
Talking about Health: A Topic Analysis of Narratives from Individuals with Schizophrenia and Other Serious Mental Illnesses

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.2.1. Procedures
2.2.2. Natural Language Processing
2.3. Topic Analysis
2.4. Data Analysis
3. Results
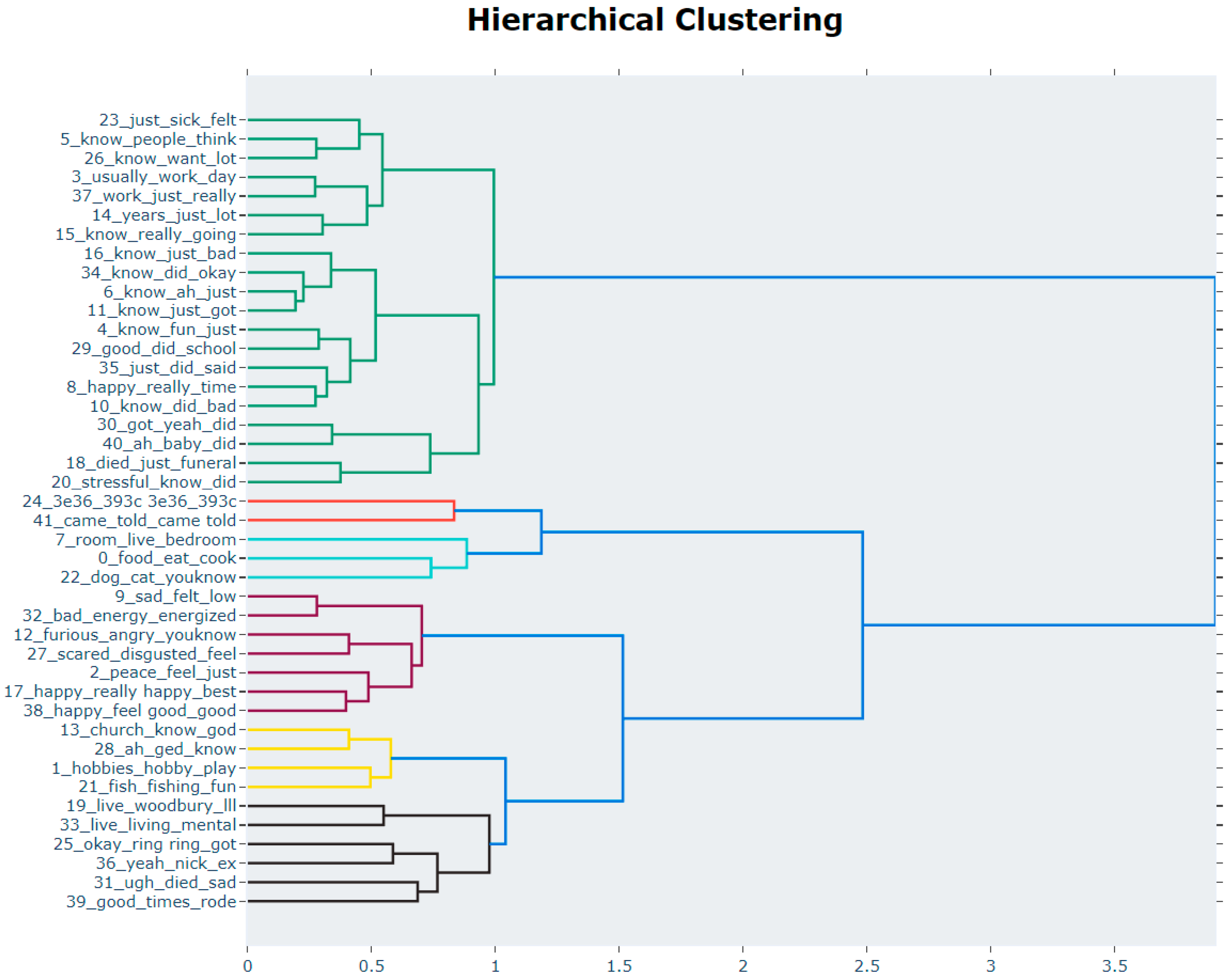
3.1. What General Topics Emerged?
3.2. What Health Related Topics Emerge and How Are They Emotionally Valenced?
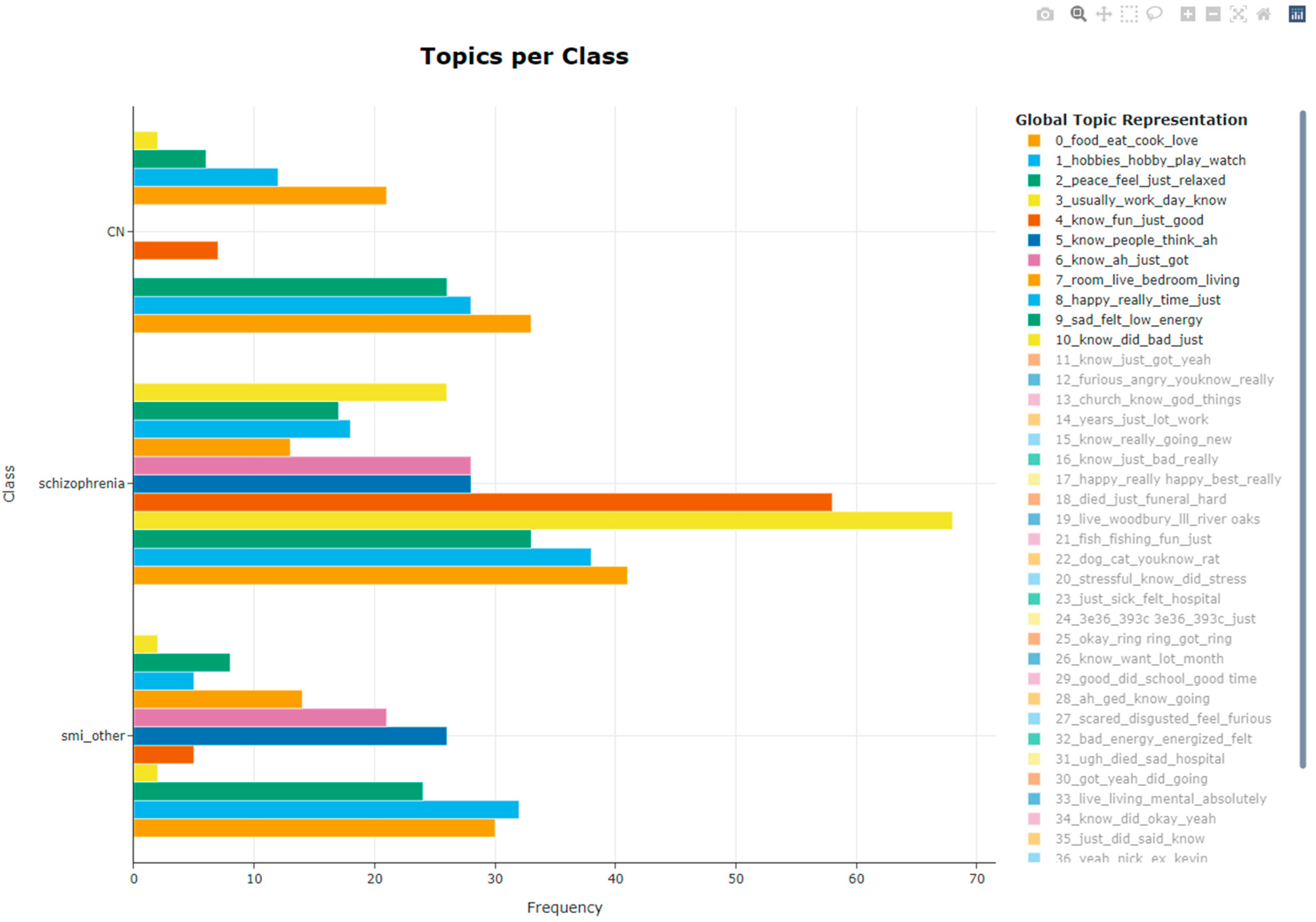
3.3. Is Frequency of Health-Related Topics Related to Patient Group?
4. Discussion
Implications for Health Promotion
5. Limitations and Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Hert, M.; Correll, C.U.; Bobes, J.; Cetkovich-Bakmas, M.; Cohen, D.; Asai, I.; Detraux, J.; Gautam, S.; Möller, H.-J.; Ndetei, D.M.; et al. Physical Illness in Patients with Severe Mental Disorders. I. Prevalence, Impact of Medications and Disparities in Health Care. World Psychiatry 2011, 10, 52–77. [Google Scholar] [CrossRef] [PubMed]
- Hjorthøj, C.; Stürup, A.E.; McGrath, J.J.; Nordentoft, M. Years of Potential Life Lost and Life Expectancy in Schizophrenia: A Systematic Review and Meta-Analysis. Lancet Psychiatry 2017, 4, 295–301. [Google Scholar] [CrossRef]
- Brown, S.; Inskip, H.; Barraclough, B. Causes of the Excess Mortality of Schizophrenia. Br. J. Psychiatry 2000, 177, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Chant, D.; Welham, J.; McGrath, J. A Systematic Review of the Prevalence of Schizophrenia. PLoS Med. 2005, 2, e141. [Google Scholar] [CrossRef]
- Westman, J.; Eriksson, S.V.; Gissler, M.; Hällgren, J.; Prieto, M.L.; Bobo, W.V.; Frye, M.A.; Erlinge, D.; Alfredsson, L.; Ösby, U. Increased Cardiovascular Mortality in People with Schizophrenia: A 24-Year National Register Study. Epidemiol. Psychiatr. Sci. 2018, 27, 519–527. [Google Scholar] [CrossRef]
- Goff, D.C.; Sullivan, L.M.; McEvoy, J.P.; Meyer, J.M.; Nasrallah, H.A.; Daumit, G.L.; Lamberti, S.; D’Agostino, R.B.; Stroup, T.S.; Davis, S.; et al. A Comparison of Ten-Year Cardiac Risk Estimates in Schizophrenia Patients from the CATIE Study and Matched Controls. Schizophr. Res. 2005, 80, 45–53. [Google Scholar] [CrossRef]
- Von Hausswolff-Juhlin, Y.; Bjartveit, M.; Lindström, E.; Jones, P. Schizophrenia and Physical Health Problems. Acta Psychiatr. Scand. 2009, 119, 15–21. [Google Scholar] [CrossRef]
