PES Pathogens in Severe Community-Acquired Pneumonia




Abstract
:1. Severe Community-Acquired Pneumonia: What Is the Current Definition?
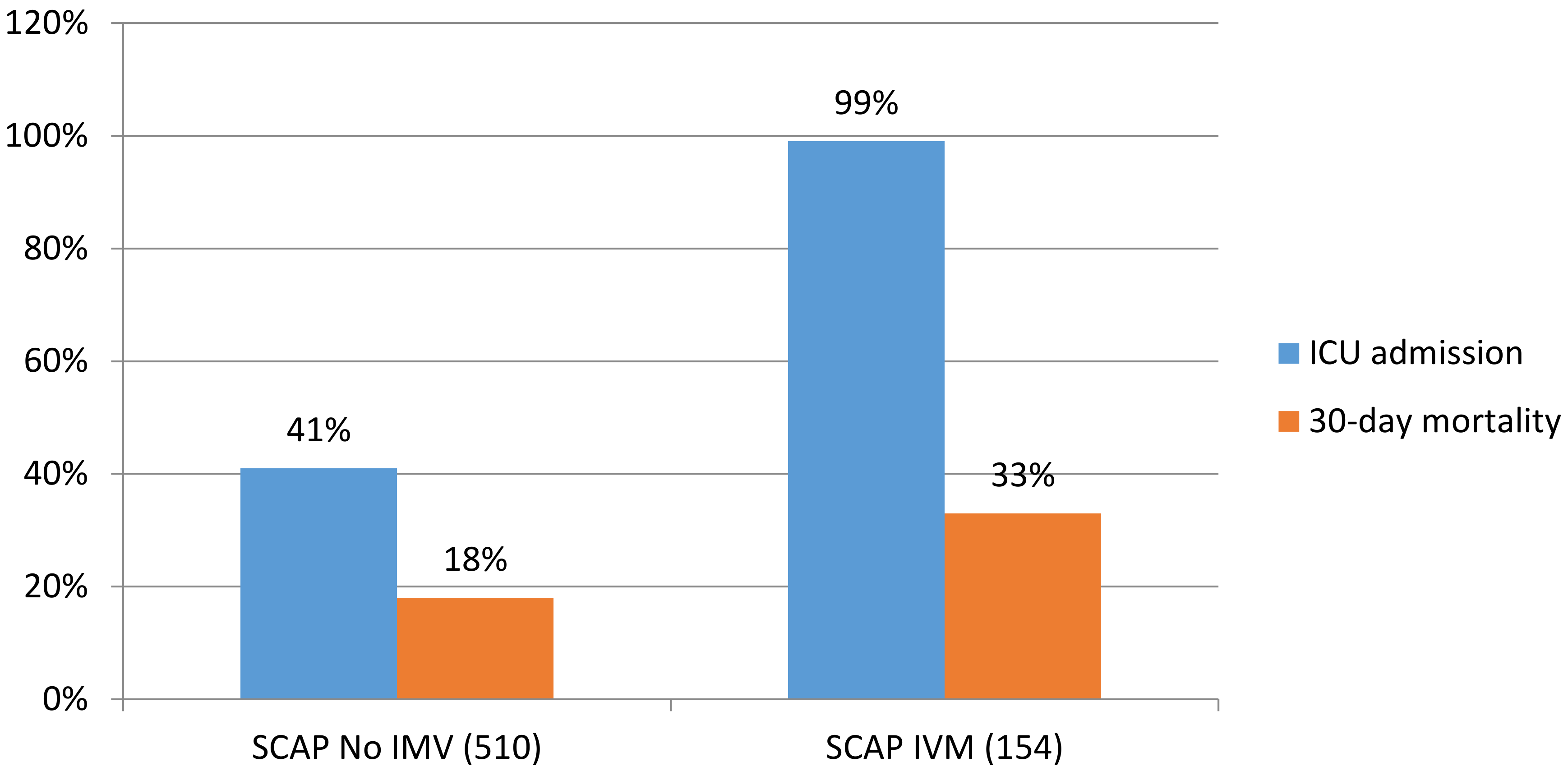
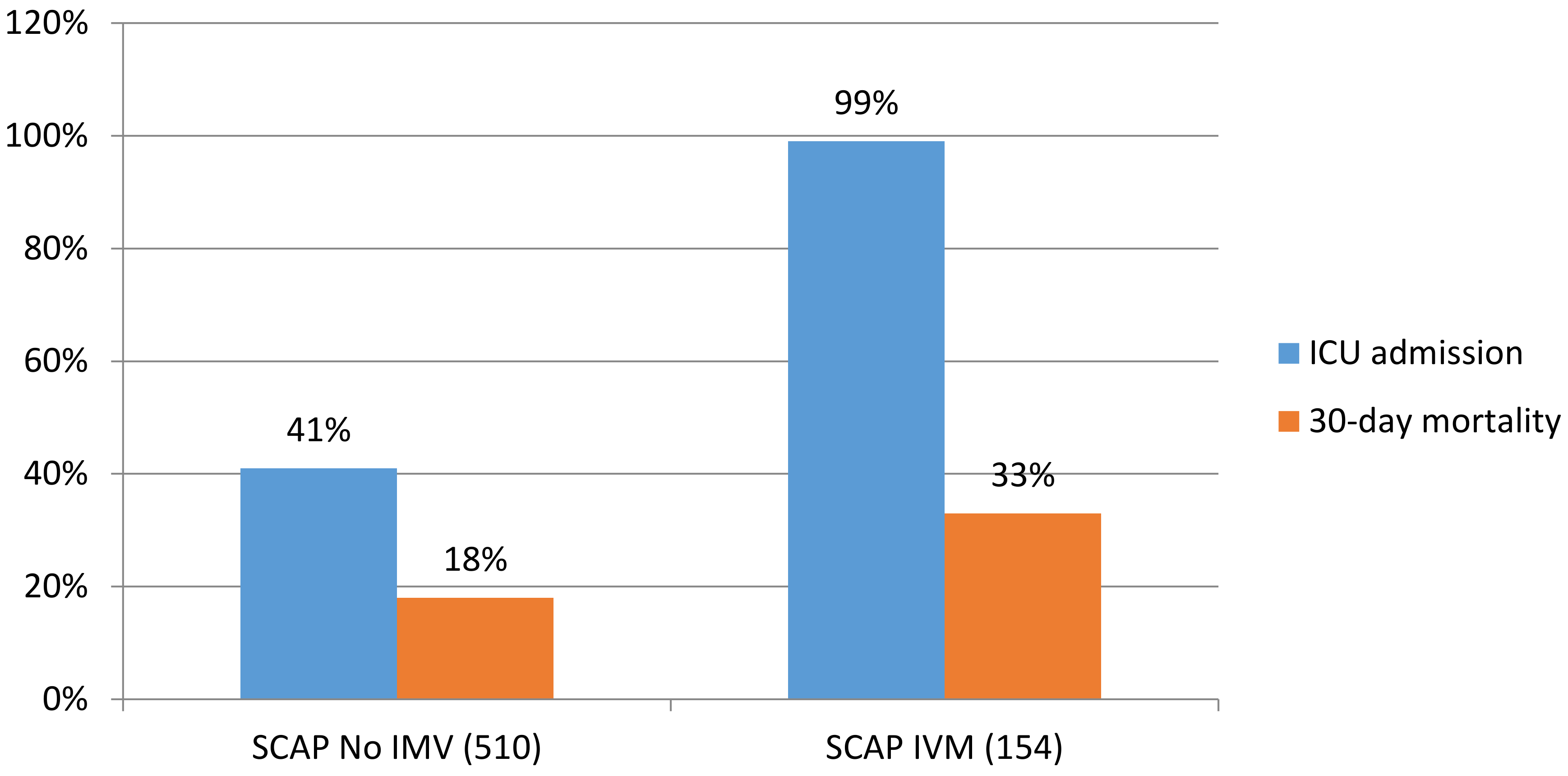
2. Admission to Intensive Care Units: What Is the Real Impact?
3. Outcomes of Patients with Severe Cap: What Are the Main Determinants?
4. Pathogens Beyond the Core Microorganisms of Cap: Should We Be Worried About Them?
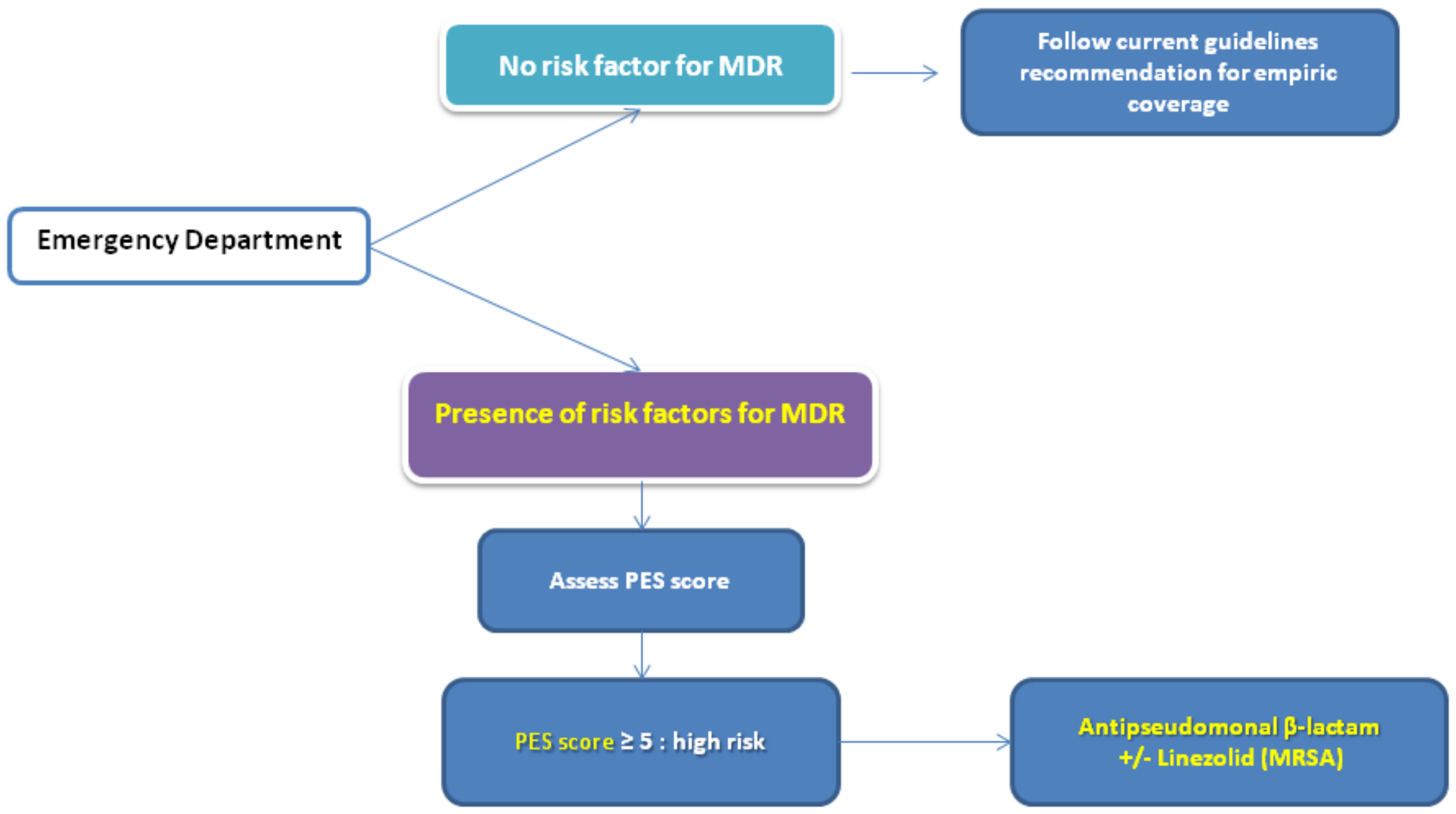
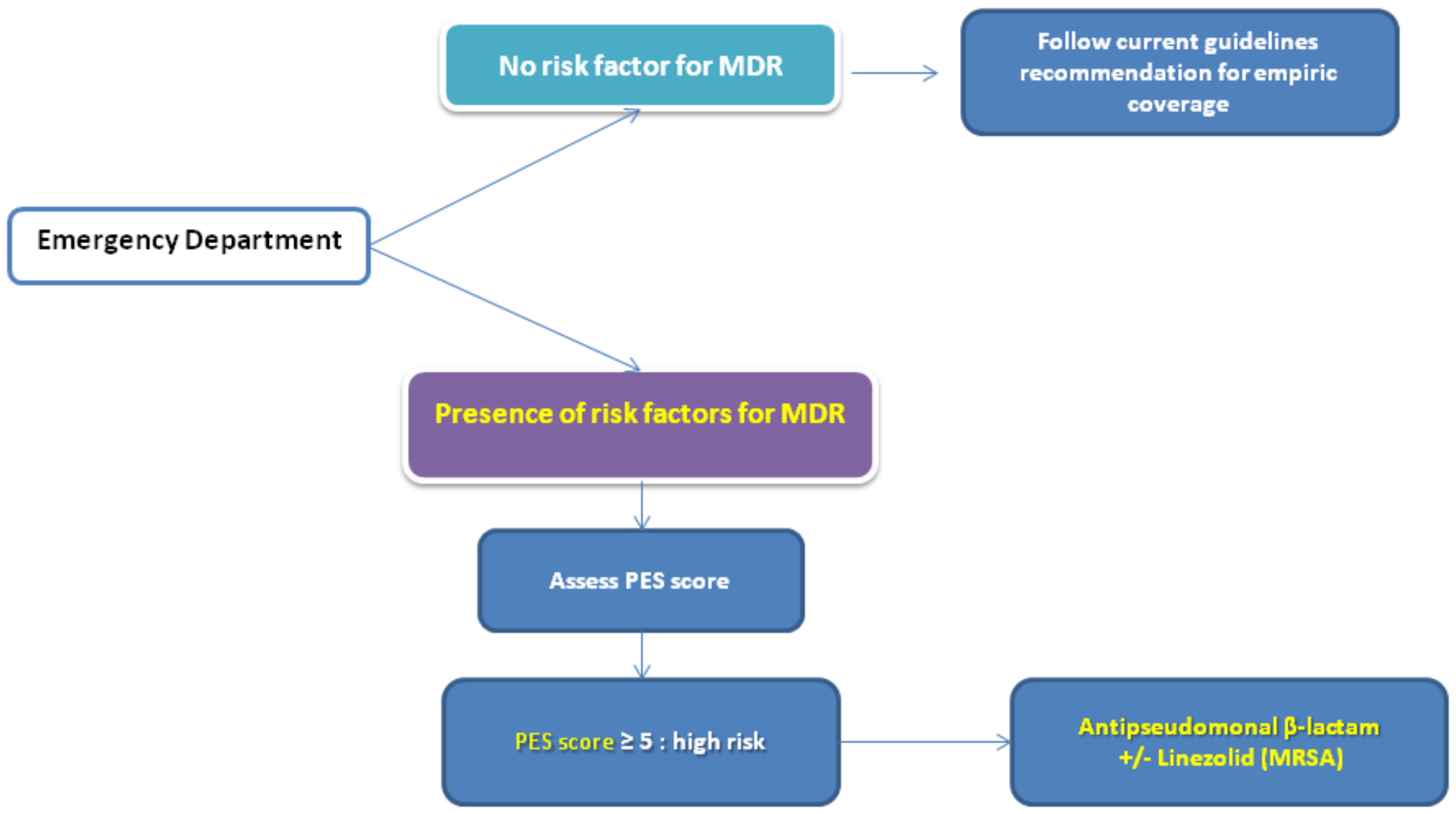
Risk Scores for Specific Pathogens (MRSA and P. aeruginosa)
5. Empiric Antibiotic Therapy in Severe CAP Caused by PES Pathogens: Is There Something New?
6. Are There Any New Antibiotics for PES Pathogens in Severe CAP?
- Loading dose: 200 mg by intravenous infusion over 60 min on day 1 or 100 mg by intravenous infusion over 30 min twice on day 1.
- Maintenance dose: 100 mg by intravenous infusion over 30 min once daily or 300 mg orally once daily.
- Duration: 7 to 14 days.
7. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44, S27–S72. [Google Scholar] [CrossRef] [PubMed]
- Flaatten, H.; de Lange, D.W.; Artigas, A.; Bin, D.; Moreno, R.; Christensen, S.; Joynt, G.M.; Bagshaw, S.M.; Sprung, C.L.; Benoit, D.; et al. The status of intensive care medicine research and a future agenda for very old patients in the ICU. Intensive Care Med. 2017, 43, 1319–1328. [Google Scholar] [CrossRef] [PubMed]
- Harpaz, R.; Dahl, R.M.; Dooling, K.L. Prevalence of Immunosuppression Among US Adults, 2013. JAMA 2016, 316, 2547–2548. [Google Scholar] [CrossRef] [PubMed]
- Linden, P.K. Approach to the immunocompromised host with infection in the intensive care unit. Infect. Dis. Clin. North. Am. 2009, 23, 535–556. [Google Scholar] [CrossRef] [PubMed]
- Florescu, D.F.; Sandkovsky, U.; Kalil, A.C. Sepsis and Challenging Infections in the Immunosuppressed Patient in the Intensive Care Unit. Infect. Dis. Clin. North. Am. 2017, 31, 415–434. [Google Scholar] [CrossRef] [PubMed]
