


The Impact of Exposure to Hexavalent Chromium on the Incidence and Mortality of Oral and Gastrointestinal Cancers and Benign Diseases: A Systematic Review of Observational Studies, Reviews and Meta-Analyses

 ,
,  ,
, 
Abstract
1. Introduction
1.1. Rationale
1.2. Objectives
2. Materials and Methods
2.1. Registration
2.2. Eligibility Criteria
2.3. Information Sources and Search Strategy
- Exposure assessment: leather tanning, stainless steel, cement, welding, metal/chrome plating, chrome pigment, chromate production, electroplating, ferrochrome, abrasive blasting, battery/candle/dye/rubber maker, printers, brazing, soldering, Cr(VI), chromium, heavy metal, toxic metal
- Outcome assessment: stomach–gastric/anal/bile duct/colon/esophageal/gallbladder/liver/pancreatic/rectal/small intestine/gastric cancer (or tumor), gastritis, gastroesophageal reflux disease, ulcer, irritable bowel syndrome, hemorrhoids, Crohn, ulcerative colitis, constipation, gastrointestinal bleeding, diverticulitis, celiac disease, gallstones, cholelithiasis, cirrhosis.
2.4. Study Selection
2.5. Data Extraction
2.6. Study Risk-of-Bias Assessment
2.7. Data Synthesis
3. Results
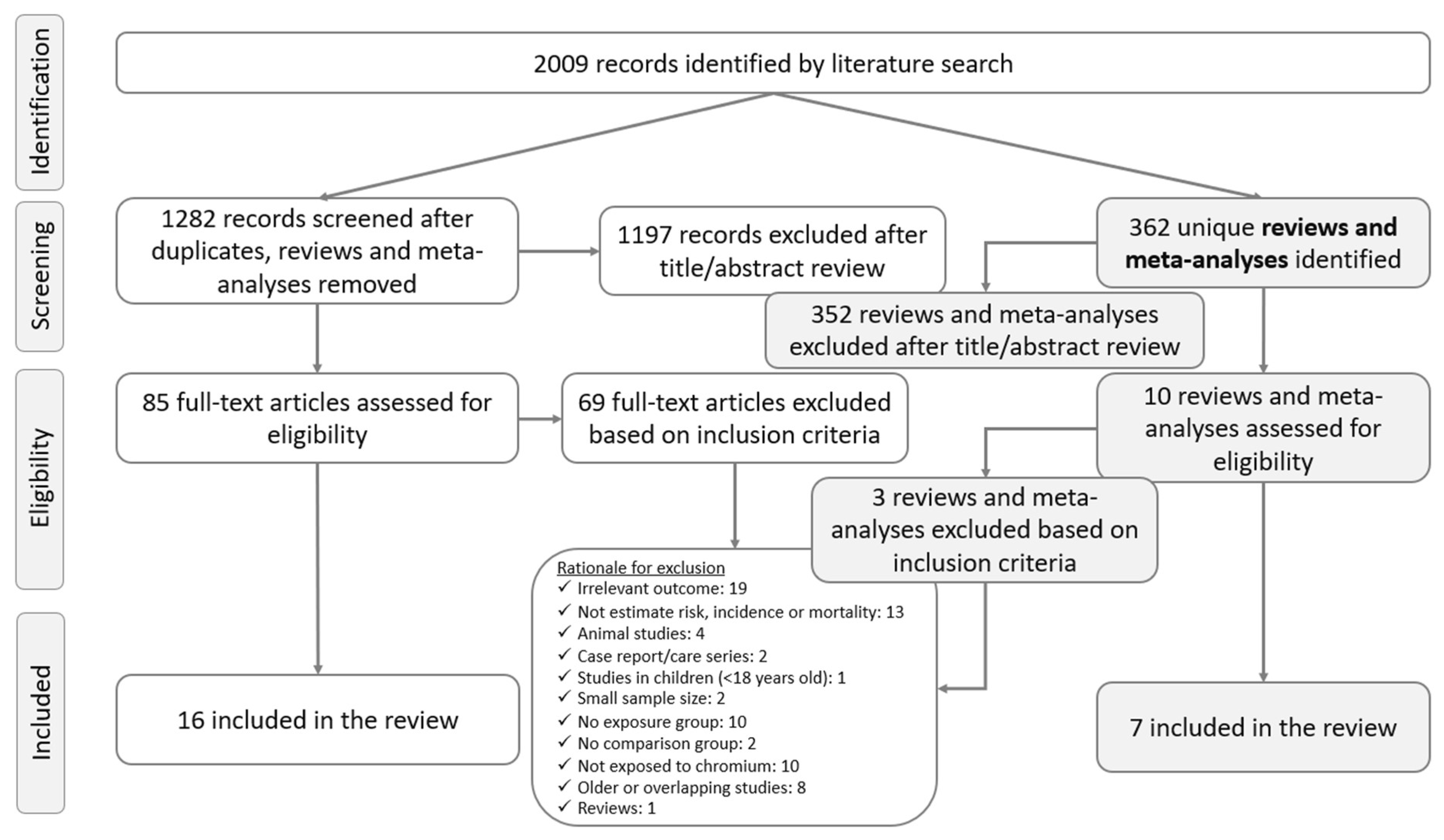
3.1. Study Selection Process
3.2. Study Risk-of-Bias (RoB) Assessment Results
3.3. Gastrointestinal Cancers
3.3.1. Oral Cancer
3.3.2. Esophageal Cancer
3.3.3. Gastric Cancer
3.3.4. Small Intestinal Cancer
3.3.5. Colorectal Cancer
3.3.6. Hepatocellular Cancer
3.3.7. Pancreatic Cancer
3.3.8. Cancer of Gallbladder and Extrahepatic Bile Ducts