- Connolly, M.; Kelly, C. Lifestyle and Physical Health in Schizophrenia. Adv. Psychiatr. Treat 2005, 11, 125–132. [Google Scholar] [CrossRef]
- McCreadie, R.G.; Group, S.S.L. Diet, Smoking and Cardiovascular Risk in People with Schizophrenia: Descriptive Study. Br. J. Psychiatry 2003, 183, 534–539. [Google Scholar] [CrossRef]
- Scott, D.; Happell, B.; Strange, S.; Platania-Phung, C. Investigating Self-Reported Health Behaviors in Australian Adults with Mental Illness. Behav. Med. 2013, 39, 60–65. [Google Scholar] [CrossRef]
- Dickerson, F.B.; Brown, C.H.; Daumit, G.L.; LiJuan, F.; Goldberg, R.W.; Wohlheiter, K.; Dixon, L.B. Health Status of Individuals With Serious Mental Illness. Schizophr. Bull. 2006, 32, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Holmberg, S.K.; Kane, C. Health and Self-Care Practices of Persons with Schizophrenia. Psychiatr. Serv. 1999, 50, 827–829. [Google Scholar] [CrossRef] [PubMed]
- Parletta, N.; Aljeesh, Y.; Baune, B.T. Health Behaviors, Knowledge, Life Satisfaction, and Wellbeing in People with Mental Illness across Four Countries and Comparisons with Normative Sample. Front. Psychiatry 2016, 7, 145. [Google Scholar] [CrossRef] [PubMed]
- Janney, C.A.; Ganguli, R.; Tang, G.; Cauley, J.A.; Holleman, R.G.; Richardson, C.R.; Kriska, A.M. Physical Activity and Sedentary Behavior Measured Objectively and Subjectively in Overweight and Obese Adults With Schizophrenia or Schizoaffective Disorders. J. Clin. Psychiatry 2015, 76, 14469. [Google Scholar] [CrossRef]
- Hayes, J.F.; Marston, L.; Walters, K.; King, M.B.; Osborn, D.P.J. Mortality Gap for People with Bipolar Disorder and Schizophrenia: UK-Based Cohort Study 2000–2014. Br. J. Psychiatry 2017, 211, 175–181. [Google Scholar] [CrossRef]
- Tanskanen, A.; Tiihonen, J.; Taipale, H. Mortality in Schizophrenia: 30-Year Nationwide Follow-up Study. Acta Psychiatr. Scand. 2018, 138, 492–499. [Google Scholar] [CrossRef]
- Cabassa, L.J.; Camacho, D.; Vélez-Grau, C.M.; Stefancic, A. Peer-Based Health Interventions for People with Serious Mental Illness: A Systematic Literature Review. J. Psychiatr. Res. 2017, 84, 80–89. [Google Scholar] [CrossRef]
