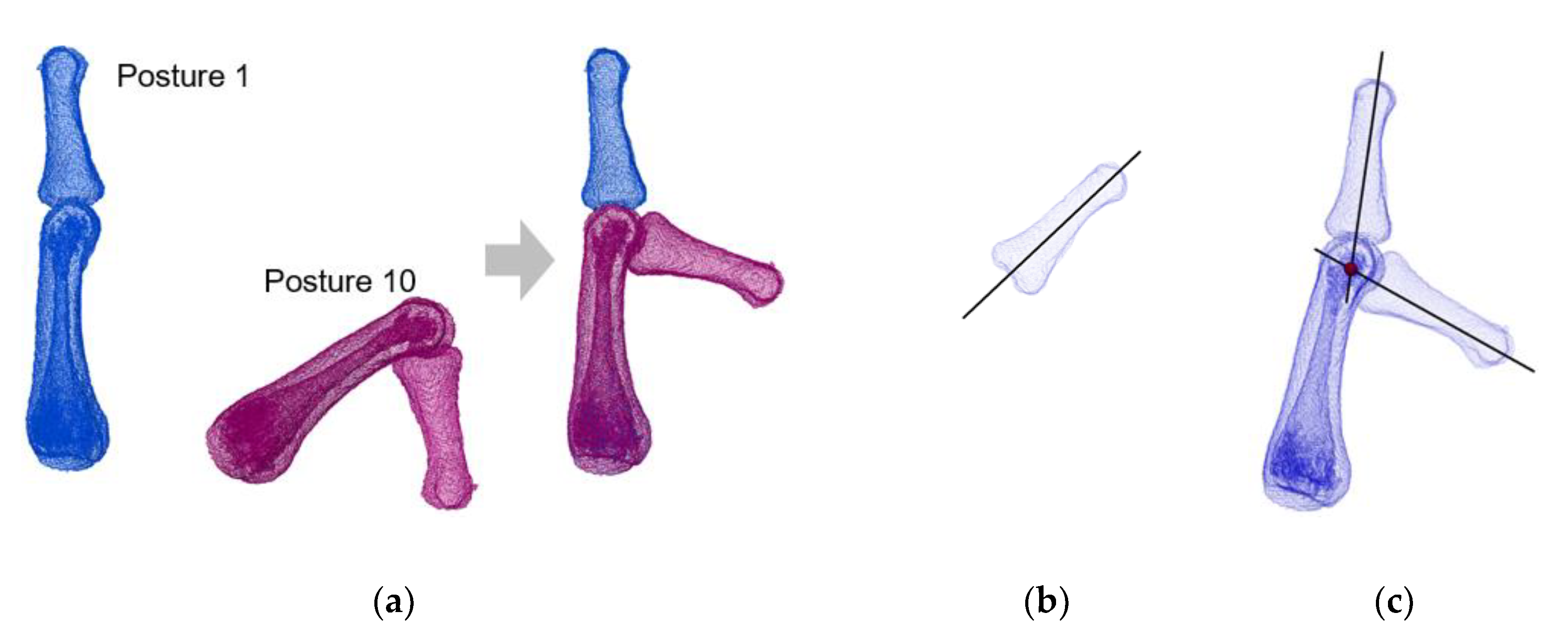
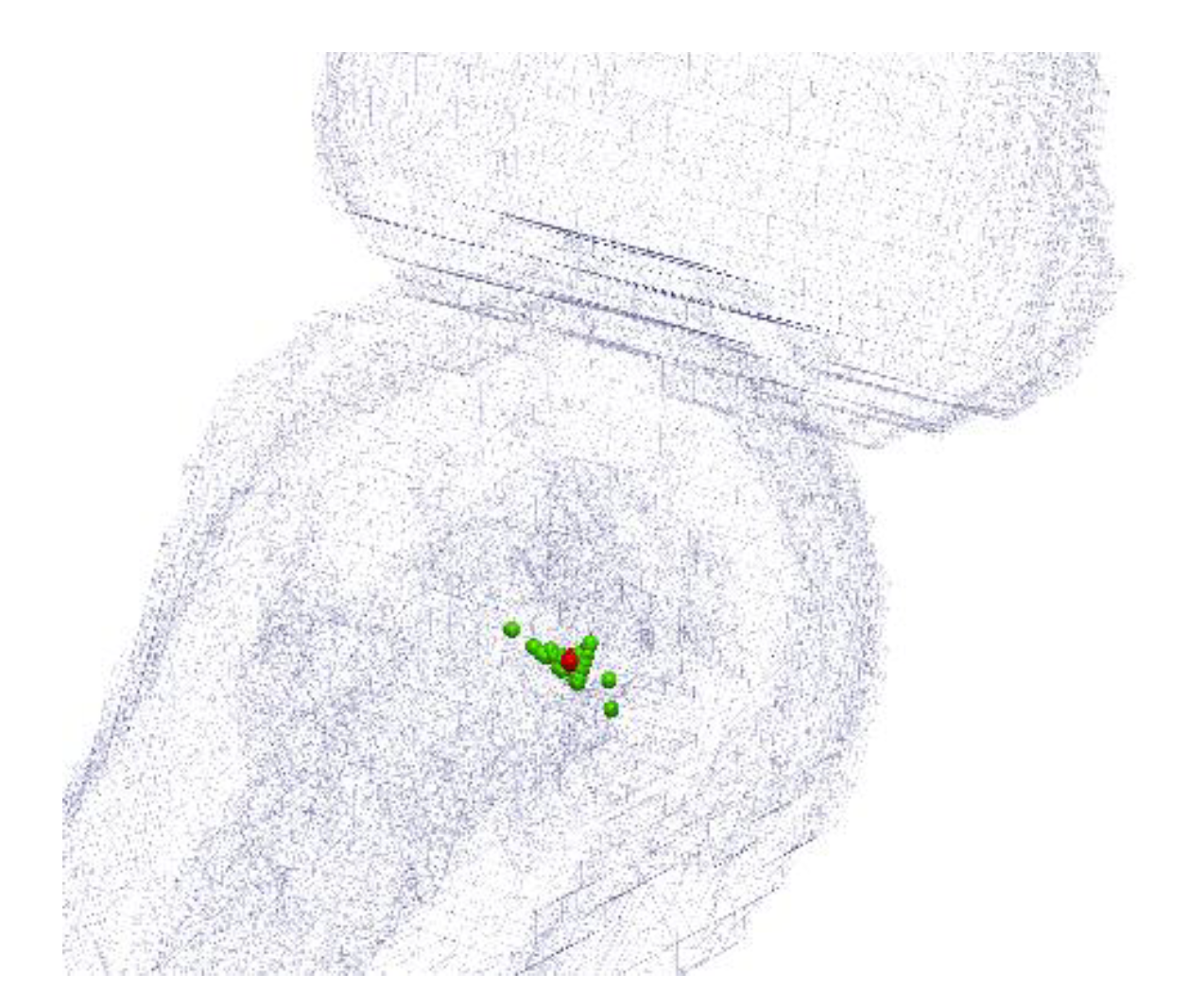
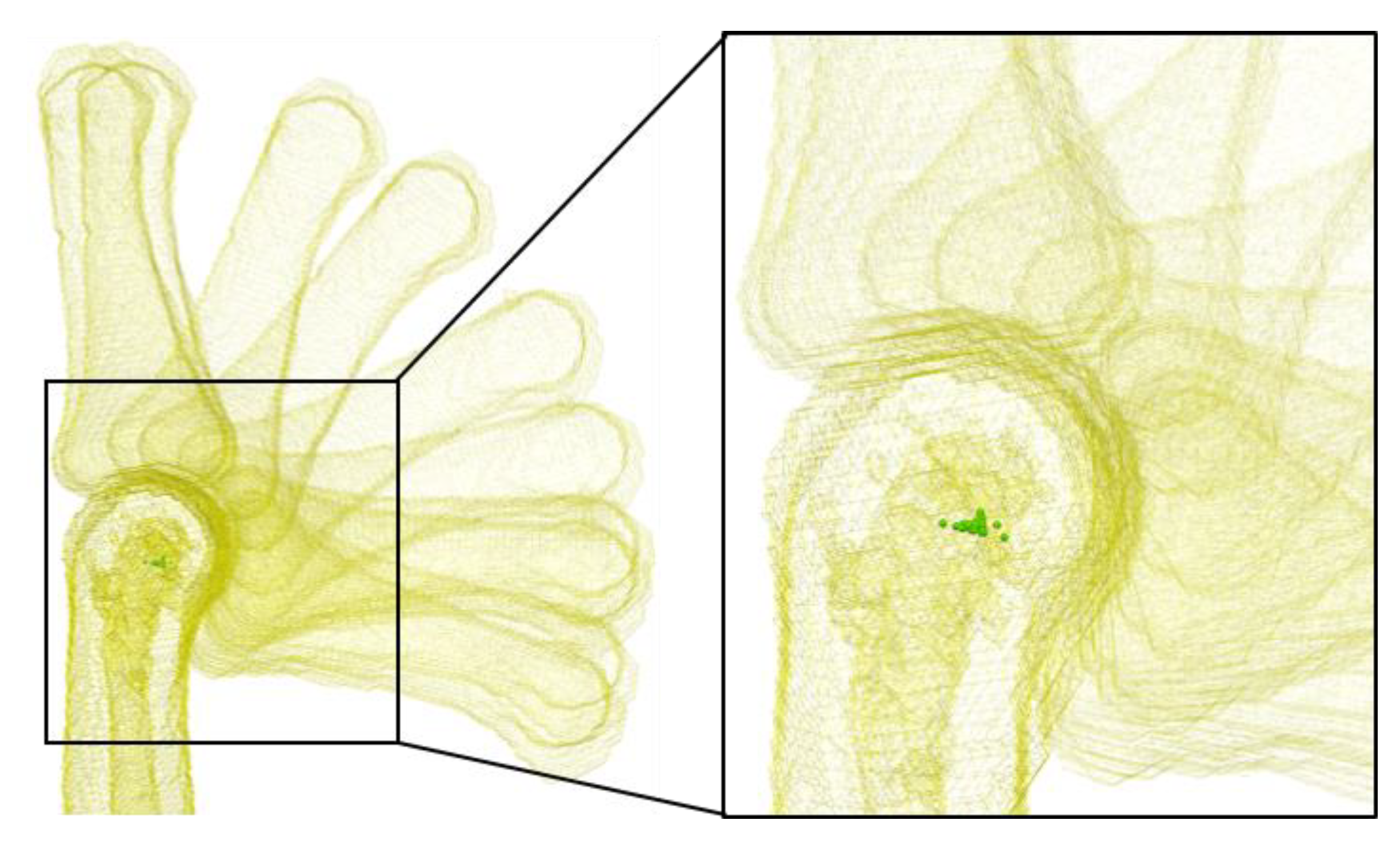
2.3. Joint Centers Estimation
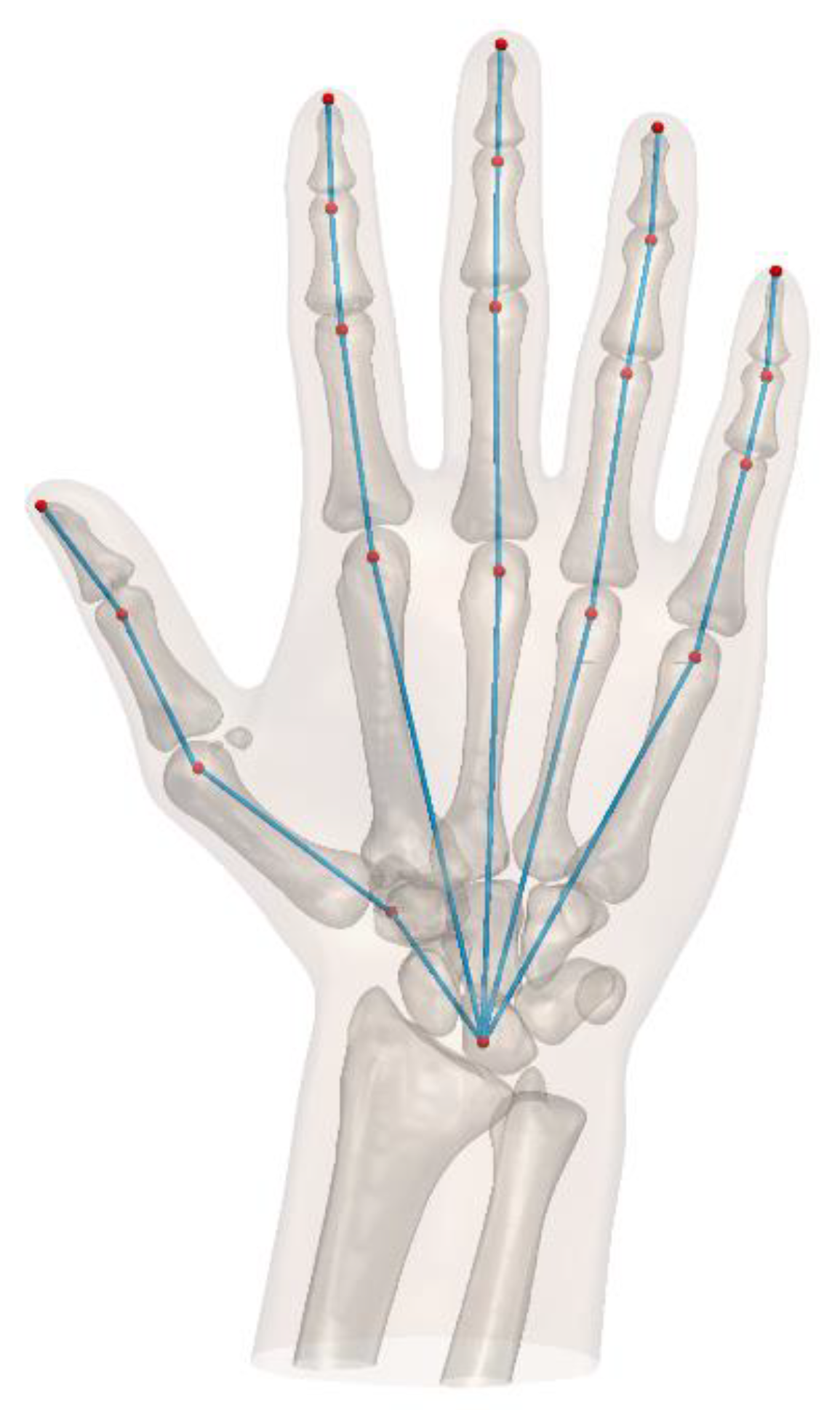
2.4. Linkage System Establishment
2.5. Regression Models Establishment
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zhang, X.; Lee, S.-W.; Braido, P. Towards an integrated high-fidelity linkage representation of the human skeletal system based on surface measurement. Int. J. Ind. Ergon. 2004, 33, 215–227. [Google Scholar] [CrossRef]
- Zhang, X. Deformation of angle profiles in forward kinematics for nullifying end-point offset while preserving movement properties. J. Biomech. Eng. 2002, 124, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Risher, D.W.; Schutte, L.M.; Runge, C.F. The use of inverse dynamics solutions in direct dynamics simulations. J. Biomech. Eng. 1997, 119, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Kroemer, K.H.E. Engineering anthropometry. Ergonomics 1989, 32, 767–784. [Google Scholar] [CrossRef]
- Roebuck, J.A.; Kroemer, K.H.E.; Thomson, W.G. Engineering Anthropometry Methods; Wiley: New York, NY, USA, 1975. [Google Scholar]
- Roebuck, J.A. Anthropometric Methods: Designing to Fit the Human Body; Human Factors and Ergonomics Society: Santa Monica, CA, USA, 1995. [Google Scholar]