3.4. Benign Gastrointestinal Diseases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| ATSDR | Agency for Toxic Substances and Disease Registry |
| NIOSH | National Institute for Occupational Safety and Health |
| RoB | Risk-of-bias |
| Cr(VI) | Hexavalent chromium |
| RR | Relative risk |
| SMR | Standardized mortality ratio |
| SIR | Standardized incidence ratio |
| OR | Odds ratio |
| HR | Hazard ratio |
| ASR | Age-standardized incidence rate |
References
- NIH. Hexavalent Chromium. 2023. Available online: https://www.niehs.nih.gov/health/topics/agents/hex-chromium/index.cfm (accessed on 3 February 2023).
- NIOSH. Criteria for a Recommended Standard: Occupational Exposure to Hexavalent Chromium; Centers for Disease Control and Prevention: Washington, DC, USA, 2013.
- OSHA. Chromium—Overview. 2013. Available online: https://www.osha.gov/chromium (accessed on 6 February 2023).
- PubChem Chromium(6+). 2004. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/29131 (accessed on 6 February 2023).
- ATSDR. Chromium (Cr) Toxicity: What Are the Physiologic Effects of Chromium Exposure? 2013. Available online: https://www.atsdr.cdc.gov/csem/chromium/physiologic_effects_of_chromium_exposure.html#:~:text=When%20inhaled%2C%20chromium%20compounds%20are%20respiratory%20tract%20irritants%20and%20can,with%20Cr(VI)%20compounds (accessed on 26 March 2023).
- EFSA. Scientific Opinion on the Risks to Public Health Related to the Presence of Chromium in Food and Drinking Water. 2014. Available online: https://www.efsa.europa.eu/en/efsajournal/pub/3595 (accessed on 26 March 2023).
