
The Variation in 3D Face Shapes of Dutch Children for Mask Design

 , ,
, ,  and
and
Abstract
1. Introduction
2. Method
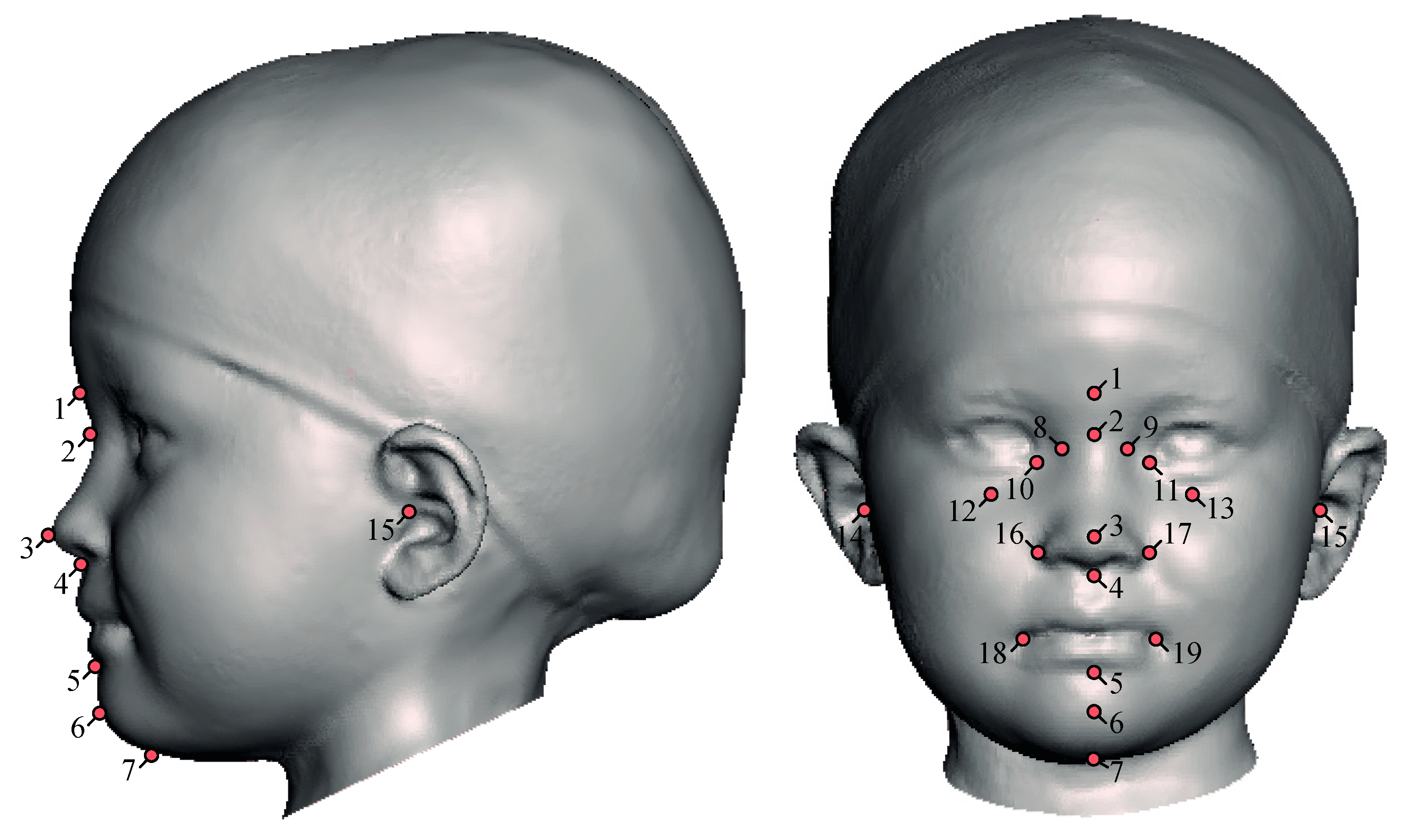
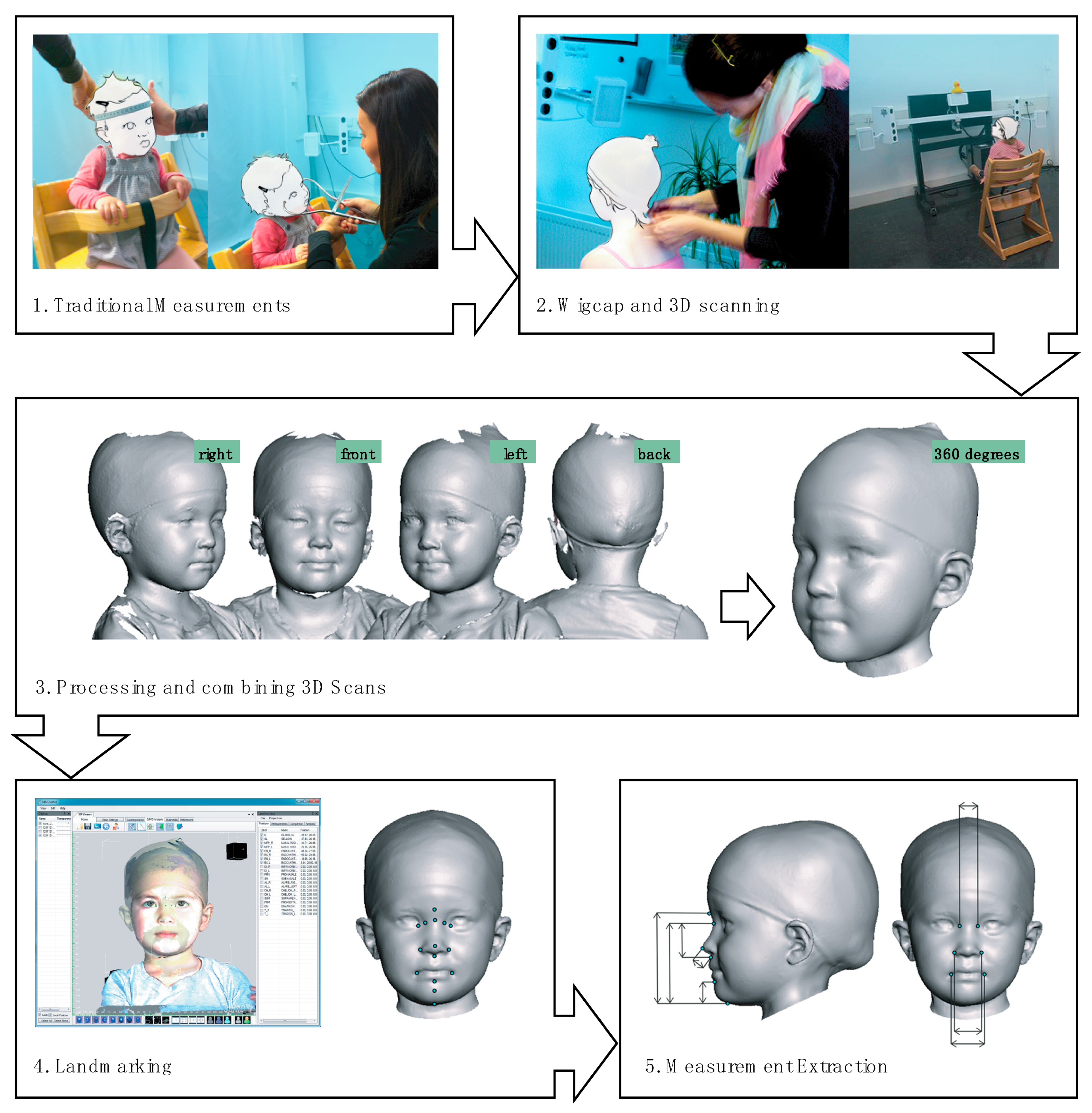
2.1. Participants and Data Collection
2.2. Data Analysis Procedure
2.2.1. Comparison between Genders
2.2.2. Measurement Based Analysis of Face Variation
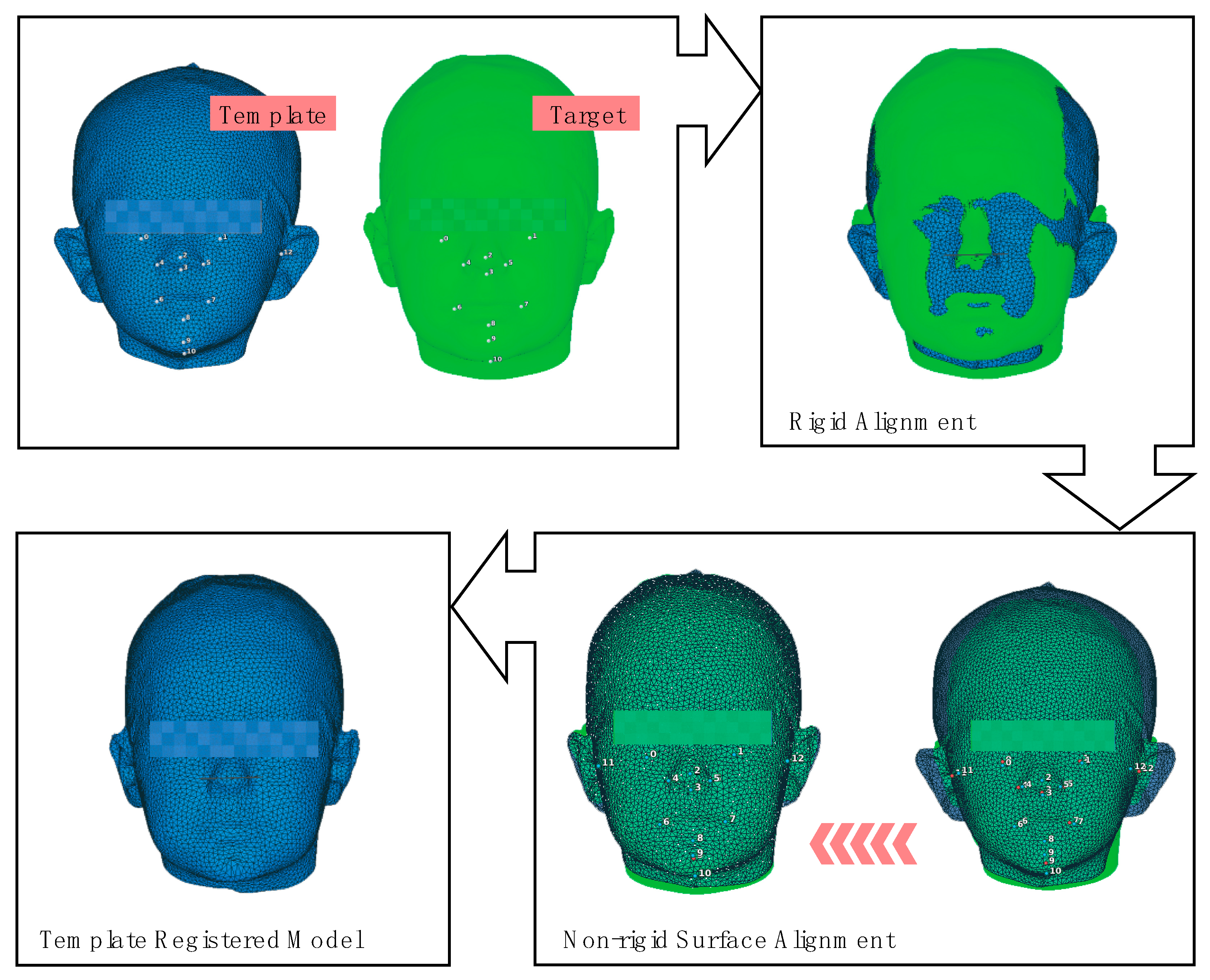
2.2.3. 3D Shape Based Analysis of Face Variation
3. Results
3.1. Gender Comparison
3.2. Face Variation
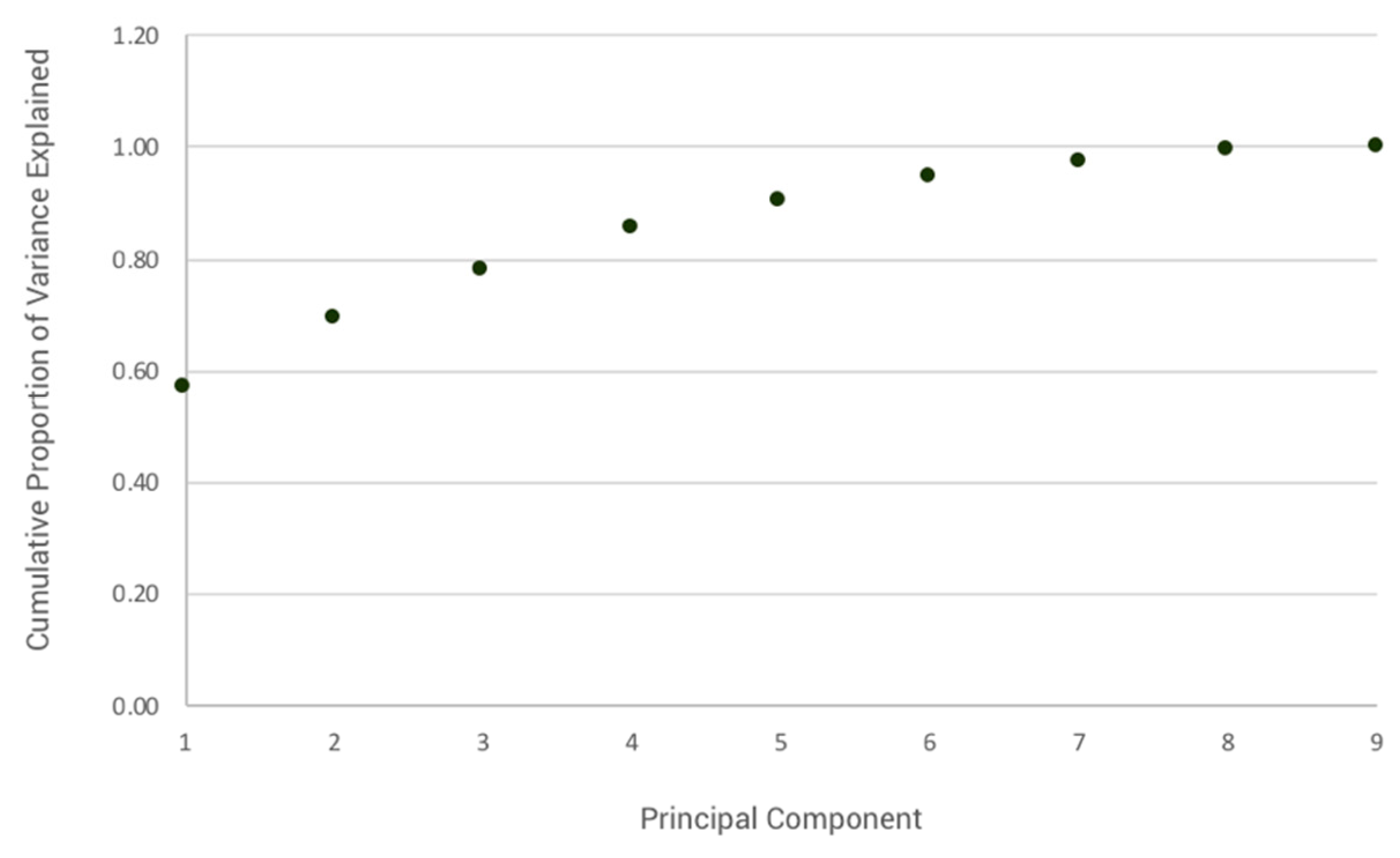
3.3. Face Shape Variation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hsiao, H. Anthropometric Procedures for Protective Equipment Sizing and Design. Hum. Factors J. Hum. Factors Erg. Soc. 2013, 55, 6–35. [Google Scholar] [CrossRef]
- Lee, W.; Yang, X.; Jung, D.; Park, S.; Kim, H.; You, H. Ergonomic evaluation of pilot oxygen mask designs. Appl. Erg. 2018, 67, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Drinnan, M.; Hyde, P.; Munguia, J. Mask interface for continuous positive airway pressure therapy: Selection and design