- Chaffin, D.B.; Andersson, G.B.J.; Martin, B.J. Occupational Biomechanics, 3rd ed.; Wiley: New York, NY, USA, 1999. [Google Scholar]
- Buchholz, B.; Armstrong, T.J.; Goldstein, A. Anthropometric data for describing the kinematics of the human hand. Ergonomics 1992, 35, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Reuleaux, F. The Kinematics of Machinery: Outline of a Theory of Machines; Kennedy, A.B.W., Translator; MacMillan and Co.: London, UK, 1876. [Google Scholar]
- Fowler, N.K.; Nicol, A.C.; Condon, B.; Hadley, D. Method of determination of three dimensional index finger moment arms and tendon lines of action using high resolution MRI scans. J. Biomech. 2001, 34, 791–797. [Google Scholar] [CrossRef]
- Halvorsen, K.; Lesser, M.; Lundberg, A. A new method for estimating the axis of rotation and the center of rotation. J. Biomech. 1999, 32, 1221–1227. [Google Scholar] [CrossRef]
- Knight, J.K.; Semwal, S.K. Unbiased closed-form solutions for center of rotation. In Computer Vision, Imaging and Computer Graphics. Theory and Applications; Ranchordas, A., Pereira, J.M., Araújo, H.J., Tavares, J.M.R.S., Eds.; VISIGRAPP 2009, Communications in Computer and Information Science, 68; Springer: Berlin/Heidelberg, Germany, 2010; pp. 73–88. [Google Scholar]
- Piazza, S.J.; Erdemir, A.; Okita, N.; Cavanagh, P.R. Assessment of the functional method of hip joint center location subject to reduced range of hip motion. J. Biomech. 2004, 37, 349–356. [Google Scholar] [CrossRef]
