
Prognostic Efficacy of Complete Blood Count Indices for Assessing the Presence and the Progression of Myxomatous Mitral Valve Disease in Dogs

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Classification of Myxomatous Mitral Valve Disease
2.3. Laboratory Analysis
2.4. Thoracic Radiography
2.5. Echocardiography
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
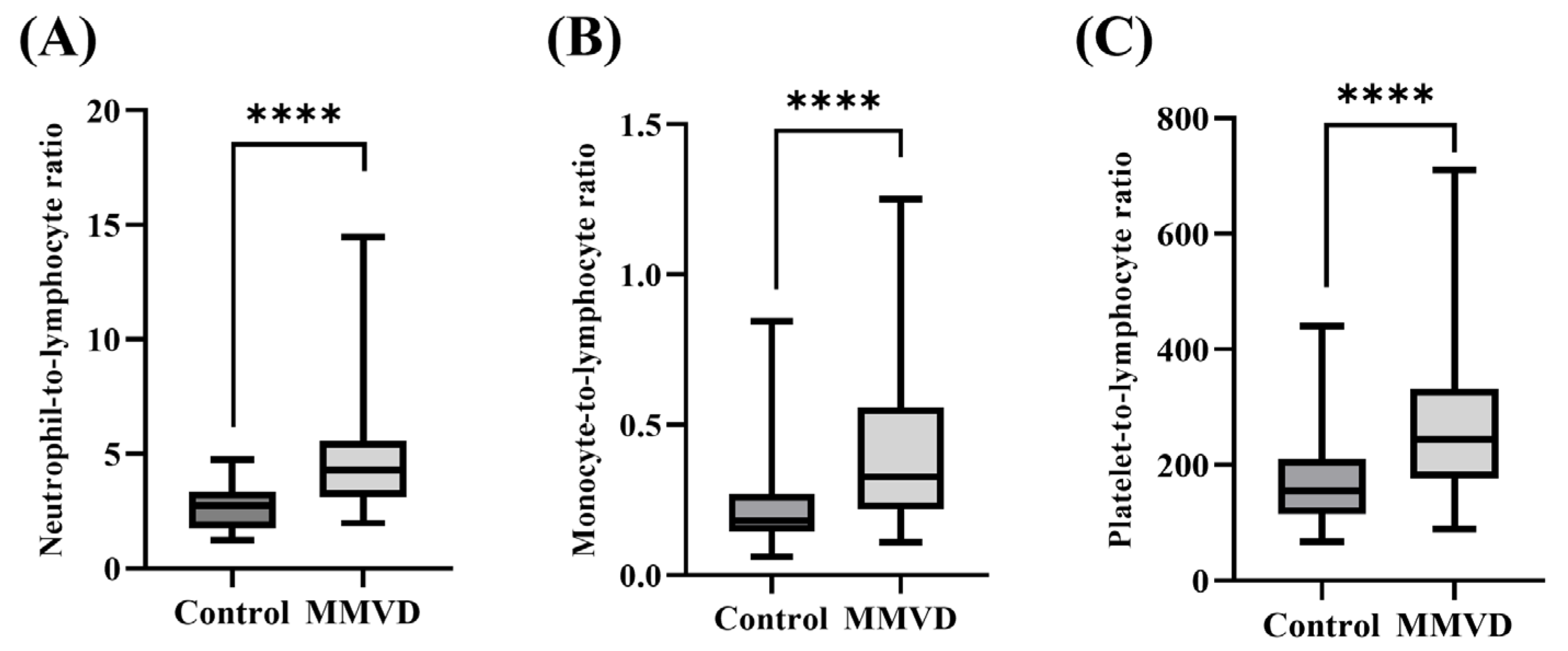
3.2. Comparison of Clinical and Hematological Variables between Healthy Dogs and Those with MMVD
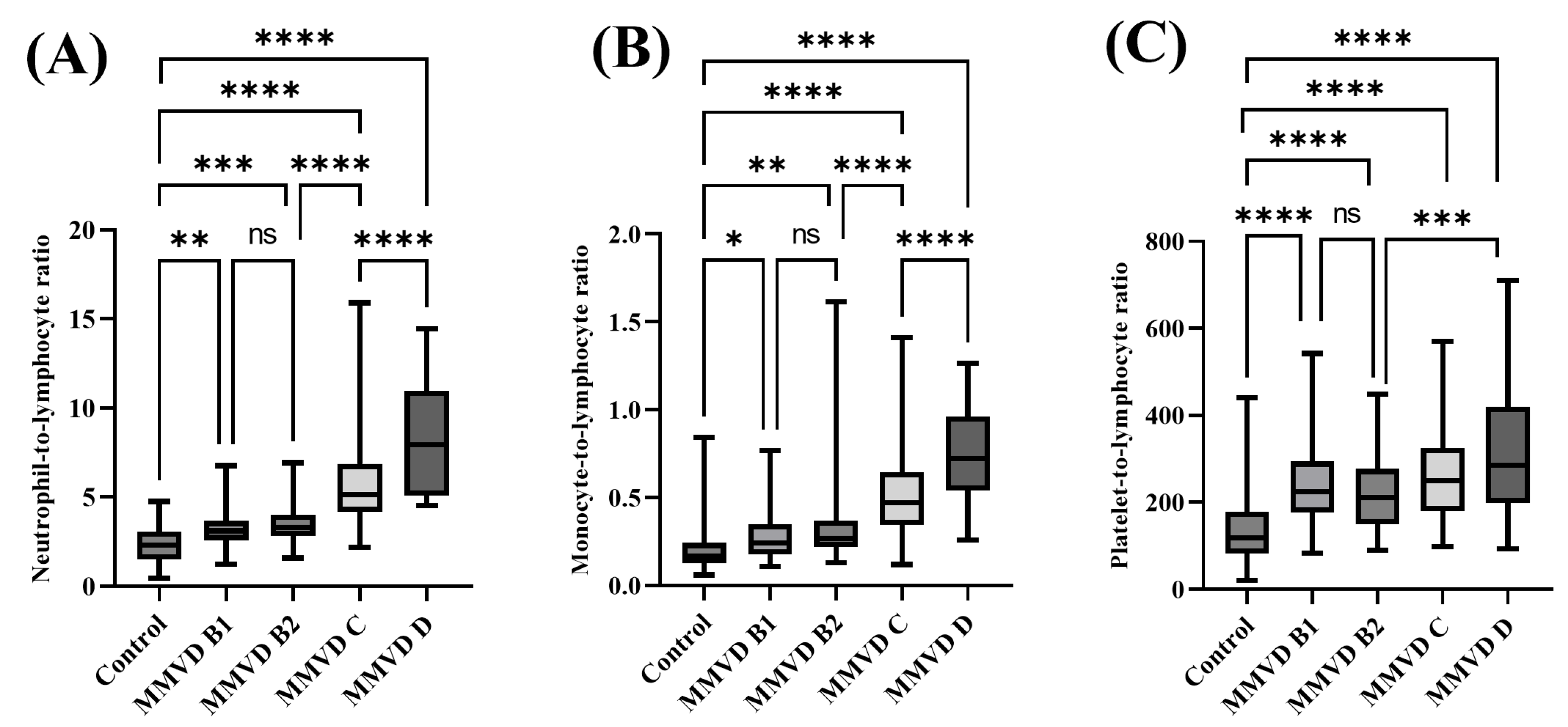
3.3. Comparison of Clinical and Hematological Variables between Healthy Dogs and Those with MMVD at Different Stages
3.4. Comparison between CBC Indices According to the Presence of PE in the Symptomatic MMVD Groups
3.5. Correlations of CBC Indices with Conventional Biomarker, Radiographic, and Echocardiographic Variables
3.6. Efficacy of CBC Indices for Predicting MMVD
3.7. Diagnostic Efficacy of CBC Indices for Detecting the Severity of MMVD
3.8. Survival Analysis According to the Increase in the NLR, MLR, and PLR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Keene, B.W.; Atkins, C.E.; Bonagura, J.D.; Fox, P.R.; Häggström, J.; Fuentes, V.L.; Oyama, M.A.; Rush, J.E.; Stepien, R.; Uechi, M. ACVIM Consensus Guidelines for the Diagnosis and Treatment of Myxomatous Mitral Valve Disease in Dogs. J. Vet. Intern. Med. 2019, 33, 1127–1140. [Google Scholar] [CrossRef] [PubMed]
- Piantedosi, D.; Musco, N.; Palatucci, A.T.; Carriero, F.; Rubino, V.; Pizzo, F.; Nasir, S.; Molinaro, G.; Ruggiero, G.; Terrazzano, G.; et al. Pro-Inflammatory and Immunological Profile of Dogs with Myxomatous Mitral Valve Disease. Vet. Sci. 2022, 9, 326. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.-I.; Han, D.-H.; Lee, S.-G.; Hung, Y.-W.; Choi, R.; Hyun, C. Chronic Mitral Valve Insufficiency in Dogs: Recent Advances in Diagnosis and Treatment. In Canine Medicine: Recent Topics and Advanced Research; BoD–Books on Demand: Norderstedt, Germany, 2016; pp. 95–124. [Google Scholar] [CrossRef]
- Cunningham, S.M.; Rush, J.E.; Freeman, L.M. Systemic Inflammation and Endothelial Dysfunction in Dogs with Congestive Heart Failure. J. Vet. Intern. Med. 2012, 26, 547–557. [Google Scholar] [CrossRef]