- IARC. Arsenic, Metals, Fibres, and Dusts. IARC Monogr. Eval. Carcinog. Risks Hum. 2012, 100, 11–465. [Google Scholar]
- den Braver-Sewradj, S.P.; van Benthem, J.; Staal, Y.C.M.; Ezendam, J.; Piersma, A.H.; Hessel, E.V.S. Occupational Exposure to Hexavalent Chromium. Part II. Hazard Assessment of Carcinogenic Effects. Regul. Toxicol. Pharmacol. 2021, 126, 105045. [Google Scholar] [CrossRef] [PubMed]
- ATSDR Toxicological Profile for Chromium. Available online: https://wwwn.cdc.gov/TSP/ToxProfiles/ToxProfiles.aspx?id=62&tid=17 (accessed on 20 December 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- DeBono, N.L.; Logar-Henderson, C.; Warden, H.; Shakik, S.; Dakouo, M.; MacLeod, J.; Demers, P.A. Cancer Surveillance among Workers in Plastics and Rubber Manufacturing in Ontario, Canada. Occup. Environ. Med. 2020, 77, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Salerno, C.; Cucciniello, A.C. Former Workers of a Bright Electroplating Factory Located in Vercelli: A Cohort Study From 1974 to 2016: Legal Expertise Results. J. Occup. Environ. Med. 2019, 61, e374–e377. [Google Scholar] [CrossRef] [PubMed]
- Sciannameo, V.; Ricceri, F.; Soldati, S.; Scarnato, C.; Gerosa, A.; Giacomozzi, G.; d’Errico, A. Cancer Mortality and Exposure to Nickel and Chromium Compounds in a Cohort of Italian Electroplaters. Am. J. Ind. Med. 2019, 62, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Gibb, H.J.; Lees, P.S.J.; Wang, J.; Grace O’Leary, K. Extended Followup of a Cohort of Chromium Production Workers. Am. J. Ind. Med. 2015, 58, 905–913. [Google Scholar] [CrossRef]
- Girardi, P.; Bressan, V.; Mabilia, T.; Merler, E. Confirmation of an excess of cancer mortality in a cohort of workers of a chromium thin-layer plating. Epidemiol. Prev. 2015, 39, 183–187. [Google Scholar]
- Gerosa, A.; Scarnato, C.; Giacomozzi, G.; d’Errico, A. Mortality study in metal electroplating workers in Bologna (Northern Italy). Epidemiol. Prev. 2013, 37, 376–385. [Google Scholar]
- Wu, W.-T.; Lu, Y.-H.; Lin, Y.-J.; Yang, Y.-H.; Shiue, H.-S.; Hsu, J.-H.; Li, C.-Y.; Yang, C.-Y.; Liou, S.-H.; Wu, T.-N. Mortality among Shipbreaking Workers in Taiwan--a Retrospective Cohort Study from 1985 to 2008. Am. J. Ind. Med. 2013, 56, 701–708. [Google Scholar] [CrossRef]
- Koh, D.-H.; Kim, T.-W.; Jang, S.; Ryu, H.-W. Dust Exposure and the Risk of Cancer in Cement Industry Workers in Korea. Am. J. Ind. Med. 2013, 56, 276–281. [Google Scholar] [CrossRef]
- Ilychova, S.A.; Zaridze, D.G. Cancer Mortality among Female and Male Workers Occupationally Exposed to Inorganic Lead in the Printing Industry. Occup. Environ. Med. 2012, 69, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Kendzia, B.; Kaerlev, L.; Ahrens, W.; Merletti, F.; Eriksson, M.; Guénel, P.; Lynge, E.; Costa-Pereira, A.; Morales Suárez-Varela, M.; Jöckel, K.-H.; et al. Lifetime Exposure to Welding Fumes and Risk of Some Rare Cancers. Am. J. Epidemiol. 2022, 191, 1753–1765. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.C.; Boffetta, P.; Johnson, K.C.; Hu, J.; Palli, D.; Ferraroni, M.; Tsugane, S.; Hamada, G.S.; Hidaka, A.; Zaridze, D.; et al. Occupational Exposures and Odds of Gastric Cancer: A StoP Project Consortium Pooled Analysis. Int. J. Epidemiol. 