considerations. Expert Rev. Med. Devices 2018, 15, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Nicki, B.; Matt, W.; Heather, E. A Review of the Benefits, Challenges and the Future for Interfaces for Long Term Non-Invasive Ventilation in Children. Int. J. Respir. Pulm. Med. 2018, 5, 1–7. [Google Scholar] [CrossRef]
- Luximon, Y.; Ball, R.; Justice, L. The 3D Chinese head and face modeling. Comput. Des. 2012, 44, 40–47. [Google Scholar] [CrossRef]
- Lacko, D.; Huysmans, T.; Parizel, P.M.; De Bruyne, G.; Verwulgen, S.; Van Hulle, M.; Sijbers, J. Evaluation of an anthropometric shape model of the human scalp. Appl. Erg. 2015, 48, 70–85. [Google Scholar] [CrossRef]
- Zhuang, Z.; Benson, S.; Slice, D.; Viscusi, D.; Lynch, S. Shape analysis of 3D head scan data for U.S. respirator users. EURASIP J. Adv. Signal. Process. 2010, 2010, 248954. [Google Scholar] [CrossRef]
- Lee, W.; Lee, B.; Yang, X.; Jung, H.; Bok, I.; Kim, C.; Kwon, O.; You, H. A 3D anthropometric sizing analysis system based on North American CAESAR 3D scan data for design of head wearable products. Comput. Ind. Eng. 2018, 117, 121–130. [Google Scholar] [CrossRef]