- Domanjko Petrič, A.; Lukman, T.; Verk, B.; Nemec Svete, A. Systemic Inflammation in Dogs with Advanced-Stage Heart Failure. Acta Vet. Scand. 2018, 60, 20. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.; Dai, C.; Xu, K.; Wu, M. Predictive Value of Neutrophil to Lymphocyte Ratio and Red Cell Distribution Width on Death for ST Segment Elevation Myocardial Infarction. Sci. Rep. 2021, 11, 11506. [Google Scholar] [CrossRef] [PubMed]
- Balta, S.; Ozturk, C. The Platelet-Lymphocyte Ratio: A Simple, Inexpensive and Rapid Prognostic Marker for Cardiovascular Events. Platelets 2015, 26, 680–681. [Google Scholar] [CrossRef]
- Liu, Z.; Li, Y.; Wang, Y.; Zhang, H.; Lian, Y.; Cheng, X. The Neutrophil-to-Lymphocyte and Monocyte-to-Lymphocyte Ratios Are Independently Associated with the Severity of Autoimmune Encephalitis. Front. Immunol. 2022, 13, 911779. [Google Scholar] [CrossRef]
- Angkananard, T.; Anothaisintawee, T.; McEvoy, M.; Attia, J.; Thakkinstian, A. Neutrophil Lymphocyte Ratio and Cardiovascular Disease Risk: A Systematic Review and Meta-Analysis. Biomed Res. Int. 2018, 2018, 2703518. [Google Scholar] [CrossRef]
- Börekçi, A.; Gür, M.; Türkoʇlu, C.; Baykan, A.O.; Seker, T.; Sahin, D.Y.; Harbalioʇlu, H.; Elbasan, Z.; Topuz, M.; Çayli, M. Neutrophil to Lymphocyte Ratio Predicts Left Ventricular Remodeling in Patients with ST Elevation Myocardial Infarction after Primary Percutaneous Coronary Intervention. Korean Circ. J. 2016, 46, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, D.; Bozgul, S.M.K.; Emgin, O.; Butun, O.; Kose, T.; Simsek, E.; Hekimgil, M.; Kilic, S. Mortal İnteraction between Hemophagocytic Syndrome and Newly Developed Heart Fail. Arq. Bras. Cardiol. 2021, 116, 395–401. [Google Scholar] [CrossRef]
- Urbanowicz, T.; Olasińska-Wiśniewska, A.; Michalak, M.; Rodzki, M.; Witkowska, A.; Straburzyńska-Migaj, E.; Perek, B.; Jemielity, M. The Prognostic Significance of Neutrophil to Lymphocyte Ratio (NLR), Monocyte to Lymphocyte Ratio (MLR) and Platelet to Lymphocyte Ratio (PLR) on Long-Term Survival in Off-Pump Coronary Artery Bypass Grafting (OPCAB) Procedures. Biology 2022, 11, 34. [Google Scholar] [CrossRef] [PubMed]
- Afari, M.E.; Bhat, T. Neutrophil to Lymphocyte Ratio (NLR) and Cardiovascular Diseases: An Update. Expert Rev. Cardiovasc. Ther. 2016, 14, 573–577. [Google Scholar] [CrossRef]