- Haas, L.E.M.; Karakus, A.; Holman, R.; Cihangir, S.; Reidinga, A.C.; de Keizer, N.F. Trends in hospital and intensive care admissions in the Netherlands attributable to the very elderly in an ageing population. Crit Care 2015, 19. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Webb, S.A.R.; Delaney, A.; George, C.; Pilcher, D.; Hart, G.K.; Bellomo, R. Very old patients admitted to intensive care in Australia and New Zealand: A multi-centre cohort analysis. Crit Care 2009, 13, R45. [Google Scholar] [CrossRef]
- Roch, A.; Wiramus, S.; Pauly, V.; Forel, J.-M.; Guervilly, C.; Gainnier, M.; Papazian, L. Long-term outcome in medical patients aged 80 or over following admission to an intensive care unit. Crit Care 2011, 15, R36. [Google Scholar] [CrossRef]
- Tabah, A.; Philippart, F.; Timsit, J.F.; Willems, V.; Français, A.; Leplège, A.; Carlet, J.; Bruel, C.; Misset, B.; Garrouste-Orgeas, M. Quality of life in patients aged 80 or over after ICU discharge. Crit Care 2010, 14, R2. [Google Scholar] [CrossRef]
- Pavoni, V.; Gianesello, L.; Paparella, L.; Buoninsegni, L.T.; Mori, E.; Gori, G. Outcome and quality of life of elderly critically ill patients: An Italian prospective observational study. Arch. Gerontol Geriatr 2012, 54, e193–e198. [Google Scholar] [CrossRef]
- Andersen, F.H.; Kvåle, R. Do elderly intensive care unit patients receive less intensive care treatment and have higher mortality? Acta Anaesthesiol Scand 2012, 56, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Wunsch, H. Is there a Starling curve for intensive care? Chest 2012, 141, 1393–1399. [Google Scholar] [CrossRef] [PubMed]
- Laporte, L.; Hermetet, C.; Jouan, Y.; Gaborit, C.; Rouve, E.; Shea, K.M.; Si-Tahar, M.; Dequin, P.-F.; Grammatico-Guillon, L.; Guillon, A. Ten-year trends in intensive care admissions for respiratory infections in the elderly. Ann. Intensive Care 2018, 8, 84. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, M.; Travierso, C.; Cilloniz, C.; Gabarrus, A.; Ranzani, O.T.; Polverino, E.; Liapikou, A.; Blasi, F.; Torres, A. Severe community-acquired pneumonia: Characteristics and prognostic factors in ventilated and non-ventilated patients. PLoS ONE 2018, 13, e0191721. [Google Scholar] [CrossRef]