- Lorig, K.; Ritter, P.L.; Pifer, C.; Werner, P. Effectiveness of the Chronic Disease Self-Management Program for Persons with a Serious Mental Illness: A Translation Study. Community Ment. Health J. 2014, 50, 96–103. [Google Scholar] [CrossRef]
- Scheewe, T.W.; Backx, F.J.G.; Takken, T.; Jörg, F.; van Strater, A.C.P.; Kroes, A.G.; Kahn, R.S.; Cahn, W. Exercise Therapy Improves Mental and Physical Health in Schizophrenia: A Randomised Controlled Trial. Acta Psychiatr. Scand. 2013, 127, 464–473. [Google Scholar] [CrossRef]
- Goldman, M.L.; Spaeth-Rublee, B.; Pincus, H.A. The Case for Severe Mental Illness as a Disparities Category. Psychiatr. Serv. 2018, 69, 726–728. [Google Scholar] [CrossRef]
- Lancet, T. The Health Crisis of Mental Health Stigma. Lancet 2016, 387, 1027. [Google Scholar] [CrossRef]
- Crawford, M.J.; Jayakumar, S.; Lemmey, S.J.; Zalewska, K.; Patel, M.X.; Cooper, S.J.; Shiers, D. Assessment and Treatment of Physical Health Problems among People with Schizophrenia: National Cross-Sectional Study. Br. J. Psychiatry 2014, 205, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L.; Roalfe, A.; Wilson, S.; Lester, H. Physical Health Care of Patients with Schizophrenia in Primary Care: A Comparative Study. Fam. Pract. 2007, 24, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Shefer, G.; Henderson, C.; Howard, L.M.; Murray, J.; Thornicroft, G. Diagnostic Overshadowing and Other Challenges Involved in the Diagnostic Process of Patients with Mental Illness Who Present in Emergency Departments with Physical Symptoms—A Qualitative Study. PLoS ONE 2014, 9, e111682. [Google Scholar] [CrossRef]
- Kidd, S.A.; Frederick, T.; Tarasoff, L.A.; Virdee, G.; Lurie, S.; Davidson, L.; Morris, D.; McKenzie, K. Locating Community among People with Schizophrenia Living in a Diverse Urban Environment. Am. J. Psychiatr. Rehabil. 2016, 19, 103–121. [Google Scholar] [CrossRef]
- Rastad, C.; Martin, C.; Åsenlöf, P. Barriers, Benefits, and Strategies for Physical Activity in Patients With Schizophrenia. Phys. Ther. 2014, 94, 1467–1479. [Google Scholar] [CrossRef]
- Rotenberg, M.; Tuck, A.; Anderson, K.K.; McKenzie, K. Green Space and the Incidence of Schizophrenia in Toronto, Canada. Can. J. Psychiatry 2022, 67, 238–240. [Google Scholar] [CrossRef]
- Strauss, G.P. A Bioecosystem Theory of Negative Symptoms in Schizophrenia. Front. Psychiatry 2021, 12. [Google Scholar] [CrossRef]