- Chen, H.; Li, M.; Liu, L.; Dang, X.; Zhu, D.; Tian, G. Monocyte/Lymphocyte Ratio Is Related to the Severity of Coronary Artery Disease and Clinical Outcome in Patients with Non-ST-Elevation Myocardial Infarction. Medicine 2019, 98, 16267. [Google Scholar] [CrossRef] [PubMed]
- Dadouli, K.; Janho, M.B.; Hatziefthimiou, A.; Voulgaridi, I.; Piaha, K.; Anagnostopoulos, L.; Ntellas, P.; Mouchtouri, V.A.; Bonotis, K.; Christodoulou, N.; et al. Neutrophil-to-Lymphocyte, Monocyte-to-Lymphocyte, Platelet-to-Lymphocyte Ratio and Systemic Immune-Inflammatory Index in Different States of Bipolar Disorder. Brain Sci. 2022, 12, 1034. [Google Scholar] [CrossRef] [PubMed]
- Fries, R.C.; Kadotani, S.; Stack, J.P.; Kruckman, L.; Wallace, G. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in Cats with Hypertrophic Cardiomyopathy. Front. Vet. Sci. 2022, 9, 813524. [Google Scholar] [CrossRef]
- Neumann, S. Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios in Dogs and Cats with Acute Pancreatitis. Vet. Clin. Pathol. 2021, 50, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Pierini, A.; Esposito, G.; Gori, E.; Benvenuti, E.; Ruggiero, P.; Lubas, G.; Marchetti, V. Platelet Abnormalities and Platelet-to-Lymphocyte Ratios in Canine Immunosuppressant-Responsive and Non-Responsive Enteropathy: A Retrospective Study in 41 Dogs. J. Vet. Med. Sci. 2021, 83, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Sottnik, J.L.; Rao, S.; Lafferty, M.H.; Thamm, D.H.; Morley, P.S.; Withrow, S.J.; Dow, S.W. Association of Blood Monocyte and Lymphocyte Count and Disease-Free Interval in Dogs with Osteosarcoma. J. Vet. Intern. Med. 2010, 24, 1439–1444. [Google Scholar] [CrossRef]
- Druzhaeva, N.; Nemec Svete, A.; Ihan, A.; Pohar, K.; Domanjko Petrič, A. Peripheral Blood Lymphocyte Subtypes in Dogs with Different Stages of Myxomatous Mitral Valve Disease. J. Vet. Intern. Med. 2021, 35, 2112–2122. [Google Scholar] [CrossRef] [PubMed]
- Hamilton-Elliott, J.; Ambrose, E.; Christley, R.; Dukes-McEwan, J. White Blood Cell Differentials in Dogs with Congestive Heart Failure (CHF) in Comparison to Those in Dogs without Cardiac Disease. J. Small Anim. Pract. 2018, 59, 364–372. [Google Scholar] [CrossRef]
- Rubio, C.P.; Saril, A.; Kocaturk, M.; Tanaka, R.; Koch, J.; Ceron, J.J.; Yilmaz, Z. Changes of Inflammatory and Oxidative Stress Biomarkers in Dogs with Different Stages of Heart Failure. BMC Vet. Res. 2020, 16, 433. [Google Scholar] [CrossRef]