- Zhang, X.; Lee, S.-W.; Braido, P. Determining finger segmental centers of rotation in flexion–extension based on surface marker measurement. J. Biomech. 2003, 36, 1097–1102. [Google Scholar] [CrossRef]
- Yang, X.; Lim, Z.; Jung, H.; Hong, Y.; Zhang, M.; Park, D.; You, H. Estimation of finite finger joint centers of rotation using 3D hand skeleton motions reconstructed from CT scans. Appl. Sci. 2020, 10, 9129. [Google Scholar] [CrossRef]
- Nolden, M.; Zelzer, S.; Seitel, A.; Wald, D.; Müller, M.; Franz, A.M.; Maleike, D.; Fangerau, M.; Baumhauer, M.; Maier-Hein, L.; et al. The medical imaging interaction toolkit: Challenges and advances: 10 years of open-source development. Int. J. Comput. Assist. Radiol. Surg. 2013, 8, 607–620. [Google Scholar] [CrossRef] [PubMed]
- Besl, P.J.; McKay, N.D. A method for registration of 3-D shapes. IEEE Trans. Pattern Anal. Mach. Intell. 1992, 14, 239–256. [Google Scholar] [CrossRef]
- Dempster, W.T. Space Requirements of the Seated Operator: Geometrical, Kinematic, and Mechanical Aspects of the Body with Special Reference to the Limbs; Wright Air Development Center Technical Report; Wright-Patterson Air Force Base: Greene, OH, USA, 1955. [Google Scholar]