- Aschbrenner, K.; Carpenter-Song, E.; Mueser, K.; Kinney, A.; Pratt, S.; Bartels, S. A Qualitative Study of Social Facilitators and Barriers to Health Behavior Change Among Persons with Serious Mental Illness. Community Ment. Health J. 2013, 49, 207–212. [Google Scholar] [CrossRef]
- Degnan, A.; Berry, K.; Sweet, D.; Abel, K.; Crossley, N.; Edge, D. Social Networks and Symptomatic and Functional Outcomes in Schizophrenia: A Systematic Review and Meta-Analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 873–888. [Google Scholar] [CrossRef]
- Roberts, S.H.; Bailey, J.E. An Ethnographic Study of the Incentives and Barriers to Lifestyle Interventions for People with Severe Mental Illness. J. Adv. Nurs. 2013, 69, 2514–2524. [Google Scholar] [CrossRef]
- Shiner, B.; Whitley, R.; Van Citters, A.D.; Pratt, S.I.; Bartels, S.J. Learning What Matters for Patients: Qualitative Evaluation of a Health Promotion Program for Those with Serious Mental Illness. Health Promot. Int. 2008, 23, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.A.; Osborn, D.P.J.; Nazareth, I.; King, M.B. Prevention of Coronary Heart Disease in People with Severe Mental Illnesses: A Qualitative Study of Patient and Professionals’ Preferences for Care. BMC Psychiatry 2006, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Yarborough, B.J.H.; Stumbo, S.P.; Yarborough, M.T.; Young, T.J.; Green, C.A. Improving Lifestyle Interventions for People with Serious Mental Illnesses: Qualitative Results from the STRIDE Study. Psychiatr. Rehabil. J. 2016, 39, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.S.; Alpert, M.; Nienow, T.M.; Dinzeo, T.J.; Docherty, N.M. Computerized Measurement of Negative Symptoms in Schizophrenia. J. Psychiatr. Res. 2008, 42, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.S.; McGovern, J.E.; Dinzeo, T.J.; Covington, M.A. Speech Deficits in Serious Mental Illness: A Cognitive Resource Issue? Schizophr. Res. 2014, 160, 173–179. [Google Scholar] [CrossRef]
- Docherty, N.M.; Cohen, A.; Nienow, T.; Dinzeo, T.; Dangelmaier, R. Stability of Formal Thought Disorder and Referential Communication Disturbances in Schizophrenia. J. Abnorm. Psychol. 2003, 112, 469–475. [Google Scholar] [CrossRef]
- Loper, E.; Bird, S. NLTK: The Natural Language Toolkit. arXiv 2002, arXiv:cs/0205028. [Google Scholar]