- Bolkart, T.; Bose, P.; Shu, C.; Wuhrer, S. A general framework to generate sizing systems from 3D motion data applied to face mask design. In Proceedings of the 2014 2nd International Conference on 3D Vision, Tokyo, Japan, 8–11 December 2014; pp. 425–431. [Google Scholar] [CrossRef]
- Kouchi, M.; Mochimaru, M. Analysis of 3D face forms for proper sizing and CAD of spectacle frames. Ergonomics 2004, 47, 1499–1516. [Google Scholar] [CrossRef]
- Zhuang, Z.; Benson, S.; Viscusi, D. Digital 3-D headforms with facial features representative of the current US workforce. Ergonomics 2010, 53, 661–671. [Google Scholar] [CrossRef]
- Yu, Y.; Benson, S.; Cheng, W.; Hsiao, J.; Liu, Y.; Zhuang, Z.; Chen, W. Digital 3-D headforms representative of Chinese workers. Ann. Occup. Hyg. 2011, 56, 113–122. [Google Scholar] [CrossRef][Green Version]
- Ellena, T.; Skals, S.; Subic, A.; Mustafa, H.; Pang, T.Y. 3D digital headform models of Australian cyclists. Appl. Erg. 2017, 59, 11–18. [Google Scholar] [CrossRef]