- Rejec, A.; Butinar, J.; Gawor, J.; Petelin, M. Evaluation of Complete Blood Count Indices (NLR, PLR, MPV/PLT, and PLCRi) in Healthy Dogs, Dogs with Periodontitis, and Dogs with Oropharyngeal Tumors as Potential Biomarkers of Systemic Inflammatory Response. J. Vet. Dent. 2017, 34, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Sahn, D.J.; DeMaria, A.; Kisslo, J.; Weyman, A. Recommendations Regarding Quantitation in M-Mode Echocardiography: Results of a Survey of Echocardiographic Measurements. Circulation 1978, 58, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F. Research Methods for Business. Educ. + Train. 2007, 49, 336–337. [Google Scholar] [CrossRef]
- Cohn, J.N.; Ferrari, R.; Sharpe, N. Cardiac Remodeling-Concepts and Clinical Implications: A Consensus Paper from an International Forum on Cardiac Remodeling. J. Am. Coll. Cardiol. 2000, 35, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Farabaugh, A.E.; Freeman, L.M.; Rush, J.E.; George, K.L. Lymphocyte Subpopulations and Hematologic Variables in Dogs with Congestive Heart Failure. J. Vet. Intern. Med. 2004, 18, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Totani, L.; Evangelista, V. Platelet-Leukocyte Interactions in Cardiovascular Disease and Beyond. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 2357–2361. [Google Scholar] [CrossRef] [PubMed]
- Durmus, E.; Kivrak, T.; Gerin, F.; Sunbul, M.; Sari, I.; Erdogan, O. Relações Neutrófilo-Linfócito e Plaqueta-Linfócito Como Preditores de Insuficiência Cardíaca. Arq. Bras. Cardiol. 2015, 105, 606–613. [Google Scholar] [CrossRef]
- Gijsberts, C.M.; Ellenbroek, G.H.J.M.; ten Berg, M.J.; Huisman, A.; van Solinge, W.W.; Lam, C.S.; Asselbergs, F.W.; den Ruijter, H.M.; Pasterkamp, G.; Hoefer, I.E.; et al. Effect of Monocyte-to-Lymphocyte Ratio on Heart Failure Characteristics and Hospitalizations in a Coronary Angiography Cohort. Am. J. Cardiol. 2017, 120, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.; Li, Y.; Fan, Z.; Zuo, B.; Jian, X.; Li, L.; Liu, T. Monocyte/Lymphocyte Ratio Predicts the Severity of Coronary Artery Disease: A Syntax Score Assessment. BMC Cardiovasc. Disord. 2017, 17, 90. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Ambrosy, A.P.; Greene, S.J.; Mentz, R.J.; Subacius, H.P.; Maggioni, A.P.; Swedberg, K.; Nodari, S.; Zannad, F.; Konstam, M.A.; et al. Predictive Value of Low Relative Lymphocyte Count in Patients Hospitalized for Heart Failure with Reduced Ejection Fraction. Circ. Heart Fail. 2012, 5, 750–758. [Google Scholar] [CrossRef]