- Kanungo, T.; Mount, D.M.; Netanyahu, N.S.; Silverman, R.; Piatko, C.D.; Wu, A.Y. An efficient k-means clustering algorithm: Analysis and implementation. IEEE Trans. Pattern Anal. Mach. Intell. 2002, 24, 881–892. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection. 1990 Recommendations of the International Commission on Radiological Protection; ICRP Publication 60; Pergamon Press: Oxford, UK, 1991. [Google Scholar]
- Feix, T.; Kivell, T.L.; Pouydebat, E.; Dollar, A.M. Estimating thumb–index finger precision grip and manipulation potential in extant and fossil primates. J. R. Soc. Interface 2015, 12, 20150176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karakostis, F.A.; Haeufle, D.; Anastopoulou, I.; Moraitis, K.; Hotz, G.; Tourloukis, V.; Harvati, K. Biomechanics of the human thumb and the evolution of dexterity. Curr. Biol. 2021, 31, 1317–1325. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Finger | Joint 1 | Joint 2 | Joint 3 | Bone Tip | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| x | y | z | x | y | z | x | y | z | x | y | z | |
| Thumb | −21.28 | 20.81 | −22.29 | −56.92 | 46.32 | −14.02 | −71.19 | 74.12 | −9.77 | −85.52 | 93.31 | −4.01 |
| Index | −22.85 | 85.41 | 0.00 | −29.84 | 125.91 | 0.28 | −33.45 | 148.23 | −3.80 | −34.53 | 167.84 | −3.30 |
| Middle | 0.00 | 83.51 | 0.00 | −3.06 | 131.01 | −4.84 | −4.38 | 158.07 | −10.28 | −4.26 | 178.90 | −8.80 |
| Ring | 15.85 | 76.70 | -6.95 | 20.05 | 120.37 | −13.07 | 22.94 | 145.64 | −20.02 | 23.66 | 165.85 | −18.04 |