- Liu, H.; Li, Z.; Zheng, L. Rapid preliminary helmet shell design based on three-dimensional anthropometric head data. J. Eng. Des. 2008, 19, 45–54. [Google Scholar] [CrossRef]
- Lee, W.; Jeong, J.; Park, J.; Jeon, E.; Kim, H.; Jung, D.; Park, S.; You, H. Analysis of the facial measurements of Korean Air Force pilots for oxygen mask design. Ergonomics 2013, 56, 1451–1464. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.-H.; Huang, S.-H.; Yang, C.-K.; Tseng, C.-Y. Design customization of respiratory mask based on 3D face anthropometric data. Int. J. Precis. Eng. Manuf. 2015, 16, 487–494. [Google Scholar] [CrossRef]
- Lacko, D.; Vleugels, J.; Fransen, E.; Huysmans, T.; De Bruyne, G.; Van Hulle, M.; Sijbers, J.; Verwulgen, S. Ergonomic design of an EEG headset using 3D anthropometry. Appl. Erg. 2017, 58, 128–136. [Google Scholar] [CrossRef]
- Ulijaszek, S.; Bogin, B. Patterns of Human Growth. Man 1989, 24, 529. [Google Scholar] [CrossRef]
- Child Anthropometry: A literature scan of national and international publications; The Canadian Institute of Child Health: Ottawa, CA, USA, 2007.