- Demirtas, S.; Karahan, O.; Yazici, S.; Guclu, O.; Caliskan, A.; Yavuz, C.; Kucuker, A.; Mavitas, B. The Relationship between Complete Blood Count Parameters and FontainE′s Stages in Patients with Peripheral Arterial Disease. Vascular 2014, 22, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, R.; Murota, A.; Nagashima, Y.; Yamane, Y. Changes in Platelet Life Span in Dogs with Mitral Valve Regurgitation. J. Vet. Intern. Med. 2002, 16, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Szydełko, J.; Szydełko-Gorzkowicz, M.; Matyjaszek-matuszek, B. Neutrophil-to-lymphocyte, Platelet-to-lymphocyte Ratios, and Systemic Immune-inflammation Index as Potential Biomarkers of Chronic Inflammation in Patients with Newly Diagnosed Acromegaly: A Single-centre Study. J. Clin. Med. 2021, 10, 3997. [Google Scholar] [CrossRef]
- Bai, B.; Cheng, M.; Jiang, L.; Xu, J.; Chen, H.; Xu, Y. High Neutrophil to Lymphocyte Ratio and Its Gene Signatures Correlate with Diastolic Dysfunction in Heart Failure With Preserved Ejection Fraction. Front. Cardiovasc. Med. 2021, 8, 614757. [Google Scholar] [CrossRef] [PubMed]
- Hua, Y.; Sun, J.-Y.; Lou, Y.-X.; Sun, W.; Kong, X.-Q. Monocyte-to-Lymphocyte Ratio Predicts Mortality and Cardiovascular Mortality in the General Population. Int. J. Cardiol. 2023, 379, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Pourafkari, L.; Wang, C.K.; Tajlil, A.; Afshar, A.H.; Schwartz, M.; Nader, N.D. Platelet-Lymphocyte Ratio in Prediction of Outcome of Acute Heart Failure. Biomark. Med. 2018, 12, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, S.; Nagai, Y.; Shutta, R.; Masuda, D.; Yamashita, S.; Seo, M.; Yamada, T.; Nakagawa, A.; Yasumura, Y.; Nakagawa, Y.; et al. Combination of Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios as a Novel Predictor of Cardiac Death in Patients with Acute Decompensated Heart Failure with Preserved Left Ventricular Ejection Fraction: A Multicenter Study. J. Am. Heart Assoc. 2023, 12, 26326. [Google Scholar] [CrossRef]
