1. Introduction
Diarrhea refers to too frequent stooling, daily emissions, or passage of liquid or very soft stool greater than 300 g/day in weight or at least three very loose stools and liquid stools per day and is “the second leading cause of death in children under five years old” [
1]. The disease is caused by a wide range of pathogens that find their way into the enteric system and may include mostly bacteria and at times, viruses and parasites. Ingested pathogenic organisms may be confined to the gastrointestinal tract or pathogens may originate from the gut and then spread to other parts of the body where they establish infections or produce toxins injurious to the host cells [
2].
The emergence and resurgence of drug resistance have been a big concern in healthcare delivery globally [
3,
4]. Diarrhoeagenic bacteria are not excluded in the development of resistance to previously effective antibiotics [
5,
6]. The phenomenal increase in the acquisition of resistance to antimicrobial drugs by pathogens has mostly been attributed to the indiscriminate and improper use of antimicrobials [
3,
7]. Infections due to
Staphylococcus aureus are presently resistant to beta-lactams, while
Enterococcus strains are resistant to vancomycin, ampicillin, gentamycin, and streptomycin [
8]. Gram-negative pathogens such as
Salmonella spp.,
Pseudomonas aeruginosa, and
Klebsiella pneumoniae have several times been reported to be multi-drug resistant [
7,
8,
9]. The loss of clinical efficacy of such previously effective first-line drugs led to a shift to the second-line or third-line antibiotics which are often more expensive and more troublesome [
3,
4]. Drug resistance presents an ever-increasing global health threat that involves all major microbial pathogens and antimicrobial drugs [
3,
4,
10]. There have been reported evidences of multi-drug resistant diarrhoeagenic bacteria [
5,
6,
11] around the world including in Nigeria.
The rural communities of Africa (including Nigeria) and other parts of the world have been using herbal drugs to manage diarrhea caused by bacteria [
12,
13,
14] and the organisms
E. coli,
B. cereus and
S. aureus have all been reported as causing childhood diarrhea [
14,
15]. An herbal medicine could have similar pharmacological effects as conventional drugs [
16] and concomitant use may result in diminution, addition, or potentiation of the two single effects. The implications of herb–drug interactions are, therefore, considered to be multi-dimensional and multi-factorial [
16,
17].
The plants—Vernonia amygdalina and Garcinia kola—are well known indigenous plant with several pharmacological activities but it is not yet known, scientifically, if any synergy (and at what combination ratio) exist between them. Also, in the management of multi-drug resistant diarrhoeagenic bacterial infections, we do not have any scientific proof that both plants can be used to control them. This research work, therefore, seeks to evaluate the combined effects of Vernonia amygdalina and Garcinia kola, locally used individually to manage bacteria diarrhea, as well as the combined effects of the herbal extracts with some orthodox drugs (tetracycline and metronidazole) against diarrhea causing bacteria. This study may justify, or otherwise invalidate, the indigenous use of the plant extracts in the treatment of diarrheal diseases.
3. Results
Table 1 shows the yields after extraction and lyophilization for the two plants. The ethanolic extracts present a better extraction yield.
The result of the confirmatory tests for the diarrhea causing bacteria isolates (
Bacillus cereus,
Escherichia coli,
Staphylococcus aureus, and
Salmonella spp.) are shown in
Figure 1. Mannitol salt agar identified the presence of
Staphylococcus aureus (creamy big cluster colonies);
Salmonella-shigellae agar was used to identify the presence of
Salmonella spp. (blackish rod like colonies), starch agar revealed the presence of
Bacillus cereus (yellow colored slightly opalescent gel—clearing around the colony) while MacConkey agar helped in the identification of
E. coli (dry pinkish colonies) as previously reported by Cheesbrough [
18].
The antibiotic susceptibility profile of the test organisms is shown in
Table 2. The microorganisms were found to be resistant to many of the standard antibiotics used.
Multi-Antibiotic Resistance Index (MARI) Calculations: The Multi-Antibiotic Resistance Indices of the isolates were calculated as
x/y [
24,
25].