- Bradtmiller, B. Sizing head forms: Design and development. SAE Tech. Pap. Ser. 1996, 443–450. [Google Scholar] [CrossRef]
- Kim, H.; Seo, H.; Myong, J.-P.; Yoon, J.-S.; Song, Y.; Kim, C. Developing Yellow Dust and Fine Particulate Masks for Children. J. Korean Soc. Occup. Env. Hyg. 2016, 26, 350–366. [Google Scholar] [CrossRef]
- Young, J.W. Selected Facial Measurements of Children for Oxygen-Mask Design; AM 66-9; United States Office of Aviation Medicine: Washington, DC, USA, 1966; pp. 1–11. [Google Scholar]
- Amirav, I.; Masumbuko, C.K.; Hawkes, M.T.; Solomon, I.; Aldar, Y.; Margalit, G.; Zvirin, A.; Honen, Y.; Sivasivugha, E.S.; Kimmel, R. 3D analysis of child facial dimensions for design of medical devices in low-middle income countries (LMIC). PLoS ONE 2019, 14, e0216548. [Google Scholar] [CrossRef]
- Lueder, R.; Berg Rice, V.J. (Eds.) Ergonomics for Children—Designing Products and Places for Toddlers to Teens; Taylor & Francis Group: London, UK, 2008; ISBN 9780415304740. [Google Scholar]
- Amirav, I.; Luder, A.S.; Halamish, A.; Raviv, D.; Kimmel, R.; Waisman, D.; Newhouse, M.T. Design of aerosol face masks for children using computerized 3D face analysis. J. Aerosol Med. Pulm. Drug Deliv. 2014, 27, 272–278. [Google Scholar] [CrossRef]
- Seo, H.; Song, Y.; Kim, C.; Kim, H. Characteristics of Korean children’s facial anthropometry evaluated by three-dimensional imaging. J. Int. Soc. Respir. Prot. 2016, 33, 23–38. [Google Scholar]
- Lee, W.; Goto, L.; Molenbroek, J.F.M.; Goossens, R.H.M.; Wang, C.C.C. A shape-based sizing system for facial wearable product design. In Proceedings of the 5th International Digital Human Modeling Symposium; Wischniewski, S., Bonin, D., Alexander, T., Eds.; Federal Institute for Occupational Safety and Health: Berlin, Germany, 2017; pp. 150–158. [Google Scholar]
- Goto, L.; Lee, W.; Molenbroek, J.F.; Cabo, A.J.; Goossens, R.H. Traditional and 3D scan extracted measurements of the heads and faces of Dutch children. Int. J. Ind. Erg. 2019, 73, 73. [Google Scholar] [CrossRef]
- Luximon, A.; Zhang, Y.; Luximon, Y.; Xiao, M. Sizing and grading for wearable products. Comput. Des. 2012, 44, 77–84. [Google Scholar] [CrossRef]
- Molenbroek, J.F.; Goossens, R.H.; You, H.; Goto, L.; Jung, H.; Yang, X.; Lee, W. Application of massive 3D head and facial scan datasets in ergonomic head-product design. Int. J. Digit. Hum. 2016, 1, 344. [Google Scholar] [CrossRef]
- Zhuang, Z.; Bradtmiller, B.; Shaffer, R.E. New Respirator Fit Test Panels Representing the Current U.S. Civilian Work Force. J. Occup. Env. Hyg. 2007, 4, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Lacko, D.; Huysmans, T.; Vleugels, J.; De Bruyne, G.; Van Hulle, M.M.; Sijbers, J.; Verwulgen, S. Product sizing with 3D anthropometry andk-medoids clustering. Comput. Des. 2017, 91, 60–74. [Google Scholar] [CrossRef]
- Xi, P.; Shu, C. Consistent parameterization and statistical analysis of human head scans. Vis. Comput. 2009, 25, 863–871. [Google Scholar] [CrossRef]
- Meunier, P.; Shu, C.; Xi, P. Revealing the internal structure of human variability for design purposes. In Proceedings of the 17th World Congress on Ergonomics, Beijing, China, 9 August 2009. [Google Scholar]
- Medialdea, L.; Bazaco, C.; Del Campo, M.D.D.; Sierra-Martínez, C.; González-José, R.; Vargas, A.; Marrodán, M.D. Describing the children’s body shape by means of Geometric Morphometric techniques. Am. J. Phys. Anthr. 2019, 168, 651–664. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zhuang, Z.; Benson, S.; Du, L.; Yu, D.; Landsittel, U.; Wang, L.; Viscusi, D.; Shaffer, R.E. New Respirator Fit Test Panels Representing the Current Chinese Civilian Workers. Ann. Occup. Hyg. 2009, 53, 297–305. [Google Scholar] [CrossRef][Green Version]