- Ku, D.; Chae, Y.; Kim, C.; Koo, Y.; Lee, D.; Yun, T.; Chang, D.; Kang, B.-T.; Yang, M.-P.; Kim, H. Severity of Myxomatous Mitral Valve Disease in Dogs May Be Predicted Using Neutrophil-to-Lymphocyte and Monocyte-to-Lymphocyte Ratio. Am. J. Vet. Res. 2023, 84, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cremer, S.E.; Singletary, G.E.; Olsen, L.H.; Wallace, K.; Häggström, J.; Ljungvall, I.; Höglund, K.; Reynolds, C.A.; Pizzinat, N.; Oyama, M.A. Serotonin Concentrations in Platelets, Plasma, Mitral Valve Leaflet, and Left Ventricular Myocardial Tissue in Dogs with Myxomatous Mitral Valve Disease. J. Vet. Intern. Med. 2014, 28, 1534–1540. [Google Scholar] [CrossRef]
- Nemec Svete, A.; Verk, B.; Čebulj-Kadunc, N.; Salobir, J.; Rezar, V.; Domanjko Petrič, A. Inflammation and Its Association with Oxidative Stress in Dogs with Heart Failure. BMC Vet. Res. 2021, 17, 176. [Google Scholar] [CrossRef]
- Yalim, Z.; Ersoy, İ. Evaluation of Inflammation Markers in Mitral Valve Prolapse. Arch. Cardiol. Mex. 2022, 92, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Dobbe, L.; Rahman, R.; Elmassry, M.; Paz, P.; Nugent, K. Cardiogenic Pulmonary Edema. Am. J. Med. Sci. 2019, 358, 389–397. [Google Scholar] [CrossRef]
- Pappas, L.; Filippatos, G. Pulmonary congestion in acute heart failure: From hemodynamics to lung injury and barrier dysfunction. Rev. Esp. Cardiol. 2011, 64, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Arfsten, H.; Cho, A.; Prausmüller, S.; Spinka, G.; Novak, J.; Goliasch, G.; Bartko, P.E.; Raderer, M.; Gisslinger, H.; Kornek, G.; et al. Inflammation-Based Scores as a Common Tool for Prognostic Assessment in Heart Failure or Cancer. Front. Cardiovasc. Med. 2021, 8, 725903. [Google Scholar] [CrossRef] [PubMed]
- Hussein, F.I.; Hariyanto, D.; Izzah, A.Z. Correlation of Neutrophil to Lymphocyte Ratio (NLR) Values to Ejection Fraction, Fraction Shortening, and E/A Ratio in Children with Rheumatic Heart Disease (RHD) at Dr. M. Djamil General Hospital, Padang, Indonesia. Biosci. Med. J. Biomed. Transl. Res. 2022, 6, 2789–2793. [Google Scholar] [CrossRef]
- Li, Z.; Rong, H.; Wu, W.; Huang, T.; Xu, J. Application Value of NT-ProBNP Combined with NLR in Evaluation of Major Adverse Cardiac Events in Elderly Patients with Chronic Heart Failure. Emerg. Med. Int. 2022, 2022, 3689445. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Control | MMVD B1 | MMVD B2 | MMVD C | MMVD D |
|---|---|---|---|---|---|
| Number of dogs | 75 | 90 | 49 | 92 | 18 |
| Clinical variables | |||||
| Sex (male/female) | 40/35 | 52/38 | 29/20 | 45/47 | 8/10 |