Where x is the number of antibiotics to which the isolate was resistant and y is the number of antibiotics to which the isolate was subjected = 11.
All the isolates have a MARI of more than 20% with three-quarter of them having a MARI of even greater than 50% (
Table 3). Higher MARI signifies high multi-drug resistance character.
The antibacterial activities of the aqueous and ethanolic extracts of
Garcinia kola on the test isolates are shown in
Table 4 indicating that the isolates were more susceptible to the ethanolic extracts of the tested plants compared to the aqueous extracts. The zones of inhibition exhibited by the extracts against the tested bacterial isolates ranged between 0.0 to 9.0 mm.
The antibacterial activities of the aqueous and ethanolic extracts of
Vernonia amygdalina on the test isolates are shown in
Table 5. Isolates showed higher susceptibility to the ethanolic extract compared to the aqueous extracts. The zones of inhibition exhibited by the extracts against the tested bacterial isolates ranged between 0.0 to 15.0 mm.
The crude ethanolic extracts of the plants were more active against the test isolates (with MIC range 3.125–6.25 mg/mL) than the crude aqueous extracts of the plants (with MIC range 12.5–50 mg/mL)
Table 6.
The FIC indices for combination of crude extracts and then combination of the extracts with either metronidazole or tetracycline ranged from 6.55–0.21 as shown in
Table 7,
Table 8,
Table 9 and
Table 10. The combination of metronidazole and tetracycline showed mostly synergism against all test isolates. The combination of ethanolic
V. amygdalina extract and ethanolic
G. kola were synergistic only against
S. aureus and
E. coli and at selected combinations.
The tetracycline/ethanolic V. amygdalina extract combinations showed synergism mostly against E. coli compared to the other isolates and least synergy against B. cereus. Tetracycline/ethanolic G. kola extract combination performed better against the test isolates than the tetracycline/ethanolic V. amygdalina combination.
Metronidazole/ethanolic V. amygdalina extract combination was observed to show synergy only against E. coli and at selected combination ratios. However, the results were better than combinations of metronidazole with ethanolic G. kola extract. Metronidazole/aqueous G. kola extract combinations performed better than the metronidazole/ethanolic G. kola extract combination. For B. cereus and S. aureus diarrhoea, the best treatment appears to be metronidazole/aqueous G. kola extract combinations.
When the extracts were combined, the E.G. /A.G. and E.V./A.G combinations gave excellent results against S. aureus. The E.V. /A.G. combination proved to be a wrong combination.
Generally, the combinations aqueous G. kola + ethanolic G. kola and aqueous G. kola + ethanolic V. amygdalina showed more pronounced synergistic effects against the Staphylococcus aureus than B. cereus isolates with the fractional inhibition concentration (FIC) indices ranging from 0.32–0.95. The synergistic effects of tetracycline + crude extracts and metronidazole combinations were more pronounced on the test isolates and especially on the Gram-negative organism (E. coli) than B. cereus and S. aureus with FIC indices ranging from 0.41–0.91.