- Zhuang, Z.; Shu, C.; Xi, P.; Bergman, M.; Joseph, M. Head-and-face shape variations of U.S. civilian workers. Appl. Erg. 2013, 44, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Luximon, Y.; Ball, R.M.; Justice, L. The Chinese face: A 3D anthropometric analysis. In Proceedings of the 8th International Symposium on Tools and Methods of Competitive Engineering, Ancona, Italy, 12–16 April 2010; Volume 1, pp. 255–265. [Google Scholar]
- Luximon, Y.; Ball, R.M.; Chow, E.H. A design and evaluation tool using 3D head templates. Comput. Des. Appl. 2015, 13, 153–161. [Google Scholar] [CrossRef]
- Goto, L.; Molenbroek, J.F.; Goossens, R.H. 3D Anthropometric Data Set of the Head and Face of Children Aged 0.5–6 Years for Design Applications. In Proceedings of the Proceedings of the 4th International Conference on 3D Body Scanning Technologies, Long Beach, CA, USA, 19–20 November 2013; pp. 157–165. [Google Scholar]
- ISO 15535. General Requirements for Establishing Anthropometric Databases; ISO: Geneva, Switzerland, 2007. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Dyke, R.M.; Zhou, F.; Lai, Y.-K.; Rosin, P.L.; Guo, D.; Li, K.; Marin, R.; Yang, J. SHREC’20: Non-rigid shape correspondence of physically-based deformations. In Proceedings of the Eurographics Workshop on 3D Object Retrieval; Schreck, T., Theoharis, T., Eds.; The Eurographics Association: Graz, Austria, 2020. [Google Scholar]
- Gower, J.C. Generalized procrustes analysis. Psychometrika 1975, 40, 33–51. [Google Scholar] [CrossRef]
- Solves, C.; Nácher, B.; Benages, L.; Marzo, R.; Soriano, C.; Alemany, S. Research on the Existence and Availability of Anthropometric Data of Children. Internal Report of Deutsches Institut für Normung; 2017; Unpublished. [Google Scholar]
- Steenbekkers, L.P.A. Child Development, Design Implications and Accident Prevention; Delft University Press: Delft, The Netherlands, 1993; ISBN 90-6275-895-9. [Google Scholar]
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150202. [Google Scholar] [CrossRef]
- Huysmans, T.; Goto, L.; Molenbroek, J.F.M.; Goossens, R.H.M. Dined mannequin: An open platform for 3D anthropometry. Tijdschr. Hum. Factors 2020, 45, 4–7. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group 1 (n = 33) | Age Group 2 (n = 28) | Age Group 3 (n = 29) | Age Group 4 (n = 32) | Age Group 5 (n = 67) | Age Group 6 (n = 65) | Age Group 7 (n = 49) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Stature * | 768.7 | 55.8 | 875.3 | 65.1 | 994.9 | 50.6 | 1068.6 | 53.6 | 1116.4 | 51.9 | 1195.9 | 53.3 | 1230.5 | 53.3 |
| Weight * | 9.6 | 1.4 | 12.4 | 1.9 | 15.1 | 1.8 | 18.2 | 2.8 | 19.5 | 2.5 | 22.1 | 2.9 | 23.4 | 2.5 |
| Head circumference * | 460.9 | 17.5 | 484.0 | 12.7 | 497.6 | 18.9 | 509.4 | 16.9 | 509.4 | 13.5 | 511.3 | 15.7 | 513.2 | 14.1 |
| Head width * | 126.8 | 8.2 | 135.0 | 7.5 | 136.3 | 6.3 | 140.2 | 5.4 | 140.5 | 6.8 | 143.5 | 6.5 | 144.4 | 7.4 |
| Head length * | 154.3 | 8.0 | 167.1 | 7.0 | 169.6 | 11.2 | 175.0 | 7.3 | 177.3 | 7.0 | 177.1 | 7.3 | 177.8 | 7.9 |
| Head height * | 160.8 | 9.5 | 173.1 | 10.6 | 178.8 | 14.2 | 186.7 | 10.5 | 189.0 | 9.9 | 192.0 | 10.6 | 194.6 | 8.8 |
| Face width * | 100.9 | 6.0 | 103.2 | 6.9 | 105.4 | 4.6 | 108.6 | 5.3 | 107.9 | 5.5 | 109.7 | 6.3 | 111.4 | 6.8 |