2020, 49, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, R.; Sato, Y.; Kobayashi, Y. Manufacturing Industry Cancer Risk in Japan: A Multicenter Hospital-Based Case Control Study. Asian Pac. J. Cancer Prev. 2020, 21, 2697–2707. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, H.; Xiang, X.; Liu, F. Outline of Occupational Chromium Poisoning in China. Bull. Environ. Contam. Toxicol. 2013, 90, 742–749. [Google Scholar] [CrossRef]
- Núñez, O.; Fernández-Navarro, P.; Martín-Méndez, I.; Bel-Lan, A.; Locutura, J.F.; López-Abente, G. Arsenic and Chromium Topsoil Levels and Cancer Mortality in Spain. Environ. Sci. Pollut. Res. 2016, 23, 17664–17675. [Google Scholar] [CrossRef]
- Chen, K.; Liao, Q.L.; Ma, Z.W.; Jin, Y.; Hua, M.; Bi, J.; Huang, L. Association of Soil Arsenic and Nickel Exposure with Cancer Mortality Rates, a Town-Scale Ecological Study in Suzhou, China. Environ. Sci. Pollut. Res. Int. 2015, 22, 5395–5404. [Google Scholar] [CrossRef]
- García-Pérez, J.; López-Abente, G.; Castelló, A.; González-Sánchez, M.; Fernández-Navarro, P. Cancer Mortality in Towns in the Vicinity of Installations for the Production of Cement, Lime, Plaster, and Magnesium Oxide. Chemosphere 2015, 128, 103–110. [Google Scholar] [CrossRef]
- NTP OHAT. OHAT Risk of Bias Rating Tool for Human and Animal Studies. 2019. Available online: https://ntp.niehs.nih.gov/whatwestudy/assessments/noncancer/riskbias/index.html (accessed on 18 March 2023).
- Hessel, E.V.S.; Staal, Y.C.M.; Piersma, A.H.; den Braver-Sewradj, S.P.; Ezendam, J. Occupational Exposure to Hexavalent Chromium. Part I. Hazard Assessment of Non-Cancer Health Effects. Regul. Toxicol. Pharmacol. 2021, 126, 105048. [Google Scholar] [CrossRef]
- Suh, M.; Wikoff, D.; Lipworth, L.; Goodman, M.; Fitch, S.; Mittal, L.; Ring, C.; Proctor, D. Hexavalent Chromium and Stomach Cancer: A Systematic Review and Meta-Analysis. Crit. Rev. Toxicol. 2019, 49, 140–159. [Google Scholar] [CrossRef]
- Deng, Y.; Wang, M.; Tian, T.; Lin, S.; Xu, P.; Zhou, L.; Dai, C.; Hao, Q.; Wu, Y.; Zhai, Z.; et al. The Effect of Hexavalent Chromium on the Incidence and Mortality of Human Cancers: A Meta-Analysis Based on Published Epidemiological Cohort Studies. Front. Oncol. 2019, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- Donato, F.; Garzaro, G.; Pira, E.; Boffetta, P. Mortality and Cancer Morbidity among Cement Production Workers: A Meta-Analysis. Int. Arch. Occup. Environ. Health 2016, 89, 1155–1168. [Google Scholar] [CrossRef] [PubMed]
- Welling, R.; Beaumont, J.J.; Petersen, S.J.; Alexeeff, G.V.; Steinmaus, C. Chromium VI and Stomach Cancer: A Meta-Analysis of the Current Epidemiological Evidence. Occup. Environ. Med. 2015, 72, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.S.; Sadoff, M.M.; Jiang, X.; Fryzek, J.P.; Garabrant, D.H. A Review and Meta-Analysis of Cancer Risks in Relation to Portland Cement Exposure. Occup. Environ. Med. 2014, 71, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Lucas, J.; Kramkowski, R. Health Hazard Evaluation Determination Report Number 74-87-221; Center for Disease Control: Cincinnati, OH, USA, 1975.