- Grootendorst, M. BERTopic: Neural Topic Modeling with a Class-Based TF-IDF Procedure. arXiv 2022, arXiv:2203.05794. [Google Scholar]
- Blei, D.M.; Ng, A.Y.; Jordan, M.I. Latent Dirichlet Allocation. J. Mach. Learn. Res. 2003, 3, 993–1022. [Google Scholar]
- McInnes, L.; Healy, J.; Astels, S. Hdbscan: Hierarchical Density Based Clustering. JOSS 2017, 2, 205. [Google Scholar] [CrossRef]
- Thornicroft, G. Physical Health Disparities and Mental Illness: The Scandal of Premature Mortality. Br. J. Psychiatry 2011, 199, 441–442. [Google Scholar] [CrossRef] [PubMed]
- van Nieuwenhuizen, A.; Henderson, C.; Kassam, A.; Graham, T.; Murray, J.; Howard, L.M.; Thornicroft, G. Emergency Department Staff Views and Experiences on Diagnostic Overshadowing Related to People with Mental Illness. Epidemiol. Psychiatr. Sci. 2012, 22, 255–262. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, J.H.; Gheewala, N.M.; O’Keefe, J.O. Dietary Strategies for Improving Post-Prandial Glucose, Lipids, Inflammation, and Cardiovascular Health. J. Am. Coll. Cardiol. 2008, 51, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Sami, W.; Ansari, T.; Butt, N.S.; Hamid, M.R.A. Effect of Diet on Type 2 Diabetes Mellitus: A Review. Int. J. Health Sci. 2017, 11, 65–71. [Google Scholar]
- McEvedy, S.M.; Sullivan-Mort, G.; McLean, S.A.; Pascoe, M.C.; Paxton, S.J. Ineffectiveness of Commercial Weight-Loss Programs for Achieving Modest but Meaningful Weight Loss: Systematic Review and Meta-Analysis. J. Health Psychol. 2017, 22, 1614–1627. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Ecological systems theory. In Six Theories of Child Development: Revised Formulations and Current Issues; Jessica Kingsley Publishers: London, UK, 1992; pp. 187–249. ISBN 978-1-85302-137-4. [Google Scholar]
- Berkowitz, S.A.; Karter, A.J.; Corbie-Smith, G.; Seligman, H.K.; Ackroyd, S.A.; Barnard, L.S.; Atlas, S.J.; Wexler, D.J. Food Insecurity, Food “Deserts,” and Glycemic Control in Patients With Diabetes: A Longitudinal Analysis. Diabetes Care 2018, 41, 1188–1195. [Google Scholar] [CrossRef]
- Fortuna, K.L.; Williams, A.; Mois, G.; Jason, K.; Bianco, C.L. Social Processes Associated With Health and Health Behaviors Linked to Early Mortality in People with a Diagnosis of a Serious Mental Illness. Perspect. Psychol. Sci. 2022, 17, 183–190. [Google Scholar] [CrossRef]