| Little | 34.44 | 69.58 | -9.72 | 42.07 | 104.60 | −13.93 | 44.92 | 120.93 | −18.17 | 45.94 | 140.19 | −19.38 |
| Finger | Segment 1 | Segment 2 | Segment 3 | Segment 4 |
|---|---|---|---|---|
| Thumb | 0.190 ± 0.003 (0.996, −4.0–3.7, [0.184, 0.196]) | 0.233 ± 0.002 (0.998, −2.5–3.7, [0.229, 0.237]) | 0.179 ± 0.002 (0.998, −2.7–3.0, [0.175, 0.183]) | 0.137 ± 0.002 (0.998, −2.1–2.2, [0.133, 0.141]) |
| Index | 0.476 ± 0.005 (0.998, −7.0–4.9, [0.465, 0.487]) | 0.231 ± 0.002 (0.999, −2.2–2.7, [0.227, 0.235]) | 0.128 ± 0.001 (0.999, −1.5–2.1, [0.126, 0.130]) | 0.109 ± 0.002 (0.996, −2.7–1.8, [0.105, 0.113]) |
| Middle | 0.458 ± 0.004 (0.999, −4.8–5.8, [0.449, 0.467]) | 0.258 ± 0.002 (0.999, −3.5–2.2, [0.254, 0.262]) | 0.151 ± 0.001 (0.999, −2.1–2.2, [0.149, 0.153]) | 0.116 ± 0.002 (0.997, −2.3–1.8, [0.112, 0.120]) |
| Ring | 0.433 ± 0.004 (0.999, −5.6–4.0, [0.424, 0.442]) | 0.241 ± 0.003 (0.999, −3.8–3.0, [0.235, 0.247]) | 0.145 ± 0.001 (0.999, −1.5–1.4, [0.143, 0.147]) | 0.118 ± 0.002 (0.997, −2.8–1.8, [0.114, 0.122]) |
| Little | 0.425 ± 0.004 (0.999, −7.0–3.3, [0.416, 0.434]) | 0.192 ± 0.002 (0.999, −1.8–3.0, [0.188, 0.196]) | 0.100 ± 0.003 (0.991, −3.2–2.6, [0.094, 0.106]) | 0.105 ± 0.002 (0.997, −2.8–1.4, [0.101, 0.109]) |
| Coordinate | Thumb | Index | Middle | Ring | Little |
|---|---|---|---|---|---|