- Mancuso, R.F. Occupational Cancer and Other Health Hazards in a Chromate Plant: A Medical Appraisal. II. Clinical and Toxicologic Aspects. Ind. Med. Surg. 1951, 20, 393–407. [Google Scholar] [PubMed]
- Sassi, C. Occupational Disease in a Chromate Factory. Med. Lav. 1956, 47, 314–327. [Google Scholar]
- Sterekhova, N.P.; Zeleneva, N.I.; Solomina, S.N.; Tiushniakova, N.V.; Miasnikova, A.G. Stomach pathology in workers in chromium salt manufacture. Gig. Tr. Prof. Zabol. 1978, 3, 19–23. [Google Scholar]
- Moulin, J.J.; Wild, P.; Mantout, B.; Fournier-Betz, M.; Mur, J.M.; Smagghe, G. Mortality from Lung Cancer and Cardiovascular Diseases among Stainless-Steel Producing Workers. Cancer Causes Control 1993, 4, 75–81. [Google Scholar] [CrossRef]
- Georgopoulos, S.D.; Michopoulos, S.; Rokkas, T.; Apostolopoulos, P.; Giamarellos, E.; Kamberoglou, D.; Mentis, A.; Triantafyllou, K. Hellenic Consensus on Helicobacter Pylori Infection. Ann. Gastroenterol. 2020, 33, 105–124. [Google Scholar] [CrossRef]
- Hundahl, S.A.; Phillips, J.L.; Menck, H.R. The National Cancer Data Base Report on Poor Survival of U.S. Gastric Carcinoma Patients Treated with Gastrectomy: Fifth Edition American Joint Committee on Cancer Staging, Proximal Disease, and the “Different Disease” Hypothesis. Cancer 2000, 88, 921–932. [Google Scholar] [CrossRef]
- Yuan, W.; Yang, N.; Li, X. Advances in Understanding How Heavy Metal Pollution Triggers Gastric Cancer. Biomed. Res. Int. 2016, 2016, 7825432. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, R.; Renu, K.; Eladl, M.A.; El-Sherbiny, M.; Elsherbini, D.M.A.; Mirza, A.K.; Vellingiri, B.; Iyer, M.; Dey, A.; Valsala Gopalakrishnan, A. Mechanism of Chromium-Induced Toxicity in Lungs, Liver, and Kidney and Their Ameliorative Agents. Biomed. Pharmacother. 2022, 151, 113119. [Google Scholar] [CrossRef] [PubMed]
- Linos, A.; Petralias, A.; Christophi, C.A.; Christoforidou, E.; Kouroutou, P.; Stoltidis, M.; Veloudaki, A.; Tzala, E.; Makris, K.C.; Karagas, M.R. Oral Ingestion of Hexavalent Chromium through Drinking Water and Cancer Mortality in an Industrial Area of Greece—An Ecological Study. Environ. Health 2011, 10, 50. [Google Scholar] [CrossRef] [PubMed]
- Bednar, C.M.; Kies, C. Inorganic Contaminants in Drinking Water Correlated with Disease Occurrence in Nebraska. JAWRA J. Am. Water Resour. Assoc. 1991, 27, 631–635. [Google Scholar] [CrossRef]
- Dhimal, M.; Chirico, F.; Bista, B.; Sharma, S.; Chalise, B.; Dhimal, M.L.; Ilesanmi, O.S.; Trucillo, P.; Sofia, D. Impact of Air Pollution on Global Burden of Disease in 2019. Processes 2021, 9, 1719. [Google Scholar] [CrossRef]
- Bugeja, R.; Shoemake, C. Heavy Metal Concentrations in Maltese Potable Water. Environments 2015, 2, 186–199. [Google Scholar] [CrossRef]
- Ghosh, B.; Padhy, P.K.; Niyogi, S.; Patra, P.K.; Hecker, M. A Comparative Study of Heavy Metal Pollution in Ambient Air and the Health Risks Assessment in Industrial, Urban and Semi-Urban Areas of West Bengal, India: An Evaluation of Carcinogenic, Non-Carcinogenic, and Additional Lifetime Cancer Cases. Environments 2023, 10, 190. [Google Scholar] [CrossRef]