- Cilloniz, C.; Ferrer, M.; Liapikou, A.; Garcia-Vidal, C.; Gabarrus, A.; Ceccato, A.; Puig de La Bellacasa, J.; Blasi, F.; Torres, A. Acute respiratory distress syndrome in mechanically ventilated patients with community-acquired pneumonia. Eur. Respir. J. 2018, 51. [Google Scholar] [CrossRef] [PubMed]
- Kolditz, M.; Ewig, S.; Klapdor, B.; Schütte, H.; Winning, J.; Rupp, J.; Suttorp, N.; Welte, T.; Rohde, G.; CAPNETZ study group. Community-acquired pneumonia as medical emergency: Predictors of early deterioration. Thorax 2015, 70, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Montull, B.; Menéndez, R.; Torres, A.; Reyes, S.; Méndez, R.; Zalacaín, R.; Capelastegui, A.; Rajas, O.; Borderías, L.; Martin-Villasclaras, J.; et al. Predictors of Severe Sepsis among Patients Hospitalized for Community-Acquired Pneumonia. PLoS ONE 2016, 11, e0145929. [Google Scholar] [CrossRef]
- Cavalleri, M.; Barbagelata, E.; Diaz de Teran, T.; Ferraioli, G.; Esquinas, A.; Nicolini, A. Noninvasive and invasive ventilation in severe pneumonia: Insights for the noninvasive ventilatory approach. J. Crit. Care 2018. [Google Scholar] [CrossRef]
- Jain, S.; Self, W.H.; Wunderink, R.G.; Fakhran, S.; Balk, R.; Bramley, A.M.; Reed, C.; Grijalva, C.G.; Anderson, E.J.; Courtney, D.M.; et al. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. N. Engl. J. Med. 2015, 373, 415–427. [Google Scholar] [CrossRef]
- David-João, P.G.; Guedes, M.H.; Réa-Neto, Á.; de Chaiben, V.B.O.; Baena, C.P. Noninvasive ventilation in acute hypoxemic respiratory failure: A systematic review and meta-analysis. J. Crit. Care 2018, 49, 84–91. [Google Scholar]