| x | −0.261 ± 0.008 (0.986, −6.9–6.0, [−0.278, −0.244]) | −0.264 ± 0.003 (0.998, −2.1-1.4, [−0.270, −0.258]) | 0.000 1 (-) | 0.208 ± 0.003 (0.997, −2.1–1.7, [0.202, 0.214]) | 0.403 ± 0.005 (0.998, −3.8-3.4, [0.392, 0.414]) |
| y | 0.110 ± 0.003 (0.990, −3.5–4.5, [0.104, 0.116]) | 0.461 ± 0.005 (0.998, −6.9–5.4, [0.450, 0.472]) | 0.458 ± 0.004 (0.999, −4.8-5.8, [0.449, 0.467]) | 0.421 ± 0.004 (0.999, −5.4–4.0, [0.412, 0.430]) | 0.380 ± 0.004 (0.999, −5.9-4.0, [0.371, 0.389]) |
| z | −0.225 ± 0.005 (0.993, −2.8–3.1, [−0.236, −0.214]) | 0.000 1 (-) | 0.000 1 (-) | −0.028 ± 0.003 (0.883, −5.0–2.8, [−0.034, −0.022]) | −0.054 ± 0.005 (0.889, −8.7-4.3, [−0.065, −0.043]) |
| Finger | Segment 1 | Segment 2 | Segment 3 | Segment 4 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Actural | Estimated | Difference | Actural | Estimated | Difference | Actural | Estimated | Difference | Actural | Estimated | Difference | |
| Thumb | 35.8 | 35.9 | 0.1 | 47.9 | 44.0 | −3.9 | 35.0 | 33.8 | −1.2 | 26.0 | 25.9 | −0.1 |
| Index | 91.9 | 90.0 | −1.9 | 41.3 | 43.7 | 2.4 | 23.8 | 24.2 | 0.4 | 21.1 | 20.6 | −0.5 |
| Middle | 86.1 | 86.6 | 0.5 | 47.6 | 48.8 | 1.2 | 27.2 | 28.5 | 1.3 | 22.5 | 21.9 | −0.6 |
| Ring | 81.4 | 81.8 | 0.4 | 44.0 | 45.5 | 1.5 | 24.9 | 27.4 | 2.5 | 23.3 | 22.3 | −1.0 |
| Little | 77.8 | 80.3 | 2.5 | 33.8 | 36.3 | 2.5 | 18.7 | 18.9 | 0.2 | 20.5 | 19.8 | −0.7 |
| Finger | x | y | z | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Actural | Estimated | Difference | Actural | Estimated | Difference | Actural | Estimated | Difference | |