| [IM:CM]/[IF:SF] | [6:34]/[17:18] | [6:46]/[6:32] | [3:26]/[3:17] | [3:42]/[9:38] | [1:7]/[4:6] |
| Age (years) | 6.48 ± 4.46 | 12.21 ± 3.07 a | 12.35 ± 2.29 a | 12.51 ± 2.95 a | 12.06 ± 3.40 a |
| SBP (mmHg) | 135.21 ± 14.82 | 141.39 ± 14.95 | 138.84 ± 11.87 | 136.98 ± 15.02 | 134.89 ± 17.08 |
| Heart rate (beats/min) | 140.20 ± 28.00 | 144.30 ± 27.89 | 142.52 ± 27.32 | 149.39 ± 29.57 | 159.78 ± 17.64 |
| Radiographic variable | |||||
| VHS | 10.01 ± 0.50 | 9.90 ± 1.17 | 10.98 ± 0.70 a,b | 11.54 ± 1.03 a,b,c | 12.28 ± 1.05 a,b,c,d |
| Echocardiographic variables | |||||
| FS (%) | 45.76 ± 12.83 | 52.34 ± 10.62 | 54.46 ± 10.04 a | 56.16 ± 8.35a | 54.54 ± 8.11 a |
| EF (%) | 76.00 ± 15.10 | 92.54 ± 83.23 | 85.59 ± 7.72 | 86.60 ± 7.80 | 85.56 ± 8.20 |
| LA/Ao | 1.16 ± 0.23 | 1.19 ± 0.50 | 1.45 ± 0.29 a,b | 1.83 ± 0.59 a,b,c | 2.14 ± 0.65 a,b,c,d |
| E/A | 2.13 ± 8.85 | 0.92 ± 0.26 | 0.98 ± 0.26 | 1.32 ± 0.68 b,c | 1.86 ± 1.07 |
| E′/A′ | 1.11 ± 1.59 | 0.71 ± 0.24 | 0.79 ± 0.38 | 1.07 ± 0.53 | 1.25 ± 0.78 |
| E/E′ | 11.50 ± 3.38 | 12.59 ± 2.92 | 13.21 ± 4.10 | 12.60 ± 5.28 | 14.69 ± 9.77 |
| Group | Control | MMVD B1 | MMVD B2 | MMVD C | MMVD D |
|---|---|---|---|---|---|
| Number of dogs | 22 | 38 | 19 | 43 | 5 |
| Conventional biomarker | |||||
| NT-proBNP (pmol/L) | 668.50 (446.50–738.00) | 748.50 (574.50–1574.50) | 1458.00 (883.00–2126.00) a | 2745.00 (1820.00–5515.00) a,b,c | 5000.00 (3177.00–6842.00) a,b,c |
| Variables | Before PSM | After PSM | ||||
|---|---|---|---|---|---|---|
| Control Group (n = 75) | MMVD Group (n = 249) | p-Value | Control Group (n = 40) | MMVD Group (n = 96) | p-Value | |
| Clinical variables | ||||||
| Age (years) | 6.48 ± 4.45 | 12.34 ± 2.91 a | <0.0001 | 9.75 ± 3.40 | 10.73 ± 3.01 | 0.099 |
| Hematological variables | ||||||
| WBC (K/μL) | 9.61 ± 5.35 | 11.56 ± 5.22 a | 0.006 | 9.79 ± 7.09 | 11.74 ± 4.96 | 0.069 |
| Neutrophil (K/μL) | 5.46 ± 1.74 | 8.47 ± 4.49 a | <0.0001 | 5.61 ± 1.97 | 8.68 ± 4.40 a | <0.0001 |
| Monocyte (K/μL) | 0.48 ± 0.29 | 0.77 ± 0.55 a | <0.0001 | 0.45 ± 0.30 | 0.73 ± 0.44 a | <0.0001 |
| Lymphocyte (K/μL) | 2.43 ± 1.05 | 1.92 ± 0.65 a | <0.0001 | 2.22 ± 0.74 | 1.86 ± 0.55 a | 0.007 |
| Platelet (K/μL) | 311.58 ± 114.18 | 440.61 ± 145.39 a | <0.0001 | 331.67 ± 128.51 | 456.34 ± 161.89 a | 0.002 |
| NLR | 2.33 ±0.93 | 4.58 ± 2.33 a | <0.0001 | 2.67 ± 0.87 | 4.83 ± 2.50 a | <0.0001 |