{kind=link}
| Author | Study Design | Study Population | Number of Study Participants | Exposure/ Target Group | Comparison Group | Outcome | Measure | Key Findings | Tier |
|---|---|---|---|---|---|---|---|---|---|
| DeBono et al., 2020 [11] | Retrospective cohort | Canada | 2.18 million workers; 81,127 workers in the exposure group | Plastics and rubber manufacturing | Rest of the workers | Incidence | HR | ↑ HR for esophageal and gastric Ca in job-specific subgroups | 2 |
| Salerno and Cucciniello, 2019 [12] | Retrospective cohort | Italy | 899 workers | Electroplating factory workers | Regional population | Mortality | SMR | ↑ SMR for digestive tract and hepatocellular Ca | 2 |
| Sciannameo et al., 2019 [13] | Retrospective cohort | Italy | 2991 workers | Electroplating factory workers | Non-exposed workers | Mortality | HR | NS different risk for GI Ca with exposure to Cr | 1 |
| Gibb et al., 2015 [14] | Prospective cohort | USA | 2354 workers | Chromate production | National data | Mortality | SMR | NS in SMR for all GI Ca | 2 |
| Girardi et al., 2015 [15] | Retrospective cohort | Italy | 127 workers | Chromium thin-layer plating | Northern Italy population | Mortality | SMR | ↑ SMR for pancreatic Ca | 2 |
| Gerosa et al., 2013 [16] | Retrospective cohort | Italy | 2983 workers | Electroplating workers | Northern Italy population | Mortality | SMR | ↑ SMR for rectal Ca | 2 |
| Wu et al., 2013 [17] | Retrospective cohort | Taiwan | 4962 workers | Shipbreaking Workers | National data | Mortality | SMR | (1) ↑ SMR for oral, nasopharyngeal and hepatocellular Ca and cirrhosis in male workers (2) NS in SMR for all female workers | 2 |
| Koh et al., 2013 [18] | Retrospective cohort | Korea | 1324 male workers | Cement industry workers | National data | Incidence | SIR | (1) ↑ SIR for rectal Ca in all workers (2) ↑ SIR for gastric Ca in high dust exposure group | 2 |
| Ilychova and Zaridze, 2012 [19] | Retrospective cohort | Moscow, Russia | 4525 workers | Printing industry workers | Moscow population | Mortality | SMR | NS in SMR for all GI Ca | 2 |
| Kendzia et al., 2022 [20] | Case–control | 7 European countries + | 644 male cases; 1959 male controls | Workers exposed to welding fumes | Non-exposed | Incidence | OR | Regular welding and lifetime exposure was associated with an increased risk of small intestinal Ca | 1 |
| Shah et al., 2020 [21] | Pooled case–control | 8 countries ++ | 5279 GI Ca cases; 12,297 controls | Occupational exposure to Cr | Non-exposed | Incidence | OR | ↑ Odds for gastric Ca in workers exposed to Cr | 1 |
| Kaneko et al., 2020 [22] | Case–control | Japan | 40,370 Ca cases; 26,746 controls | Various manufacturing industry categories | Non-exposed | Incidence | OR | (1) ↑ Odds for colon Ca in printing industry workers (2) ↑ Odds for pancreatic and hepatocellular Ca in leather tanning, leather products and fur workers | 1 |
| Yang et al., 2013 [23] | Pooled case–control | China | 6998 workers | Occupational exposure to Cr | Non-exposed | Incidence; Mortality | SMR, OR | (1) ↑ Odds for hepatocellular Ca in male workers exposed to Cr (2) NS in SMR for hepatocellular Ca | 2 |