| Thumb | −22.8 | −24.5 | −1.7 | 21.0 | 20.8 | −0.2 | −18.1 | −21.2 | −3.1 |
| Index | −24.7 | −24.8 | −0.1 | 88.5 | 87.1 | −1.4 | 0.0 | 0.0 | 0.0 |
| Middle | 0.0 | 0.0 | 0.0 | 86.1 | 86.6 | 0.5 | 0.0 | 0.0 | 0.0 |
| Ring | 18.2 | 19.6 | 1.4 | 79.0 | 79.6 | 0.6 | −7.0 | −5.3 | 1.7 |
| Little | 35.1 | 37.9 | 2.8 | 68.3 | 71.8 | 3.5 | −12.3 | −10.2 | 2.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, Y.; Yang, X.; Lim, Z.; Jung, H.; Park, D.; You, H. A Linkage Representation of the Human Hand Skeletal System Using CT Hand Scan Images. Appl. Sci. 2021, 11, 5857. https://doi.org/10.3390/app11135857
Cao Y, Yang X, Lim Z, Jung H, Park D, You H. A Linkage Representation of the Human Hand Skeletal System Using CT Hand Scan Images. Applied Sciences. 2021; 11(13):5857. https://doi.org/10.3390/app11135857
Chicago/Turabian StyleCao, Ying, Xiaopeng Yang, Zhichan Lim, Hayoung Jung, Dougho Park, and Heecheon You. 2021. "A Linkage Representation of the Human Hand Skeletal System Using CT Hand Scan Images" Applied Sciences 11, no. 13: 5857. https://doi.org/10.3390/app11135857
APA StyleCao, Y., Yang, X., Lim, Z., Jung, H., Park, D., & You, H. (2021). A Linkage Representation of the Human Hand Skeletal System Using CT Hand Scan Images. Applied Sciences, 11(13), 5857. https://doi.org/10.3390/app11135857