- Cohen, J.; Vincent, J.-L.; Adhikari, N.K.J.; Machado, F.R.; Angus, D.C.; Calandra, T.; Jaton, K.; Giulieri, S.; Delaloye, J.; Opal, S.; et al. Sepsis: A roadmap for future research. Lancet Infect. Dis 2015, 15, 581–614. [Google Scholar] [CrossRef]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. International Forum of Acute Care Trialists Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Georges, H.; Journaux, C.; Devos, P.; Alfandari, S.; Delannoy, P.Y.; Meybeck, A.; Chiche, A.; Boussekey, N.; Leroy, O. Improvement in process of care and outcome in patients requiring intensive care unit admission for community acquired pneumonia. BMC Infect. Dis. 2013, 13, 196. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Carlet, J.M.; Masur, H.; Gerlach, H.; Calandra, T.; Cohen, J.; Gea-Banacloche, J.; Keh, D.; Marshall, J.C.; Parker, M.M.; et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Intensive Care Med. 2004, 30, 536–555. [Google Scholar] [CrossRef]
- Gattarello, S.; Borgatta, B.; Solé-Violán, J.; Vallés, J.; Vidaur, L.; Zaragoza, R.; Torres, A.; Rello, J. Community-Acquired Pneumonia en la Unidad de Cuidados Intensivos II Study Investigators. Decrease in mortality in severe community-acquired pneumococcal pneumonia: Impact of improving antibiotic strategies (2000–2013). Chest 2014, 146, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, S.; Cilloniz, C.; Chalmers, J.D.; Zanaboni, A.M.; Cosentini, R.; Tarsia, P.; Pesci, A.; Blasi, F.; Torres, A. Multidrug-resistant pathogens in hospitalised patients coming from the community with pneumonia: A European perspective. Thorax 2013, 68, 997–999. [Google Scholar] [CrossRef]
- Falcone, M.; Russo, A.; Giannella, M.; Cangemi, R.; Scarpellini, M.G.; Bertazzoni, G.; Alarcón, J.M.; Taliani, G.; Palange, P.; Farcomeni, A.; et al. Individualizing risk of multidrug-resistant pathogens in community-onset pneumonia. PLoS ONE 2015, 10, e0119528. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Aliberti, S.; Di Pasquale, M.; Zanaboni, A.M.; Cosentini, R.; Brambilla, A.M.; Seghezzi, S.; Tarsia, P.; Mantero, M.; Blasi, F. Stratifying risk factors for multidrug-resistant pathogens in hospitalized patients coming from the community with pneumonia. Clin. Infect. Dis. 2012, 54, 470–478. [Google Scholar] [CrossRef]