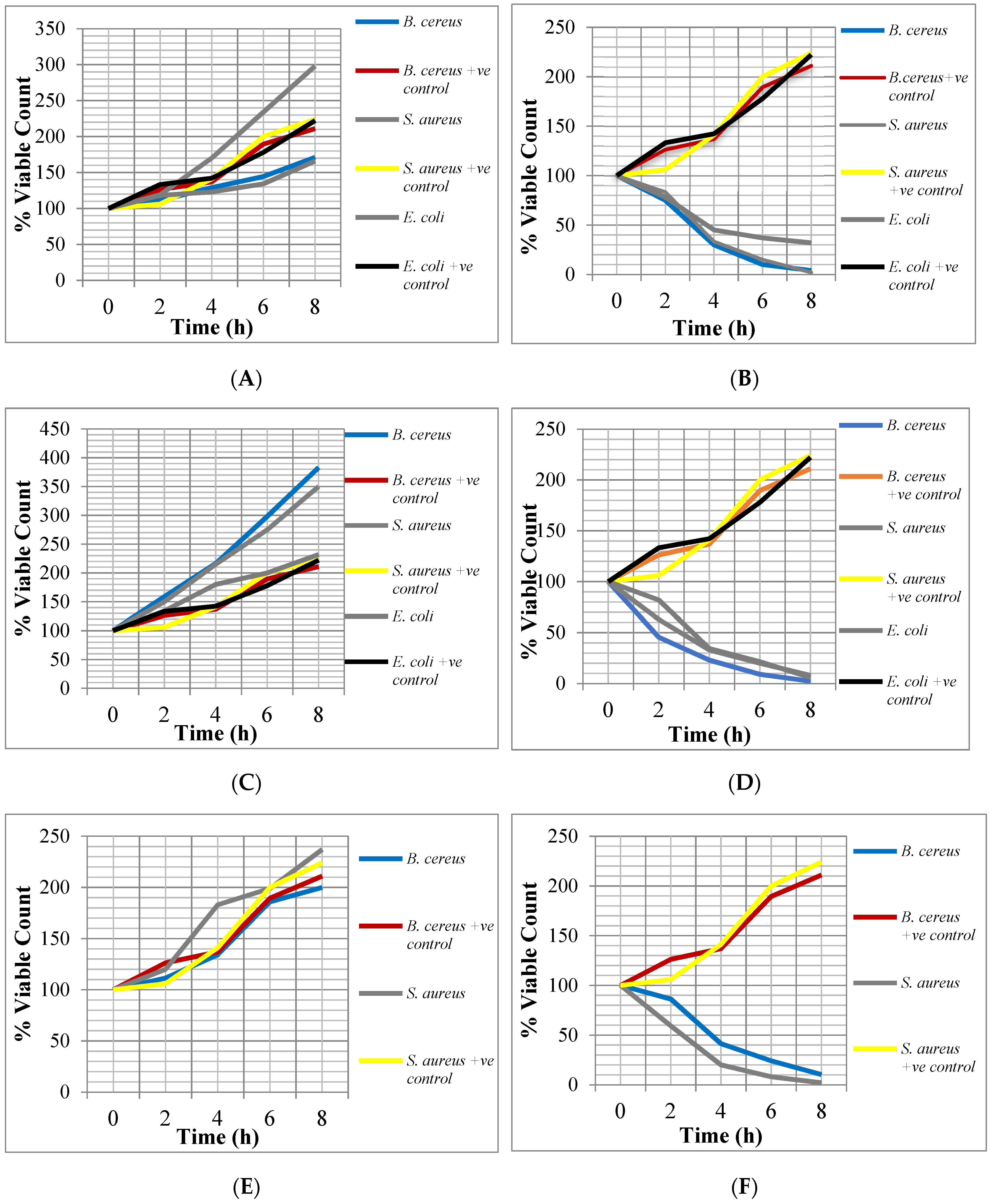
From
Figure 2, it can be observed that the crude extracts of the two plants showed bactericidal activity against
E. coli,
S. aureus and
B. cereus during the Time-Kill assay. After 2–4 h of incubating the bacteria with the ½ x MICs and 2 x MICs, the percentage viable cell count ranged between 216.2% and 20%. After 6–8 h of incubation with these different concentrations, the percentage viable cell count ranged between 186% and 2%. The bactericidal activity of the crude extracts against the test isolates increased with twice the MICs of the extracts but decreased at half their MICs.
4. Discussion
Indiscriminate use of antibiotics among the general population has favoured the emergence of resistant strains. Multi-drug resistance was observed in the test bacterial isolates with a MARI > 20%. Similar results were shown in earlier studies and results were attributed to selective pressure due antibiotic misuse [
7,
25,
26]. The susceptibility testing results are in line with the findings of antibiotic susceptibility tests done by other researchers [
27,
28] which showed that the isolates (
Escherichia coli,
Bacillus cereus,
Staphylococcus aureus, and
Salmonella spp.) are susceptible to some of the antibiotics used in this work (ofloxacin, ciprofloxacin, gentamicin, erythromycin, and ceftriaxone). The isolate
Bacillus cereus is particular resistant to the commercial antibiotics tested
Generally, the ethanolic extracts were more active than the aqueous extracts. They showed broader spectrum activity against the test isolates while the aqueous extracts showed less spectrum of activity. This could be attributed to the poor extractive power/strength of water as a solvent.