| Face length | 90.6 | 4.8 | 96.5 | 5.3 | 100.2 | 4.4 | 104.3 | 5.7 | 107.0 | 5.5 | 109.7 | 5.6 | 111.2 | 4.8 |
| Sellion-menton length | 76.9 | 4.6 | 81.8 | 3.9 | 86.9 | 3.4 | 91.6 | 4.7 | 93.3 | 4.1 | 96.2 | 4.6 | 96.9 | 4.5 |
| Lower face length | 48.8 | 3.6 | 51.3 | 2.9 | 54.1 | 2.8 | 57.0 | 4.0 | 57.4 | 3.5 | 58.5 | 3.7 | 58.7 | 3.4 |
| Intercanthal width | 29.3 | 2.4 | 30.4 | 2.2 | 31.3 | 2.4 | 31.9 | 2.1 | 32.2 | 2.1 | 32.5 | 2.4 | 32.8 | 2.4 |
| Nasal root breadth | 19.3 | 1.9 | 19.6 | 2.1 | 20.5 | 1.5 | 21.1 | 1.7 | 21.2 | 1.7 | 21.4 | 1.9 | 21.5 | 1.8 |
| Nose length | 28.1 | 1.8 | 30.4 | 2.4 | 32.8 | 2.2 | 34.6 | 2.1 | 35.9 | 2.0 | 37.6 | 2.5 | 38.1 | 2.6 |
| Nose bridge length | 18.9 | 1.8 | 20.6 | 2.2 | 22.4 | 1.7 | 23.6 | 2.2 | 24.3 | 2.0 | 25.7 | 2.2 | 25.9 | 2.8 |
| Nasal tip protrusion | 11.5 | 0.9 | 12.0 | 1.3 | 13.0 | 1.6 | 13.8 | 1.2 | 14.5 | 1.1 | 15.0 | 1.4 | 15.3 | 1.1 |
| Nose width | 25.7 | 1.5 | 26.5 | 1.9 | 27.8 | 2.2 | 27.8 | 1.9 | 28.2 | 1.5 | 28.7 | 1.6 | 29.1 | 1.5 |
| Mouth width | 34.3 | 4.7 | 34.9 | 3.0 | 36.7 | 2.9 | 37.0 | 2.9 | 38.0 | 3.0 | 39.2 | 3.3 | 40.4 | 3.2 |
| Chin height | 18.1 | 2.2 | 20.9 | 2.3 | 23.7 | 2.3 | 24.9 | 3.3 | 24.9 | 2.7 | 25.7 | 2.4 | 26.2 | 2.5 |
| Sellion-sublabiale length | 58.8 | 4.5 | 60.9 | 3.4 | 63.3 | 3.0 | 66.7 | 3.6 | 68.3 | 3.5 | 70.5 | 3.9 | 70.7 | 3.8 |
| Sellion-pogonion length | 67.2 | 4.9 | 69.9 | 3.7 | 73.7 | 4.2 | 76.4 | 3.8 | 78.5 | 3.9 | 80.4 | 4.3 | 80.7 | 4.2 |
| Inter-pupillary distance | 50.4 | 2.8 | 52.5 | 2.5 | 53.4 | 2.7 | 54.9 | 2.8 | 55.3 | 2.3 | 56.0 | 2.9 | 57.1 | 3.0 |
| Measurement | Definition |
|---|---|
| Face length | Straight-line distance between the sellion (s) and menton (me) landmarks |
| Sellion-pogonion length | Straight-line distance between the sellion (s) and pogonion (pg) landmarks |
| Nose bridge length | Straight-line distance between the sellion (s) to pronasale (prn) landmarks |
| Mouth width | Straight-line distance between the left and right chelion landmarks (ch-ch) |
| Nose tip protrusion | Straight-line distance between the the subnasale (sn) and the pronasale (prn) landmarks |
| Nasal root breadth | The horizontal breadth of the nosals root spanning from the left nasal root point to the right (nrp-nrp) |
| Nose breadth | Straight line distance between the left and right alare landmarks (al-al) |
| Inter-pupillary distance | The straight-line distance between the centre of the left and the centre of the right pupil |
| Face width | Horizontal breadth between the left and right zygion landmarks (zy-zy) |
| Age Group 1 | Age Group 2 | Age Group 3 | Age Group 4 | Age Group 5 | Age Group 6 | Age Group 7 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean Diff | p | Mean Diff | p | Mean Diff | p | Mean Diff | p | Mean Diff | p | Mean Diff | p | Mean Diff | p | |
| Stature | 21.00 | 0.33 | −8.17 | 0.76 | −21.56 | 0.27 | 52.85 | 0.01 * | −5.95 | 0.65 | 15.04 | 0.26 | 2.49 | 0.87 |
| Weight | 0.70 | 0.18 | −0.06 | 0.94 | 0.36 | 0.60 | 1.96 | 0.09 | 0.31 | 0.62 | 1.04 | 0.14 | −0.36 | 0.62 |
| Head circumference | 19.90 | 0.00 ** | 2.54 | 0.63 | 12.03 | 0.09 | 3.38 | 0.63 | 7.51 | 0.03 * | 7.00 | 0.07 | 7.42 | 0.06 |
| Head width | 5.65 | 0.10 | 3.50 | 0.29 | 3.43 | 0.15 | 5.08 | 0.02 * | 4.50 | 0.01 ** | 6.88 | 0.11 | 5.18 | 0.01 * |
| Head length | 1.51 | 0.69 | −1.26 | 0.67 | 0.15 | 0.97 | 5.67 | 0.05 | 3.07 | 0.08 | 2.35 | 0.20 | 3.40 | 0.13 |
| Head height | −4.13 | 0.39 | 2.63 | 0.58 | −1.57 | 0.77 | 9.88 | 0.02 * | 7.95 | 0.00 ** | 4.78 | 0.07 | 7.04 | 0.00 ** |