- Prina, E.; Ranzani, O.T.; Polverino, E.; Cillóniz, C.; Ferrer, M.; Fernandez, L.; Puig de la Bellacasa, J.; Menéndez, R.; Mensa, J.; Torres, A. Risk Factors Associated with Potentially Antibiotic-Resistant Pathogens in Community-Acquired Pneumonia. Annals ATS 2014, 12, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Webb, B.J.; Dascomb, K.; Stenehjem, E.; Vikram, H.R.; Agrwal, N.; Sakata, K.; Williams, K.; Bockorny, B.; Bagavathy, K.; Mirza, S.; et al. Derivation and Multicenter Validation of the Drug Resistance in Pneumonia Clinical Prediction Score. Antimicrob. Agents Chemother. 2016, 60, 2652–2663. [Google Scholar] [CrossRef] [PubMed]
- Ishida, T.; Ito, A.; Washio, Y.; Yamazaki, A.; Noyama, M.; Tokioka, F.; Arita, M. Risk factors for drug-resistant pathogens in immunocompetent patients with pneumonia: Evaluation of PES pathogens. J. Infect. Chemother. 2017, 23, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Shorr, A.F.; Myers, D.E.; Huang, D.B.; Nathanson, B.H.; Emons, M.F.; Kollef, M.H. A risk score for identifying methicillin-resistant Staphylococcus aureus in patients presenting to the hospital with pneumonia. BMC Infect. Dis. 2013, 13, 268. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, M.I.; Babu, B.L.; Reyes, L.F.; Chalmers, J.D.; Soni, N.J.; Sibila, O.; Faverio, P.; Cilloniz, C.; Rodriguez-Cintron, W.; Aliberti, S. Burden and Risk Factors for Pseudomonas aeruginosa Community-acquired Pneumonia: A Multinational Point Prevalence Study of Hospitalised Patients. Eur. Respir. J. 2018. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, T.; Fujisawa, T.; Ishida, T.; Ito, A.; Oyamada, Y.; Fujimoto, K.; Yoshida, M.; Maeda, H.; Miyashita, N.; Nagai, H.; et al. A Therapeutic Strategy for All Pneumonia Patients: A 3-Year Prospective Multicenter-Cohort Study Using Risk Factors for Multidrug Resistant Pathogens to Select Initial Empiric Therapy. Clin. Infect. Dis. 2018. [Google Scholar] [CrossRef]