| MLR | 0.20 ± 0.11 | 0.41 ± 0.25 a | <0.0001 | 0.22 ± 0.13 | 0.40 ± 0.24 a | <0.0001 |
| PLR | 137.61 ± 77.59 | 247.94 ± 106.00 a | <0.0001 | 169.82 ± 82.68 | 265.72 ± 122.22 a | <0.0001 |
| Variables | Control (n = 75) | MMVD B1 (n = 90) | MMVD B2 (n = 49) | MMVD C (n = 92) | MMVD D (n = 18) |
|---|---|---|---|---|---|
| Clinical variables | |||||
| Age (years) | 6.48 ± 4.46 | 12.21 ± 3.07 a | 12.35 ± 2.29 a | 12.51 ± 2.95 a | 12.06 ± 3.40 a |
| Hematological variables | |||||
| WBC (K/μL) | 9.61 ± 5.35 | 8.32 ± 2.43 | 9.81 ± 2.77 | 14.58 ± 5.66 a,b,c | 17.07 ± 5.19 a,b,c |
| Neutrophil (K/μL) | 5.46 ± 1.74 | 5.95 ± 1.65 | 6.73 ± 1.76a | 11.14 ± 4.92 a,b,c | 13.70 ± 4.82 a,b,c,d |
| Monocyte (K/μL) | 0.48 ± 0.29 | 0.50 ± 0.26 | 0.68 ± 0.71 | 0.99 ± 0.52 a,b | 1.11 ± 0.50 a,b,c |
| Lymphocyte (K/μL) | 2.43 ± 1.05 | 1.85 ± 0.71 a | 2.00 ± 0.64 a | 1.99 ± 0.60 a | 1.74 ± 0.53 a |
| Platelet (K/μL) | 311.58 ± 114.18 | 400.83 ± 128.56 a | 405.39 ± 111.41 a | 485.78 ± 152.10 a | 504.56 ± 188.81 a,b,c |
| NLR | 2.33 ± 0.93 | 3.23 ± 0.98 a | 3.56 ± 1.08 a | 5.71 ± 2.18 a,b,c | 8.38 ± 3.22 a,b,c,d |
| MLR | 0.20 ± 0.11 | 0.28 ± 0.14 a | 0.33 ± 0.23 a | 0.51 ± 0.23 a,b,c | 0.74 ± 0.30 a,b,c,d |
| PLR | 137.61 ± 77.59 | 234.27 ± 92.46 a | 218.32 ± 81.44 a | 261.67 ± 104.07 a | 326.77 ± 177.01 a,b,c |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, M.-J.; Kim, J.-H. Prognostic Efficacy of Complete Blood Count Indices for Assessing the Presence and the Progression of Myxomatous Mitral Valve Disease in Dogs. Animals 2023, 13, 2821. https://doi.org/10.3390/ani13182821
Jung M-J, Kim J-H. Prognostic Efficacy of Complete Blood Count Indices for Assessing the Presence and the Progression of Myxomatous Mitral Valve Disease in Dogs. Animals. 2023; 13(18):2821. https://doi.org/10.3390/ani13182821
Chicago/Turabian StyleJung, Min-Jung, and Jung-Hyun Kim. 2023. "Prognostic Efficacy of Complete Blood Count Indices for Assessing the Presence and the Progression of Myxomatous Mitral Valve Disease in Dogs" Animals 13, no. 18: 2821. https://doi.org/10.3390/ani13182821
APA StyleJung, M.-J., & Kim, J.-H. (2023). Prognostic Efficacy of Complete Blood Count Indices for Assessing the Presence and the Progression of Myxomatous Mitral Valve Disease in Dogs. Animals, 13(18), 2821. https://doi.org/10.3390/ani13182821