| Núñez et al., 2016 [24] | Ecological study | Spain | (1) Ca Mortality data from the National Statistics Institute (2) 21,187 topsoil samples | Topsoil levels of chromium | - | Mortality | RR | Higher topsoil concentration to Cr ~ upper GI tract Ca in females | 3 |
| Chen et al., 2015 [25] | Ecological study | China | (1) Records of all residents’ deaths in Suzhou (2) 1683 topsoil samples | Topsoil levels of chromium | - | Mortality | RR | NS between Cr exposure with colon, gastric and hepatocellular Ca mortality rates | 3 |
| García-Pérez et al., 2015 [26] | Ecological study | Spain | Ca Mortality data from the National Statistics Institute | Production of cement, lime, plaster | Distance from industrial facility | Mortality | RR | (1) ↑ risk for colorectal Ca (2) ↑ risk for gastric Ca, only in men (3) NS risk for the rest GI Ca | 3 |
| Author | Study Design | Period Covered | Human Studies | Outcome | Key Findings |
|---|---|---|---|---|---|
| den Braver-Sewradj et al., 2021 [8] | Systematic review | 2012–2018 | NA * | I&M | Cr(VI) is suspected to cause gastric Ca—limited evidence from human studies. No convincing evidence that Cr(VI) can cause colorectal, esophageal and hepatocellular Ca. Insufficient evidence that Cr(VI) may cause small intestinal, oral cavity and pancreatic Ca. |
| Hessel et al., 2021 [28] | Systematic review | 2012–2018 | NA * | I&M | No convincing evidence that Cr(VI) may have GI effects in humans. |
| Suh et al., 2019 [29] | Meta-analysis | 1980–2018 | 44 | I&M | MRR = 1.08 (95%CI [0.96, 1.21]) for gastric Ca. |
| Deng et al., 2019 [30] | Meta-analysis | 1985–2016 | 47 | I&M | MSIR = 1.30 (95%CI [1.11, 1.54]) for oral Ca (n = 16); MSIR = 1.20 (95%CI [1.08, 1.32]) for gastric Ca (n = 14); MSIR = 1.05 (95%CI [1.00, 1.11]) for digestive system Ca (esophageal, gastric, pancreatic, colon, rectum, hepatobiliary system Ca; n = 51); NS MSIR for each Ca separately; MSMR = 0.97 (95%CI [0.92, 1.01]) for oral and digestive system Ca (esophageal, gastric, pancreatic, colon, rectum, hepatobiliary system and intestinal Ca; n = 99); NS MSMR for each Ca separately |
| Donato et al., 2016 [31] | Meta-analysis | 1984–2016 | 9 | I&M | MRR = 0.93 (95%CI [0.70, 1.17]) for gastric Ca; MSMR = 0.95 (95%CI [0.65, 1.26]) for gastric Ca (n = 7); MSIR = 0.85 (95%CI [0.59, 1.11]) for gastric Ca (n = 4) |
| Welling et al., 2015 [32] | Meta-analysis | 1980–2018 | 56 | I&M | MRR = 1.27 (95%CI [1.20, 1.35]) for gastric Ca; MSMR = 1.39 (95%CI [1.28, 1.51]) for gastric Ca (n = 44); MSIR = 1.17 (95%CI [1.09, 1.27]) for gastric Ca (n = 30) |
| Cohen et al., 2014 [33] | Meta-analysis | 1980–2013 | 26 | I&M | MSMR = 1.07 (95%CI [0.72, 1.59]) for gastric Ca (n = 5); MSIR = 1.05 (95%CI [0.66, 1.68]) for gastric Ca (n = 4); MSMR = 1.05 (95%CI [0.79, 1.40]) for colorectal Ca (n = 4); MSIR = 1.38 (95%CI [1.02, 1.88]) for colorectal Ca (n = 3) |
| Author | Outcome | Oral Ca | Esophageal Ca | Gastric Ca | Small Intestinal Ca | Colon Ca | Rectal Ca | Hepatocellular Ca | Pancreatic Ca | Gallbladder and Extrahepatic Bile Duct Ca | Benign GI Diseases |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cohort, case–control and cross-sectional studies | |||||||||||