- Lim, W.S.; Baudouin, S.V.; George, R.C.; Hill, A.T.; Jamieson, C.; Le Jeune, I.; Macfarlane, J.T.; Read, R.C.; Roberts, H.J.; Levy, M.L.; et al. BTS guidelines for the management of community acquired pneumonia in adults: Update 2009. Thorax 2009, 64, iii1–iii55. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, H.J.; Kim, Y.H. Is β-Lactam Plus Macrolide More Effective than β-Lactam Plus Fluoroquinolone among Patients with Severe Community-Acquired Pneumonia? A Systemic Review and Meta-Analysis. J. Korean Med. Sci. 2017, 32, 77–84. [Google Scholar] [CrossRef]
- Ceccato, A.; Cilloniz, C.; Martin-Loeches, I.; Ranzani, O.T.; Gabarrus, A.; Bueno, L.; Garcia-Vidal, C.; Ferrer, M.; Niederman, M.S.; Torres, A. Effect of Combined β-Lactam/Macrolide Therapy on Mortality According to the Microbial Aetiology and Inflammatory Status of Patients with Community—Acquired Pneumonia. Chest 2018. [Google Scholar] [CrossRef]
- Garin, N.; Genné, D.; Carballo, S.; Chuard, C.; Eich, G.; Hugli, O.; Lamy, O.; Nendaz, M.; Petignat, P.-A.; Perneger, T.; et al. β-Lactam monotherapy vs. β-lactam-macrolide combination treatment in moderately severe community-acquired pneumonia: A randomized noninferiority trial. JAMA Intern. Med. 2014, 174, 1894–1901. [Google Scholar] [CrossRef] [PubMed]
- Postma, D.F.; van Werkhoven, C.H.; van Elden, L.J.R.; Thijsen, S.F.T.; Hoepelman, A.I.M.; Kluytmans, J.A.J.W.; Boersma, W.G.; Compaijen, C.J.; van der Wall, E.; Prins, J.M.; et al. Antibiotic treatment strategies for community-acquired pneumonia in adults. N. Engl. J. Med. 2015, 372, 1312–1323. [Google Scholar] [CrossRef] [PubMed]
- European Commission. A European One Health Action Plan Against Antimicrobial Resistance 2017. Available online: https://ec.europa.eu/health/amr/sites/amr/files/amr_action_plan_2017_en.pdf (accessed on 6 February 2019).