The ethanolic extracts of
Vernonia amygdalina leaves showed greater activity against
S. aureus, B. cereus and
E. coli. The inactivity or low antibacterial activity of the aqueous
V. amygdalina extract confirmed the work of Sule and Agbabiaka [
29] who recorded no antimicrobial activity of its aqueous extracts on strains of
E. coli, Klebsiella spp., and
Shigellae spp. and also reduced activity on
Salmonella spp. compared with the ethanolic extracts of the plant. The ethanolic extract of
G. kola seed showed activity against all the test isolates except
Salmonella while the aqueous extract showed activity against
B. cereus and
S. aureus. This may be due to the fact that ethanol was found to be a better solvent of extraction of the active principles of medicinal importance in plant [
30].
Ethanolic crude extract of
V. amygdalina displayed lower MICs (i.e., higher inhibitory activity) against the Gram-positive isolates than the Gram-negative isolates while aqueous
G. kola recorded high MICs (i.e. lower inhibitory activity) on test isolate (
Staphylococcus aureus). The difference between their MICs against the test isolate was extremely statistically significant (
p < 0.0007) compared with the statistical significances of ethanolic extracts of
V. amygdalina and
G. kola combined with the antibiotics (E.
V. vs. Metronidazole = 0.001, E.
G. vs. Metronidazole = 0.01, E.
V. vs. Tetracycline =
p < 0.05). This is consistent with the report by Ghamba et al. [
20], on in vitro antibacterial activity of crude ethanol, acetone, and aqueous
G. kola seed extracts on selected clinical isolates. Also, Adetunji et al. [
31] investigated the bacterial activity of crude extracts of
V. amygdalina on clinical isolates and reported that cold and hot ethanolic extract of
V. amygdalina rather than the aqueous extract of
V. amygdalina produced effective antimicrobial activities against
S. aureus,
P. aeruginosa and
E. coli; and the MICs were 25, 50, and 50 mg/mL for
S. aureus,
P. aeruginosa and
E. coli respectively, while the aqueous extract of
V. amygdalina did not show activity.
The ethanol extracts showed more activity against the bacteria isolates than the water extracts. This may be due to the higher polarity of the ethanol which tends to extract more active compounds from the plants than water [
31]. The killing ability of the plant extracts are quantity and time dependent. The growing problem of multi-drug-resistant pathogens has posed an age-long concern in the choice of antimicrobial therapy [
32]. Synergism from the combination of antimicrobial agents with crude plant extracts was verified and the results revealed the importance of plant extracts when combined with antibiotics to control diarrhoeagenic bacteria. The combinations (aqueous
G. kola + ethanolic
G. kola and aqueous
G. kola + ethanolic
V. amygdalina) showed more pronounced synergistic effects against
Staphylococcus aureus than
Bacillus cereus. The synergistic effects of tetracycline + crude extracts (ethanolic
G. kola, aqueous
G. kola and ethanolic
V. amygdalina) and metronidazole + crude extracts combinations were pronounced on the test isolates. The improvement in the activity of tetracycline and the crude extract may be due to the accumulation of inhibitory concentrations at the target site or due to other mechanisms. The combinations of metronidazole and crude ethanolic and aqueous extracts
G. kola and
V. amygdalina showed more indifference and less antagonistic effects. However, the combination of metronidazole with aqueous
G. kola recorded synergistic activities against
B. cereus and S. aureus. According to Chimezie et al. [
33], synergistic activity suggests different mode of actions of the combining compounds. Combined antimicrobials are preferred as microbial resistance is less likely to develop against substances having more than one mode of action [
34]. The antibacterial activities of all the extracts either when used separately or combined were concentration dependent as zones of growth inhibition increased with increasing concentration of the extracts. Some researchers had reported that the efficacy of most plant extracts is concentration-dependent [
35,
36].

 ,
, 


{kind=link}
{kind=link}