- Soundy, A.; Wampers, M.; Probst, M.; De Hert, M.; Stubbs, B.; Vancampfort, D.; Attux, C.; Leutwyler, H.; Ströhle, A. Physical Activity and Sedentary Behaviour in Outpatients with Schizophrenia: A Systematic Review and Meta-Analysis. Int. J. Ther. Rehabil. 2013, 20, 588–595. [Google Scholar] [CrossRef]
- Vancampfort, D.; De Hert, M.; Vansteenkiste, M.; De Herdt, A.; Scheewe, T.W.; Soundy, A.; Stubbs, B.; Probst, M. The Importance of Self-Determined Motivation towards Physical Activity in Patients with Schizophrenia. Psychiatry Res. 2013, 210, 812–818. [Google Scholar] [CrossRef]
- Henson, P.; Pearson, J.F.; Keshavan, M.; Torous, J. Impact of Dynamic Greenspace Exposure on Symptomatology in Individuals with Schizophrenia. PLoS ONE 2020, 15, e0238498. [Google Scholar] [CrossRef] [PubMed]
- South, E.C.; Hohl, B.C.; Kondo, M.C.; MacDonald, J.M.; Branas, C.C. Effect of Greening Vacant Land on Mental Health of Community-Dwelling Adults: A Cluster Randomized Trial. JAMA Netw. Open 2018, 1, e180298. [Google Scholar] [CrossRef] [PubMed]
- Walsan, R.; Feng, X.; Mayne, D.J.; Pai, N.; Bonney, A. Neighborhood Environment and Type 2 Diabetes Comorbidity in Serious Mental Illness. J. Prim. Care Community Health 2020, 11, 2150132720924989. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study 1 | Study 2 | Study 3 | Total | |
|---|---|---|---|---|
| (Docherty et al., 2003) | (Cohen et al., 2008) | (Cohen et al., 2014) | ||
| Sample Size (Schizophrenia Spectrum/Other SMI/Controls) | 141/0/0 | 0/94/0 | 43/50/38 | 184/144/38 |
| Number of Language Samples (Schizophrenia Spectrum/Other SMI/Controls) | 591/0/0 | 0/94/0 | 298/236/247 | 889/330/247 |
| Sex (Men/Women) | 68/60 | 63/21 | 57/42 | 188/123 |
| Race (Black/White/Other) | 23/79/1 | 53/31/0 | 41/59/4 | 117/169/5 |
| Age (M ± SD) | 37.2 ± 8.7 | 41.3 ± 8.2 | 41.7 ± 11.8 | 39.8 ± 10.1 |
| Speaking Task | Affectively good, bad, and neutral life memories | Affectively unspecified life memories | Affectively good, bad, and neutral life memories | - |
| Speaking K and Length | 4 recordings, each 10 min long | 1 recording, 5 min long | 5 recordings, each 1.5 min long | - |
| Speaking Task Format | Conversation with interviewer | Conversation with interviewer | Monologue | - |
| Geographic Region | North-central US | North-central US | South-central US | - |