- Hebeisen, P.; Heinze-Krauss, I.; Angehrn, P.; Hohl, P.; Page, M.G.; Then, R.L. In vitro and in vivo properties of Ro 63-9141, a novel broad-spectrum cephalosporin with activity against methicillin-resistant staphylococci. Antimicrob. Agents Chemother. 2001, 45, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, S.C.; Welte, T.; File, T.M.; Strauss, R.S.; Michiels, B.; Kaul, P.; Balis, D.; Arbit, D.; Amsler, K.; Noel, G.J. A randomised, double-blind trial comparing ceftobiprole medocaril with ceftriaxone with or without linezolid for the tretableatment of patients with community-acquired pneumonia requiring hospitalisation. Int. J. Antimicrob. Agents 2012, 39, 240–246. [Google Scholar] [CrossRef]
- Basilea Pharmaceutica—News and Media. Available online: http://www.basilea.com/News-and-Media/Basilea-reports-2015-half-year-results-Major-milestones-achieved-for-CRESEMBA-and-Zevtera/8cd5fd46-684f-247f-ef91-f9c42113a5a7/ (accessed on 4 December 2018).
- CNW|Cardiome Announces Agreement with Basilea for Distribution of Zevtera®/Mabelio® (Ceftobiprole) in Europe and Israel. Available online: https://www.newswire.ca/news-releases/cardiome-announces-agreement-with-basilea-for-distribution-of-zevteramabelio-ceftobiprole-in-europe-and-israel-643915603.html (accessed on 5 December 2018).
- File, T.M.; Low, D.E.; Eckburg, P.B.; Talbot, G.H.; Friedland, H.D.; Lee, J.; Llorens, L.; Critchley, I.A.; Thye, D.A.; FOCUS 1 investigators. FOCUS 1: A randomized, double-blinded, multicentre, Phase III trial of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in community-acquired pneumonia. J. Antimicrob. Chemother. 2011, 66, iii19–iii32. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E.; File, T.M.; Eckburg, P.B.; Talbot, G.H.; David Friedland, H.; Lee, J.; Llorens, L.; Critchley, I.A.; Thye, D.A.; FOCUS 2 investigators. FOCUS 2: A randomized, double-blinded, multicentre, Phase III trial of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in community-acquired pneumonia. J. Antimicrob. Chemother. 2011, 66, iii33–iii44. [Google Scholar] [CrossRef] [PubMed]
- Drug Approval Package: Teflaro (ceftaroline fosamil) NDA #200327. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/200327orig1s000toc.cfm (accessed on 6 February 2019).