| Face width | 4.24 | 0.09 | 2.38 | 0.44 | 3.32 | 0.05 | 1.75 | 0.43 | 1.90 | 0.17 | −0.37 | 0.82 | −0.42 | 0.83 |
| Face length | 1.32 | 0.45 | 3.51 | 0.10 | 1.21 | 0.47 | 3.52 | 0.13 | 2.82 | 0.02 * | 1.39 | 0.32 | 2.38 | 0.08 |
| Sellion-menton length | 1.74 | 0.30 | 1.96 | 0.21 | 0.70 | 0.59 | 3.02 | 0.12 | 1.94 | 0.06 | 1.52 | 0.19 | 3.35 | 0.01 * |
| Lower face length | 1.02 | 0.43 | 1.36 | 0.24 | 0.50 | 0.64 | 3.03 | 0.06 | 1.83 | 0.03 * | 0.10 | 0.91 | 2.10 | 0.03 * |
| Intercanthal width | 1.89 | 0.02 * | −0.09 | 0.92 | 0.97 | 0.29 | 1.41 | 0.10 | 0.43 | 0.41 | 0.02 | 0.98 | 0.46 | 0.50 |
| Nasal root breadth | 1.70 | 0.01 * | 0.44 | 0.60 | 0.54 | 0.35 | 0.73 | 0.30 | 0.27 | 0.52 | −0.01 | 0.99 | 0.13 | 0.80 |
| Nose length | 0.72 | 0.27 | 0.60 | 0.54 | 0.20 | 0.81 | −0.02 | 0.99 | 0.10 | 0.84 | 1.42 | 0.02 * | 1.25 | 0.10 |
| Nose bridge length | 0.45 | 0.48 | 0.96 | 0.28 | 0.38 | 0.56 | 0.01 | 0.99 | −0.07 | 0.89 | 0.55 | 0.32 | 1.49 | 0.06 |
| Nasal tip protrusion | 0.22 | 0.49 | −0.27 | 0.60 | 0.15 | 0.81 | 0.12 | 0.82 | 0.03 | 0.91 | 0.77 | 0.03 * | −0.05 | 0.87 |
| Nose width | 0.73 | 0.17 | 1.20 | 0.12 | 0.83 | 0.32 | 0.77 | 0.34 | 1.31 | 0.00 ** | 0.78 | 0.06 | 0.59 | 0.18 |
| Mouth width | 3.38 | 0.04 * | 0.45 | 0.72 | 1.00 | 0.36 | 1.72 | 0.15 | 2.59 | 0.00 ** | 0.15 | 0.86 | −0.08 | 0.93 |
| Chin height | −0.69 | 0.39 | 0.01 | 0.99 | −0.67 | 0.44 | 2.12 | 0.12 | 1.21 | 0.07 | 0.09 | 0.88 | 0.21 | 0.77 |
| Sellion-sublabiale length | 2.43 | 0.13 | 1.95 | 0.15 | 1.37 | 0.23 | 0.89 | 0.55 | 0.72 | 0.41 | 1.43 | 0.15 | 3.14 | 0.00 ** |
| Sellion-pogonion length | 2.55 | 0.14 | 1.41 | 0.34 | 1.81 | 0.26 | 2.78 | 0.07 | 0.61 | 0.53 | 2.10 | 0.05 | 2.23 | 0.06 |
| Inter-pupillary distance | 2.32 | 0.02 * | 0.65 | 0.52 | 0.56 | 0.58 | 1.93 | 0.09 | 0.69 | 0.23 | −0.01 | 0.99 | 0.69 | 0.43 |
| Component Matrix | |||||
|---|---|---|---|---|---|
| Face Dimensions | PC1 | PC2 | PC3 | PC4 | PC5 |
| Face width | 0.62 | 0.31 | 0.28 | 0.62 | 0.17 |
| Face Length | 0.91 | −0.32 | −0.01 | 0.06 | −0.01 |
| Sellion-pogonion length | 0.85 | −0.39 | 0.07 | 0.07 | −0.09 |
| Inter-pupillary distance | 0.82 | 0.30 | −0.31 | −0.07 | −0.15 |
| Nasal root width | 0.64 | 0.47 | −0.56 | −0.05 | −0.04 |
| Nasal bridge length | 0.77 | −0.46 | −0.07 | −0.08 | −0.12 |
| Nasal tip protrusion | 0.75 | −0.19 | −0.13 | −0.27 | 0.48 |
| Nose width | 0.73 | 0.17 | 0.36 | −0.28 | −0.36 |
| Width of mouth | 0.65 | 0.41 | 0.42 | −0.28 | 0.18 |
| Variance explained (%) | 56.94 | 12.22 | 9.00 | 7.07 | 5.16 |
| Cumulative variance explained (%) | 56.94 | 69.16 | 78.16 | 85.23 | 90.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goto, L.; Lee, W.; Huysmans, T.; Molenbroek, J.F.M.; Goossens, R.H.M. The Variation in 3D Face Shapes of Dutch Children for Mask Design. Appl. Sci. 2021, 11, 6843. https://doi.org/10.3390/app11156843
Goto L, Lee W, Huysmans T, Molenbroek JFM, Goossens RHM. The Variation in 3D Face Shapes of Dutch Children for Mask Design. Applied Sciences. 2021; 11(15):6843. https://doi.org/10.3390/app11156843
Chicago/Turabian StyleGoto, Lyè, Wonsup Lee, Toon Huysmans, Johan F. M. Molenbroek, and Richard H. M. Goossens. 2021. "The Variation in 3D Face Shapes of Dutch Children for Mask Design" Applied Sciences 11, no. 15: 6843. https://doi.org/10.3390/app11156843
APA StyleGoto, L., Lee, W., Huysmans, T., Molenbroek, J. F. M., & Goossens, R. H. M. (2021). The Variation in 3D Face Shapes of Dutch Children for Mask Design. Applied Sciences, 11(15), 6843. https://doi.org/10.3390/app11156843