| Topic | Name | Emotional Valence | Top Contributing Terms |
|---|---|---|---|
| 0 | Food * | Positive | food, eat, cook, love, chicken, cooking, eating, good, favorite, lot |
| 1 | Hobbies * | Positive | hobbies, hobby, play, watch, love, read, just, favorite, lot, music |
| 2 | peace | peace, feel, relaxed, outside, just, calm, felt, really, peaceful, feeling | |
| 3 | Routine * | Neutral | usually, work, day, habits, just, home, things, time, ah, watch |
| 4 | memories | know, fun, just, good, went, lot, used, memories, time, remember | |
| 5 | people | know, people, think, ah, just, person, things, lot, time, kind | |
| 6 | life | just, got, people, want, life, going, yes, good, know, ah | |
| 7 | home | room, live, bedroom, living, kitchen, house, living room, nice, roommate, tv | |
| 8 | happy | happy, best, time, just, know, good, got, award, school, real | |
| 9 | sad | sad, felt, low, energy, feel, low energy, feel sad, passed, times, away | |
| 10 | Scared * | Negative | know, run, bad, snake, really, got, time, going, sad, dad |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cowan, T.; Rodriguez, Z.B.; Granrud, O.E.; Masucci, M.D.; Docherty, N.M.; Cohen, A.S. Talking about Health: A Topic Analysis of Narratives from Individuals with Schizophrenia and Other Serious Mental Illnesses. Behav. Sci. 2022, 12, 286. https://doi.org/10.3390/bs12080286
Cowan T, Rodriguez ZB, Granrud OE, Masucci MD, Docherty NM, Cohen AS. Talking about Health: A Topic Analysis of Narratives from Individuals with Schizophrenia and Other Serious Mental Illnesses. Behavioral Sciences. 2022; 12(8):286. https://doi.org/10.3390/bs12080286
Chicago/Turabian StyleCowan, Tovah, Zachary B. Rodriguez, Ole Edvard Granrud, Michael D. Masucci, Nancy M. Docherty, and Alex S. Cohen. 2022. "Talking about Health: A Topic Analysis of Narratives from Individuals with Schizophrenia and Other Serious Mental Illnesses" Behavioral Sciences 12, no. 8: 286. https://doi.org/10.3390/bs12080286
APA StyleCowan, T., Rodriguez, Z. B., Granrud, O. E., Masucci, M. D., Docherty, N. M., & Cohen, A. S. (2022). Talking about Health: A Topic Analysis of Narratives from Individuals with Schizophrenia and Other Serious Mental Illnesses. Behavioral Sciences, 12(8), 286. https://doi.org/10.3390/bs12080286