- Zinforo|European Medicines Agency. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/zinforo#authorisation-details-section (accessed on 6 February 2019).
- Press Releases NUZYRA (omadacycline). Available online: https://investors.nabriva.com/news-releases/news-release-details/nabriva-therapeutics-announces-positive-topline-results-pivotal (accessed on 4 January 2019).
- Stets, R.; Popescu, M.; Gonong, J.; Mitha, I.; Nseir, W.; Madej, A.; Kirsch, C.; Das, A.; Garrity-Ryan, L.; Steenbergen, J.N.; et al. A Phase 3 Randomized, Double-Blind, Multi-Center Study to Compare the Safety and Efficacy of IV to Oral Omadacycline to Moxifloxacin for the Treatment of Adult Patients with CABP (The OPTIC Study). 1. Open Forum Infect. Dis. 2017, 4, S543–S544. [Google Scholar] [CrossRef]
- Pharmaceuticals, P. Paratek Announces Acceptance of European Marketing Authorization Application for Oral and Intravenous Omadacycline. Available online: http://globenewswire.com/news-release/2018/10/04/1603448/0/en/Paratek-Announces-Acceptance-of-European-Marketing-Authorization-Application-for-Oral-and-Intravenous-Omadacycline.html (accessed on 6 February 2019).
- Navriba Threrapeutics. Lefamulin Evaluation Against Pneumonia (LEAP 1) Phase 3 Topline Results. Available online: https://investors.nabriva.com/static-files/6e30369b-5ef7-4baf-b461-8ae5580771c1 (accessed on 6 February 2019).
- Navriba therapeutics. Lefamulin Evaluation Against Pneumonia (LEAP 2) Phase 3 Topline Results. Available online: https://investors.nabriva.com/static-files/5c34b447-99cc-4739-b9d6-d4ea4c7d13b9 (accessed on 6 February 2019).

{kind=link}
{kind=link}
| Major Criteria |
|---|
| Invasive mechanical ventilation |
| Septic shock |
| Minor Criteria |
| Blood urea nitrogen level ≥20 mg/dL (7.14 mmol/L) |
| Confusion/disorientation |
| Hypotension requiring aggressive fluid resuscitation |
| Hypothermia (core temperature <96.8°F (36 °C)) |
| Leukopenia (white blood cell count <4000 cells/mm3 (4.00 × 109/L)) |
| Multilobar infiltrates |
| PaO2/FiO2 ratio ≤250 |
| Respiratory rate ≥30 breaths/minute |
| Thrombocytopenia (platelets <100 × 103 cells/mm3 (100 × 109/L)) |
| Category | Definition |
|---|---|
| Multidrug resistance (MDR) | Non-susceptibility to at least one agent in three or more antimicrobial categories |
| Extensively drug resistance (XDR) | Non-susceptibility to at least one agent in all but two or fewer antimicrobial categories |
| Pan drug resistance (PDR) | Non-susceptibility to all agents in all antimicrobial categories |
| Score to PES Pathogen | Points |
|---|---|
| Age > 65 | 1 point |
| Male | 2 point |
| Previous antibiotic use | 2 point |
| Chronic respiratory disorder | 2 point |
| Chronic renal disease | 2 point |
| At Emergency | |
| Consciousness impairment or aspiration evidence | 2 point |
| Fever or shivers | −1 point |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cillóniz, C.; Dominedò, C.; Nicolini, A.; Torres, A. PES Pathogens in Severe Community-Acquired Pneumonia. Microorganisms 2019, 7, 49. https://doi.org/10.3390/microorganisms7020049
Cillóniz C, Dominedò C, Nicolini A, Torres A. PES Pathogens in Severe Community-Acquired Pneumonia. Microorganisms. 2019; 7(2):49. https://doi.org/10.3390/microorganisms7020049
Chicago/Turabian StyleCillóniz, Catia, Cristina Dominedò, Antonello Nicolini, and Antoni Torres. 2019. "PES Pathogens in Severe Community-Acquired Pneumonia" Microorganisms 7, no. 2: 49. https://doi.org/10.3390/microorganisms7020049
APA StyleCillóniz, C., Dominedò, C., Nicolini, A., & Torres, A. (2019). PES Pathogens in Severe Community-Acquired Pneumonia. Microorganisms, 7(2), 49. https://doi.org/10.3390/microorganisms7020049