| DeBono et al., 2020 [11] | I | X * | X * | X | X | ||||||
| Salerno and Cucciniello, 2019 [12] | M | X | X | X | X | X | X * | X | |||
| Sciannameo et al., 2019 [13] | M | X | X | X | X | X | X | X | |||
| Gibb et al., 2015 [14] | M | X | X | X | X | X | X | X | X | X | |
| Girardi et al., 2015 [15] | M | X | X | X | X | X | X | X * | X | ||
| Gerosa et al., 2013 [16] | M | X | X | X | X | X * | X | X | X | ||
| Wu et al., 2013 [17] | M | X + | X | X | X + | X | X + | ||||
| Koh et al., 2013 [18] | I | X | X | X + | X | X + | X | X | |||
| Ilychova and Zaridze, 2012 [19] | M | X | X | X | X | X | X | X | |||
| Kendzia et al., 2022 [20] | I | X * | X | ||||||||
| Shah et al., 2020 [21] | I | X * | |||||||||
| Kaneko et al., 2020 [22] | I | X | X | X * | X * | X * | |||||
| Yang et al., 2013 [23] | Both | X + | |||||||||
| Núñez et al., 2016 [24] | M | X | X ++ | X ++ | X | X | X | X | |||
| Chen et al., 2015 [25] | M | X | X | X | X | X | |||||
| García-Pérez et al., 2015 [26] | M | X | X | X + | X | X * | X * | X | X | X | |
| Reviews and meta-analyses | |||||||||||
| den Braver-Sewradj et al., 2021 [8] | Both | X | X | X | X | X | X | X | X | ||
| Hessel et al., 2021 [28] | Both | X | |||||||||
| Suh et al., 2019 [29] | Both | X | |||||||||
| Deng et al., 2019 [30] | Both | X * | X | X * | X | X | X | X | X | X | |
| Donato et al., 2016 [31] | Both | X | |||||||||
| Welling et al., 2015 [32] | Both | X * | |||||||||
| Cohen et al., 2014 [33] | Both | X | X * | X * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsas, K.; Diamantis, D.V.; Linos, A.; Psaltopoulou, T.; Triantafyllou, K. The Impact of Exposure to Hexavalent Chromium on the Incidence and Mortality of Oral and Gastrointestinal Cancers and Benign Diseases: A Systematic Review of Observational Studies, Reviews and Meta-Analyses. Environments 2024, 11, 11. https://doi.org/10.3390/environments11010011
Katsas K, Diamantis DV, Linos A, Psaltopoulou T, Triantafyllou K. The Impact of Exposure to Hexavalent Chromium on the Incidence and Mortality of Oral and Gastrointestinal Cancers and Benign Diseases: A Systematic Review of Observational Studies, Reviews and Meta-Analyses. Environments. 2024; 11(1):11. https://doi.org/10.3390/environments11010011
Chicago/Turabian StyleKatsas, Konstantinos, Dimitrios V. Diamantis, Athena Linos, Theodora Psaltopoulou, and Konstantinos Triantafyllou. 2024. "The Impact of Exposure to Hexavalent Chromium on the Incidence and Mortality of Oral and Gastrointestinal Cancers and Benign Diseases: A Systematic Review of Observational Studies, Reviews and Meta-Analyses" Environments 11, no. 1: 11. https://doi.org/10.3390/environments11010011
APA StyleKatsas, K., Diamantis, D. V., Linos, A., Psaltopoulou, T., & Triantafyllou, K. (2024). The Impact of Exposure to Hexavalent Chromium on the Incidence and Mortality of Oral and Gastrointestinal Cancers and Benign Diseases: A Systematic Review of Observational Studies, Reviews and Meta-Analyses. Environments, 11(1), 11. https://doi.org/10.3390/environments11010011